Disclosure: Some links on this site are affiliate links. If you purchase through these links, we may earn a commission at no extra cost to you. Thank you for supporting our site.·For informational purposes only—not medical advice.
GLP‑1 Hair Loss (Ozempic, Wegovy, Zepbound): What the Data Shows + What To Do
By the WPG Research Team | Last verified: February 2026 | Sources: FDA prescribing information, published clinical trials, peer-reviewed dermatology research — see full source list below
Yes, GLP‑1 medications are linked to hair loss — and if you're finding more hair in your brush or shower drain a few months into treatment, you're not imagining it. FDA clinical trial data confirms hair loss was reported in 3–5% of people taking weight-loss GLP‑1s like Wegovy and Zepbound (compared to about 1% on placebo). Real-world frequency is still uncertain — rates may differ due to reporting and how fast or how much weight loss varies person to person.
Here's what matters most: in most cases, this is temporary. The culprit is usually a condition called telogen effluvium — a reversible shedding pattern triggered by rapid weight loss and nutritional shifts, not permanent follicle damage. Shedding often improves over ~3–6 months once the trigger stabilizes, and visible density can take additional months to return.
But “temporary” doesn't mean “ignore it.” There are specific steps you can take right now to slow shedding, speed recovery, and know when something more serious might be going on. We built this guide to be the only page you need — with FDA label data for the major GLP‑1s most commonly used for weight loss (and the most-searched brand-name diabetes versions), a clear timeline of what to expect, and an action plan you can start today.

*For educational purposes only — not medical advice.*
FDA Evidence Table: Hair Loss Rates by GLP‑1 Medication
Before we get into the “why,” here's what the FDA prescribing labels actually say — drug by drug. We pulled this directly from the official FDA label for each medication so you can verify it yourself.
| Medication | Active Ingredient | Hair Loss in FDA Label? | Reported Rate | vs. Placebo | Key Detail |
|---|---|---|---|---|---|
| Wegovy (injection) | Semaglutide 2.4 mg | Yes — clinical trial adverse reaction | 3% (adults); 4% (adolescents) | 1% (adults); 0% (adolescents) | Listed as adverse reaction in trials (adults and pediatrics) |
| Zepbound | Tirzepatide | Yes — listed in FDA label adverse reaction table (≥2% and greater than placebo) | 4–5% by dose (5/4/5%) | ~1% | More frequent in women (reported); associated with weight reduction |
| Ozempic | Semaglutide 0.5–2 mg | Yes — postmarketing section only | No clinical trial rate listed | — | Alopecia appears in postmarketing reports; same active ingredient as Wegovy at lower dose |
| Mounjaro | Tirzepatide | Yes — postmarketing section only | No clinical trial rate listed | — | Same active ingredient as Zepbound; approved for diabetes (not weight loss) |
| Saxenda | Liraglutide | Yes — postmarketing experience includes alopecia | No clinical trial frequency reported | — | Added to postmarketing section in 2025 label revision |
What this table tells you: Hair loss is a recognized side effect in the FDA labels for the two major weight-loss GLP‑1s (Wegovy and Zepbound). For the diabetes-indication versions of the same drugs (Ozempic and Mounjaro), it appears in postmarketing reports but wasn't captured at significant rates in their original trials — likely because those trials involved less aggressive weight loss.
The key finding: Outside the U.S., Canada's Wegovy product monograph notes that hair loss was reported more often in adults who lost ≥20% of their body weight (5.3%) compared to those who lost less than 20% (2.5%). That's a strong signal that the weight loss itself — not the drug molecule — is the primary driver.
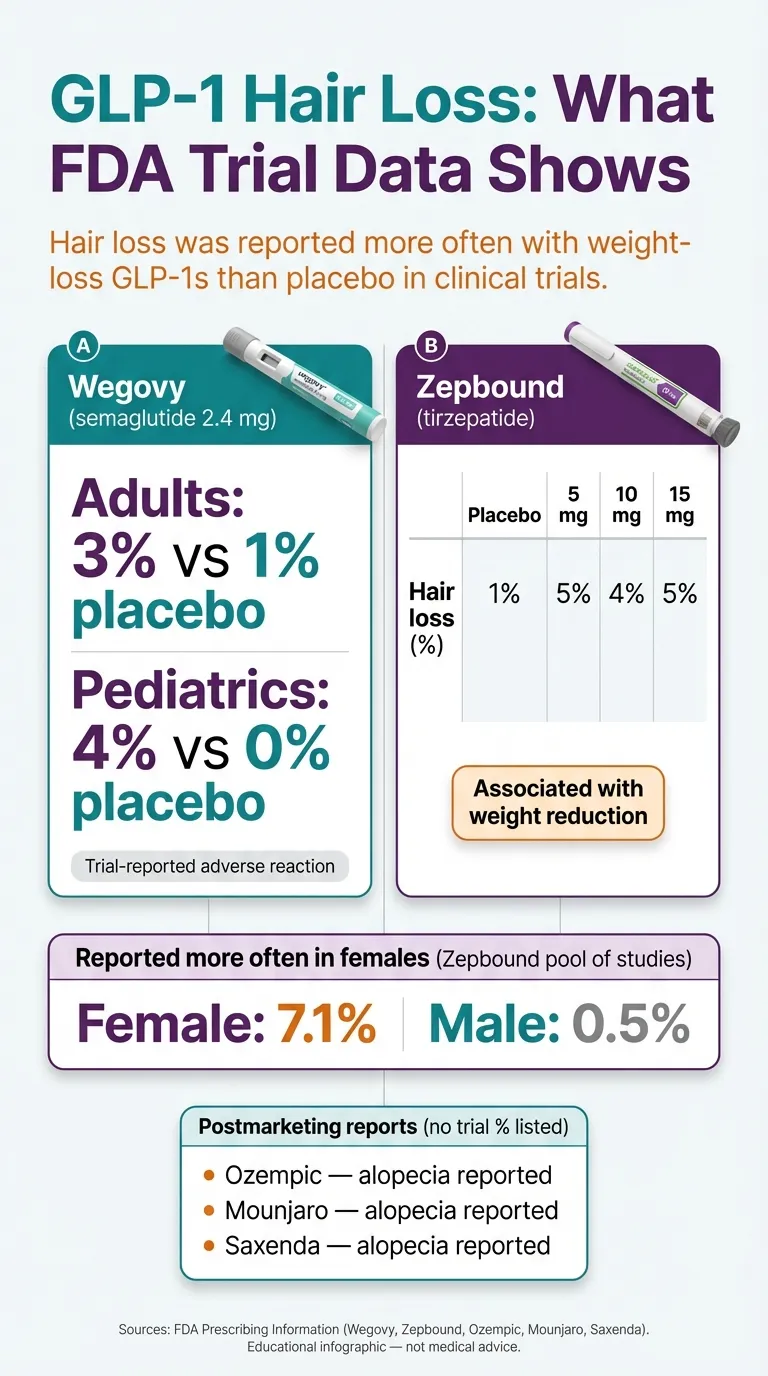
Sources: FDA Prescribing Information (Wegovy, Zepbound, Ozempic, Mounjaro, Saxenda). Educational infographic — not medical advice.
