GLP-1 and Anxiety: What We Know, What’s Rumor, and What to Do If You Feel Worse
Disclosure: Some links on this site are affiliate links. If you purchase through these links, we may earn a commission at no extra cost to you. Thank you for supporting our site.·For informational purposes only—not medical advice.
If you searched “GLP-1 and anxiety,” you’re probably in one of two places right now: you just started Ozempic, Wegovy, Mounjaro, or Zepbound and something feels off — racing thoughts, a knot in your chest, maybe your first panic attack in years — or you’re thinking about starting one and the internet has you terrified.
Here’s what we found after reviewing 15+ peer-reviewed studies, the FDA’s prescribing labels, and their most recent safety analysis:
The FDA’s 2026 meta-analysis of 91 clinical trials (107,910 patients) found no increased risk of anxiety, depression, suicidal thoughts, or other psychiatric side effects in GLP-1 users compared to placebo. They’ve since asked manufacturers to remove suicide-related warnings from Wegovy, Zepbound, and Saxenda labels.
But that’s not the full picture.
Some real-world studies do show higher rates of anxiety among GLP-1 users. A 2024 cohort of 162,253 patients found a 108% increased risk of anxiety diagnoses — though it couldn’t prove the drug caused it. Rodent research shows GLP-1 is both anxiety-increasing in the short term and anxiety-reducing with continued use. And in the adolescent Wegovy trial (ages 12–17), 4% reported anxiety compared to 2% on placebo.
So which is it? That’s exactly what the rest of this page breaks down — what’s actually in the prescribing labels, why the studies disagree, what’s most likely causing your symptoms, and what to do about it today.
If you’re anxious right now and need to know whether it’s a red flag: jump to our triage section below.
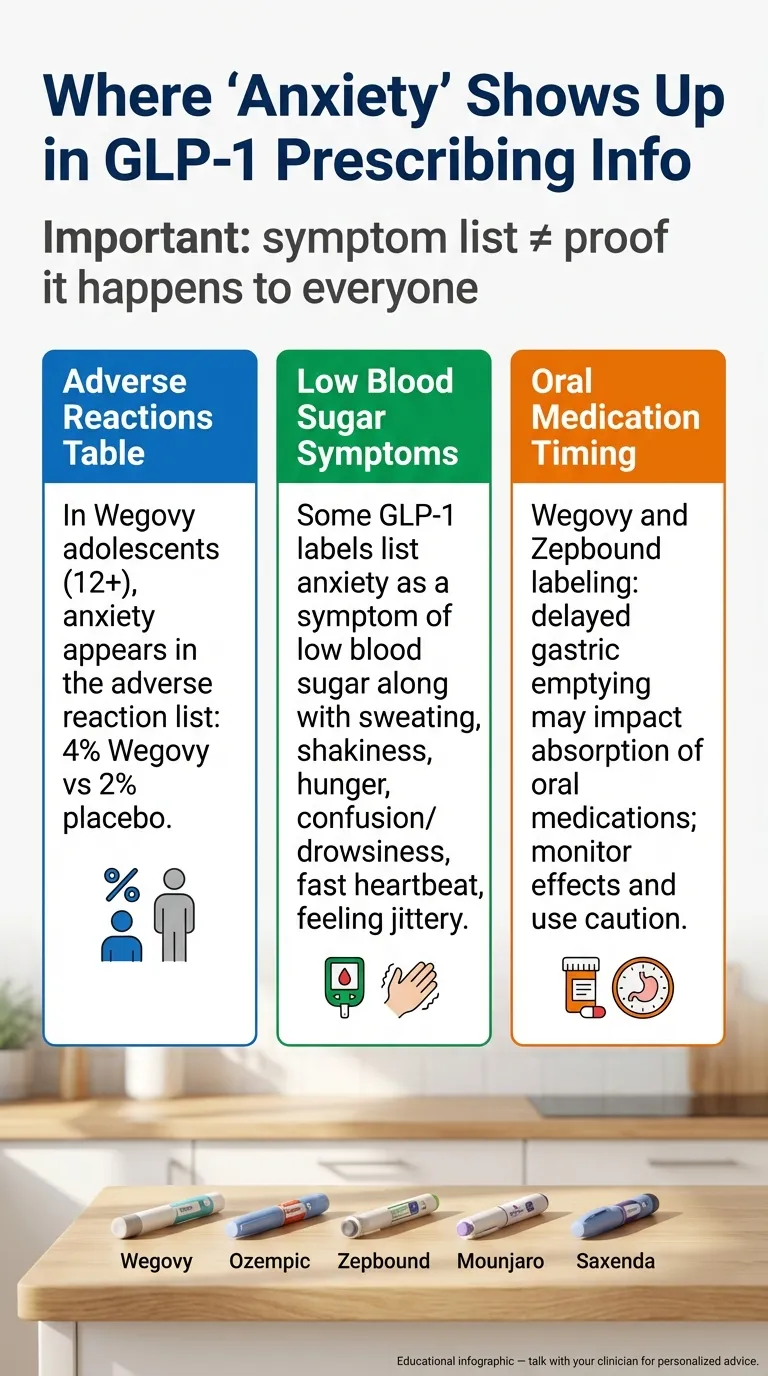
Is Anxiety Listed as a Side Effect? What the Prescribing Labels Actually Say
Before we get into studies and speculation, let’s start with what’s in the official FDA-approved prescribing information — the documents your doctor is supposed to follow. This matters because most articles online blur the line between “what’s in the label” and “what someone posted on Reddit.”
We pulled data directly from the current prescribing information for each major GLP-1 medication. Here’s what we found:
| Medication | Active Ingredient | Where “Anxiety” Appears in Label | Anxiety Rate in Trials | Suicidal Ideation Warning (Feb 2026) | Heart Rate Increase? |
|---|---|---|---|---|---|
| Wegovy | Semaglutide | Listed in pediatric adverse reactions (4% vs 2% placebo). Also listed as a symptom of low blood sugar. | 4% drug vs 2% placebo (adolescents 12–17) | Removed (FDA requested 01/2026; label updated 02/2026) | Yes (class effect) |
| Ozempic | Semaglutide | Listed as a symptom of low blood sugar | Not separately reported for anxiety | Never had one | Yes (class effect) |
| Zepbound | Tirzepatide | Not listed as adverse reaction. Gastric emptying interaction warning exists. | Not prominently flagged | Removed (FDA requested 01/2026; label updated 02/2026) | Yes |
| Mounjaro | Tirzepatide | Not listed as adverse reaction | Not prominently flagged | Never had one | Yes |
| Saxenda | Liraglutide | Anxiety/irritability listed as hypoglycemia symptoms | Not separately reported for anxiety*† | Removed (FDA requested 01/2026; label updated 02/2026) | Yes |
| Rybelsus | Semaglutide | Listed as a symptom of low blood sugar | Limited data | Never had one | Yes |
*†Note on Saxenda: In the STEP-8 head-to-head trial, liraglutide had 15.0% “Psychiatric disorders” system organ class events (driven largely by insomnia) vs. 5.6% for semaglutide — but this is a broad category, not an anxiety-specific rate.
Sources: Wegovy prescribing information (novo-pi.com/wegovy.pdf); Zepbound prescribing information (pi.lilly.com/us/zepbound-uspi.pdf); Saxenda prescribing information revised 02/2026 (novo-pi.com/saxenda.pdf); FDA Drug Safety Communication, January 13, 2026.
The mistake many articles make
Here’s something important that most posts get wrong: the 4% anxiety figure for Wegovy comes from the pediatric (ages 12–17) adverse reaction table, not adults. And in several prescribing labels, “anxiety” appears as a symptom of low blood sugar, not as a standalone side effect of the medication itself.
That’s a meaningful distinction. If your blood sugar drops because you’re eating significantly less on a GLP-1, you might feel anxious, shaky, irritable, and sweaty. That’s hypoglycemia mimicking anxiety — not the drug directly causing psychiatric symptoms.
We’re not saying medication-related anxiety doesn’t happen. We’re saying you deserve accuracy about what the labels actually say before reading someone else’s interpretation.
