For informational purposes only—not medical advice.
Verified against FDA prescribing information | Sources: FDA.gov, NIH/PMC, clinical trial data | Written by WPG Research Team
How to Take GLP-1 Safely: The Complete Checklist for Every Medication

Taking a GLP-1 medication safely comes down to five things: use a legitimate prescription from a licensed provider, follow your dose escalation schedule exactly, inject or take it correctly, manage side effects before they become problems, and know the warning signs that need medical attention. If you get those five right, you're ahead of most people starting these medications.
This guide covers every safety step for semaglutide (Ozempic, Wegovy), tirzepatide (Mounjaro, Zepbound), liraglutide (Saxenda), dulaglutide (Trulicity), and oral formulations (Rybelsus, oral Wegovy) — with verified dose schedules, a side effect triage chart, missed dose rules, storage tables, and a printable safety checklist. Every dosing detail has been verified against current FDA prescribing information.
But here's what most guides won't tell you: the biggest safety risks aren't the scary headlines about thyroid tumors or pancreatitis. They're the quiet mistakes — skipping a dose level to “speed up” results, not drinking enough water, ignoring nausea until you're dehydrated, or using a compounded product without verifying the source. Those are the things that actually send people to the ER. So let's make sure that doesn't happen to you.
Your Medication at a Glance
Before anything else, confirm what you're taking. This matters more than you think — different GLP-1 medications have different injection frequencies, dose schedules, and storage rules.
| Medication | Brand Names | How You Take It | How Often | Starting Dose | One Thing to Know |
|---|---|---|---|---|---|
| Semaglutide | Ozempic | Pre-filled pen | Once weekly | 0.25 mg | FDA-approved for type 2 diabetes |
| Semaglutide | Wegovy (injection) | Pre-filled pen | Once weekly | 0.25 mg | FDA-approved for weight management |
| Semaglutide | Rybelsus | Oral tablet | Daily | 3 mg | Must take on empty stomach with 4 oz water or less |
| Semaglutide | Wegovy (pill) | Oral tablet | Daily | 1.5 mg | FDA-approved December 2025 for weight loss |
| Tirzepatide | Mounjaro | Pre-filled pen | Once weekly | 2.5 mg | FDA-approved for type 2 diabetes |
| Tirzepatide | Zepbound | Pre-filled pen | Once weekly | 2.5 mg | FDA-approved for weight management |
| Liraglutide | Saxenda | Pre-filled pen | Once daily | 0.6 mg | Carries black box warning re: thyroid C-cell tumors |
| Liraglutide | Victoza | Pre-filled pen | Once daily | 0.6 mg | FDA-approved for type 2 diabetes |
| Dulaglutide | Trulicity | Pre-filled pen | Once weekly | 0.75 mg | Hidden needle design — good for needle anxiety |
Source: FDA prescribing information for each medication. Last verified February 2026.
If your medication isn't on this list — especially if it came as “drops,” an “oral liquid,” or something labeled “for research use only” — read the legitimacy section below before taking anything.
Looking for a licensed GLP-1 provider? We've compared the major telehealth programs on medical oversight, pricing, and speed — see which one fits your situation.
The 5-Step GLP-1 Safety Checklist
Print this. Screenshot it. Tape it to your fridge. These five steps prevent the vast majority of problems people run into with GLP-1 medications.
Step 1: Confirm your medication is legitimate.
You have a prescription from a licensed provider. Your medication comes from a state-licensed pharmacy. The label matches what your provider prescribed. There are no red flags (misspellings, wrong addresses, unfamiliar pharmacy names). If anything feels off, call your pharmacy before using it.
Step 2: Follow your dose schedule exactly.
Start at the lowest dose. Increase only at your prescriber's interval (weekly for Saxenda/Victoza, typically 4-week steps for once-weekly injections). Never skip a dose level to “catch up” or “get faster results.” Never double up on a missed dose.
Step 3: Take it correctly.
For injections: right site, right technique, rotate locations. For oral tablets: empty stomach, small sip of water, wait 30 minutes before eating or drinking anything else. Small details here make a big difference.
Step 4: Prevent the common problems before they start.
Stay well hydrated — it's easy to drink less on GLP-1s, especially if you're eating less or feeling nauseated (many people target ~64 oz per day, unless your clinician has you on fluid restrictions). Eat smaller, protein-rich meals. Eat slowly. Get at least 25 grams of fiber. These habits prevent the nausea, constipation, and dehydration that derail most people in the first month.
Step 5: Know when something is normal and when it's not.
Mild nausea in the first week? Normal. Severe abdominal pain radiating to your back? That's an emergency. The triage chart below tells you exactly which category your symptoms fall into.