Does GLP‑1 Actually Cause Hair Loss — or Is It the Weight Loss?
This is the most important question, and the honest answer is: it's mostly the weight loss, but we can't completely rule out a direct medication effect.
The evidence pointing to weight loss as the primary driver
The strongest piece of evidence is the dose-response relationship with weight loss. Canada's Wegovy product monograph shows that people who lost more than 20% of their body weight had roughly double the hair loss rate (5.3%) compared to those who lost less (2.5%). That pattern is consistent with something called telogen effluvium — a well-documented reaction to rapid body changes that happens with any type of significant weight loss, not just GLP‑1s. Bariatric surgery patients experience telogen effluvium at rates up to 57%, according to research published in Obesity Surgery. Severe diets, post-pregnancy recovery, and major illness all trigger the same pattern.
A 2025 study from the University of British Columbia analyzed claims data from 16 million patients and found that semaglutide users had a 52% higher risk of hair loss compared to people taking bupropion-naltrexone (Contrave). But semaglutide also causes significantly more rapid weight loss than Contrave — so the difference may reflect the intensity of weight change, not a unique property of the drug.
The evidence that leaves the door open
The FDA's Adverse Event Reporting System (FAERS) has flagged both semaglutide and tirzepatide for alopecia signals. A disproportionality analysis of FAERS reports found higher reporting odds of alopecia for semaglutide (ROR ~2.46) and tirzepatide, which is a signal of disproportionate reporting — not a measure of how common it is and not proof the drug caused the event. And a large matched cohort study (Vidal et al., 547,993 matched adults) published online February 9, 2026 in the Journal of the American Academy of Dermatology reported higher odds of nonscarring hair loss and androgenetic alopecia at 6 months, and higher odds of telogen effluvium at 12 months among GLP‑1 RA users vs matched controls (observational — cannot prove causation).
Some researchers have also hypothesized that GLP‑1 medications may trigger hormonal shifts — particularly involving thyroid function and androgens — that could independently affect hair cycling. But this remains theoretical, not proven.
What this means for you
The most likely explanation for your shedding is that rapid weight loss put your body under metabolic stress, which pushed your hair follicles into a resting phase. The medication facilitated the weight loss; the weight loss triggered the shedding. You probably don't need to stop your medication — but you should take steps to support your body through the transition.
What Is Telogen Effluvium and Why Does It Happen on GLP‑1s?
Understanding what's happening in your body makes the whole thing less scary — so let's break down the mechanism in plain language.
Your hair grows in cycles. At any given time, about 85–90% of your scalp hairs are in the anagen (active growth) phase, which lasts 2–6 years. Around 5–10% are in the telogen (resting) phase, which lasts about 3 months before those hairs naturally shed and are replaced by new growth.
Telogen effluvium happens when something stresses your body enough that a larger-than-normal proportion of hair follicles get shoved into the resting phase all at once. Instead of 5–10% resting, you might have 30–50% resting simultaneously. A few months later, when those resting hairs finally release, you see what feels like alarming amounts of shedding.
On GLP‑1 medications, three things typically converge to create this stress:
1. The metabolic shock of rapid weight loss. When your body suddenly takes in far fewer calories than it's used to, it triages. Vital organs get priority. Hair growth — a biologically “optional” function — gets deprioritized. The faster the weight loss, the stronger this signal.
2. Nutritional gaps from eating less. GLP‑1s suppress appetite, which is the point — but it also means you're likely consuming less protein, iron, zinc, vitamin D, and B12 than before. Your hair is made of keratin, a protein. When protein intake drops, your body diverts what's available to critical tissues. Hair loses.
3. Hormonal recalibration. Significant weight loss changes insulin sensitivity, cortisol levels, thyroid function, and sex hormone balance. All of these affect hair cycling. Women in perimenopause or with PCOS may be especially sensitive to these shifts.
The critical detail people miss
The hair you're losing today was triggered to shed 2–3 months ago. There's a built-in delay between the stress event and the visible shedding. That's why hair loss seems to appear “suddenly” around months 3–6 of GLP‑1 treatment — it's not sudden at all. Your body made this decision weeks ago.
This also means that stopping the medication today won't immediately stop the shedding. The hairs already in the resting phase are going to shed regardless. What will help is stabilizing the triggers going forward — nutrition, rate of weight loss, and correcting deficiencies.
GLP‑1 Hair Loss Timeline: When It Starts, Peaks, and Stops
One of the most stressful parts of GLP‑1 hair loss is not knowing what to expect. Here's the typical timeline, based on clinical descriptions of telogen effluvium from the Cleveland Clinic and published dermatology literature.
| Phase | Timeframe | What's Happening Inside | What You'll Notice |
|---|---|---|---|
| Trigger | Months 0–2 | Rapid weight loss begins; follicles start shifting to telogen phase | Nothing yet — this is the silent period |
| Onset | Months 2–4 | Resting hairs begin to release as new follicles push them out | More hair in your brush, drain, or on your pillow |
| Peak Shedding | Months 4–6 | Maximum proportion of follicles in resting phase; heaviest shedding | Most alarming phase — this is when people panic |
| Stabilization | Months 6–9 | Weight loss slows or plateaus; new anagen growth begins | Shedding noticeably decreases; you may see short “baby hairs” |
| Recovery | Months 9–12+ | New hair grows in; density gradually returns | Hair feels thicker; volume returns over several months |

Source: Cleveland Clinic (telogen effluvium). Educational infographic — not medical advice.
A few important notes: This timeline assumes your weight eventually stabilizes. If you're still losing weight rapidly at month 8, the shedding window may extend. That's not a reason to stop treatment — it's a reason to talk to your provider about titration pace.
Hair grows about half an inch per month. Even after shedding stops and new growth begins, it takes several months before you notice meaningful density improvement. Progress photos (same lighting, same hair part) are more reliable than the mirror.