Feeling Anxious on a GLP-1 Right Now? Start Here
If you’re reading this mid-anxiety episode, you don’t need a research review. You need a quick answer: Is this dangerous, and what do I do right now?
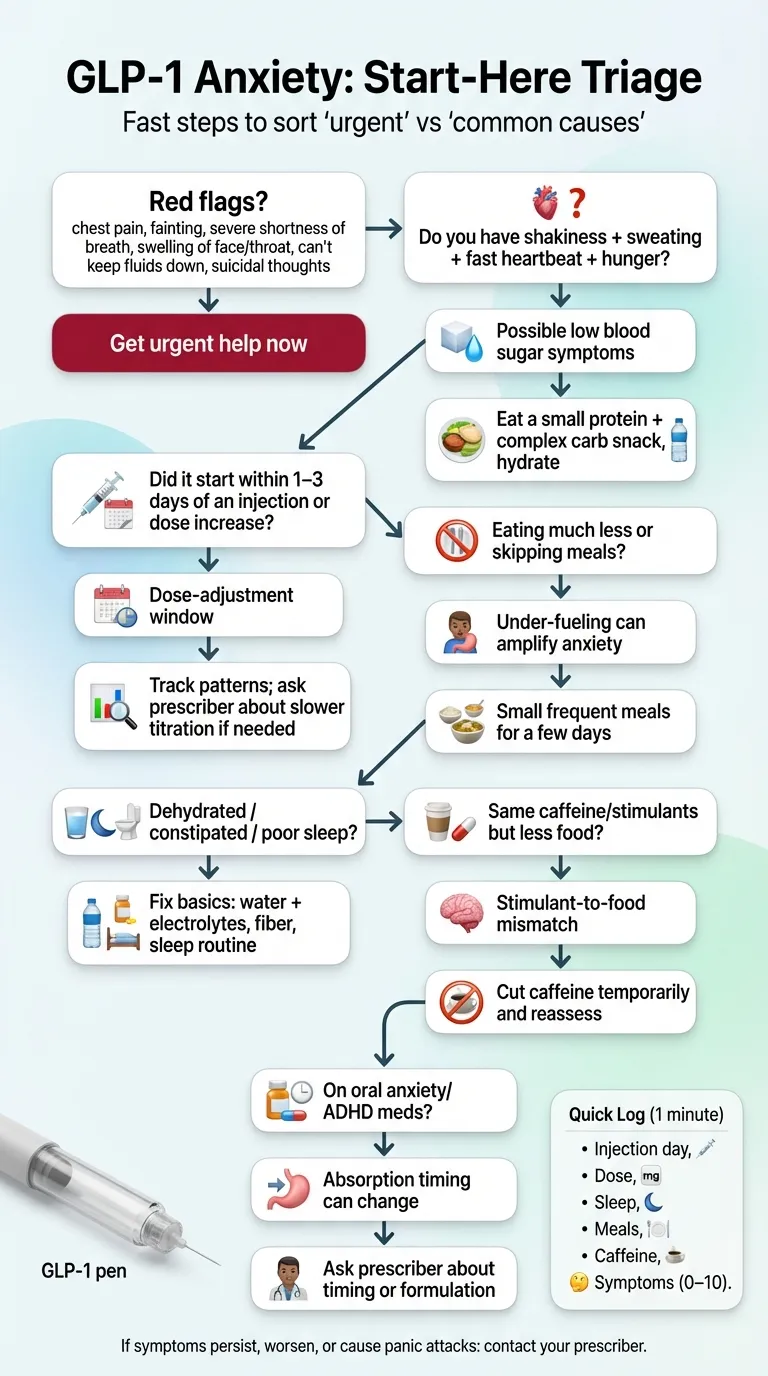
Red flags — seek urgent care if any of these apply
Stop reading and get help now if you’re experiencing:
- Severe chest pain, fainting, or severe shortness of breath
- Signs of a severe allergic reaction (swelling of face/throat, difficulty breathing)
- Severe dehydration (can’t keep fluids down for 24+ hours, confusion, dark urine)
- Suicidal thoughts or thoughts of self-harm → Call 988 (Suicide and Crisis Lifeline) or go to your nearest emergency room
We are not doctors. This page is not medical advice. But we take this seriously, and so should you.
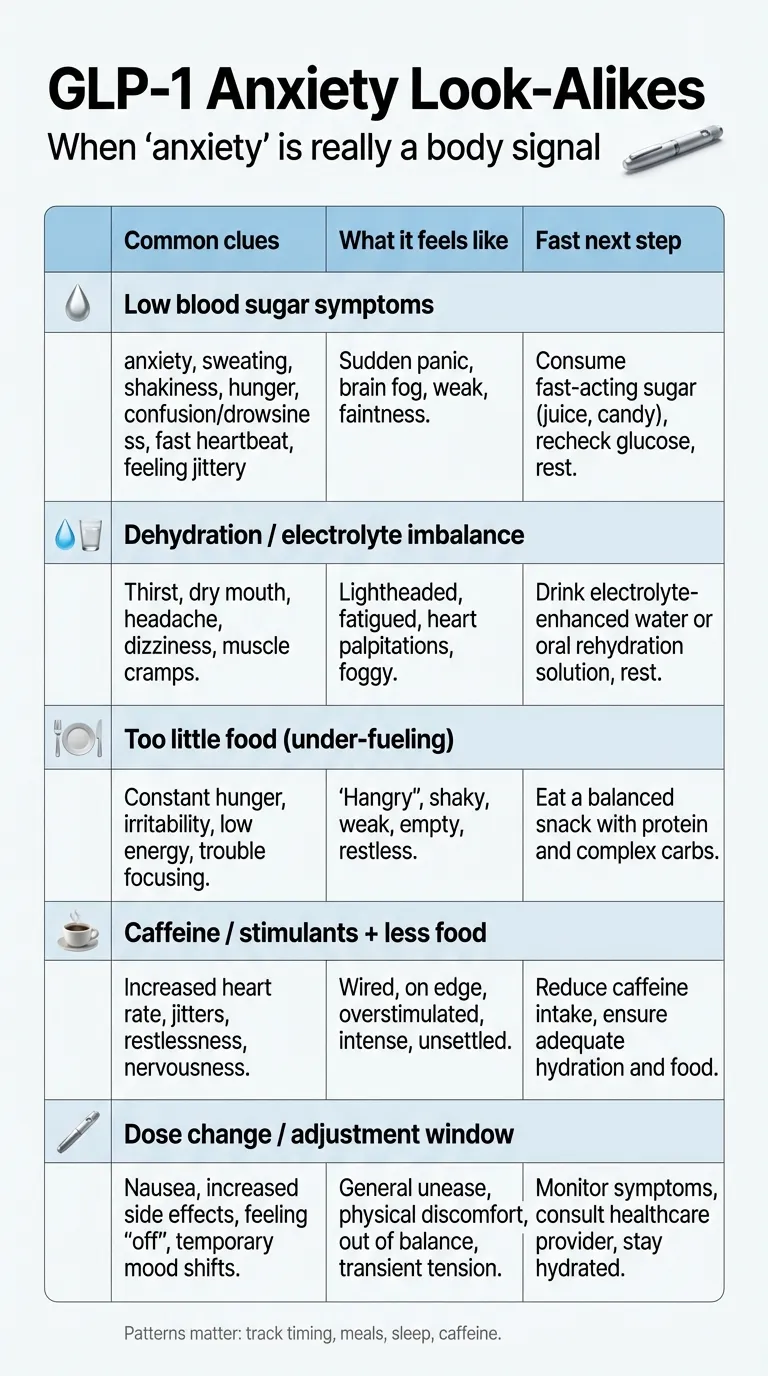
Quick sort: Is this anxiety — or something else that feels like anxiety?
This is the part most pages skip, and it matters a lot. Many GLP-1 “anxiety” symptoms have a physical explanation that’s easier to fix than you’d think. Ask yourself these questions:
1. Did symptoms start within 24–72 hours of your injection or a dose increase?
→ If yes: Dose-escalation windows are the most common trigger for anxiety-like symptoms. Your body is adjusting to a higher level of GLP-1 receptor activation. Research in rodents shows this acute response often subsides with continued use.
