How to Prevent Muscle Loss on GLP-1 Medications
The complete, evidence-based guide to preserving muscle while losing weight on Ozempic, Wegovy, Mounjaro, and Zepbound—with specific protein targets, workout plans, and pacing strategies.
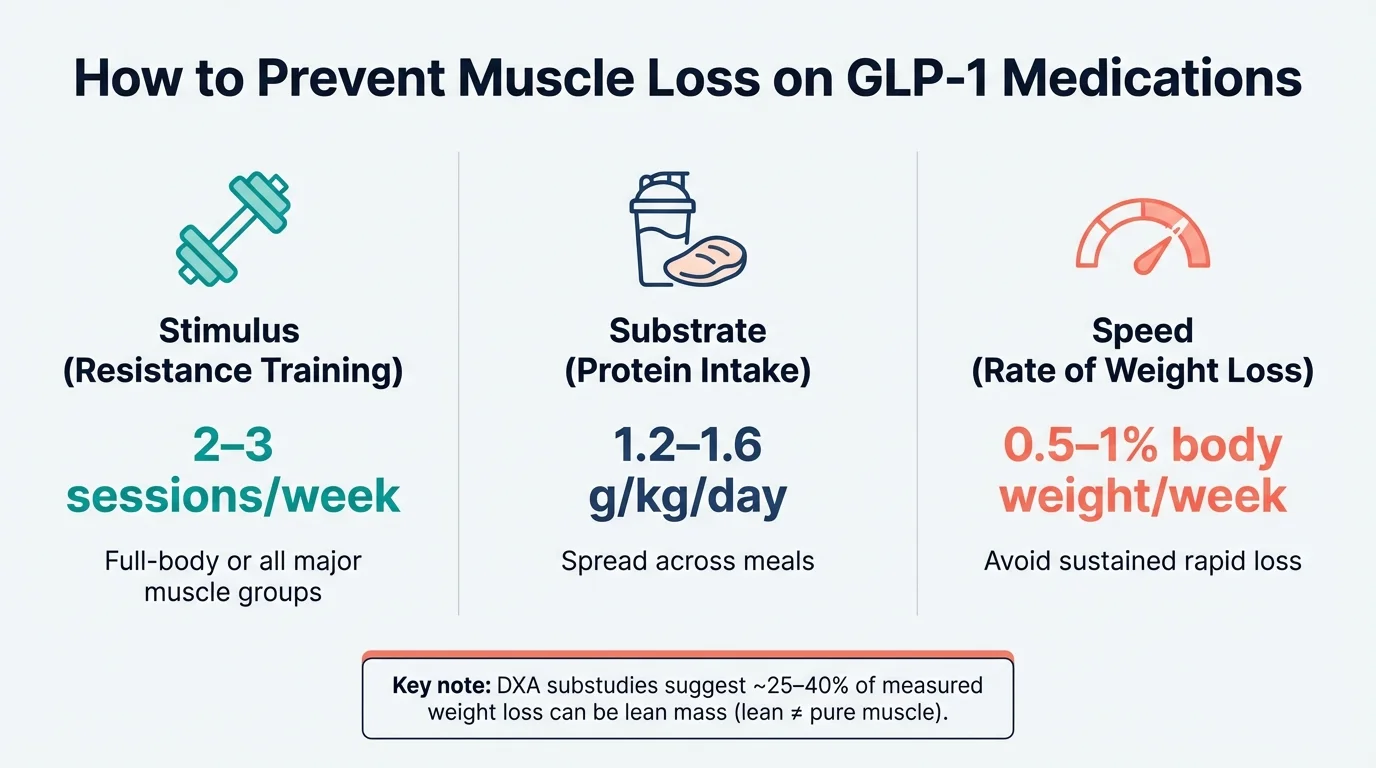
Quick answer: Prevent GLP-1 (also written GLP 1) muscle loss with three strategies: eat 1.2–1.6g protein per kg body weight daily, strength train 2–3x weekly, and limit weight loss to 0.5–1% per week. Evidence suggests proper protein intake and resistance training can substantially reduce the proportion of lean mass lost during weight loss.
Disclosure: Some links on this site are affiliate links. If you purchase through these links, we may earn a commission at no extra cost to you. Thank you for supporting our site.·For informational purposes only—not medical advice.
Preventing muscle loss on GLP-1 medications comes down to three things: eat enough protein (1.2–1.6 grams per kilogram of body weight daily), do resistance training at least twice a week, and don't lose weight too fast. In DXA substudies of GLP-1 weight-loss trials, a meaningful portion of measured weight loss can come from lean mass (which includes more than just muscle). Research suggests you can reduce lean mass loss and preserve strength with adequate protein and resistance training, though results vary by age, starting muscle mass, and rate of loss.
This guide gives you the exact targets, a complete workout plan, troubleshooting for when appetite is low, and a way to track your progress. Everything is backed by peer-reviewed research and clinical guidelines.
| The 3 Levers That Protect Muscle | Your Target |
|---|---|
| Stimulus (Resistance Training) | 2–3 sessions per week, all major muscle groups |
| Substrate (Protein Intake) | 1.2–1.6 g per kg body weight, spread across meals |
| Speed (Rate of Weight Loss) | 0.5–1% of body weight per week (roughly 1–2 lbs for most people) |
Get these three right, and you'll lose mostly fat while keeping the muscle that supports your metabolism, strength, and long-term health.
Table of Contents
The 7-Day Quick Start Plan
If you're just starting a GLP-1 medication—or realizing you need a plan—here's what to do this week. This is your minimum viable protocol for protecting muscle while losing fat.
Day 1–7 Checklist
- Eat at least 100g of protein (more if you weigh over 180 lbs)
- Spread protein across 3–4 meals (25–35g each)
- Drink at least 64 oz of water
- Walk 7,000+ steps
- Complete a 30–45 minute full-body strength workout (see the plan below)
- Switch to smaller, more frequent meals
- Use protein shakes or Greek yogurt as your protein source
- Eat protein first before anything else on your plate
For more strategies, see our GLP-1 nausea relief guide.
- Calculate your personal protein target using our GLP-1 Protein Calculator
- Schedule your strength training days for the coming weeks
- Take baseline measurements (weight, waist circumference, a few key lifts)
This isn't complicated. The challenge is doing it consistently, especially when the medication suppresses your appetite. The rest of this guide explains why each piece matters and how to dial it in.
Do GLP-1 Medications Actually Cause Muscle Loss?
Here's the honest answer: GLP-1 medications don't directly attack your muscles. What they do is create a calorie deficit by reducing your appetite. And any significant calorie deficit—whether from dieting, surgery, or medication—causes some lean mass loss along with fat loss. This isn't unique to Ozempic or Mounjaro.
But the numbers you may have seen—"40% of weight loss is muscle!"—need context.
What the Clinical Trials Actually Show
| Trial (DXA Substudy) | Medication | What Changed | What It Suggests |
|---|---|---|---|
| STEP-1 | Semaglutide 2.4mg (Wegovy) | Fat mass −8.36 kg; lean body mass −5.26 kg | Roughly ~60% fat / ~40% lean in DXA compartments (lean ≠ pure muscle) |
| SURMOUNT-1 | Tirzepatide (Zepbound) | ~75% fat mass / 25% lean mass contribution to weight loss | Proportionally less lean mass loss vs STEP-1 DXA results |
| Bariatric surgery (average) | N/A | Variable | 25–30% from lean mass |
| Diet-only studies (average) | N/A | 8–10 kg total | 25–30% from lean mass |
DXA values shown are from STEP-1 Supplementary Appendix Table S5 subpopulation analysis.