If your shedding follows a completely different pattern — started before you began GLP‑1 treatment, is concentrated in patches rather than diffuse across your scalp, or is accompanied by scalp pain, redness, or scaling — something else may be going on. We cover that next.
Am I Shedding Hair… or Actually Losing It? (The Diagnostic Framework)
Not all hair loss is the same, and knowing the difference matters because the treatments are completely different. This table is a non-diagnostic framework — it's not a replacement for a dermatologist, but it can help you figure out what to bring up at your appointment.
| What You're Seeing | Most Likely Pattern | Common Triggers | What Helps | Who to See |
|---|---|---|---|---|
| Diffuse shedding all over scalp | Telogen effluvium | Rapid weight loss, calorie deficit, nutritional deficiency | Nutrition optimization, slow weight loss, time | Start with prescriber; derm if persists >6 months |
| Widening part, thinning crown, or receding temples | Androgenetic alopecia (DHT-related) | Genetics, hormones, aging; may be unmasked by weight loss | Minoxidil, prescription options (clinician-directed) | Dermatologist |
| Round or oval bald patches | Alopecia areata | Autoimmune; can be triggered by stress | Prescription treatments; clinician-directed | Dermatologist (sooner rather than later) |
| Scaling, flaking, itching + broken hairs | Scalp inflammation / fungal infection | Various; may coexist with other conditions | Medicated shampoo, antifungals; clinician-directed | Dermatologist |
| Pain, burning, scarring, permanent-looking bald areas | Scarring alopecia | Various inflammatory conditions | Urgent — early treatment matters | Dermatologist (urgent) |
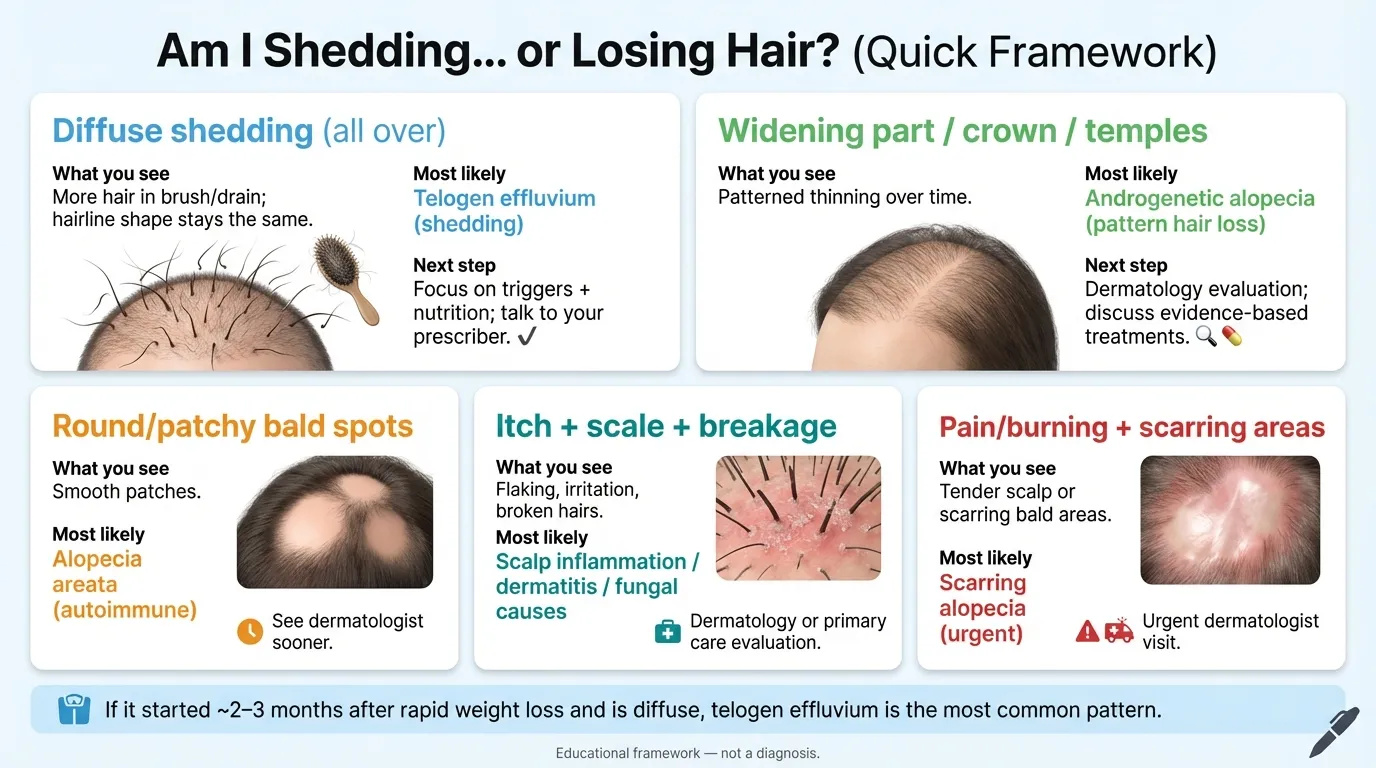
Educational framework — not a diagnosis.
The critical distinction for GLP‑1 users: If your shedding started 2–4 months after beginning or increasing your GLP‑1 dose, is diffuse (all over, not patchy), and your hairline shape hasn't changed — that's the classic telogen effluvium pattern. It's the most common scenario and the most reassuring one.
But here's a nuance most articles miss: Rapid weight loss can also unmask pre-existing androgenetic alopecia. Some dermatologists are seeing patients where the telogen effluvium reveals underlying pattern thinning that was previously hidden by thicker hair. If your shedding resolves but you notice your hair isn't quite the same — especially at the temples, crown, or part line — that's worth a dermatology consult. It's a different condition with different (and effective) treatments.
Red flags — see a dermatologist soon
- Patchy bald spots (not just diffuse thinning)
- Scalp pain, burning, redness, or scarring
- Shedding that started before your GLP‑1 or has persisted longer than 6 months after weight stabilized
- Other symptoms alongside hair loss: extreme fatigue, cold intolerance, menstrual irregularity, or unexplained weight changes (these could signal thyroid dysfunction)
- Eyebrow or eyelash loss
GLP‑1 Hair Loss in Women: Why It's Reported More Often
Women search for “GLP‑1 hair loss” far more than men, and the data backs up why.
The Zepbound prescribing label reported hair loss more frequently in women than in men during clinical trials. The UBC study found that women taking semaglutide had roughly double the risk of hair loss compared to women on bupropion-naltrexone, while the numbers for men were too small to draw conclusions (22 female cases vs. just 1 male case in that cohort).