2. Are you eating substantially less than usual?
→ If yes: Low blood sugar (hypoglycemia) symptoms include anxiety, shakiness, racing heart, sweating, irritability, and confusion. These overlap almost perfectly with a panic attack. If you’re eating less than 1,000 calories a day, this could be your answer.
3. Do you have shakiness, sweating, hunger, or irritability along with the anxiety?
→ If yes: This is a classic low blood sugar symptom cluster. Eat something with protein and complex carbs. If symptoms improve within 15–20 minutes, blood sugar was likely the issue.
4. Are you dehydrated, constipated, or sleeping poorly?
→ If yes: GLP-1 side effects like nausea and reduced appetite often lead to dehydration and poor sleep. Both are strong drivers of anxiety. This isn’t trivial — chronic dehydration and sleep deprivation can mimic clinical anxiety disorders.
5. Have you changed your caffeine or stimulant intake?
→ If yes: If you dropped food intake but kept your 3-cup coffee habit, the stimulant-to-food ratio just changed dramatically. Caffeine on an empty stomach with dehydration is an anxiety factory.
6. Did you recently change your SSRI, SNRI, benzodiazepine, or ADHD medication dose?
→ If yes: GLP-1 medications slow gastric emptying, which can affect how your body absorbs oral medications. Your psychiatric medication may not be absorbing at the same rate it was before. This is in the prescribing labels. We cover this in detail below.
What to do in the next 24 hours
These are safe, general actions — not medical advice, but common sense while you wait to talk to your provider:
- Hydrate aggressively. Water plus electrolytes. GLP-1 side effects (nausea, vomiting, reduced appetite) can dehydrate you faster than you realize.
- Eat something. Even if you’re not hungry. A small meal with protein and complex carbs can stabilize blood sugar.
- Cut stimulants temporarily. Reduce caffeine by half for 48 hours and see what happens.
- Track the timing. Write down: when you injected, when anxiety started, what you ate, how you slept, your caffeine intake. Patterns matter — and this data is exactly what your prescriber needs.
- Don’t stop your medication abruptly. Stopping suddenly can cause rebound effects, blood sugar spikes, and rapid weight regain. Always work with your prescriber first.
When to call your prescriber (don’t wait for your next appointment)
- Anxiety is persistent (more than a few days) or worsening week over week
- You’re having panic attacks you’ve never experienced before
- You can’t sleep more than 4 hours per night
- You feel emotionally numb, “flat,” or disconnected
- Symptoms cluster around dose escalation and don’t resolve within a week
- You’re on psychiatric medication and suspect it’s not working as well
What Did the FDA Actually Find? (The 2026 Update Most Pages Are Missing)
In January 2026, the FDA completed the most comprehensive review of GLP-1 medications and mental health to date. This matters because it directly contradicts a lot of what you’ll read online.
What they did
The FDA conducted a meta-analysis of 91 placebo-controlled clinical trials involving 107,910 patients — 60,338 on a GLP-1 medication and 47,572 on placebo. This covered every FDA-approved GLP-1 receptor agonist.
They also analyzed healthcare claims data from the FDA Sentinel System — a national electronic database covering nearly 2.25 million patients — comparing GLP-1 users to users of SGLT2 inhibitors (another popular diabetes drug class).
What they found
No increased risk of suicidal thoughts or behavior. No increased risk of anxiety, depression, irritability, or psychosis. Across 91 trials.
Based on these findings, the FDA asked Novo Nordisk and Eli Lilly to remove the suicidal ideation and behavior warnings from the labels of Wegovy, Saxenda, and Zepbound. Those warnings had originally been inherited from older weight-loss drugs and were never specific to GLP-1s.
What they didn’t say
The FDA did not say “GLP-1s cannot affect mood in any individual.” What they said is that at a population level, across the largest dataset we have, there’s no signal. They still recommend monitoring for mood changes — “no increased risk on average” is not the same as “zero risk for every person.”
This distinction matters. If you’re one of the people who does feel different on a GLP-1, the FDA review doesn’t invalidate your experience. It means your symptoms may have an explanation other than a direct psychiatric effect of the drug — and that’s actually useful information, because those other explanations (blood sugar, dehydration, sleep, medication interactions) are often fixable.
Source: FDA Drug Safety Communication, January 13, 2026. “FDA Requests Removal of Suicidal Behavior and Ideation Warning from Glucagon-Like Peptide-1 Receptor Agonist (GLP-1 RA) Medications.”
Why Do Some Studies Show the Opposite? (And What That Means for You)
If the FDA says no increased risk, why do other studies show higher anxiety rates? The answer isn’t that someone is lying — it’s that different study types answer different questions.
Understanding the evidence hierarchy
| Evidence Type | What It’s Good For | What It Found on GLP-1 + Anxiety | Weight We Give It |
|---|---|---|---|
| FDA Meta-Analysis (91 RCTs) | Best for proving causation | No increased risk of anxiety or other psychiatric events | ★★★★★ (Gold standard) |
| STEP Trial Post-Hoc Analysis (JAMA 2024) | Good for safety in controlled populations | No increased depression or suicidal ideation with semaglutide 2.4 mg vs placebo | ★★★★ |
| Real-World EHR Studies (Epic 2024) | Shows real-world patterns | Semaglutide users had lower likelihood of anxiety and depression diagnoses | ★★★ (Can’t prove causation) |
| Observational Cohort (Scientific Reports 2024) | Flags associations worth investigating | 108% increased risk of anxiety in GLP-1 users | ★★★ (Association only, major confounders) |
| FAERS/VigiBase Pharmacovigilance | Good for detecting rare signals | Anxiety signals detected for semaglutide (aROR: 1.26) | ★★ (Voluntary, unverified, biased by awareness) |
| Social Media/Anecdotes | Useful for hypothesis generation | Anxiety is the 2nd most discussed mental health topic on GLP-1 subreddits | ★ (No controls, extreme selection bias) |
Why the Scientific Reports study (108% increased risk) sounds scarier than it is
This study gets cited everywhere, usually without context. Researchers looked at 162,253 propensity-score-matched patients using the TriNetX database — half on GLP-1s, half not. They found GLP-1 users had higher rates of anxiety, depression, and suicidal behavior diagnoses.
But here’s what they couldn’t control for:
- People who start GLP-1s see doctors more often, get screened more, and are more likely to receive a psychiatric diagnosis — not necessarily develop one.
- They didn’t account for concurrent medications. If someone started an SSRI at the same time, that wouldn’t be captured.
- They couldn’t separate the drug from the weight loss. Rapid weight loss itself — from any cause, including surgery — is independently associated with mood changes and anxiety.
- Obesity itself carries higher psychiatric risk. People prescribed GLP-1s already have elevated baseline rates of anxiety and depression.
Why real-world studies sometimes show the opposite — lower anxiety
A 2024 Epic Research analysis of electronic health records found that most GLP-1 medications were actually correlated with a lower likelihood of anxiety and depression diagnoses after starting treatment. Semaglutide specifically showed this pattern in non-diabetic patients.
In a Taiwanese nationwide cohort of adults with diabetes, GLP-1 RA use — especially longer than 180 days — was associated with a lower risk of anxiety diagnoses (aHR 0.41), and dulaglutide was associated with lower risk of both anxiety and depression.
Sources: Epic Research, 2024; Tsai WH et al., Frontiers in Pharmacology, 2022 (diabetes cohort); Kornelius et al., Scientific Reports, 2024.
How GLP-1 Medications Actually Affect Your Brain (The Science, in Plain Language)
GLP-1 was originally thought of as a “gut hormone.” It’s not. GLP-1 receptors are found throughout your brain — in the amygdala (your brain’s fear and anxiety center), the hippocampus (memory and stress processing), the nucleus accumbens (reward and pleasure), and the dorsal raphe nucleus (the main hub for serotonin production).
This is why a medication designed to reduce appetite can also affect mood, motivation, pleasure, and anxiety. It’s not a bug in the system — it’s the biology.