Sources: STEP-1 Supplementary Appendix (Table S5), SURMOUNT-1 DXA substudy (Look et al., 2025; PMID: 39996356)
The "Lean Mass" Confusion
Here's something most articles get wrong: lean mass is not the same as muscle.
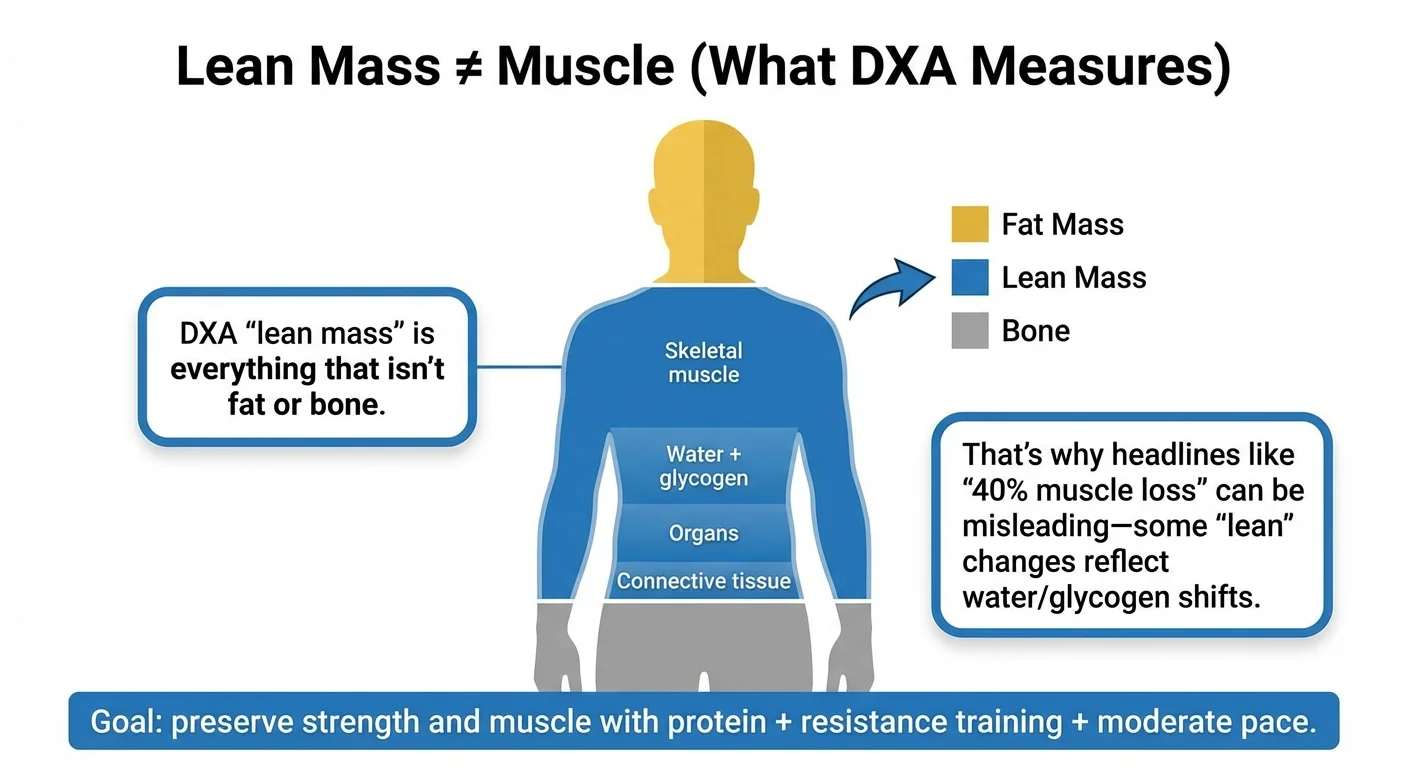
When researchers measure "lean mass" using DEXA scans, they're measuring everything that isn't fat or bone. That includes:
- Skeletal muscle (what you want to keep)
- Water and glycogen stored in tissues
- Organs
- Connective tissue
When you lose weight quickly, you also lose glycogen and the water stored with it, along with other short-term body-water shifts. This can show up as "lean mass" change on DXA even when true muscle tissue loss is smaller.
Because DXA "lean mass" includes more than skeletal muscle, DXA-reported lean mass changes should not be interpreted as pure muscle change. This doesn't mean muscle loss isn't happening—it is—but the headline "40% muscle loss" overstates the reality for most people.
What This Means for You
Yes, you'll lose some muscle during weight loss. This happens with any effective weight loss method. The question is: how much, and can you minimize it?
The answer to the second question is yes. Research suggests lean mass loss can be meaningfully reduced when people combine higher protein intake with resistance training during weight loss. The exact proportion varies person to person based on factors like age, starting muscle mass, training history, and adherence.
The bottom line: The difference between losing excessive lean mass and preserving most of it is the difference between feeling weak and depleted versus feeling strong and healthy at your new weight. That's what this guide helps you achieve.
Why Muscle Loss Happens (And What You Control)
Understanding the mechanism helps you target the right interventions. Muscle loss during GLP-1 therapy happens for specific, addressable reasons.
Reason 1: You're Not Eating Enough Protein
GLP-1 medications work by suppressing appetite. You feel full faster and think about food less. This is great for creating a calorie deficit, but it creates a problem: when you eat less overall, you often eat less protein too.
Your body needs protein to maintain muscle. Specifically, it needs amino acids from protein to run a process called muscle protein synthesis—the constant rebuilding of muscle tissue. When protein intake drops, muscle protein breakdown starts exceeding synthesis, and you lose muscle mass. This is the most common and most fixable cause of excessive muscle loss on GLP-1s.
Reason 2: No Resistance Training Stimulus
Your body is efficient. It won't maintain tissue that requires energy to sustain unless it has a reason to. Maintaining muscle supports strength, function, and helps preserve resting energy expenditure during weight loss. That reason to keep muscle is resistance training.
When you lift weights or do resistance exercises, you signal to your body: "I need this muscle. Keep it." Without that signal, your body sees muscle as excess tissue it can sacrifice during a calorie deficit. Many people on GLP-1 medications skip strength training, either because they don't know it matters or because they feel too tired. This is a mistake. Even two 30-minute sessions per week makes a significant difference.
Reason 3: Losing Weight Too Fast
Faster weight loss means more lean mass loss. This is consistent across all weight loss methods.
When you lose weight very quickly, your body can't adapt fast enough. It pulls energy from both fat stores and muscle tissue. Slower, more controlled loss gives your body time to preferentially burn fat while preserving muscle—especially if you're supporting it with protein and training. GLP-1 medications can cause rapid weight loss, particularly in the first few months or when doses increase. This is partly why the "muscle loss" concern is louder with these medications than with traditional dieting.
Reason 4: Side Effects That Reduce Intake
Nausea, early satiety, and digestive issues are common with GLP-1 medications, especially early on. These side effects can make it nearly impossible to eat enough, let alone hit protein targets. If you're barely eating due to nausea, muscle preservation becomes much harder. This is why the section on eating strategies when appetite is low matters. For immediate help, see our GLP-1 SOS side effect relief tool.