Several factors make women more vulnerable:
Iron deficiency is far more common in women, especially those who menstruate heavily. Low ferritin — your body's iron storage marker — is one of the most well-established triggers for telogen effluvium, and it's frequently missed because standard “normal range” lab values are set too low for hair health. Many dermatologists recommend a ferritin level above 40 ng/mL for optimal hair growth, even though labs may call anything above 12 “normal.”
The GLP‑1 demographic overlaps with perimenopause. Many women starting these medications are in their 40s and 50s — exactly when estrogen and progesterone levels are already declining. Those hormonal shifts independently affect hair cycling. Add rapid weight loss on top, and you've got overlapping triggers.
Women with PCOS — a common reason for seeking weight loss treatment — already have hormonal imbalances (elevated androgens, insulin resistance) that can affect hair. GLP‑1 treatment can actually improve these markers over time, but the initial rapid body changes can temporarily worsen shedding before things stabilize.
What to do if you're a woman experiencing GLP‑1 hair loss
Everything in the action plan below applies, but pay particular attention to getting your ferritin and thyroid levels checked. If your ferritin is below 40 ng/mL, correcting that alone can make a significant difference. And if you're in perimenopause, consider discussing your hormonal picture with your provider — hair loss may be a convergence of multiple factors, not just the GLP‑1.
Is GLP‑1 Hair Loss Permanent?
For the vast majority of people: no. Telogen effluvium is, by definition, a temporary disruption. Your hair follicles aren't damaged or destroyed — they're resting. Once the trigger resolves (weight stabilizes, nutrition improves, deficiencies are corrected), those follicles cycle back into active growth.
Most people see shedding slow within 3–6 months after their weight plateaus and full density recovery within 6–12 months — even if they continue taking the medication.
The important caveat we mentioned earlier: If GLP‑1-related weight loss unmasks or accelerates underlying androgenetic alopecia (pattern hair loss driven by genetics and DHT), that component won't fully self-resolve. Androgenetic alopecia is progressive without treatment. The good news is that effective treatments exist — topical minoxidil, oral medications, and other options your dermatologist can recommend.
How to tell if you're dealing with something beyond telogen effluvium:
- Your shedding has persisted more than 6 months after your weight stabilized
- The thinning follows a pattern (widening part, receding temples, thinning crown) rather than being diffuse
- Your hair grew back but looks finer or less dense in specific areas
In any of these scenarios, a dermatologist visit is worthwhile. A simple scalp examination — and sometimes a dermoscopy or blood work — can differentiate between conditions and get you on the right treatment path.
Is GLP‑1 Hair Loss DHT-Related?
This question comes up frequently in search, so let's address it directly.
If your shedding is diffuse (all over your scalp) and started 2–4 months after beginning a GLP‑1, it's most likely telogen effluvium — which is not DHT-driven. Telogen effluvium is a stress response, not a hormonal hair loss pattern.
However, DHT-related hair loss (androgenetic alopecia) can enter the picture in two ways:
First, rapid weight loss can unmask pre-existing androgenetic alopecia that was previously hidden. When you lose significant body weight, hormonal ratios shift, and pattern thinning that was subtle before may become more visible — especially once the diffuse shedding from telogen effluvium thins out your overall hair volume.
Second, some researchers have theorized that GLP‑1-mediated hormonal changes could influence androgen metabolism, potentially accelerating DHT-related thinning in genetically susceptible individuals. This hasn't been proven, but it's been hypothesized in the literature.
The practical takeaway
If your hair loss is diffuse and fits the telogen effluvium timeline, DHT isn't your primary concern — nutrition and weight loss management are. If your thinning is patterned (temples, crown, widening part) or persists long after shedding should have resolved, ask your dermatologist about androgenetic alopecia specifically. Treatments for DHT-related loss — minoxidil, finasteride (men), spironolactone (women) — are well-established and effective when started early.
How to Stop GLP‑1 Hair Loss: Your Step-by-Step Action Plan
If you're already shedding, here's what to do — in order of priority.
Educational checklist — not medical advice.
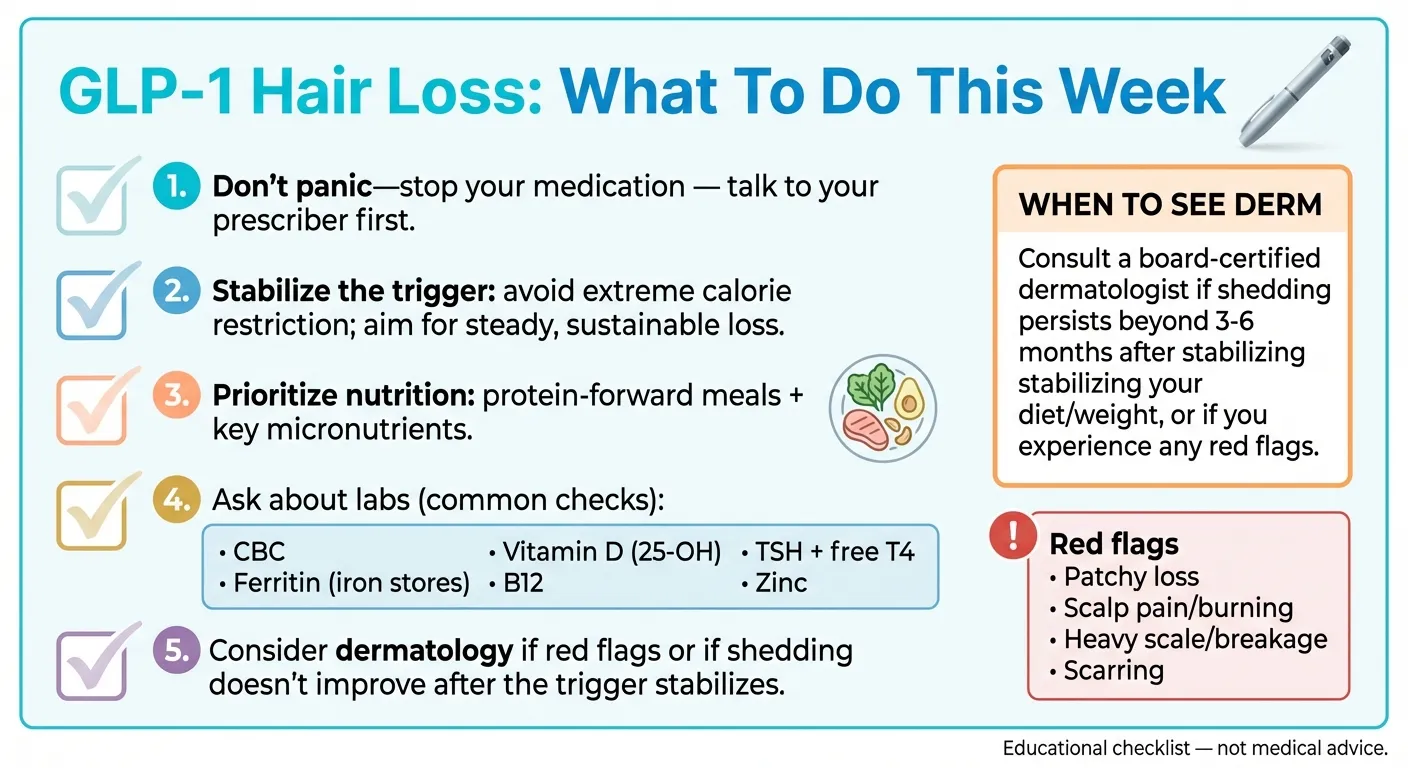
Step 1: Don't Panic-Stop Your Medication
We know this is counterintuitive when your hair is falling out, but here's why stopping abruptly usually isn't the answer:
- The hair shedding you're seeing now was triggered 2–3 months ago. Stopping the medication today won't stop the current shedding — those hairs are already in the pipeline.