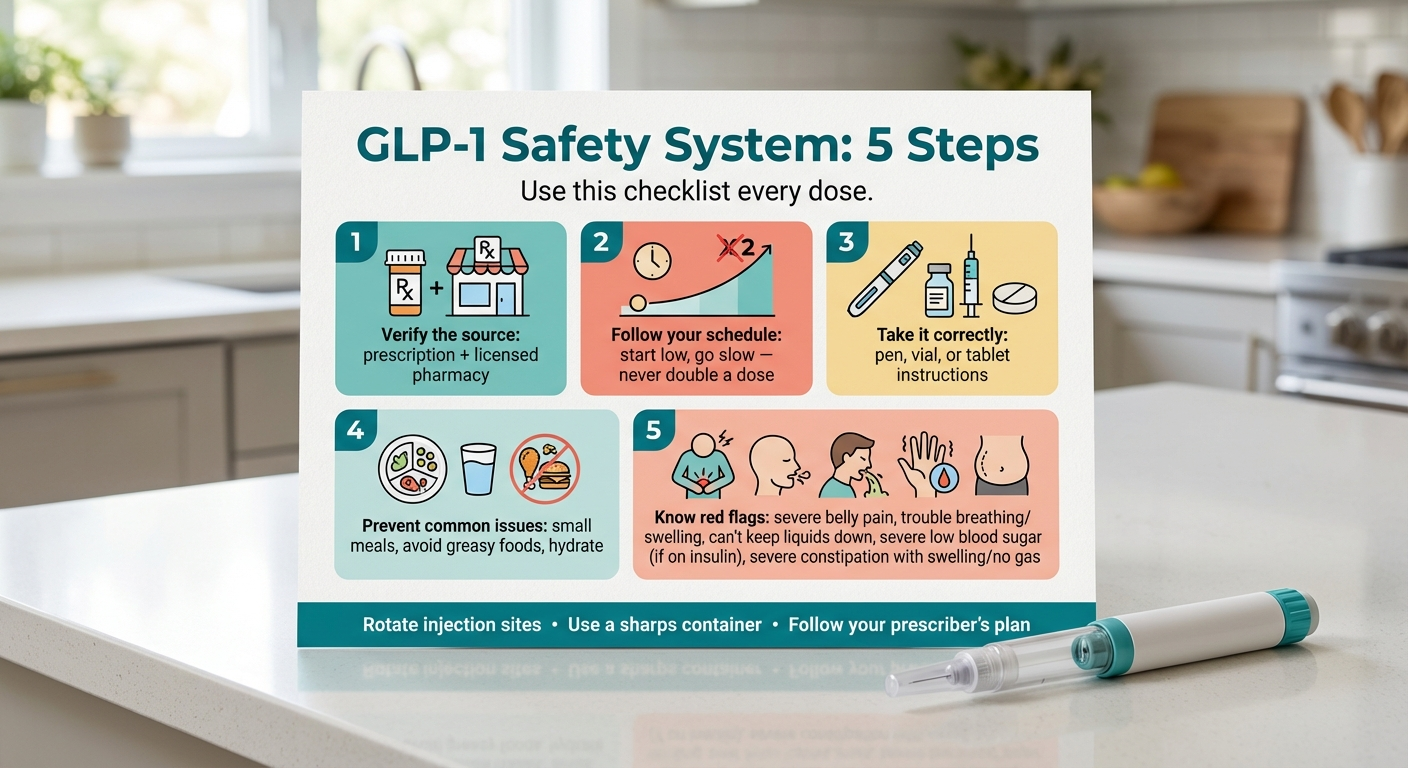
The 5-step GLP-1 safety checklist: legitimate source, correct dose schedule, proper technique, prevention, and knowing warning signs.
Illustrations are for education; product appearance and packaging may vary.
Need help with Step 1? Our provider comparison guide reviews the top GLP-1 telehealth programs on safety, medical screening quality, and cost.
How Do You Inject a GLP-1 Medication Safely? (Pre-Filled Pen)
If you're using Ozempic, Wegovy, Mounjaro, Zepbound, Saxenda, or Trulicity, your medication comes in a pre-filled pen with a tiny, thin needle (30-32 gauge — thinner than a standard sewing needle). Most people are surprised by how little it hurts. The anxiety beforehand is almost always worse than the actual injection.
What You Need
- Your medication pen (check the label: correct medication name, correct dose, not expired)
- Alcohol swabs
- A sharps container for needle disposal (a rigid, puncture-proof container — you can buy one at any pharmacy, or use an empty laundry detergent bottle in a pinch)
- A timer or watch (some pens require you to hold for a specific count)
Before You Inject
Take the pen out of the refrigerator 10-15 minutes before your injection. Room-temperature medication stings less. Leave the cap on during this time.
Check the solution through the pen window. It should be clear and free of particles; color may be colorless or slightly yellow depending on the product (Mounjaro and Zepbound, for example, can be slightly yellow — that's normal). If it looks cloudy, has particles floating in it, or is discolored beyond what your label describes — do not use it. Contact your pharmacy for a replacement.
Wash your hands thoroughly with soap and water.
Pick Your Device Type
GLP-1 pens fall into two categories. The injection steps differ, so use the right set for your pen.
Type A: Dial-a-Dose Pen With Attachable Needle (Ozempic, Saxenda, Victoza)
These are multi-dose pens — you attach a new needle and dial your dose before each injection.
- Remove the pen cap. Set it aside.
- Attach a new needle to the pen tip and remove the outer and inner needle caps.
- Prime the pen (first use of a new pen only). Dial to the flow-check symbol and press the button until a drop appears at the needle tip. This removes air and confirms the pen is working.
- Dial your prescribed dose on the dose counter.
- Choose your injection site. Three options:
- Abdomen — at least 2 inches from your belly button. Most popular site. Easy to reach, usually least painful.
- Front of thigh — middle area. Good alternative if your abdomen is tender.
- Back of upper arm — you may need someone to help with this one.
- Clean the injection site with an alcohol swab. Let it air dry completely (injecting through wet alcohol stings).
- Pinch a fold of skin at the cleaned site.
- Insert the needle straight in at a 90-degree angle. Push it all the way in.
- Press the dose button and hold until the dose counter returns to “0.”
- Keep holding the button and keep the needle in your skin while you slowly count to 6. This ensures the full dose is delivered.
- After counting to 6, remove the needle. Then release the button.