The paradox: GLP-1 can be both anxiety-increasing AND anxiety-reducing
This is the single most important scientific finding that almost nobody is communicating clearly, and it explains a lot of the confusion.
A landmark 2016 study published in Psychoneuroendocrinology tested GLP-1 and its long-acting analog Exendin-4 in rodents across multiple anxiety tests. Here’s what they found:
- Acute (single-dose) GLP-1 receptor activation increased anxiety-like behavior. This was consistent across three different anxiety tests.
- Chronic (ongoing) GLP-1 receptor activation did not increase anxiety — and actually reduced depression-like behavior.
- The antidepressant effect was not simply from weight loss. Control rats that were pair-fed (given the same reduced food intake) did not show the same mood improvement.
- Acute GLP-1 altered serotonin signaling in the amygdala — literally changing the chemistry of the brain’s fear center.
What does this mean for you? If you feel anxious in the first few weeks of starting a GLP-1 — especially around dose increases — there is a real neurobiological basis for that. Your brain’s anxiety circuits are being directly activated. This is not “in your head.” It’s in your amygdala. But the research also suggests this acute response may resolve with continued treatment.
Source: Anderberg RH, Richard JE, Hansson C, et al. “GLP-1 is both anxiogenic and antidepressant; divergent effects of acute and chronic GLP-1 on emotionality.” Psychoneuroendocrinology. 2016;65:54-66.
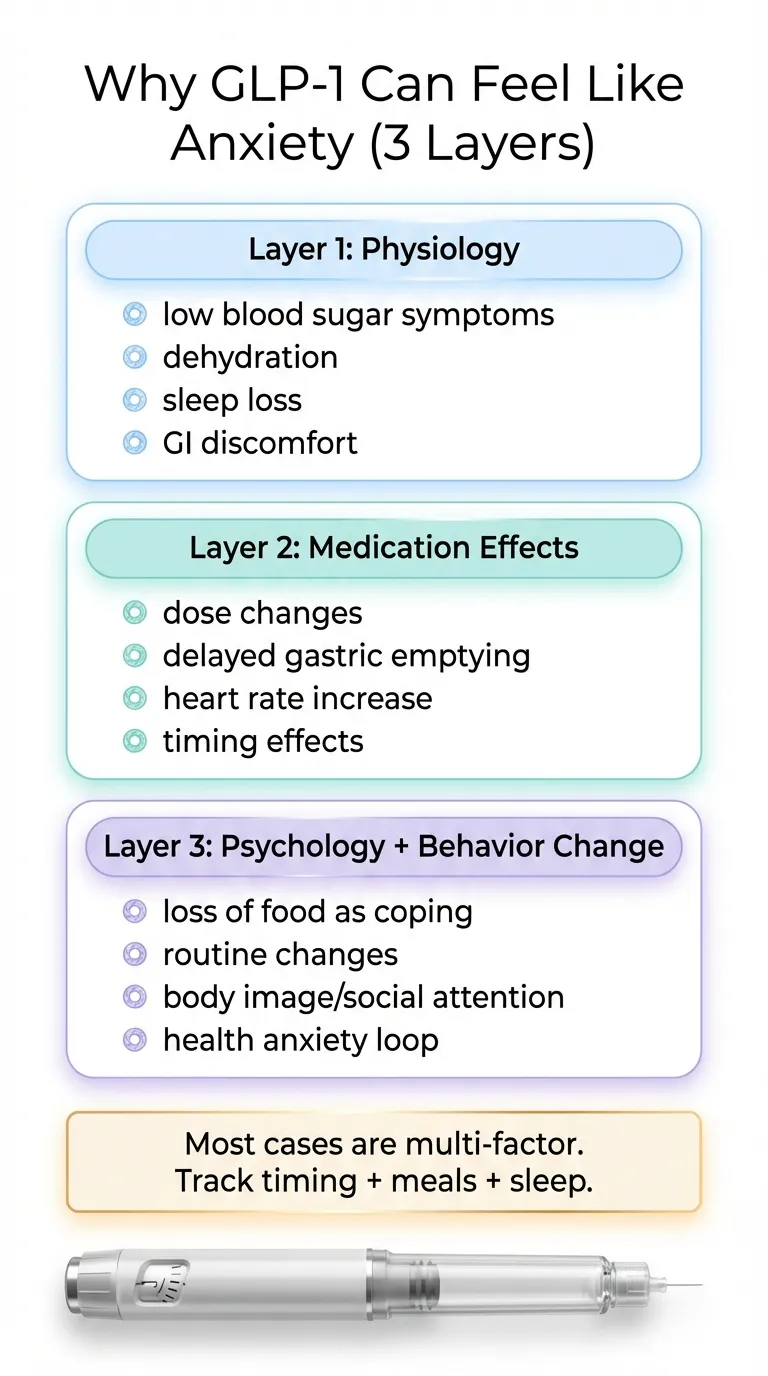
Three layers: Why some people feel anxious on GLP-1s
Not every case of GLP-1-related anxiety has the same explanation. We’ve organized the most common causes into three layers — and the fix is different for each one.
Layer 1: Physiology (the most common “hidden” causes)
These aren’t psychiatric. They’re physical. And they’re often the easiest to fix.
- Low blood sugar (hypoglycemia). GLP-1s increase insulin secretion. Symptoms: anxiety, shakiness, sweating, racing heart, irritability, confusion. Nearly identical to a panic attack.
- Dehydration and electrolyte imbalance. Nausea and reduced appetite lead to less fluid and food intake. Dehydration alone can cause anxiety, brain fog, and heart palpitations.
- Constipation and GI distress. Chronic nausea, bloating, and abdominal pain create a stress response that can register as anxiety.
- Sleep disruption. Insomnia was the #1 discussed mental health topic on GLP-1 subreddits (620 matches — more than anxiety’s 353). Poor sleep is one of the strongest predictors of anxiety.
Layer 2: Pharmacology (the medication doing its thing)
- Increased heart rate. This is a recognized class effect of all GLP-1 receptor agonists. Some people perceive a slightly faster resting heart rate as anxiety or palpitations.
- Dose escalation windows. Each step-up is, biologically, a new acute exposure. This matches the rodent data: acute activation = temporary anxiety.
- Medication interactions (delayed gastric emptying). GLP-1s significantly slow how fast your stomach empties. This can change how quickly your oral medications — including SSRIs, SNRIs, benzodiazepines, and ADHD stimulants — are absorbed.
Layer 3: Psychology and behavior change (real, not “just in your head”)
- Loss of food as a coping mechanism. If food was how you managed stress, anxiety, boredom, or loneliness, and that coping mechanism suddenly stops working — that’s a genuine psychological loss.
- Identity and social pressure from rapid weight loss. People treat you differently. You don’t recognize yourself. This can trigger social anxiety and body dysmorphia.
- Health anxiety. You’re injecting yourself with a medication, reading about side effects, monitoring every sensation. For anxious people, this feedback loop can amplify symptoms.
- Reduced alcohol, nicotine, or compulsive behaviors. GLP-1s appear to reduce cravings for substances beyond food. If these were part of your anxiety management toolkit, losing them can feel destabilizing.
Is This Normal or a Red Flag? How to Tell the Difference
This is the section that doesn’t exist anywhere else, and it’s the one we think matters most. Not every person experiencing anxiety on a GLP-1 is in the same situation.
Scenario A: Early-treatment adjustment (most common)
What it looks like:
- Mild restlessness, nervousness, or feeling “wired”
- Started within the first 1–4 weeks, or right after a dose increase
- No panic attacks, no suicidal thoughts, no inability to function
- Gradually improving week over week
What’s probably happening: Acute GLP-1 receptor activation in your brain. Your serotonin signaling in the amygdala is adjusting.
What to do: Monitor for 2–4 more weeks. Track symptoms daily. Stay in touch with your prescriber. This pattern often resolves as your body adjusts.