- The metabolic and weight loss benefits of GLP‑1 treatment often outweigh temporary hair loss.
- Abruptly stopping can cause weight regain, which creates another body stress that can trigger another round of telogen effluvium.
Instead, talk to your prescriber. They may recommend slowing your titration, adjusting your dose, or focusing on nutritional support — all of which address the root triggers without abandoning treatment.
Step 2: Fix the Nutrition Bottleneck
This is the highest-leverage intervention. GLP‑1s suppress appetite, which means you're eating less — and “less” often means not enough of the specific nutrients your hair needs.
Protein: Aim for 70–100 grams per day. This is non-negotiable for hair health. Your hair is made of keratin, a protein. During caloric restriction, protein is the first thing your body redirects away from “optional” functions like hair growth. If you're struggling to eat enough due to appetite suppression, protein shakes, Greek yogurt, eggs, and lean meats are efficient ways to hit your target. Use our GLP‑1 Protein Calculator to find your daily target.
Key micronutrients to prioritize:
- Iron — Especially critical for women. Target ferritin >40 ng/mL (not just “within normal range”)
- Vitamin D — Target >30 ng/mL. Deficiency is extremely common and worsens shedding
- Zinc — 8–11 mg daily. Easy to become depleted when eating less
- Vitamin B12 — Especially important if you're also taking metformin
- Biotin — 2,500–5,000 mcg daily. One caution: biotin can interfere with certain lab tests (including thyroid panels), so tell your doctor you're taking it before any blood work
Don't crash diet on top of your GLP‑1. The medication already reduces your appetite significantly. Intentionally restricting below 1,200 calories per day compounds the metabolic stress and dramatically increases hair loss risk.
Step 3: Get the Right Blood Work
Don't supplement blindly — test first. Ask your provider for:
- CBC (complete blood count)
- Ferritin (iron stores — this is different from serum iron and more relevant for hair)
- Vitamin D (25-hydroxyvitamin D)
- Zinc
- Vitamin B12
- Thyroid panel (TSH, Free T4) — especially if you're experiencing fatigue, cold intolerance, or menstrual changes alongside hair loss
This blood work serves two purposes: it identifies correctable deficiencies that may be driving your shedding, and it rules out thyroid dysfunction or other medical conditions that can mimic telogen effluvium.
Step 4: Consider Evidence-Based Treatments
If nutrition optimization alone isn't enough, these are the treatments with the strongest evidence:
Topical minoxidil (Rogaine). Over-the-counter, available in 2% and 5% formulations. The most well-studied hair growth stimulant available without a prescription. Can be used during GLP‑1 treatment. Takes 3–6 months to show results.
Low-dose oral minoxidil. Prescription-only. Growing body of evidence for efficacy in multiple types of hair loss. Discuss with a dermatologist — they'll weigh the benefits against potential side effects for your specific situation.
Rosemary oil. Small studies have suggested it may be comparable to 2% minoxidil for certain types of hair loss. Low risk, low cost. Can be used as a prewash scalp massage to support circulation. Not a substitute for addressing nutritional deficiencies, but a reasonable add-on.
For pattern-type thinning specifically: Finasteride (men), spironolactone (women), and other prescription anti-androgens — all clinician-directed. These target DHT and are irrelevant for pure telogen effluvium.
Step 5: Know What Won't Help
Save your money and stress on these:
- Expensive “detox scrubs” — Can cause mechanical breakage and scalp inflammation, making things worse
- Random supplement stacks without blood work — You're guessing, and some supplements (like iron) can be harmful in excess
- Tight hairstyles, excessive heat styling, harsh chemical treatments — All add traction and damage stress to already-fragile hair
- Stopping your GLP‑1 abruptly — As explained above, this won't stop current shedding and may trigger new problems
Step 6: Track Progress Objectively
Your mirror is a terrible measurement tool. Instead:
- Take monthly progress photos: same lighting, same hair part, same angle
- Note daily shedding roughly (light/moderate/heavy) in a simple log
- Track weight loss rate alongside shedding — if you can see the correlation, you can manage it
How to Prevent GLP‑1 Hair Loss Before It Starts
If you haven't started a GLP‑1 yet — or you're early in treatment and haven't noticed shedding — you're in the best position to minimize risk.
The GLP‑1 Hair Loss Prevention Checklist
Get baseline blood work before starting. Ferritin, vitamin D, B12, zinc, thyroid panel, CBC. Correcting deficiencies before you start is far easier than catching up later.
Set a protein target from day one. 70–100 grams daily. Plan for this before appetite suppression kicks in. Have protein-dense foods and shakes ready to go.
Discuss titration pace with your provider. The goal is gradual dose escalation — losing 1–2 pounds per week is generally better tolerated than faster rates. The evidence is clear: more rapid weight loss = higher hair loss risk.
Take baseline photos. Same lighting, same hair part. If shedding happens later, you'll have an objective comparison point instead of relying on memory and anxiety.
Plan for nausea. Nausea is the most common GLP‑1 side effect, and it directly impacts your ability to eat. Have a plan: smaller frequent meals, ginger, anti-nausea strategies from your provider. If you can't eat, you can't get the nutrients your hair needs.