Reason 5: Higher Risk Factors
Some people face higher muscle loss risk:
| Risk Factor | Why It Matters |
|---|---|
| Age over 50 | Natural muscle loss (sarcopenia) is already occurring |
| Low starting muscle mass | Less buffer to lose |
| Sedentary lifestyle | No training stimulus |
| Very rapid weight loss | Higher lean mass percentage lost |
| Very low protein intake | Insufficient substrate for muscle maintenance |
| History of yo-yo dieting | May have reduced muscle from previous cycles |
If multiple risk factors apply to you, being more aggressive with protein and training is even more important.
How Much Protein You Need on GLP-1
This is the section that actually matters. Generic advice says "eat more protein." Here are the specific numbers. For personalized calculations, use our GLP-1 Protein Calculator.
Your Daily Protein Target
The standard recommendation for healthy adults is 0.8 grams of protein per kilogram of body weight. That's enough to prevent deficiency in someone who isn't losing weight or exercising intensely. It is not enough for someone in a calorie deficit trying to preserve muscle.
For GLP-1 users, the research-supported range is:
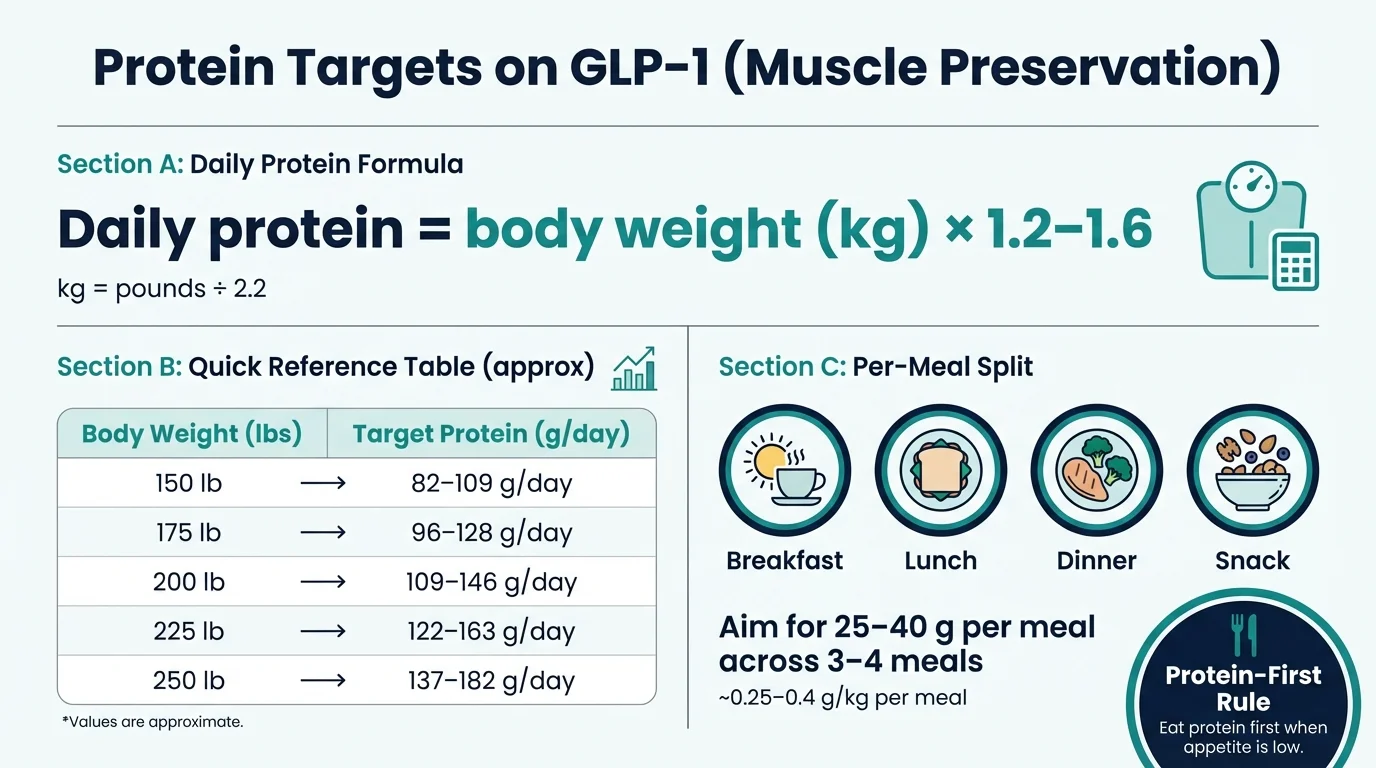
1.2–1.6 grams of protein per kilogram of body weight per day
Some experts recommend up to 2.0 g/kg for highly active individuals or those losing weight rapidly.
How to Calculate Your Target
Step 1: Convert your weight to kilograms (divide pounds by 2.2)
Step 2: Multiply by 1.2 (minimum) and 1.6 (optimal)
- 180 ÷ 2.2 = 82 kg
- Minimum: 82 × 1.2 = 98 grams per day
- Optimal: 82 × 1.6 = 131 grams per day
Quick Reference Table
| Your Weight | Minimum Protein | Optimal Protein |
|---|---|---|
| 150 lbs (68 kg) | 82g | 109g |
| 175 lbs (80 kg) | 96g | 128g |
| 200 lbs (91 kg) | 109g | 146g |
| 225 lbs (102 kg) | 122g | 163g |
| 250 lbs (114 kg) | 137g | 182g |
If you're significantly overweight, you can calculate based on your goal body weight or an "adjusted" weight (roughly halfway between current and goal). A 300-pound person doesn't necessarily need 200+ grams of protein—using goal weight makes targets more realistic.
Why Distribution Matters
For muscle support, many researchers recommend distributing protein across meals rather than saving it all for one sitting. The muscle protein synthesis response to a meal appears to plateau, so a common evidence-based target is roughly 0.25–0.4 g/kg per meal (often ~25–40g for many adults), depending on body size and age. This aligns with the ISSN position stand on protein and exercise.
This means eating 120 grams of protein in one sitting may not be as effective for muscle support as spreading it across meals.
Aim for 25–40 grams of protein per meal, across 3–4 meals per day.
Sample Meal Distribution
| Meal | Protein Target | Example |
|---|---|---|
| Breakfast | 30g | 3 eggs (18g) + Greek yogurt (15g) |
| Lunch | 35g | 5 oz chicken breast (35g) |
| Dinner | 35g | 6 oz salmon (34g) |
| Snack | 20g | Protein shake (20–25g) |
| Total | 120g |
The Best Protein Sources (High-Protein, Low-Volume Options)
When your appetite is suppressed, you want maximum protein per bite. These are ranked by protein density—protein content relative to volume—making them easier to eat on GLP-1. (Protein varies by brand and serving; check labels.)
- • Whey/plant protein shake: ~20–30g
- • Chicken breast (4–5 oz): ~30–40g
- • White fish (4–5 oz): ~25–35g
- • Shrimp (4–5 oz): ~25–30g
- • Egg whites (½ cup): ~12–15g
- • Greek yogurt (1 cup): ~15–25g
- • Cottage cheese (1 cup): ~20–25g
- • Lean beef, 93% (4 oz): ~25–30g
- • Turkey breast (4 oz): ~25–30g
- • Tofu, firm (½ cup): ~10–15g
- • Eggs, whole (2 large): ~12g
- • Salmon (4 oz): ~25g
- • Lentils (1 cup cooked): ~18g
- • Black beans (1 cup): ~15g
- • Edamame (1 cup): ~17g
- • Peanut butter: Only ~8g per 2 tbsp (mostly fat)
- • Almonds: Only ~6g per oz (mostly fat)
- • Cheese: Varies, but often ~7g per oz with significant fat
- • Protein bars: Many have more sugar than protein—check labels
The "Protein First" Rule
When appetite is suppressed, a simple rule changes everything: eat your protein first.