Scenario B: Side-effect-driven anxiety
What it looks like:
- Anxiety spikes when you’ve eaten very little (shakiness, sweating, rapid heartbeat, hunger)
- Anxiety is worst when you’re nauseous or after vomiting
- Your heart rate is faster at rest than usual
What’s probably happening: Your anxiety is a downstream effect of physiological side effects — not a direct psychiatric effect of the drug.
What to do: Treat the root cause. Eat regular small meals. Hydrate aggressively with electrolytes. Talk to your prescriber about anti-nausea strategies.
Scenario C: Medication interaction (under-recognized, potentially serious)
What it looks like:
- You’re on an SSRI, SNRI, benzodiazepine, ADHD stimulant, or sleep medication
- Your psychiatric medication seems less effective since starting the GLP-1
- Anxiety feels like a recurrence of old symptoms rather than a new experience
What’s probably happening: GLP-1 medications slow gastric emptying, which can reduce or delay absorption of oral medications. A WHO pharmacovigilance analysis found reports of suicidal ideation with semaglutide showed higher disproportionality when antidepressants (ROR 4.45) or benzodiazepines (ROR 4.07) were co-reported.
What to do: Contact your prescriber soon — this is not a “wait and see” situation. Do not stop either medication on your own. Your doctor may need to adjust timing, dosing, or switch to extended-release formulations.
Scenario D: Red flags — contact your provider now
Seek immediate evaluation if:
- Suicidal thoughts or thoughts of self-harm (call 988 now)
- Panic attacks you’ve never had before, especially if frequent
- Inability to function at work or in daily life
- Severe insomnia (less than 4 hours per night for more than a week)
- Complete emotional numbness — you can’t feel anything
- Paranoia, hallucinations, or feeling disconnected from reality
- Rapid, severe onset after a dose increase with no improvement after 7 days
What to do: Contact your healthcare provider immediately. Don’t stop the medication cold turkey. Your provider may reduce your dose, pause treatment, or refer you for psychiatric evaluation.
Scenario E: Pre-existing anxiety resurfacing
What it looks like:
- You had anxiety before — maybe managed, maybe undertreated
- The GLP-1 seems to have “reactivated” old patterns
- Life circumstances have changed alongside the medication
What’s probably happening: Multiple factors may be converging. The medication may be one contributor, but so are the psychological impacts of rapid body change and loss of familiar coping mechanisms.
What to do: Consider working with a therapist alongside your GLP-1 prescriber. A provider who integrates mental health screening into GLP-1 treatment is ideal.
Do GLP-1s Interact With Anxiety Meds or ADHD Meds?
This is one of the most under-discussed topics in the GLP-1 conversation, and based on what we see in prescribing labels and pharmacovigilance data, it shouldn’t be.
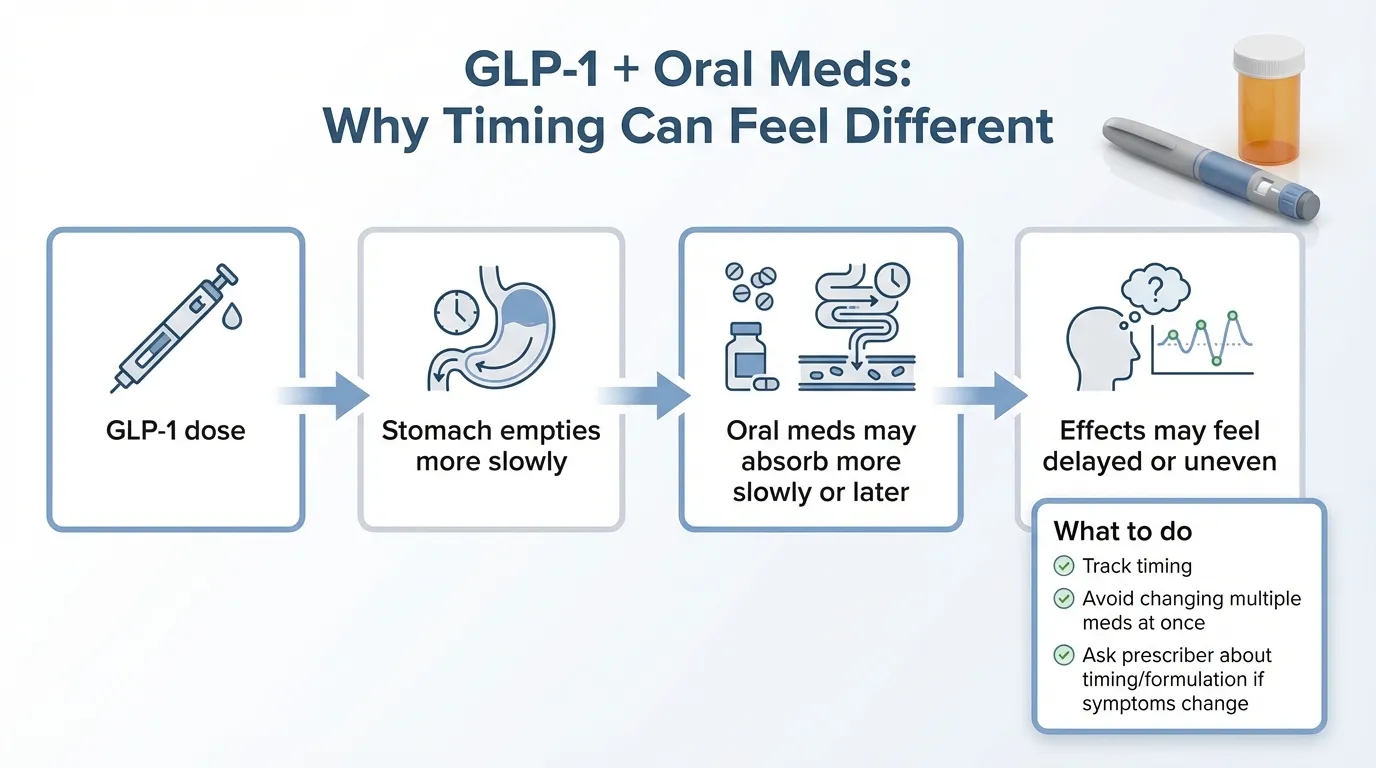
The key mechanism: delayed gastric emptying
GLP-1 receptor agonists slow down how quickly food (and medications) move through your stomach. This is part of how they work — it increases satiety and reduces appetite. But it also means oral medications may be absorbed more slowly or unpredictably. The Zepbound prescribing information explicitly notes this: tirzepatide delays gastric emptying and may impact absorption of concomitant oral medications.
What this means by medication type
SSRIs/SNRIs (Zoloft, Lexapro, Prozac, Effexor, Cymbalta)
If absorption is delayed, you may experience a “wearing off” effect — anxiety or depression symptoms returning as effective blood levels drop. This can look exactly like “the GLP-1 is causing anxiety” when the real issue is your antidepressant isn’t absorbing properly.
Benzodiazepines (Xanax, Klonopin, Ativan, Valium)
These are especially absorption-sensitive. Delayed absorption could mean the medication takes longer to kick in when you need it, potentially increasing anxiety during the wait.
ADHD stimulants (Adderall, Vyvanse, Ritalin, Concerta)
Slowed absorption could affect how quickly stimulants take effect and how long they last. This matters for both immediate-release and extended-release formulations.
Beta blockers (Propranolol)
Often prescribed for performance anxiety. Delayed absorption could reduce their effectiveness when taken “as needed.”
Sleep medications
If your sleep med takes longer to absorb, you may toss and turn longer — and poor sleep is one of the strongest anxiety drivers.
What to ask your prescriber
If you take any oral psychiatric medication alongside a GLP-1, bring this up proactively:
- “Could my GLP-1 be affecting how my [medication] absorbs?”
- “Should I change the timing of when I take my [medication] relative to my injection?”
- “Would an extended-release version work better for me now?”
- “Should we check blood levels of my [medication]?”
In a WHO pharmacovigilance disproportionality analysis (JAMA Network Open, 2024), reports of suicidal ideation with semaglutide showed higher disproportionality when antidepressants (ROR 4.45) or benzodiazepines (ROR 4.07) were co-reported. This is a signal in spontaneous reports — not proof of causation — but it’s a strong enough signal that your prescriber should be aware of it.