Don't stack calorie restriction on top of the medication. Let the GLP‑1 do its job. Aggressive dieting on top of appetite suppression creates the exact metabolic stress environment that maximizes telogen effluvium risk.
Supplement any confirmed deficiencies immediately. Don't wait for symptoms.
The Supplement Decision Grid: What's Actually Worth Taking
Supplements are helpful when they correct a real deficiency. Otherwise, evidence is mixed and costs add up fast. Here's how to think about it.
| Supplement | Helpful If… | How to Verify | Risk of Overdoing It | Notes |
|---|---|---|---|---|
| Iron | Ferritin <40 ng/mL | Blood test (ferritin, not just serum iron) | Yes — excess iron is toxic; never supplement without testing | Most important for menstruating women |
| Vitamin D3 | Level <30 ng/mL | Blood test (25-hydroxyvitamin D) | Low risk at 1,000–2,000 IU/day; high doses need monitoring | Extremely common deficiency |
| Zinc | Deficient or borderline on blood work, or eating very little | Blood test (serum zinc) | Can cause copper depletion at high doses | Supplement only if deficiency is confirmed |
| B12 | Low on blood work, or taking metformin | Blood test | Very low risk (water-soluble) | Sublingual or injection if absorption is an issue |
| Biotin | Rarely actually deficient; may support keratin production | Blood test (rarely done, deficiency is uncommon) | Low risk, but interferes with some lab tests — tell your doctor | Popular but overhyped; nutrition matters more |
| Protein powder | You can't hit 70–100g protein through food alone | Track daily intake for 3 days | Very low risk | Whey, pea, or collagen — preference matters less than total grams |
Our honest take: If you're going to spend money, spend it on a comprehensive blood panel first. A $200 lab workup will tell you exactly what you need far more reliably than a $60/month supplement subscription based on marketing.
Can GLP‑1s Actually Help Hair Growth?
This might seem contradictory after everything above, but the science is more nuanced than “GLP‑1s cause hair loss.”
One proposed mechanism in published reviews is that GLP‑1 receptors are expressed around hair follicles and may influence growth pathways (e.g., MAPK/ERK signaling), though this is still early-stage research and not a basis to expect hair regrowth from GLP‑1 treatment alone.
In 2024, a published case study documented a 57-year-old man with male-pattern baldness who experienced notable improvement in hair density after one year of tirzepatide treatment. His insulin resistance improved, his metabolic health normalized, and his hair visibly thickened. A few small studies on tirzepatide have also reported hair improvement in some patients with pre-existing androgenetic alopecia.
The mechanism makes some biological sense: improved insulin sensitivity, reduced systemic inflammation, better hormonal balance, and increased scalp blood flow could all create a more favorable environment for hair growth over time.
The catch: These are case studies and small samples. We can't generalize from them. But they're worth mentioning because they add context — the relationship between GLP‑1s and hair isn't simply “medication = hair loss.” For some people, the long-term metabolic improvements may actually benefit their hair once the initial weight-loss stress resolves.
This is another reason not to panic-stop a medication that's working for you.
Compounded Semaglutide and Hair Loss: Is the Risk Different?
The hair loss risk appears driven mostly by the amount and speed of weight loss and nutritional status — not the brand name. But compounded GLP‑1 products can vary: FDA has warned that some compounded products use semaglutide salt forms (e.g., semaglutide sodium or semaglutide acetate), which are different active ingredients than the base form used in approved semaglutide drugs, and has also alerted providers about dosing errors associated with compounded semaglutide and tirzepatide.
That said, compounded medications aren't FDA-approved, and they don't undergo the same quality and consistency verification as brand-name products. That introduces a separate set of concerns — not specifically about hair loss, but about overall safety and dosing accuracy. Read our compounded semaglutide safety guide for more.
If you're using compounded semaglutide or tirzepatide:
- Make sure you have a legitimate prescription from a licensed provider
- Verify the pharmacy is state-licensed (ideally PCAB-accredited)
- Confirm dosing is transparent and consistent
- Maintain the same nutritional and monitoring protocols as brand-name users
- Be cautious of pricing that seems too cheap to be legitimate
The hair loss prevention and management strategies in this guide apply equally regardless of whether you're on brand-name or compounded formulations.
What to Ask Your Doctor About GLP‑1 Hair Loss
Most people get better outcomes when they bring specific information to their appointment instead of a general “I'm losing hair.” Here's a script you can adapt:
Copy/paste for your next appointment:
“I started [medication name] on [date] at [dose]. My current dose is [dose]. I've lost approximately [X pounds / X%] since starting. I first noticed increased hair shedding around [date/month]. The shedding is [diffuse/patchy/patterned — describe what you see]. I [am/am not] experiencing other symptoms like fatigue, cold intolerance, or menstrual changes.
I'd like to discuss:
- Could this be telogen effluvium from the weight loss?
- Can we check my ferritin, vitamin D, B12, zinc, and thyroid?
- Should we adjust my titration pace or current dose?
- At what point should I see a dermatologist?
- Are there nutritional targets I should be hitting?”
Bringing this level of specificity helps your provider help you faster. Instead of a vague conversation about hair loss, you're giving them the clinical context to make informed recommendations.
Choosing a GLP‑1 Provider That Actually Monitors for This
One thing we've learned researching GLP‑1 providers: not all of them are equal when it comes to managing side effects like hair loss.
Some telehealth platforms are essentially prescription mills — you answer a questionnaire, get a script, and never hear from a clinician again unless you initiate contact. Others provide comprehensive care: baseline labs, nutritional guidance, dose titration based on your response, and ongoing clinician access.