Before you take a bite of rice, vegetables, or bread, eat your protein source. If you can only eat half your meal before feeling full, at least you got the protein in. This single habit is the difference between hitting your target and falling short.
Protein Timing Around Workouts
If you're strength training (and you should be), there's a window where protein intake is especially effective:
- Before workout: Having protein within a few hours before training can help, but isn't critical
- After workout: Consuming 25–40g of protein within 2 hours after training optimizes muscle protein synthesis
Don't overthink timing. Total daily protein matters more than precise timing. But if you're optimizing, a protein-rich meal or shake after training is beneficial.
When Protein Supplements Make Sense
Whole foods are ideal, but supplements have their place:
Use protein powder when:
- You can't stomach solid food due to nausea
- You're consistently missing your protein target
- You need a quick option when whole food isn't available
- You're hitting your calorie limit but not your protein target
Best options:
- Whey protein isolate (fast-absorbing, complete amino acid profile)
- Casein protein (slower release, good before bed)
- Pea + rice protein blend (for dairy-free needs)
A single 20–30g protein shake can easily close the gap on days you're struggling.
The Strength Training Plan
Protein gives your body the raw materials. Strength training tells your body what to do with them. Without the training stimulus, even perfect nutrition won't fully prevent muscle loss.
Why Resistance Training Is Non-Negotiable
When you're in a calorie deficit, your body looks for energy sources to tap. Muscle tissue is metabolically expensive—your body would happily sacrifice it if nothing signals that it's needed.
Resistance training creates that signal. When you challenge your muscles against resistance, you trigger a cascade of molecular signals that tell your body: "Preserve and rebuild this tissue." Without that signal, muscle is fair game for your body's energy-saving adaptations.
This is why cardio alone doesn't protect muscle. Running, cycling, and swimming are great for cardiovascular health, but they don't send the same preservation signal that lifting weights does. In fact, excessive cardio in a calorie deficit can accelerate muscle loss.
The Minimum Effective Dose
You don't need to live in the gym. Research shows significant muscle preservation benefits from just two full-body resistance sessions per week, with each session lasting 30–45 minutes. More is fine if you enjoy it and can recover, but two sessions is the floor. Below that, you're leaving muscle protection on the table.
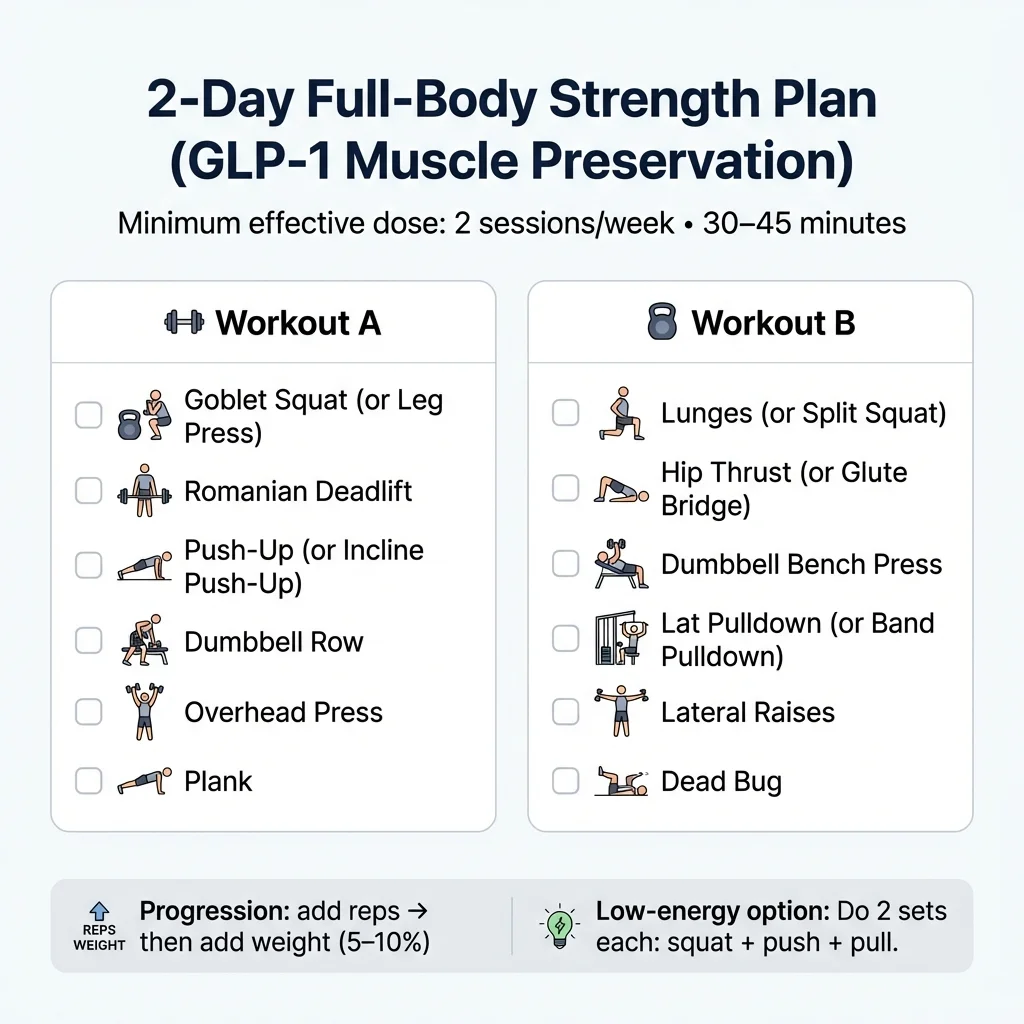
The 4-Week Beginner Program
This program works whether you have a gym or just a set of dumbbells at home. It hits all major muscle groups twice per week with compound movements that give you the most benefit per exercise.
Schedule:
- Option A (2x/week): Monday (Workout A) + Thursday (Workout B)
- Option B (3x/week): Monday (A), Wednesday (B), Friday (A) — alternate the next week
| Exercise | Sets | Reps | Rest | Notes |
|---|---|---|---|---|
| Goblet Squat (or Leg Press) | 3 | 10–12 | 90 sec | Keep chest up, go as deep as comfortable |
| Romanian Deadlift | 3 | 10–12 | 90 sec | Slight knee bend, hinge at hips |
| Push-Up (or Incline Push-Up) | 3 | 8–12 | 60 sec | Modify angle to match your strength |
| Dumbbell Row | 3 | 10–12 each | 60 sec | Pull elbow to hip, squeeze at top |
| Overhead Press | 3 | 8–10 | 60 sec | Standing or seated |
| Plank | 3 | 30–45 sec | 45 sec | Keep body straight, don't sag |
| Exercise | Sets | Reps | Rest | Notes |
|---|---|---|---|---|
| Lunges (or Split Squat) | 3 | 10–12 each | 90 sec | Step forward or stationary |
| Hip Thrust (or Glute Bridge) | 3 | 12–15 | 60 sec | Squeeze glutes at top |
| Dumbbell Bench Press | 3 | 8–10 | 90 sec | Lower to chest, press up |
| Lat Pulldown (or Band Pulldown) | 3 | 10–12 | 60 sec | Pull to upper chest |
| Lateral Raises | 3 | 12–15 | 45 sec | Keep slight elbow bend |
| Dead Bug | 3 | 10 each side | 45 sec | Keep lower back pressed to floor |
Progressive Overload: The Key to Results
Doing the same workout with the same weights forever won't maintain muscle. You need progressive overload—gradually increasing the challenge over time.