Who Is Most Likely to Experience Anxiety on a GLP-1?
Not everyone has the same risk profile. Based on the available evidence, certain groups should be monitored more closely.
People with pre-existing mental health conditions
If you have a history of panic disorder, generalized anxiety disorder, OCD, PTSD, postpartum anxiety, or depression, you deserve extra monitoring — not because GLP-1s are proven to worsen these conditions, but because:
- You were excluded from the clinical trials that established GLP-1 safety data. We simply have less controlled evidence for your situation.
- You may be on medications whose absorption could be affected.
- Rapid weight loss and body change carry psychological weight that intersects with pre-existing conditions.
- You may be more sensitive to the acute neurobiological effects of GLP-1 receptor activation.
This does not mean GLP-1s are off-limits. It means you need a prescriber who screens for mental health, monitors regularly, and has a plan if symptoms emerge.
People on certain medications
Anyone taking oral psychiatric medications — especially SSRIs, SNRIs, benzodiazepines, or stimulants — has an additional risk factor due to potential absorption changes. People combining GLP-1s with insulin or sulfonylureas face higher hypoglycemia risk, which mimics anxiety.
People with significant behavioral changes
If you’ve dramatically reduced calories, stopped eating comfort foods entirely, quit or reduced alcohol, changed your exercise routine substantially, and/or are sleeping poorly — all at the same time as starting a GLP-1 — you’ve changed multiple variables simultaneously. Any one of those could drive anxiety. Teasing apart which factor is responsible requires tracking.
Anxiety Data by Specific GLP-1 Medication
Not all GLP-1s are the same molecule, and the data differs. If you’re considering switching medications, this breakdown matters.
Ozempic (Semaglutide 1 mg) and Anxiety
Ozempic is the lower-dose form of semaglutide, approved for type 2 diabetes. It has never carried a suicide-related warning. Anxiety is not listed as an adverse reaction in the adult prescribing information — it appears only as a symptom of low blood sugar. Ozempic and Wegovy contain the same molecule, but Wegovy is used at a higher dose (2.4 mg vs. 1 mg). If you’re sensitive to side effects, dose may matter.
Wegovy (Semaglutide 2.4 mg) and Anxiety
In clinical trials, 4% of adolescent patients (ages 12–17) reported anxiety compared to 2% on placebo. In January 2026, the FDA requested removal of the suicidal ideation warning. In the STEP-8 head-to-head trial, semaglutide had a 5.6% rate of psychiatric events — compared to 15.0% for liraglutide and 10.6% for placebo.
A post-hoc analysis of the STEP trials published in JAMA Internal Medicine found that semaglutide 2.4 mg did not increase depression or suicidal ideation compared to placebo.
Mounjaro and Zepbound (Tirzepatide) and Anxiety
Tirzepatide is a dual GIP/GLP-1 receptor agonist. Anxiety is not listed as an adverse reaction in either prescribing label. The SURMOUNT trials did not prominently flag psychiatric events. If semaglutide-based medications are causing anxiety issues for you, tirzepatide is a reasonable option to discuss with your prescriber — but be aware that the psychiatric data is thinner, not necessarily better.
Saxenda (Liraglutide 3 mg) and Anxiety
The psychiatric data here is the least favorable. In the STEP-8 head-to-head trial, liraglutide had a 15.0% “Psychiatric disorders” system organ class event rate (driven largely by insomnia) — compared to 5.6% for semaglutide and 10.6% for placebo.
If you’re currently on Saxenda and experiencing anxiety, switching to semaglutide or tirzepatide may be worth discussing with your doctor. The data suggests liraglutide has a less favorable psychiatric profile in this class.
GLP-1 and Dopamine: Emotional Blunting, Anhedonia, and “Ozempic Personality”
“Ozempic personality” is the pop-culture term for mood and behavior changes some people report on GLP-1 medications — feeling “flat,” losing interest in things they used to enjoy, emotional numbness, or personality shifts.
What’s known vs. what’s speculation
GLP-1 receptors are present in the nucleus accumbens — the brain’s reward center — and in dopaminergic pathways. GLP-1 medications appear to modulate dopamine signaling, which is why they reduce cravings for food, alcohol, nicotine, and other substances. But dopamine doesn’t just drive cravings. It drives motivation, anticipation, pleasure, and engagement with life. If a medication turns down dopamine signaling broadly, some people may experience reduced pleasure across the board.
What to do if you feel emotionally “flat”
- Don’t dismiss it. This is a real experience reported by enough people to warrant attention.
- Track it. Is it getting worse, stable, or improving? Did it start with a dose change?
- Talk to your prescriber. They may adjust your dose or consider switching medications.
- Consider therapy. If you’ve lost food as a coping mechanism, a therapist who specializes in body image and adjustment can help.
- Don’t stop abruptly. Always work with your medical team before changing medications.
Can GLP-1 Medications Actually Help Anxiety or Depression?
This might sound contradictory after everything above, but it’s an important part of the full picture — and it’s increasingly supported by evidence.
Why some people feel better on GLP-1s
- Reduced “food noise.” The constant mental chatter about food quiets down. For people whose anxiety was partly driven by food-related stress, this feels like genuine relief.
- Improved physical health and self-efficacy. Losing weight, improving blood sugar control, having more energy, sleeping better.
- Reduced systemic inflammation. Obesity is associated with chronic low-grade inflammation, which is increasingly linked to depression and anxiety.
- The chronic biological effect. As the rodent research suggests, chronic GLP-1 receptor activation may have genuine antidepressant properties independent of weight loss.
What the research says (without overclaiming)
In a Taiwanese nationwide cohort (Tsai WH et al., Frontiers in Pharmacology, 2022), GLP-1 RA use — especially longer than 180 days — was associated with a significantly lower risk of anxiety diagnoses (aHR 0.41, 95% CI 0.27–0.61). Dulaglutide specifically was associated with lower risk of both anxiety and depression.
Researchers are now conducting trials of GLP-1 medications for bipolar disorder, substance use disorders, and depression. Roger McIntyre, a prominent psychiatry researcher, wrote in Psychiatric Times (July 2025) that GLP-1 receptor agonists represent “a transformative possibility” for psychiatric medicine.
GLP-1 medications are not approved for any psychiatric condition. Do not take them for anxiety or depression. If you happen to experience mental health improvements alongside weight loss, that’s a welcome side benefit, not the indication.
If You’re Using Compounded Semaglutide or Tirzepatide
As of February 2026, the FDA maintains active warnings about unapproved GLP-1 products. Their concerns include dosing errors, temperature/shipping problems, fraud (counterfeit products), salt forms that haven’t been evaluated for safety, and adverse events that are harder to report or trace.
Why this matters for anxiety specifically
If you’re using a compounded GLP-1 and experiencing anxiety, you have an additional variable: you may not be getting the dose you think you’re getting.
- Overdosing can intensify GI side effects, which create the anxiety cascade (nausea → not eating → low blood sugar → anxiety symptoms).
- Underdosing followed by correct dosing can feel like an abrupt increase, triggering the acute anxiety response.
- Incorrect salt forms may have different pharmacokinetic profiles — meaning they’re absorbed differently.
How to evaluate your compounded product
- Is it from a state-licensed compounding pharmacy (not a “wellness center” or online reseller)?
- Did it arrive temperature-controlled (cold chain maintained)?
- Are dosing instructions clear and specific (not vague)?
- Does the pharmacy have a verifiable physical address and pharmacist-in-charge?
- Red flags: spelling errors on packaging, claims it’s “research use only,” no pharmacy license number, prices dramatically below market rate.
How to Start (or Continue) a GLP-1 If You Have Anxiety: A Step-by-Step Plan
Before your first dose
- Establish a baseline. Rate your anxiety 0–10 for a week before starting. This gives you (and your prescriber) a reference point.
- Tell your prescriber about your mental health history. All of it. Including medications, previous episodes, and current symptoms.
- Set up a tracking system. A simple daily log: anxiety level, sleep quality, food intake, hydration, caffeine, injection date.