- Apply gentle pressure with a cotton ball or clean finger. Do not rub the site — rubbing can cause bruising.
- Remove the needle from the pen and dispose of it in your sharps container. Never throw loose needles in the trash.
- Replace the pen cap and store properly.
Type B: Single-Dose Autoinjector Pen (Wegovy Injection, Mounjaro, Zepbound, Trulicity)
These are pre-filled, single-use pens — no needle to attach, no dose to dial. The dose is preset.
- Remove the pen cap (or base cap for Trulicity). Set it aside.
- Choose your injection site (abdomen, front of thigh, or back of upper arm — same three options as above).
- Clean the injection site with an alcohol swab. Let it air dry completely.
- Place the pen flat and firmly against your skin at a 90-degree angle.
- Start the injection based on your pen type, then keep holding it firmly against your skin until the dose is finished:
- Wegovy: Press the pen firmly against your skin to start (no button). Keep holding until the yellow bar stops moving (you may hear 2 clicks).
- Mounjaro/Zepbound: Unlock, then press and hold the button. Keep holding for 10 seconds after the second click.
- Trulicity: Unlock, then press and hold the button until the indicator shows the injection is complete.
- Remove the pen from your skin.
- Apply gentle pressure with a cotton ball or clean finger. Do not rub the site — rubbing can cause bruising.
- Dispose of the entire pen in your sharps container. These are single-use — never reuse them.
One critical rule: GLP-1 injections are subcutaneous — they go into the fatty tissue just under the skin. Never inject into a vein or muscle. The pinch-and-inject technique at a 90-degree angle keeps the medication where it needs to be.
Injection Site Rotation (Why It Matters)
Injecting in the same spot repeatedly can cause lipodystrophy — hardened lumps of fatty tissue under the skin that affect how the medication absorbs. It can also cause scarring and persistent soreness.
Use a simple rotation system:
- Week 1: Left side of abdomen
- Week 2: Right side of abdomen
- Week 3: Left thigh
- Week 4: Right thigh
- Week 5: Start over
Always inject at least 1 inch away from your previous injection site. Avoid scar tissue, bruises, stretch marks, or areas of skin irritation.
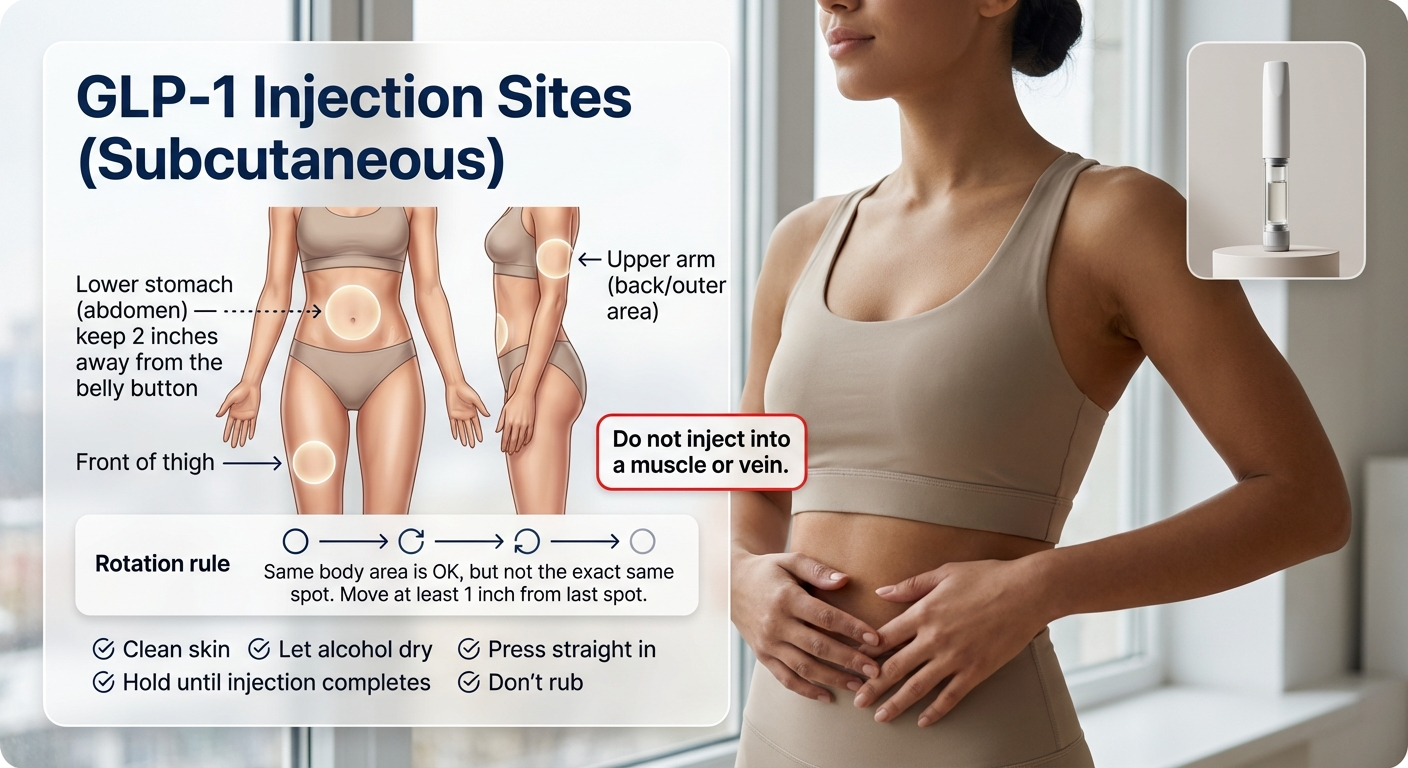
Subcutaneous injection sites for GLP-1 medications: abdomen, front of thigh, and back of upper arm.