How to progress:
- When you can complete all reps with good form for all sets, increase the weight by 5–10%
- If you can't increase weight, add 1–2 reps per set
- If you can't add reps, add one more set
- Track every workout so you know where you are
- Week 1: Goblet Squat, 20 lbs, 3×10
- Week 2: Goblet Squat, 20 lbs, 3×12 (hit top of rep range)
- Week 3: Goblet Squat, 25 lbs, 3×10 (increased weight, dropped reps slightly)
- Week 4: Goblet Squat, 25 lbs, 3×11 (building back up)
Modifications for Low Energy Days
GLP-1 medications can cause fatigue, especially when combined with a calorie deficit. Some days you won't feel like training. Here's how to adjust:
- • Reduce weight by 20–30%
- • Reduce sets from 3 to 2
- • Focus on completing the movement pattern, not maximal effort
- • A lighter workout is infinitely better than no workout
- • Do a "minimum viable" session: 2 sets each of squats, push-ups, and rows
- • Takes 10–15 minutes, preserves the training stimulus
- • Better than skipping entirely
Stop and contact your healthcare provider. These aren't normal "tired" feelings.
The Home Version (Minimal Equipment)
You can run this entire program with a set of adjustable dumbbells (or a few fixed weights), a resistance band set, and a sturdy chair.
Every gym exercise has a home substitute:
- Leg Press → Goblet Squat, Lunges, or Step-Ups
- Lat Pulldown → Band Pulldown or Doorway Row
- Bench Press → Floor Press with Dumbbells or Push-Ups
- Leg Curl → Slider Leg Curl or Stability Ball Curl
No equipment at all? Bodyweight training still works:
- Squats, lunges, step-ups for legs
- Push-ups (regular, incline, decline) for chest/shoulders
- Inverted rows under a table for back
- Pike push-ups for shoulders
The stimulus matters more than the equipment.
Recovery: The Forgotten Factor
Training breaks muscle down. Recovery is when it rebuilds. Skimp on recovery, and you undermine everything else.
Sleep is non-negotiable. Aim for 7–9 hours nightly. Growth hormone release peaks during deep sleep, which directly supports muscle repair and preservation. Poor sleep also increases cortisol, a hormone that promotes muscle breakdown.
If GLP-1 side effects are disrupting your sleep (some people experience insomnia or GI discomfort at night), address this. Timing your dose differently, avoiding late-night eating, and standard sleep hygiene practices can help.
Rest between training sessions. Don't train the same muscles on consecutive days. The recommended schedule (full-body 2–3x per week with at least one day between) already accounts for this.
Manage stress. Chronic stress elevates cortisol, which is catabolic (promotes breakdown). Activities like walking, light stretching, meditation, or whatever helps you decompress support your body's recovery processes.
Deload when needed. Every 4–6 weeks, consider reducing training intensity or volume by 30–50% for one week. This allows accumulated fatigue to clear and can actually improve subsequent progress.
The Weight Loss Speed Limit
This is where many GLP-1 users get into trouble. The medication works too well, and rapid loss leads to excessive lean mass loss.
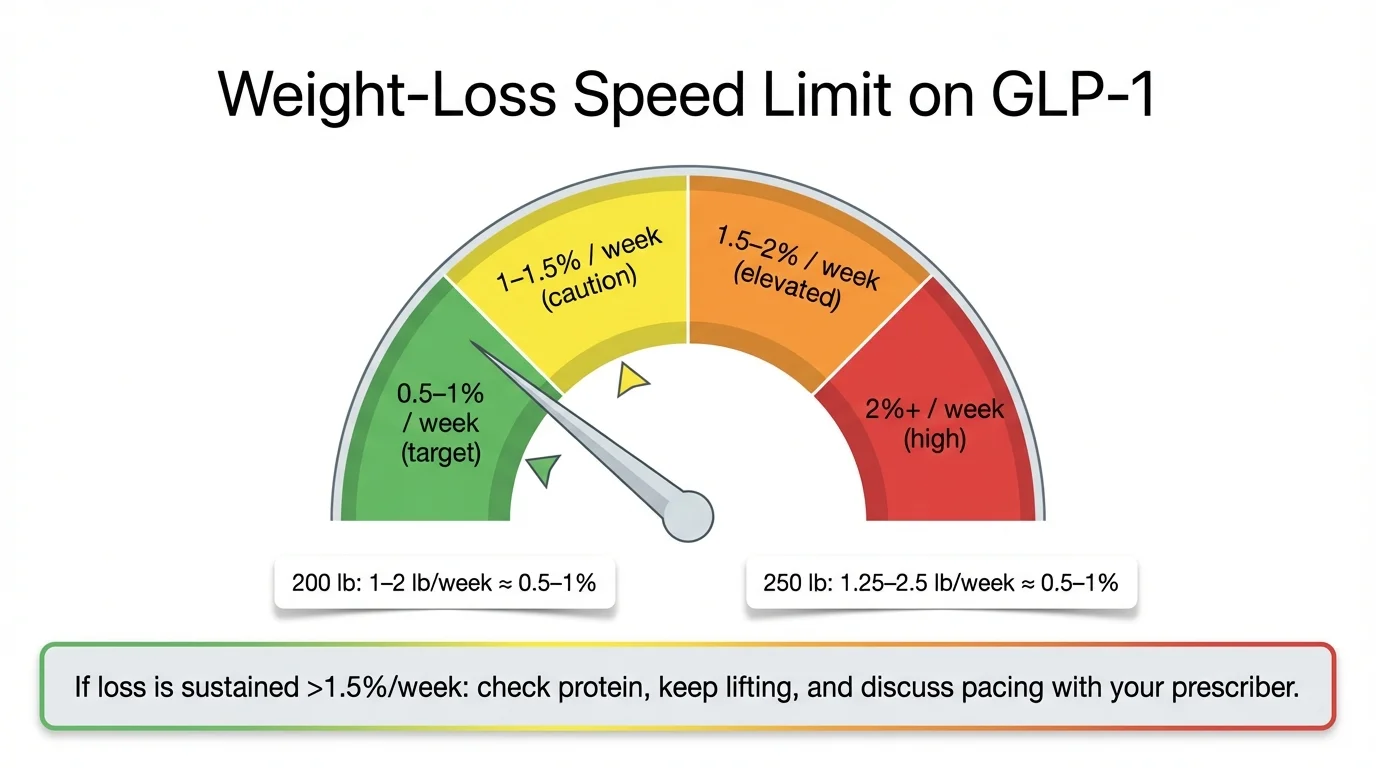
How Fast Is Too Fast?
A good rule of thumb: aim to lose 0.5–1% of your body weight per week.