- Identify your “check-in” person. A partner, friend, or therapist who can give you honest feedback about behavior changes you might not notice yourself.
- Optimize sleep and hydration before starting. You’ll be better equipped to handle any adjustment symptoms if your baseline is solid.
The first 4 weeks
- Expect GI side effects. Nausea is the most common. Have anti-nausea strategies ready.
- Eat enough. The appetite suppression can be dramatic. Eating too little is the fastest route to the anxiety cascade.
- Watch dose-escalation timing. If anxiety spikes after a dose increase, note the pattern. Your prescriber may slow the titration schedule.
- Don’t add other big changes. This isn’t the week to start intermittent fasting, a new exercise program, and a caffeine detox simultaneously.
Ongoing
- Each dose increase is a new potential trigger window. Treat it like a mini re-start — monitor closely for 1–2 weeks after each escalation.
- If symptoms cluster around dose increases and resolve between them, discuss slower titration with your prescriber. Not everyone needs to be on the highest dose.
What to Tell Your Prescriber (Copy-Paste Scripts)
We know it can be hard to articulate what you’re feeling, especially when you’re anxious. Here are templates you can message or bring to your appointment.
The 60-second message
“Since starting [medication name] at [dose] on [date], I’ve been experiencing [specific symptoms — e.g., increased anxiety, racing heart, trouble sleeping, panic-like episodes]. Symptoms started [when] and have been [improving / stable / worsening]. I’ve been tracking and can share details. I’ve ruled out [dehydration / caffeine changes / skipping meals — whatever applies]. I’m also currently taking [list psychiatric medications if any]. Can we discuss whether this is an adjustment response, a medication interaction, or something that needs a different approach?”
If you suspect a medication interaction
“I take [SSRI/SNRI/benzodiazepine/stimulant name] orally. Since starting the GLP-1, it feels like my [psychiatric medication] isn’t working as well. I’ve read that GLP-1s can affect oral medication absorption through delayed gastric emptying. Could we review the timing of my medications or check whether my dose needs adjustment?”
If you want to discuss switching GLP-1s
“I’ve been on [current medication] for [duration] and have been experiencing persistent anxiety that doesn’t seem to be improving. I’ve seen data suggesting [different GLP-1] may have a different psychiatric profile. Would switching be worth trying before we consider stopping GLP-1 treatment entirely?”
Not sure if you qualify for a GLP-1?
Take our free 60-second eligibility quiz to find out.
Check Your EligibilityWhat to Do Next
You’ve made it through the most complete breakdown of GLP-1 and anxiety available anywhere. Here’s what matters most:
- If your anxiety is mild and improving: Keep tracking, optimize the basics (hydration, food, sleep, caffeine), and check in with your prescriber at your next appointment. The acute biological response may resolve on its own.
- If your anxiety is persistent or worsening: Don’t wait. Contact your prescriber. Bring your symptom data. Use the scripts above. There are options — dose adjustment, slower titration, switching medications, timing changes for other medications.
- If you’re choosing a GLP-1 provider and mental health matters to you: Not all providers are the same. The best ones screen for mental health at intake, offer regular check-ins, have clear protocols for side effect management, and either provide or refer to mental health support. See our full provider comparison →
If you need mental health support right now:
- 988 Suicide and Crisis Lifeline: Call or text 988 (U.S.)
- Crisis Text Line: Text HOME to 741741
- SAMHSA Helpline: 1-800-662-4357
You don’t have to choose between weight loss and mental health. With the right provider, the right monitoring, and the right information — which you now have — you can pursue both.
Frequently Asked Questions About GLP-1 and Anxiety
Does semaglutide cause anxiety?
The FDA's 2026 meta-analysis of 91 trials (107,910 patients) found no increased risk of anxiety with GLP-1 medications vs. placebo. However, anxiety is listed as a symptom of low blood sugar in semaglutide prescribing info, and 4% of pediatric Wegovy trial participants reported anxiety vs. 2% on placebo. Some people do experience anxiety, but direct causation hasn't been established.
Does Wegovy cause anxiety?
In clinical trials, 4% of adolescent patients (ages 12–17) on Wegovy reported anxiety compared to 2% on placebo. In adults, the STEP-8 trial showed semaglutide had a 5.6% psychiatric event rate — lower than both liraglutide (15%) and placebo (10.6%). The FDA requested removal of the suicidal ideation warning in January 2026; the label was updated in February 2026. Anxiety-like symptoms are more often related to low blood sugar, dehydration, or medication interactions.
Does Ozempic cause anxiety?
Anxiety is not listed as a standalone adverse reaction for Ozempic. It appears only in the context of low blood sugar symptoms. As the lower-dose semaglutide product (1 mg vs. Wegovy’s 2.4 mg), Ozempic has fewer reported psychiatric adverse events.
Does Zepbound or Mounjaro cause anxiety?
Anxiety is not listed as an adverse reaction in either prescribing label. Tirzepatide has less psychiatric-specific data available than semaglutide, but what exists has not raised significant signals. The FDA requested removal of the suicidal ideation warning from Zepbound in January 2026; the label was updated in February 2026.
Can GLP-1 medications cause panic attacks?
Panic attacks are not a recognized side effect in any GLP-1 prescribing information. However, increased heart rate (a class effect) combined with blood sugar fluctuations can produce symptoms that feel identical to a panic attack — shakiness, racing heart, sweating, shortness of breath, and intense fear. If you’re having panic attacks for the first time, check your blood sugar and heart rate, and contact your provider.
Should I stop my GLP-1 if I feel anxious?
No — don’t stop without medical guidance. Abrupt discontinuation can cause blood sugar spikes, rapid weight regain, and its own rebound effects. Talk to your prescriber first. Dose reduction, slower titration, or switching medications are usually tried before discontinuation.
Do GLP-1s interact with SSRIs or anxiety medications?
Yes, potentially. GLP-1s slow gastric emptying, which can delay absorption of oral medications. This is in the prescribing labels. If your anxiety medication seems less effective since starting a GLP-1, the interaction may be reducing its absorption. Contact your prescriber to discuss timing adjustments or alternative formulations.
Can GLP-1s make ADHD worse?
There’s no direct evidence that GLP-1s worsen ADHD symptoms. However, if you take oral ADHD stimulants (Adderall, Vyvanse, Ritalin), the gastric emptying effect could alter their absorption timing. Additionally, some people report difficulty concentrating when they’re not eating enough or sleeping poorly on GLP-1s — which could overlap with ADHD symptoms.
Why did the FDA remove suicide warnings from GLP-1 drugs?
In January 2026, the FDA completed a meta-analysis of 91 placebo-controlled trials covering 107,910 patients and found no increased risk of suicidal thoughts, behavior, anxiety, depression, irritability, or psychosis. They also analyzed healthcare claims data from 2.25 million patients with similar findings. Based on this, the FDA requested removal of the warnings; prescribing labels were updated in February 2026. The warnings had been inherited from older weight-loss drugs and were not specific to GLP-1s.
How long does anxiety last after starting a GLP-1?
Based on rodent research and user reports, acute anxiety from GLP-1 receptor activation may appear in the first 1–4 weeks and often improves with continued use. A FAERS-based pharmacovigilance analysis found a median time-to-onset of psychiatric adverse events for GLP-1 RAs of approximately 31 days (IQR 7–145 days). If anxiety persists beyond 6–8 weeks, worsens, or significantly impacts your daily life, don’t wait — contact your provider.
Are GLP-1 medications safe for people with pre-existing anxiety or depression?
Clinical trials largely excluded these patients, so we have limited controlled data for this specific population. Real-world evidence is mixed. Co-prescribed psychiatric medications increase the risk of interactions. Pre-existing mental health conditions are not an automatic disqualifier for GLP-1 treatment, but they require careful screening, monitoring, and a provider who takes mental health seriously alongside weight management.
Can GLP-1 drugs actually improve anxiety or depression?
Emerging evidence says possibly. In a Taiwanese nationwide cohort of adults with diabetes, GLP-1 RA use — especially beyond 180 days — was associated with lower anxiety diagnoses. Epic Research data showed lower anxiety diagnoses among semaglutide users. Researchers are studying GLP-1s for psychiatric conditions including bipolar disorder and substance use disorders. The chronic biological effect may be beneficial even if the initial acute effect increases anxiety. But GLP-1s are not approved for psychiatric treatment.