Illustrations are for education; product appearance and packaging may vary.
Tips to Make Injections More Comfortable
- Room-temperature medication — taking it straight from the fridge makes it sting more.
- Relax your muscles — tension at the injection site increases pain. Take a slow breath.
- Ice the spot for 30 seconds before (optional) — numbs the area slightly.
- Inject steadily — don't jab quickly. A slow, steady insertion is less painful.
- Choose Trulicity if needle anxiety is severe — its pen has a completely hidden needle. You never see it.
Most patients say some version of: “I was dreading it, and then it was nothing.” The needles are genuinely tiny. Give yourself grace on the first one, and it gets easier fast.
Common Injection Mistakes to Avoid
- Reusing needles. Fresh needle every time. Reused needles are duller, increase infection risk, and can cause more pain and bruising.
- Injecting through clothing. Always inject on clean, bare skin.
- Not rotating sites. See above — lipodystrophy is a real problem.
- Forgetting to prime a new pen. This can result in an incomplete dose.
- Not holding long enough. If you pull the needle out too early, medication may leak out and you'll get less than your full dose.
How to Take GLP-1 Safely With a Vial and Syringe (Compounded)
If you received your GLP-1 medication in a vial rather than a pre-filled pen, you're most likely using a compounded formulation. This section is important because dosing errors with compounded GLP-1s are the single biggest safety concern the FDA has flagged in the past two years.
As of July 31, 2025, the FDA had received over 605 adverse event reports related to compounded semaglutide and over 545 reports for compounded tirzepatide (adverse event reports are voluntary and cannot establish how frequently problems occur). Many of these involved patients accidentally administering 5 to 20 times their intended dose because of confusion between milligrams, units, and milliliters.
That is not a typo. Five to twenty times their dose. Some of these errors required hospitalization.
The No-Guessing Rule
If your dosing instructions are not crystal clear — if you have any confusion about how many units to draw, what markings to read on the syringe, or how to convert your prescribed dose from milligrams to units — stop and call your prescriber or pharmacist before injecting. This is not a situation where “close enough” works.
What to Ask Your Pharmacy
Before your first injection from a vial, make sure you have:
- Written dosing instructions with the exact number of units to draw (not just milligrams)
- The correct syringe size for your dose (insulin syringes come in different capacities — using the wrong one makes accurate measurement harder)
- A demonstration — many pharmacies offer video walkthroughs or in-person training. Ask for one.
Vial Injection Steps
- Wash your hands.
- Clean the top of the vial with an alcohol swab.
- Clean your injection site with a separate alcohol swab.
- Remove the syringe caps — first the plunger end, then the needle cap. Be careful with the needle.
- Draw air into the syringe equal to your dose volume.
- Insert the needle into the vial, push the air in (this prevents a vacuum).
- Flip the vial upside down and slowly pull the plunger to draw your prescribed number of units.
- Check for air bubbles. If you see any, gently tap the syringe barrel (don't hit it hard — you'll bend the needle) and push the air out. Readjust to your correct dose mark.
- Remove the syringe from the vial.
- Pinch skin at your injection site and inject at a 90-degree angle, just like the pen instructions above.
- Hold for 5-10 seconds, then remove.
- Dispose of the syringe in your sharps container.
Red Flags With Compounded Products
The FDA has identified specific concerns with compounded GLP-1 medications that you should know about:
- Warm shipments: Injectable GLP-1 medications require refrigeration. The FDA has received complaints about compounded products arriving warm or with inadequate ice packs. If your medication arrives warm — do not use it. Contact your pharmacy for a replacement.
- Unapproved salt forms: Some compounders have used semaglutide sodium or semaglutide acetate, which are different active ingredients than what's in FDA-approved products.
- Fraudulent labels: The FDA has identified compounded products with fake pharmacy names and addresses on the labels. Verify that the pharmacy on your label actually exists and is state-licensed.
- “For research use only” products: This is a massive red flag. Legitimate GLP-1 medications require a prescription and come from a licensed pharmacy. If something is labeled “for research use,” it is not intended for human injection.
Sources: FDA safety communication on compounded semaglutide dosing errors; FDA concerns with unapproved GLP-1 drugs (fda.gov); FDA warning letters issued in fall 2025 related to non-FDA-approved GLP-1 drugs.
How to Take Oral GLP-1 Tablets Safely (Rybelsus and Oral Wegovy)
Not everyone takes a GLP-1 by injection. Two oral options exist:
- Rybelsus (semaglutide 3 mg, 7 mg, or 14 mg tablets) — FDA-approved for type 2 diabetes
- Oral Wegovy (semaglutide 25 mg tablets) — FDA-approved in December 2025 for weight management. This is the first oral GLP-1 pill approved specifically for weight loss.
Oral semaglutide has strict rules that matter for it to work. This isn't like swallowing a vitamin — if you don't follow the protocol, the medication may not absorb properly and you'll get little to no benefit.
The Oral Semaglutide Rules (Non-Negotiable)
Take it first thing in the morning on a completely empty stomach. Before coffee. Before juice. Before anything.
Swallow the tablet whole with no more than 4 ounces of plain water (about half a glass). Not a full glass. Not juice. Not coffee. Plain water, small sip.
Do not crush, chew, or split the tablet.