For a 200-pound person, that's 1–2 pounds per week. For a 250-pound person, 1.25–2.5 pounds per week. Going faster than this consistently increases the proportion of lean mass you lose. Occasionally losing more (especially early when water weight drops) is fine, but sustained rapid loss is a red flag.
| Weight Loss Rate | Risk Level | What to Consider |
|---|---|---|
| 0.5% body weight/week | Low | Sustainable, muscle-preserving |
| 1% body weight/week | Moderate | Sustainable with proper protein/training |
| 1.5% body weight/week | Elevated | Check protein is maxed, training is consistent |
| 2%+ body weight/week | High | Consider speaking with prescriber about pacing |
What To Do If You're Losing Too Fast
First, confirm it's actual weight loss and not normal fluctuation. Weigh yourself under consistent conditions (same time, same state) and look at the weekly average, not daily numbers.
If you're consistently losing >1%/week, double-check protein and training. If it's sustained >1.5%/week for 2–3 weeks, consider these steps:
- Increase calories slightly — Add 100–200 calories per day, from protein if possible
- Check your protein — If you're falling short, this is the priority
- Ensure training is happening — Two sessions minimum, every week
- Talk to your prescriber — Dose titration and timing can affect loss rate
Slowing down might feel counterintuitive when you're motivated, but the goal is to reach your target weight with your muscle (and metabolism) intact. Arriving lean and strong beats arriving lighter and weak.
When Slower Is Especially Important
For some people, even 1% per week may be too aggressive:
- Adults over 60: Muscle loss with age (sarcopenia) is already occurring; preserving muscle is critical for independence
- People with low starting muscle mass: Less buffer means any loss is proportionally larger
- Those with a history of frailty or falls: Muscle supports balance and bone protection
- Anyone with chronic health conditions: Work closely with your healthcare team
Eating Enough When Your Appetite Is Gone
This might be the hardest part of muscle preservation on GLP-1s. The medication kills your hunger—that's literally how it works. But you still need to eat enough to support muscle maintenance. For more strategies, see our GLP-1 nausea food guide.
The "Protein First" Meal Strategy
We covered this above, but it bears repeating: when you sit down to eat, protein goes first. Before the salad, before the bread, before anything else. If you only eat half your meal, at least you got the important part.
Meal Timing Strategies
GLP-1 medications often cause appetite to fluctuate throughout the day. Pay attention to your patterns and use them.
- If mornings are easier: Front-load calories and protein at breakfast and lunch
- If you have a "window": Identify when you can eat more comfortably and prioritize that time
- If evening is your worst time: Get most protein in earlier; use a simple protein shake for dinner if needed
- Injection day strategy: Some people find eating easier on certain days relative to their injection—plan accordingly
Side Effect-Specific Strategies
| Side Effect | What Helps | What to Avoid |
|---|---|---|
| Nausea | Bland foods, cold foods, ginger, small portions | Greasy/fried foods, strong smells, large volumes |
| Early satiety | Calorie-dense protein sources, liquid calories | High-fiber bulky foods before protein |
| Constipation | Fiber (gradually), water, movement | Sudden fiber increases, dehydration |
| Reflux/heartburn | Upright eating, smaller meals, no late eating | Acidic foods, lying down after meals, large portions |
| Food aversions | Rotate protein sources, try different temperatures | Forcing foods that trigger aversion |
See also: GLP-1 constipation relief | GLP-1 heartburn foods
Liquid Protein Options
When solid food won't go down, liquids become your friend:
- Protein shakes: 20–30g protein, 120–200 calories
- Greek yogurt smoothies: Blend with fruit and protein powder
- Bone broth with collagen: Lower protein but easier to consume
- Milk or soy milk: 8g protein per cup
- Protein coffee: Add protein powder to cold coffee
These aren't ideal long-term—whole foods are better for satiety and micronutrients—but they're excellent tools for days when eating feels impossible.
Hydration and Electrolytes
Reduced food and fluid intake plus GI side effects (vomiting, diarrhea) can increase dehydration risk on GLP-1 medications—so intentional fluids and electrolytes matter.
Minimum targets:
- 64 oz (8 cups) of water daily
- More if you're exercising or in hot weather
Signs of dehydration:
- Dark urine
- Headaches
- Fatigue
- Dizziness when standing
If you're experiencing vomiting or diarrhea (possible side effects), electrolyte replacement becomes important. Sports drinks, electrolyte tablets, or even a pinch of salt in water can help.
Supplements: What Helps and What's Hype
The supplement industry is filled with products claiming to prevent muscle loss. Here's what the evidence actually supports.
Tier 1: Strong Evidence — Recommended
This is the most studied sports supplement in history, with decades of research supporting its safety and effectiveness (ISSN position stand). For GLP-1 users specifically:
- Enhances strength and workout performance
- Supports muscle hydration and cellular energy
- May help preserve muscle during calorie deficits
- Extensively studied, excellent safety profile
Dosage: 3–5 grams daily. No loading phase needed.
Important note: Creatine causes 1–2 pounds of water weight gain in muscles. This is inside your muscle cells, not bloating, and is actually a good thing. Don't let this "gain" discourage you—it's not fat.
Safety note: If you have kidney disease or are being monitored for kidney function, ask your clinician before using creatine.
Cost: Approximately $5–10/month
Vitamin D deficiency is linked to muscle weakness and is common in the general population. For GLP-1 users eating less food, getting enough from diet alone is harder.
Dosage: If deficient, your clinician may recommend supplementation. For general supplementation, many people use ~1,000–2,000 IU/day. The safest approach is to test your 25(OH)D levels and follow your clinician's guidance. The adult Tolerable Upper Intake Level is 4,000 IU/day (NIH ODS)—avoid exceeding this long-term without medical supervision.
Cost: Approximately $5–10/month
Tier 2: Moderate Evidence — Consider
HMB is a metabolite of the amino acid leucine. Research shows it may reduce muscle protein breakdown, particularly useful during calorie restriction or for older adults.
Dosage: 3 grams daily
Best for: Older adults, those who can't train intensely, during aggressive calorie deficits
Cost: Approximately $20–30/month
May support muscle protein synthesis and has anti-inflammatory benefits. Evidence is moderate but consistent.
Dosage: Food-first is ideal (fatty fish 2x/week). If supplementing, typical doses are ~1g/day EPA+DHA. Higher doses (2–3g) are sometimes used for triglycerides but should be under clinician guidance. FDA recommends total EPA+DHA intake not exceed 3g/day, with no more than 2g/day from supplements (NIH ODS).
Cost: Approximately $15–25/month
Tier 3: Weak Evidence — Optional
May support skin elasticity and connective tissue (relevant for "Ozempic face" concerns). Limited evidence for muscle preservation specifically.
Dosage: 10–15 grams daily if using
If you're eating enough protein, BCAAs provide no additional benefit. They're already in your protein. Save your money.
What to Avoid
- Fat burners/thermogenics: Often contain stimulants, minimal effectiveness, potential safety concerns
- "Testosterone boosters": Over-the-counter products are largely ineffective
- Proprietary blends with hidden ingredients: You don't know what you're getting
- Gray-market peptides: Unregulated, potentially dangerous, not worth the risk
The Supplement Summary
| Supplement | Evidence | Dosage | Cost/mo | Verdict |
|---|---|---|---|---|
| Creatine Monohydrate | Strong | 3–5g/day | $5–10 | Highly recommended |
| Vitamin D | Strong | 1,000–2,000 IU | $5–10 | Recommended if deficient |
| HMB | Moderate | 3g/day | $20–30 | Consider if over 50 |
| Omega-3 | Moderate | ~1g EPA+DHA | $15–25 | Consider |
| Collagen | Weak | 10–15g | $15–25 | Optional |
| BCAAs | Weak | N/A | N/A | Skip if protein adequate |
How to Track Your Progress
The scale tells you one number. It doesn't tell you whether you're losing fat, muscle, or water. Here's how to actually know what's happening.