What about "Ozempic personality" and emotional blunting?
Some users report feeling emotionally flat, losing interest in activities, or personality changes. GLP-1 receptors exist in the brain’s reward center (nucleus accumbens) and dopamine pathways, providing biological plausibility. But human evidence is mostly anecdotal. If you’re experiencing this, track it and talk to your prescriber. Don’t stop medication abruptly.
Are compounded GLP-1s riskier for mental health?
Not necessarily for mental health specifically, but compounded products introduce dosing uncertainty that can amplify anxiety-producing side effects. Overdosing can intensify GI distress and low blood sugar. Underdosing followed by correct dosing can feel like a sudden increase. The FDA warns about quality, safety, and fraud concerns with compounded GLP-1 products.
What's the safest way to get GLP-1 medications?
FDA-approved products (Ozempic, Wegovy, Mounjaro, Zepbound, Saxenda, Rybelsus) from licensed pharmacies offer the most consistent dosing and quality. If you’re considering a telehealth provider, look for ones that prescribe FDA-approved products, screen for mental health, and offer regular follow-up — not just auto-refills.
Can GLP-1s cause cancer?
This is outside the scope of this article but worth noting: GLP-1 prescribing labels include warnings about thyroid C-cell tumors based on rodent studies. The relevance to humans is uncertain. Discuss any concerns with your prescriber.
What is the 108% increased risk of anxiety finding?
A 2024 observational cohort study (Scientific Reports) of 162,253 propensity-score-matched patients found GLP-1 users had a 108% increased risk of anxiety diagnoses. However, this is an association, not proof of causation. The study couldn’t control for increased medical surveillance, concurrent medications, or the psychological effects of rapid weight loss. The FDA’s controlled trial data did not confirm this signal.
Does GLP-1 affect serotonin in the brain?
Yes. Research shows GLP-1 receptors are present in the amygdala and dorsal raphe nucleus (the main hub for serotonin production). A 2016 study found that acute GLP-1 receptor activation altered serotonin signaling in the amygdala, which may explain both the initial anxiety response and the longer-term mood improvements some users experience.
Is anxiety more common with semaglutide or tirzepatide?
There isn’t enough head-to-head psychiatric data to definitively answer this. Semaglutide has more psychiatric safety data available (including the STEP trial post-hoc analysis). In the STEP-8 trial, semaglutide had a 5.6% psychiatric event rate vs. liraglutide’s 15%. Tirzepatide has not prominently flagged anxiety in its trials, but less data doesn’t mean better — it means we know less.
What should I tell my doctor about GLP-1 and anxiety?
Tell them your specific symptoms, when they started, what medications you take (including psychiatric medications), and any patterns you’ve noticed (e.g., worse after dose increases, worse when you haven’t eaten). Ask specifically: "Could my GLP-1 be affecting how my medications absorb?" and "Should we adjust timing or formulations?"
Sources
Every factual claim in this article is cited below. We prioritize randomized controlled trials and FDA communications over observational studies and social media analysis. Where evidence is mixed, we say so.
- FDA Drug Safety Communication (January 13, 2026). “FDA Requests Removal of Suicidal Behavior and Ideation Warning from Glucagon-Like Peptide-1 Receptor Agonist (GLP-1 RA) Medications.” fda.gov
- Wegovy Prescribing Information. Novo Nordisk. Current version. novo-pi.com/wegovy.pdf
- Zepbound Prescribing Information. Eli Lilly. Current version. pi.lilly.com/us/zepbound-uspi.pdf
- Saxenda Prescribing Information. Novo Nordisk. Revised 02/2026. novo-pi.com/saxenda.pdf
- Anderberg RH, Richard JE, Hansson C, et al. “GLP-1 is both anxiogenic and antidepressant; divergent effects of acute and chronic GLP-1 on emotionality.” Psychoneuroendocrinology. 2016;65:54-66.
- Wadden TA, Brown GK, Egebjerg C, et al. “Psychiatric Safety of Semaglutide for Weight Management.” JAMA Internal Medicine. 2024. jamanetwork.com
- Kornelius E, et al. “The risk of depression, anxiety, and suicidal behavior in patients with obesity on glucagon-like peptide-1 receptor agonist therapy.” Scientific Reports. 2024. nature.com
- Schoretsanitis G, Weiler S, Barbui C, Raschi E, Gastaldon C. “Disproportionality Analysis From World Health Organization Data on Semaglutide, Liraglutide, and Suicidality.” JAMA Network Open. 2024;7(8):e2423385. jamanetwork.com
- Epic Research. “Most GLP-1 Medications Correlated With a Lower Likelihood of Anxiety and Depression Diagnoses.” 2024. epic.com
- Arillotta D, et al. “GLP-1 Receptor Agonists and Related Mental Health Issues; Insights from a Range of Social Media Platforms.” Brain Sciences. 2023;13(11):1503.
- Sa M, et al. “Psychiatric effects of GLP-1 receptor agonists: A systematic review.” Diabetes, Obesity and Metabolism. 2026.
- French nationwide case-time-control study. “Suicide and suicide attempt in users of GLP-1 receptor agonists.” Lancet eClinicalMedicine. 2024.
- Tsai WH, Sung FC, Chiu LT, et al. “Decreased Risk of Anxiety in Diabetic Patients Receiving Glucagon-like Peptide-1 Receptor Agonist.” Frontiers in Pharmacology. 2022;13:765446. pubmed.ncbi.nlm.nih.gov
- FDA. “FDA’s Concerns with Unapproved GLP-1 Drugs Used for Weight Loss.” Updated 2025. fda.gov
- NPR. “As Ozempic use grows, so do reports of possible mental health side effects.” September 2023.
- Primary Care Companion CNS Disord. “Efficacy of GLP-1 Agonists in Psychiatric Illnesses: A Scoping Review.” 2025;27(3).
- McIntyre RS. “Transformation 2.0: The GLP-1 RAs as Psychiatric Medications?” Psychiatric Times. July 2025.
- Zheng W, et al. “Psychiatric adverse events associated with GLP-1 receptor agonists: A FAERS-based pharmacovigilance analysis.” Frontiers in Pharmacology. 2024. pmc.ncbi.nlm.nih.gov
How We Keep This Guide Accurate
- Primary source verification. Every clinical claim traces back to a published study, FDA communication, or prescribing label.
- Label monitoring. We check prescribing information for Wegovy, Ozempic, Zepbound, Mounjaro, and Saxenda when FDA labeling changes are announced.
- Study tracking. We monitor PubMed for new GLP-1 psychiatric safety research and update the evidence map when significant studies are published.
- Update log. We record what changed and when, so you can see the editorial history.
Changelog: February 2026 — Initial publication. Reflects FDA January 2026 meta-analysis and label updates (prescribing information updated 02/2026). All prescribing information verified against current versions. 18 studies reviewed and cited.
Medical Disclaimer: This article is for informational purposes only and does not constitute medical advice. Always consult your healthcare provider before starting, stopping, or changing any medication. If you are experiencing suicidal thoughts or a mental health crisis, call 988 (Suicide and Crisis Lifeline) or go to your nearest emergency room.
Related Articles
Cons of GLP-1
Honest overview of GLP-1 medication downsides including side effects, risks, and limitations.
GLP-1 SOS: Side Effect Relief
Interactive tool to find immediate relief strategies for common GLP-1 side effects.
GLP-1 Nausea: What to Eat
Foods and strategies to reduce nausea while taking GLP-1 receptor agonist medications.
GLP-1 Constipation Relief
Effective dietary and lifestyle strategies for relieving constipation caused by GLP-1 medications.
Best Supplements to Take With GLP-1
Evidence-based supplement guide for GLP-1 users: protein, multivitamins, fiber, what to avoid, and when to get labs instead.
GLP-1 Heartburn Foods
Best and worst foods for managing heartburn and acid reflux on GLP-1 medications.