Wait at least 30 minutes before eating, drinking anything else, or taking other oral medications. This waiting period is critical for absorption.
Why These Rules Exist
Semaglutide is a peptide — a small protein. Your stomach acid would normally destroy it before it could be absorbed. The tablet contains a special absorption enhancer called SNAC that creates a brief window for the medication to pass through your stomach lining. This only works reliably when your stomach is empty, the water volume is small, and no food or other substances are competing for absorption. If you eat too soon, drink too much water, or take it with other medications — the drug may not absorb, and you've essentially wasted a dose.
Common Oral GLP-1 Mistakes
- Drinking a full glass of water with the tablet (use 4 oz or less)
- Taking it with coffee or other beverages instead of water
- Taking other morning medications at the same time (wait 30 minutes)
- Taking it after a snack or not on a fully empty stomach
- Storing tablets outside the original bottle (moisture degrades them)

Oral semaglutide morning protocol: empty stomach, 4 oz water or less, wait 30 minutes before eating or other medications.
Illustrations are for education; product appearance and packaging may vary.
Sources: Rybelsus prescribing information (FDA); Oral Wegovy prescribing information (FDA); Wegovy.com.
What Is the Correct GLP-1 Dose Schedule?
Every GLP-1 medication follows a “start low, go slow” dose escalation. This is not optional. Skipping dose levels to speed up weight loss is the fastest way to end up with severe nausea, vomiting, dehydration, and potentially a trip to the ER. Your body needs time to adjust at each level.
All GLP-1s use a “start low, go slow” approach, but the timing differs by medication:
- Most once-weekly injections step up in 4-week intervals.
- Liraglutide (Saxenda/Victoza) steps up weekly.
- Oral semaglutide tablets step up in 30-day intervals.
A) Once-Weekly Injections (Minimum Titration Intervals)
Your provider may hold you at any dose longer based on tolerability.
| Medication | Start | Step-Ups (Minimum) | Maintenance |
|---|---|---|---|
| Wegovy (injection) | 0.25 mg weekly x 4 weeks | 0.5 x4 → 1.0 x4 → 1.7 x4 → 2.4 | 2.4 mg weekly |
| Zepbound / Mounjaro (tirzepatide) | 2.5 mg weekly x 4 weeks | 5 x4 → 7.5 x4 → 10 x4 → 12.5 x4 → 15 x4 | 5 / 10 / 15 mg weekly |
| Ozempic | 0.25 mg weekly x 4 weeks | 0.5 x4 → 1.0 x4 (if needed) → 2.0 x4 (if needed) | 0.5–2.0 mg weekly |
| Trulicity | 0.75 mg weekly | May increase to 1.5 (after ≥4 wk) → 3 (after ≥4 wk) → 4.5 (after ≥4 wk) | 0.75–4.5 mg weekly |
B) Once-Daily Injection (Weekly Titration)
| Medication | Week 1 | Week 2 | Week 3 | Week 4 | Week 5+ |
|---|---|---|---|---|---|
| Saxenda (liraglutide) | 0.6 mg daily | 1.2 mg daily | 1.8 mg daily | 2.4 mg daily | 3.0 mg daily |
C) Oral Semaglutide Tablets (30-Day Titration)
| Medication | First 30 Days | Next 30 Days | Then |
|---|---|---|---|
| Rybelsus | 3 mg daily | 7 mg daily | 14 mg daily (if needed) |
| Wegovy (tablets) | 1.5 mg daily | 4 mg daily | 9 mg daily (30 days) → 25 mg daily |
Source: FDA prescribing information for each medication. Each dose increase represents the minimum interval — your provider may keep you at any level longer based on your response and tolerability.
Dose Escalation Safety Rules
Never skip a dose level. Going from 0.25 mg straight to 1 mg of semaglutide, for example, dramatically increases nausea and vomiting. The gradual increase exists for a reason.
Each level needs at least its prescribed interval (4 weeks for most weekly injections; weekly for Saxenda). Some people need 6-8 weeks at a step. If side effects are rough, stay at your current dose longer — or even drop back one level. This is medicine, not a race.
You may not need the maximum dose. Many patients get excellent results at mid-range doses. The goal is the lowest effective dose that gives you meaningful appetite control and weight loss with tolerable side effects. Not everyone needs to reach the top.
If your provider prescribed a different schedule — follow theirs. Compounded formulations may use different concentrations. Some providers extend each step based on your history. Individual adjustment is good medicine, not a cause for concern.
A note on tirzepatide (Mounjaro/Zepbound): Unlike semaglutide, which has one target maintenance dose (2.4 mg for weight loss), tirzepatide offers three maintenance dose options — 5 mg, 10 mg, or 15 mg. Your provider will help you find the level that balances results with how you feel. There's no requirement to reach 15 mg.
GLP-1 Side Effects: What's Normal, What's Not, and When to Get Help
This is the section that might save you an unnecessary ER visit — or make sure you get to one when you actually need it. Side effects are common with GLP-1 medications, especially in the first few weeks and after each dose increase. Most are mild and temporary. A few are serious. Knowing the difference matters.