Why the Scale Lies
Imagine two scenarios after 3 months on a GLP-1:
Person A: Lost 30 pounds. 24 lbs was fat, 6 lbs was muscle. Now weighs less but is weaker, metabolism has slowed, skin looks looser.
Person B: Lost 25 pounds. 23 lbs was fat, 2 lbs was muscle. Now weighs slightly more than Person A but is stronger, metabolism preserved, body looks toned.
The scale would say Person A did "better." Reality says the opposite. You need measures beyond weight.
Gold Standard: DEXA Scan
DEXA (Dual-Energy X-ray Absorptiometry) is the most accurate way to measure body composition outside of a research lab. It shows total body fat (in pounds and percentage), lean mass (in pounds), bone density, and regional breakdown (where fat is distributed).
How to use it:
- Get a baseline scan before or early in treatment
- Repeat every 3 months during active weight loss
- Compare fat loss vs. lean mass loss
- • 75–85% of weight lost is from fat
- • Lean mass stable or minimal decrease
- • Bone density stable
- • More than 35% of weight lost from lean mass
- • Significant lean mass drop in legs
- • Declining bone density
Cost: $50–150 per scan. Where to find: DEXA-specific clinics (BodySpec, DexaFit), some gyms, medical offices, university research centers.
Secondary Methods
If DEXA isn't accessible, combine these:
Body measurements (monthly): Waist circumference (most important for health), hip, thigh, upper arm. Waist going down while arms/thighs stay relatively stable = losing fat, preserving muscle.
Progress photos (monthly): Same lighting, same angles, same time of day. Front, side, back views. Look for muscle definition, not just size.
Strength tracking (every workout): Log weights and reps for key exercises. Are you getting stronger or weaker over time? Maintained or increasing strength = muscle preservation. This is actually the most practical day-to-day indicator.
The Monthly Check-In Protocol
Every 4 weeks, assess:
Measurements
- Weight (weekly average)
- Waist circumference
- At least one limb measurement
Strength
- Test lower body (squat)
- Test upper push (bench)
- Test upper pull (row)
- Compare to last month
Habits
- Average daily protein
- Training sessions completed
- Side effects affecting intake
Warning Signs You're Losing Too Much Muscle
Catch problems early, before they become serious.
Physical Warning Signs
- Unusual fatigue — Beyond what a calorie deficit normally causes
- Consistent strength loss — Key lifts declining for 3+ weeks straight
- Feeling "deflated" — Clothes looser but skin saggy, not toned
- Difficulty with daily activities — Stairs feel harder, carrying things is tiring
- Balance problems — Especially concerning for older adults
- Slow recovery — Taking much longer than usual to recover from workouts
Metric-Based Red Flags
| Indicator | Concerning Level | Action |
|---|---|---|
| % of weight from lean mass (DEXA) | >35% | Increase protein, ensure training, consider HMB |
| Strength on key lifts | Down >10% over 4 weeks | Review training, add volume, check recovery |
| Rate of weight loss | >1.5% body weight/week sustained | Increase calories, talk to prescriber |
| Protein intake | Consistently <1.0g/kg/day | Priority fix — this is the biggest lever |
When to Talk to Your Healthcare Provider
Contact your prescriber or healthcare team if:
- You're experiencing persistent unusual weakness
- Balance or falls are becoming an issue
- You can't eat enough due to side effects despite trying strategies
- You're losing weight much faster than expected
- You have underlying conditions (kidney disease, diabetes) that need monitoring
Your provider can adjust dosing, timing, or add supportive interventions.
Can You Build Muscle While on GLP-1?
Short answer: Yes, it's possible. But understand the tradeoffs.
The Reality of Building Muscle in a Deficit
Building muscle optimally requires a calorie surplus. Your body needs extra energy and nutrients to create new tissue. When you're in a calorie deficit (which GLP-1 medications create), you're not in the optimal state for muscle building.
However, "body recomposition"—losing fat while gaining some muscle—is possible, especially for:
- Beginners to strength training: "Newbie gains" can happen even in a deficit
- People returning after a layoff: Muscle memory helps regain lost muscle faster
- Those with significant excess fat: The body can pull energy from fat stores to support muscle building
The Recomposition Approach
If your goal is to build muscle while on GLP-1, you need:
- Protein at the top of the range: 1.6–2.0 g/kg minimum
- Consistent, progressive strength training: 3–4 sessions per week
- Moderate calorie deficit: Not aggressive cutting; closer to maintenance with slight deficit
- Patience: Recomp is slower than either pure bulking or cutting
- Creatine: The one supplement most likely to help
Realistic Expectations
Most GLP-1 users should focus on preserving muscle while losing fat, not building muscle. Once you've reached your target weight, you can shift focus to a building phase with more calories and training volume. Trying to do both simultaneously often means doing neither well. The exception is true beginners to strength training, who can see meaningful muscle gains even while losing weight.
Ozempic Face: Prevention and Treatment
"Ozempic face" has become a widely-discussed concern—the facial hollowing and sagging that can occur with rapid weight loss. Let's address it directly.
What Causes Ozempic Face
The name is misleading. GLP-1 medications don't target your face specifically. What happens:
- Rapid weight loss reduces fat throughout your body, including facial fat
- Facial fat provides structure and fullness; losing it creates a "deflated" appearance
- Muscle loss (including small facial muscles) compounds the effect
- Skin that stretched to accommodate more volume doesn't snap back instantly
This isn't unique to GLP-1s—the same thing happens with bariatric surgery or any rapid weight loss. It's just more discussed now because of how effective and widespread these medications have become.
Risk Factors
You're more likely to experience noticeable facial changes if:
- You're losing weight very quickly
- You're over 40 (skin elasticity decreases with age)
- You're losing significant muscle along with fat
- You have naturally low facial fat to begin with
- You're dehydrated
Prevention Strategies
Many of the same strategies that preserve body muscle also help preserve facial structure:
- Slow your weight loss rate — Giving your skin time to adapt reduces sagging
- Maintain adequate protein — Supports collagen production and muscle preservation
- Stay hydrated — Dehydration worsens skin appearance
- Protect your skin — Sunscreen, moisturizer, retinoids can help maintain skin quality
- Don't neglect strength training — Overall muscle preservation supports body composition
- Consider collagen supplementation — Limited evidence, but may support skin elasticity (10–15g daily)
Treatment Options (If It Happens)
If facial volume loss has already occurred:
Non-surgical options:
- Dermal fillers (hyaluronic acid) — Temporary, 6–18 months duration, $600–1,500+ per treatment
- Sculptra (poly-L-lactic acid) — Stimulates collagen, longer-lasting, multiple sessions
- Radiofrequency treatments (Morpheus8, FaceTite) — Skin tightening
Surgical options:
- Fat grafting — Uses your own fat, longer-lasting results
- Facelift — For significant sagging
Timing note: Many providers recommend waiting until weight has stabilized before pursuing treatment, so you're not chasing a moving target.