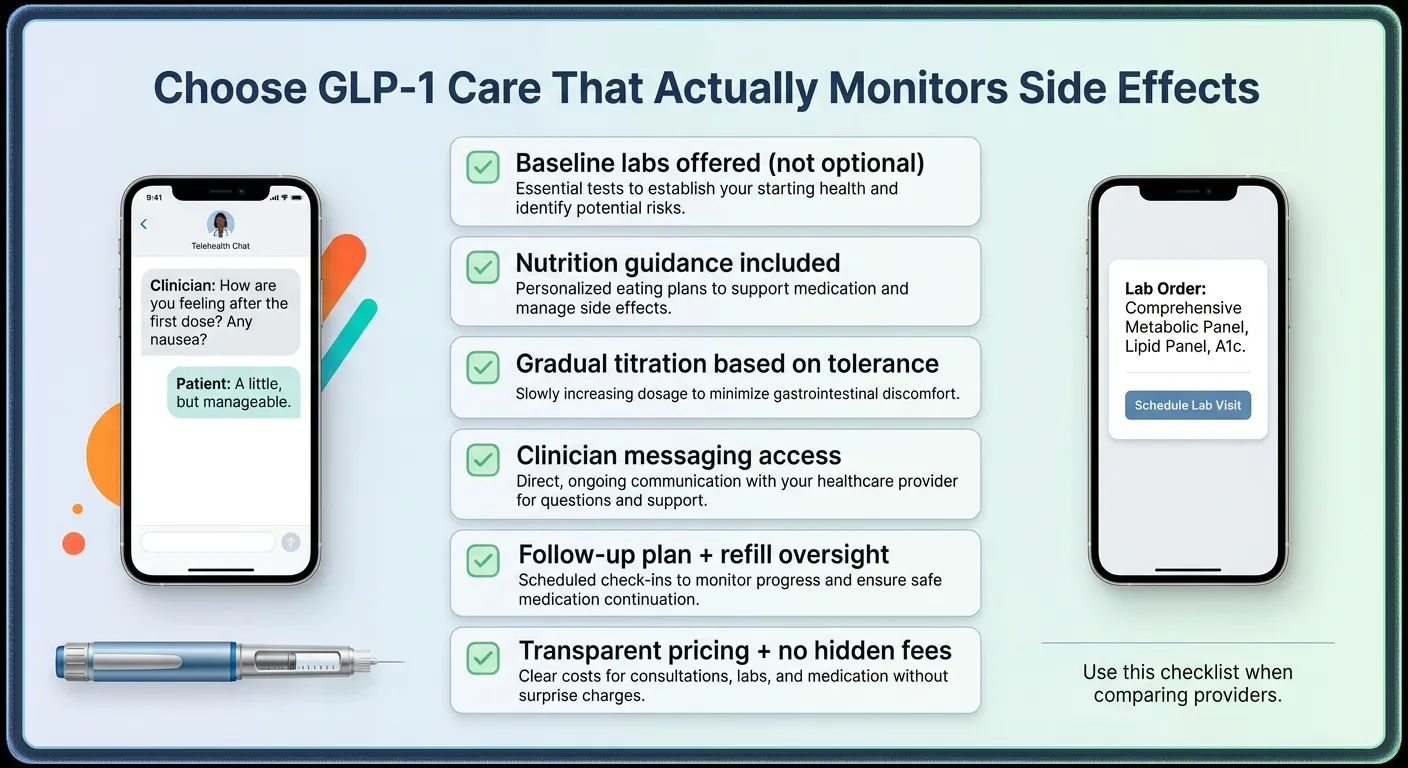
Use this checklist when comparing providers.
| Feature | Why It Matters for Hair Loss |
|---|---|
| Orders baseline blood work | Catches ferritin, vitamin D, thyroid issues before they cause shedding |
| Provides nutritional guidance | Helps you hit protein and micronutrient targets despite reduced appetite |
| Offers gradual dose titration | Slower weight loss = lower hair loss risk |
| Has clinician messaging access | You can raise hair loss concerns without waiting weeks for an appointment |
| Monitors ongoing labs | Catches developing deficiencies before they become problems |
| Transparent pricing | No hidden costs for labs or follow-ups |
The best way to minimize GLP‑1 side effects — hair loss included — is to work with a provider that treats this as a managed medical process, not just a prescription transaction.
We compared 15+ GLP‑1 telehealth providers on clinical support, pricing, lab monitoring, and more. If you're looking for a provider — or considering switching — our full comparison can help you find the right fit.
Frequently Asked Questions: GLP‑1 Hair Loss
Does GLP-1 cause hair loss?
Hair loss is a recognized side effect in the FDA labels for Wegovy (3% of adults in trials) and Zepbound (4–5%). Most evidence points to rapid weight loss as the primary trigger rather than the drug molecule directly, though research is still evolving.
Is GLP-1 hair loss permanent?
In most cases, no. Telogen effluvium — the most common type associated with GLP-1s — is temporary and typically resolves within 6–12 months once weight stabilizes. If patterned thinning persists, see a dermatologist to rule out androgenetic alopecia.
When does GLP-1 hair loss start?
Most people notice increased shedding 2–4 months after starting treatment or after a dose increase. This aligns with the telogen effluvium timeline — there's a built-in lag between the stress trigger and visible shedding.
How long does GLP-1 hair loss last?
Peak shedding typically occurs between months 4–6. Most people see significant improvement by months 6–9 and full recovery within 9–12 months, assuming weight has stabilized and nutritional deficiencies have been addressed.
Should I stop my GLP-1 if I'm losing hair?
Medical experts generally don't recommend stopping GLP-1 medications solely because of hair loss. The shedding won't stop immediately (it was triggered months ago), and abrupt discontinuation can cause weight regain — which may trigger another round of telogen effluvium. Talk to your provider about dose adjustment instead.
How common is Wegovy hair loss?
In clinical trials, 3% of adult Wegovy users reported hair loss, compared to 1% on placebo. Canada's product monograph further noted that among those who lost more than 20% of their body weight, the rate was 5.3%.
How common is Zepbound hair loss?
Zepbound's FDA label lists hair loss as a common adverse reaction (≥5%), with rates of 4–5% across doses versus approximately 1% on placebo. It was reported more frequently in women.
Does Ozempic cause hair loss?
Hair loss isn't listed in Ozempic's clinical trial data, but it appears in the postmarketing section of the label. Ozempic contains the same active ingredient (semaglutide) as Wegovy at a lower maximum dose, so the risk likely exists but at lower rates due to less aggressive weight loss.
Is GLP-1 hair loss related to DHT?
Usually not directly. Diffuse shedding from GLP-1s is most often telogen effluvium (stress-related), not DHT-driven. However, rapid weight loss can unmask underlying androgenetic alopecia, which is DHT-related, in genetically predisposed individuals.
What's the best supplement for GLP-1 hair loss?
There's no single "best" supplement. The most effective approach is testing for deficiencies first (ferritin, vitamin D, zinc, B12) and supplementing based on results. Protein intake (70–100g daily) is more impactful than any individual supplement.
Can minoxidil help with GLP-1 hair shedding?
Yes — topical minoxidil (2% or 5%) is clinically proven to stimulate hair growth and can be used alongside GLP-1 treatment. It takes 3–6 months to show results. Low-dose oral minoxidil is another option to discuss with a dermatologist.
What labs should I ask for if I'm losing hair on a GLP-1?
Request: ferritin (iron stores), vitamin D, zinc, B12, thyroid panel (TSH, Free T4), and a CBC. Ferritin is especially important — aim for >40 ng/mL, not just "within normal range."