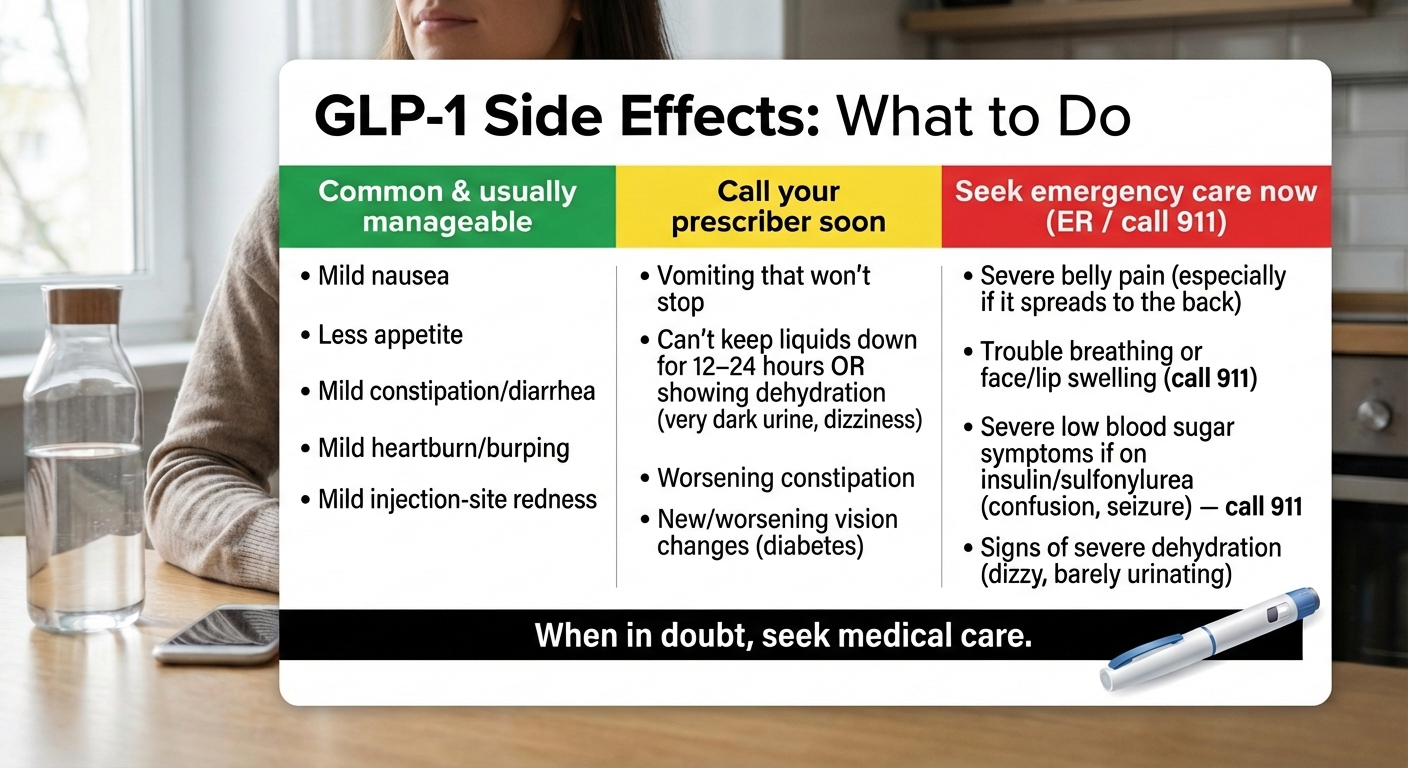
GLP-1 side effect triage chart: green (manage at home), yellow (call your provider), red (seek emergency care).
Illustrations are for education; product appearance and packaging may vary.
Normal — Manage at Home
These are common, especially in the first few weeks and after dose increases. They usually improve as your body adjusts.
| What You're Feeling | Why It's Happening | What to Do About It |
|---|---|---|
| Mild nausea | Your stomach is emptying more slowly — this is the medication working. Your body hasn't adjusted yet. | Eat smaller meals. Avoid greasy and fried food. Try ginger tea or ginger chews. Eat slowly — give your brain 20 minutes to register fullness. |
| Reduced appetite | This is the primary mechanism of GLP-1 medications. It's supposed to happen. | Focus on nutrient-dense food. Prioritize protein (aim for 60-100g/day). Don't skip meals entirely — eat less, but eat well. |
| Mild constipation | Slowed GI motility + most people don't drink enough water on GLP-1s. | Stay well hydrated (many people target ~64 oz/day, unless your clinician has you on fluid restrictions). Get 25+ grams of fiber (food or supplement). Try Miralax if lifestyle changes aren't enough. |
| Mild diarrhea | GI system adjusting in the early weeks. | Stay hydrated. Stick to bland foods temporarily. Usually resolves within 1-2 weeks. |
| Fatigue (first 1-2 weeks) | Your body is adjusting to lower caloric intake + the medication itself. | Rest when needed. Hydrate. Make sure you're actually eating enough — some people undereat dramatically in the first week. |
| Injection site redness or itching | Mild local reaction to the needle or medication. | Rotate injection sites. Apply a cool compress. Should resolve within hours. |
| Burping or mild heartburn | Slower stomach emptying can increase reflux. | Eat smaller portions. Stay upright for 30+ minutes after eating. Avoid carbonated drinks. |
| Mild headache | Often related to dehydration or caloric adjustment. | Drink more water. Seriously — this is the answer to half of early GLP-1 side effects. |
Call Your Provider (Within 24 Hours)
These need medical guidance but typically aren't emergencies.