Perspective
Facial changes can be distressing, but consider the bigger picture: the health benefits of significant weight loss—reduced cardiovascular risk, improved metabolic health, better mobility—generally far outweigh cosmetic concerns. Many people find their face "adjusts" over time as skin gradually tightens. If facial changes are a significant concern for you, discuss with your prescriber. Slowing your rate of loss may be appropriate.
Special Populations
Some groups face unique considerations for muscle preservation.
Age-related muscle loss (sarcopenia) is already occurring. GLP-1 treatment on top of this requires extra attention:
- Protein needs are higher: Aim for the upper range (1.5–2.0 g/kg)
- Strength training is critical: Focus on functional movements and balance
- Monitor more closely: Consider DEXA scans to track both muscle and bone
- HMB supplementation may help: Evidence is strongest in older adults
- Don't cut calories too aggressively: Slower loss preserves more muscle
Work closely with your healthcare team, and consider involving a physical therapist or exercise physiologist.
If you're taking GLP-1s for diabetes as well as weight loss:
- Blood sugar monitoring is essential: As you lose weight and reduce food intake, medication needs may change
- Hypoglycemia risk: Especially if on insulin or sulfonylureas alongside GLP-1
- Protein needs same as others: Diabetes doesn't change this
- Exercise benefits: Strength training improves insulin sensitivity
- Coordinate with your care team: Medication adjustments may be needed as weight drops
Protein intake recommendations need adjustment for those with reduced kidney function:
- Consult your nephrologist or renal dietitian — Don't use the general protein calculators
- Protein restriction may be necessary — But how much depends on your specific situation
- Strength training is still beneficial — May need modifications based on energy levels
This is one area where individual medical guidance is essential.
If you're already training seriously:
- Protein at top of range: 1.8–2.2 g/kg or higher
- Training volume may need reduction: Calorie deficit limits recovery capacity
- Accept temporary performance dips: You likely won't PR during aggressive weight loss
- Periodize training: Reduce volume while maintaining intensity
- Monitor recovery carefully: Insufficient recovery leads to muscle loss
GLP-1 medications' appetite suppression can interact dangerously with eating disorder patterns:
- Work with a specialized treatment team — Including therapist and dietitian
- Regular monitoring is essential — Both mental and physical health
- Be honest about thoughts and behaviors — Restriction patterns may resurface
- Know when to stop — Not everyone is a good candidate for these medications
If you have a history of eating disorders, please discuss this with your prescriber before starting GLP-1 medications.
Frequently Asked Questions
Sources and Methodology
How This Guide Was Created
This guide synthesizes information from peer-reviewed clinical trials, systematic reviews, FDA-approved prescribing information, and guidelines from major medical organizations. Every factual claim about clinical trial outcomes or medical recommendations is traceable to published research.
We prioritize:
- Randomized controlled trials — Especially those published in major journals (NEJM, Lancet, JAMA)
- Systematic reviews and meta-analyses — For broader evidence synthesis
- FDA prescribing information — For approved uses and safety data
- Guidelines from medical organizations — For clinical practice recommendations
- Recent publications — For emerging research (with appropriate caveats)
Key Sources Referenced
Clinical Trials:
- STEP-1 Trial (semaglutide): Wilding JPH, et al. New England Journal of Medicine 2021; 384:989-1002
- STEP-1 Body Composition Analysis: STEP-1 Supplementary Appendix (Table S5)
- SURMOUNT-1 Trial (tirzepatide): Jastreboff AM, et al. New England Journal of Medicine 2022; 387:205-216
Reviews and Meta-Analyses:
- "Strategies for minimizing muscle loss during use of incretin-mimetic drugs for treatment of obesity" — Diabetes, Obesity and Metabolism 2024 (PMC11611443)
Guidelines and Position Statements:
- NIH Office of Dietary Supplements: Vitamin D Fact Sheet
- NIH Office of Dietary Supplements: Omega-3 Fatty Acids Fact Sheet
- International Society of Sports Nutrition position stand on protein and exercise
- FDA prescribing information for semaglutide and tirzepatide
Medical Organization Resources:
- Cleveland Clinic
- Mass General Brigham
- UC Davis Health
- American Diabetes Association
What This Guide Is Not
This guide is educational information, not medical advice. It does not replace consultation with your healthcare provider. Individual needs vary based on medical history, medications, and personal circumstances. Always discuss changes to your diet, exercise, or supplement regimen with your doctor or registered dietitian.
Updates: This guide is reviewed and updated quarterly as new research emerges. Last update: February 2026.
The Complete Checklist (Print This)
GLP-1 MUSCLE PRESERVATION CHECKLIST
BEFORE STARTING
- Calculate your protein target: _____ g/day (weight in kg × 1.2–1.6)
- Schedule strength training days (minimum 2 per week)
- Take baseline photos and measurements
- Consider baseline DEXA scan
- Stock high-protein foods and any needed supplements
DAILY NUTRITION
- Hit protein target: _____ g
- Spread across 3–4 meals (25–40g each)
- Eat protein FIRST at every meal
- Drink 64+ oz water
- If nausea: use liquid protein, smaller meals
WEEKLY TRAINING (Minimum 2x)
- Full-body resistance session 1
- Full-body resistance session 2
- Optional session 3
- Log weights and reps for every exercise
- Progress when possible (more weight or reps)
DAILY SUPPLEMENTS (if using)
- Creatine: 3–5g
- Vitamin D: 1,000–2,000 IU (if deficient)
- Optional: HMB 3g, Omega-3 ~1g EPA+DHA
MONTHLY CHECK-IN
- Review weight trend (weekly averages)
- Measure waist and at least one limb
- Test strength on key lifts (compare to last month)
- Take progress photos
- Review protein and training consistency
EVERY 3 MONTHS
- DEXA scan (if accessible)
- Compare lean mass vs. fat mass changes
- Adjust approach if needed
WARNING SIGNS (address if present)
- Strength declining for 3+ weeks
- Losing >1.5% body weight per week consistently
- Protein consistently below target
- Unusual fatigue or weakness
- Balance problems
WHEN TO CONTACT YOUR PROVIDER
- Persistent unusual weakness
- Can't eat due to severe side effects
- Unexpectedly rapid weight loss
- Concerns about medications
- Any symptoms that worry you
Related Resources
Calculate your personalized daily protein target
What to eat when nausea makes protein hard
Instant relief strategies for all side effects
Planning for maintenance after weight loss
Compare telehealth providers
Compare medication options for weight loss
Ready to start your GLP-1 journey with proper muscle preservation support? Licensed providers can help you navigate the medication, nutrition, and exercise strategies that work best for you.
Find a GLP-1 ProviderRelated Articles
GLP-1 Diet Plan: What to Eat + 7-Day Meal Plan
Complete GLP-1 diet plan with protein-first eating framework, 7-day meal plan, grocery list, and side-effect food strategies backed by FDA and JAMA.
GLP-1 Hair Loss: Causes, Timeline & What To Do
FDA trial data on GLP-1 hair loss rates, shedding timeline, and step-by-step action plan to manage it.
GLP-1 and Anxiety: What We Know & What to Do
FDA 2026 meta-analysis findings, medication interaction warnings, brain science, and a step-by-step action plan for GLP-1-related anxiety.
Cons of GLP-1
Honest overview of GLP-1 medication downsides including side effects, risks, and limitations.
GLP-1 SOS: Side Effect Relief
Interactive tool to find immediate relief strategies for common GLP-1 side effects.
GLP-1 Nausea: What to Eat
Foods and strategies to reduce nausea while taking GLP-1 receptor agonist medications.