How much hair shedding is "normal" versus concerning?
Losing 50–100 hairs per day is normal. During telogen effluvium, this can increase to 200–300+ hairs per day. If shedding is so heavy that you're developing visible bald patches (not just overall thinning), see a dermatologist.
Will switching from one GLP-1 to another stop the hair loss?
Probably not, since the hair loss is primarily driven by weight loss and nutritional status, not the specific drug. Switching to a medication that produces slower weight loss might reduce future risk, but won't stop shedding already in progress.
Does rosemary oil work for GLP-1 hair loss?
Small studies suggest rosemary oil may support scalp health and circulation, with one study finding it comparable to 2% minoxidil for androgenetic alopecia. It's low risk and inexpensive — reasonable as a complementary approach, but not a substitute for addressing nutritional deficiencies.
When should I see a dermatologist?
See a dermatologist if: shedding persists more than 6 months after your weight has stabilized, you notice patchy (not diffuse) hair loss, your scalp shows redness or scaling, you're experiencing symptoms like extreme fatigue or cold intolerance, or the thinning follows a distinct pattern.
How much protein do I need to prevent GLP-1 hair loss?
Aim for 70–100 grams of protein daily, or roughly 1.0–1.2 grams per kilogram of body weight. This is the single most impactful nutritional intervention for reducing telogen effluvium risk.
Can I prevent hair loss before starting a GLP-1?
Yes. Get baseline blood work, correct any deficiencies, start a high-protein diet, discuss gradual dose titration with your provider, and plan for nausea management so you can maintain adequate nutrition once appetite suppression kicks in.
Does the GLP-1 dose affect hair loss risk?
Yes. Higher doses produce more rapid weight loss, which increases telogen effluvium risk. Canada's Wegovy product monograph noted roughly double the hair loss rate in patients who lost >20% of their body weight versus those who lost less.
How long until my hair grows back?
After shedding slows, visible improvement typically begins within 3–6 months. Full density recovery can take 6–12 months. Hair grows approximately half an inch per month, so patience is essential.
How We Researched This Guide
We built this resource by reviewing FDA prescribing information for the major GLP‑1 medications most commonly associated with weight-loss hair loss (Wegovy, Ozempic, Zepbound, Mounjaro, Saxenda), published clinical trial data (including the STEP and SURMOUNT trials), peer-reviewed systematic reviews and observational studies, and reporting from established medical outlets.
What we cite: FDA label data for clinical trial adverse reaction rates. Published studies from the New England Journal of Medicine, Journal of the American Academy of Dermatology, Cureus, and medRxiv. Dermatology references on telogen effluvium from the Cleveland Clinic. FAERS database analyses.
What we explicitly separate: We distinguish between FDA clinical trial data (strongest evidence for frequency), postmarketing reports (signal, not proof of causation or rate), observational studies (important but have limitations), and anecdotal reports (real experiences, but not reliable for frequency estimates).
What we're not: We're not doctors. We didn't conduct original clinical research. We compiled, verified, and synthesized publicly available medical data to help you make informed decisions with your healthcare provider. Read our editorial standards for more details.
Conflict of interest disclosure: We earn affiliate commissions from GLP‑1 provider signups. This doesn't influence our research. We cite the same FDA data and clinical evidence whether or not you click our links. If you stripped every affiliate link from this page, the information would be identical.
Sources
These are the sources we cite throughout this guide. Every clinical claim traces back to one of these:
- Wegovy (semaglutide) Prescribing Information. U.S. Food and Drug Administration. Revised August 2025. FDA Access Data
- Zepbound (tirzepatide) Prescribing Information. U.S. Food and Drug Administration. Revised March 2024. FDA Access Data
- Ozempic (semaglutide) Prescribing Information. U.S. Food and Drug Administration. Revised 2025. FDA Access Data
- Mounjaro (tirzepatide) Prescribing Information. U.S. Food and Drug Administration. Revised 2025. FDA Access Data
- Saxenda (liraglutide) Prescribing Information. U.S. Food and Drug Administration. Revised May 2025. FDA Access Data
- Wegovy (semaglutide) Product Monograph. Health Canada. HRES PDF
- Jastreboff AM, et al. “Tirzepatide Once Weekly for the Treatment of Obesity.” New England Journal of Medicine. 2022;387(3):205-216. (SURMOUNT-1 trial)
- Etminan M, et al. “Risk of Hair Loss with Semaglutide for Weight Loss.” medRxiv. 2025.
- Vidal SI, et al. “Risk for Nonscarring Hair Loss Increased in Association With GLP‑1 Receptor Agonist Use.” Journal of the American Academy of Dermatology. Published online February 9, 2026.
- “Hair Loss Associated With GLP‑1 Receptor Agonist Use: A Systematic Review.” Cureus. PMC. 2025. PMC
- “Alopecia as an Emerging Adverse Effect Associated With GLP‑1 Receptor Agonists for Weight Loss: A Scoping Review.” Cureus. August 2025.
- Hughes EC, et al. “Telogen Effluvium.” StatPearls. May 2024.
- Godfrey et al. FAERS disproportionality analysis — semaglutide and tirzepatide alopecia signal. APC Journals
- Malkud S. “Telogen Effluvium: A Review.” Journal of Clinical and Diagnostic Research. 2015;9(9):WE01-WE03.
- “Telogen Effluvium.” Cleveland Clinic. clevelandclinic.org
- Panahi Y, et al. “Rosemary oil vs minoxidil 2% for the treatment of androgenetic alopecia: a randomized comparative trial.” Skinmed. 2015;13(1):15-21. PubMed
- Tirzepatide and hair regrowth case report. PMC. 2024. PMC
- Telogen effluvium after bariatric surgery. Obesity Surgery. 2021. PubMed
- FDA. “FDA's Concerns with Unapproved GLP-1 Drugs Used for Weight Loss.” FDA.gov
- FDA. “FDA alerts health care providers, compounders and patients of dosing errors associated with compounded injectable semaglutide products.” FDA.gov
Related Guides
- Cons of GLP-1: Side Effects, Risks & Downsides
- GLP-1 and PCOS: Complete Evidence-Based Guide
- Best GLP-1 for Perimenopause
- How to Prevent Muscle Loss on GLP-1 Medications
- GLP-1 Protein Calculator: Find Your Daily Target
- GLP-1 Plateau: Why It's Not Working Anymore + Fix Plan
- How to Take GLP-1 Safely: Complete Guide
- Best GLP-1 Telehealth Providers (2026)
- What Happens When You Stop Taking GLP-1