| What You're Experiencing | Why It's Concerning | What to Do |
|---|---|---|
| Nausea or vomiting lasting more than 3 consecutive days | Prolonged vomiting risks dehydration, which can damage your kidneys. | Call your provider. They may reduce your dose, extend your current dose level, or prescribe an anti-nausea medication. |
| Unable to keep food or fluids down for more than 24 hours | Dehydration risk is now significant. | Call your provider urgently. You may need IV fluids. |
| Rapid, unexpected weight loss (more than 5 lbs in one week at a stable dose) | Could indicate excessive medication effect, dehydration, or an underlying issue. | Report to your provider for evaluation. |
| Persistent resting heart rate above 100 bpm | GLP-1s can cause a small increase in heart rate. Persistently high rates should be evaluated. | Have your provider check. Usually not dangerous, but needs monitoring. |
| Significant hair thinning | Related to rapid weight loss (telogen effluvium), not the drug directly. Similar to hair loss after bariatric surgery. | Discuss with your provider. Usually temporary. Ensure adequate protein and nutrition. |
| Changes in vision | In diabetic patients, rapid blood sugar improvement can temporarily worsen diabetic retinopathy. | See your provider promptly. An eye exam may be needed before continuing. |
| Pain in upper right abdomen, especially after fatty meals | Possible gallbladder issue. GLP-1s are associated with a modest increase in gallbladder events (related to rapid weight loss, not the drug itself). | Your provider should evaluate. You may need imaging. |
| Unusual mood changes, increased anxiety, or depression | Rare but reported. The mechanism isn't fully understood. Not consistently seen in clinical trials, but worth tracking. | Contact your provider. Keep a symptom journal for your visit. |
Seek Emergency Care Now
These are rare but serious. Do not wait.
| What's Happening | What It Might Be | What to Do Right Now |
|---|---|---|
| Severe abdominal pain radiating to your back, with or without vomiting | Acute pancreatitis — inflammation of the pancreas. | Stop the medication. Go to the ER immediately. |
| Swelling of face, lips, tongue, or throat; difficulty breathing; rapidly spreading rash | Severe allergic reaction (anaphylaxis) | Call 911. |
| Confusion, seizure, loss of consciousness (especially if also taking insulin or sulfonylureas) | Severe hypoglycemia — dangerously low blood sugar | Call 911. Administer glucagon if available. |
| Lump or swelling in the neck; persistent hoarseness; difficulty swallowing; unexplained shortness of breath | Possible thyroid issue (all GLP-1s carry a boxed warning based on rodent studies) | See a doctor urgently. Most likely nothing, but it must be evaluated. |
| Signs of severe dehydration: very dark urine, dizziness when standing, inability to urinate, confusion | Acute kidney injury risk from dehydration caused by persistent GI symptoms | Go to the ER. You may need IV fluids and kidney function testing. |
| Severe constipation with abdominal distension, inability to pass gas, and increasing pain | Possible bowel obstruction (very rare) | Go to the ER. |
Sources: FDA prescribing information (Wegovy, Ozempic, Mounjaro, Zepbound, Saxenda); Cleveland Clinic GLP-1 side effects overview; PMC: Adverse Effects of GLP-1 Receptor Agonists.
What to Eat (and Avoid) on GLP-1 Medications
Your appetite is going to decrease. That's the point. But when you're eating less, every calorie has to count more. The people who do best on GLP-1 medications are intentional about what they eat — not obsessive, just intentional.
The Priority Order
Think of your plate in this order:
- Protein first. This is non-negotiable. Studies show that up to 25-40% of weight lost on GLP-1 medications can be lean muscle mass — unless you actively protect it with adequate protein and resistance training. Aim for 60-100 grams per day, spread across meals. Chicken, fish, eggs, Greek yogurt, cottage cheese, tofu, lean beef, legumes.
- Vegetables and fiber. Fiber helps prevent constipation (one of the most common side effects), feeds your gut microbiome, and keeps you feeling satisfied. Aim for at least 25 grams daily. Vegetables, berries, legumes, whole grains. If you can't hit it through food alone, a fiber supplement like psyllium husk helps.
- Healthy fats. Avocado, olive oil, nuts, seeds. In moderation — fats are calorie-dense and you're eating less overall.
- Complex carbohydrates last. Whole grains, sweet potatoes, brown rice. Not eliminated, just deprioritized.
Foods That Help Reduce Side Effects
- Ginger (tea, chews, or fresh) — genuinely effective for GLP-1 nausea
- Bland, easy-to-digest foods in the first 2 weeks: crackers, toast, rice, bananas, broth, applesauce
- High-fiber foods to prevent constipation: broccoli, lentils, chia seeds, oatmeal
- Water — and lots of it. It's easy to drink less on GLP-1s — especially if you're eating less or feeling nauseated — so hydration needs extra attention. Set reminders. Get a large water bottle and keep it visible. Aim for good hydration (many people target ~64 oz per day), unless your clinician has you on fluid restrictions.
Foods and Habits That Make Side Effects Worse
- Greasy or fried food — significantly amplifies nausea, especially early on
- Large portions — your stomach empties slower now. A big meal will sit there and make you feel terrible. Eat smaller, eat more often if needed.
- Eating too fast — it takes 20+ minutes for fullness signals to reach your brain. Eating quickly leads to overeating leads to intense nausea. Slow down.
- Carbonated drinks — increase bloating and discomfort when gastric emptying is already slow
- Alcohol — amplifies nausea, increases dehydration risk, and is calorie-dense with zero nutritional value. If you drink, start with very small amounts — your tolerance will likely be lower than before.
Supplements to Consider
- Daily multivitamin — eating less means higher risk of micronutrient gaps
- Fiber supplement (psyllium husk / Metamucil) if dietary fiber is insufficient
- Probiotic — may help with GI adjustment, especially constipation
- Discuss vitamin D, calcium, and magnesium with your provider, especially for long-term use
Sources: American Journal of Clinical Nutrition GLP-1 dietary guidelines (2025); Cleveland Clinic GLP-1 diet guidance; Ohio State Wexner Medical Center GLP-1 nutrition guidelines; UCHealth nutrition guidance for GLP-1 users.
For a complete 30-day meal plan and week-by-week starter guide, see our GLP-1 Tips and Tricks for Beginners playbook.
What If You Miss a Dose?
This happens. Life gets busy, you forget, your pen was out of stock. Here's exactly what to do for each medication.
Missed Dose Rules by Medication
| Medication | If You Remember Within... | If More Time Has Passed... | Never Do This |
|---|---|---|---|
| Wegovy (weekly injection) | 5 days — take it as soon as you can, then resume your regular weekly schedule | More than 5 days — skip it and take the next dose on your regular day | Never take two doses to make up for one |
| Ozempic (weekly injection) | 5 days — take it as soon as you can | More than 5 days — skip and resume schedule | Never double up |
| Mounjaro / Zepbound (weekly injection) | 4 days (96 hours) — take it as soon as you can | More than 4 days — skip and take the next one on schedule | Never take two doses in one week |
| Trulicity (weekly injection) | 4 days — take it as soon as you can (at least 72 hours must remain before your next scheduled dose) | More than 4 days — skip and wait for next scheduled dose | Never take two doses within 3 days (72 hours) of each other |
| Saxenda (daily injection) | Same day — take the next dose at the usual time (don't double) | If more than 3 days since last dose — restart at 0.6 mg and re-titrate per your prescriber's instructions | Never take two doses in one day; contact prescriber if 3+ days missed |
| Rybelsus (daily oral) | You cannot make it up the same day (requires empty-stomach protocol) — skip and take tomorrow's dose normally | — | Never take two tablets in one day |
If you've missed multiple weeks (2+ weeks without any doses), contact your provider. You may need to restart at a lower dose level. Jumping back in at your previous higher dose after a long break can cause severe GI side effects — your body has lost its tolerance.
Sources: FDA prescribing information for Wegovy, Ozempic, Mounjaro, Zepbound, Trulicity, Saxenda, Rybelsus.
How to Store GLP-1 Medications Correctly
Improper storage can degrade the medication, reducing its effectiveness or making it unsafe. The rules are different for each product.
Storage Quick-Reference Table
| Medication | Before First Use | After First Use / Room Temp | Never | Notes |
|---|---|---|---|---|
| Ozempic | Refrigerate: 36-46 F (2-8 C) | Room temp up to 56 days (59-86 F / 15-30 C) | Freeze or exceed 86 F | Multi-dose pen; cap between uses |
| Wegovy (pen) | Refrigerate: 36-46 F (2-8 C) | Room temp up to 28 days (46-86 F / 8-30 C) | Freeze or exceed 86 F | Single-use pens; keep in original carton |
| Mounjaro / Zepbound | Refrigerate: 36-46 F (2-8 C) | Room temp up to 21 days (86 F / 30 C or below) | Freeze or exceed 86 F | Single-dose pens |
| Saxenda | Refrigerate: 36-46 F (2-8 C) | Room temp up to 30 days (59-86 F / 15-30 C) | Freeze or exceed 86 F | Multi-dose pen |
| Trulicity | Refrigerate: 36-46 F (2-8 C) | Room temp up to 14 days (86 F / 30 C or below) | Freeze or exceed 86 F | Single-dose pen |
| Rybelsus (oral) | Room temp: 68-77 F (20-25 C) | Same — room temp, keep in original bottle | Moisture exposure | Keep bottle sealed; store in a dry place |
| Wegovy (pill) | Room temp: 68-77 F (20-25 C) | Same — room temp, keep in original bottle | Moisture exposure | Keep bottle sealed, dry place |
Travel Tips
- Carry medication in your carry-on luggage — never in checked bags. Cargo hold temperatures can freeze injectable medications.
- Use an insulated medication travel case for temperature control. Don't place pens directly on ice packs — put a cloth or towel between them.
- TSA allows injectable medications and needles in carry-on luggage when properly labeled. Bring your prescription or a letter from your provider for smooth screening.
- Hot cars will ruin your medication. Don't leave pens in the car, trunk, or glove compartment. Take them with you.
- If your medication arrived warm or without proper cold packing — contact the pharmacy for guidance before using it. Many injectable GLP-1 products are intended to be kept refrigerated until use (each brand has a limited room-temperature window). The FDA has flagged shipping concerns as a specific issue with compounded GLP-1 products.
Sources: FDA prescribing information for each medication; FDA safety communication on compounded GLP-1 shipping concerns; GoodRx storage guides.
Should You Take GLP-1 in the Morning or at Night?
Short answer: for weekly injections, it genuinely does not matter. Pick whatever time you'll remember consistently.
For Weekly Injections (Ozempic, Wegovy, Mounjaro, Zepbound, Trulicity)
- Many people prefer evening or right before bed — if nausea occurs, you sleep through the worst of it.
- Others prefer morning — it's done and you don't have to think about it.
- Pick one day of the week and stick with it. Set a phone alarm.
If you need to change your weekly injection day: Wegovy/Ozempic (semaglutide): fine as long as there are at least 2 days (48 hours) between injections. Mounjaro/Zepbound (tirzepatide) and Trulicity (dulaglutide): fine as long as there are at least 3 days (72 hours) between injections. Always follow your prescriber's instructions.
For Daily Injections (Saxenda)
Same time each day, your choice. Many patients prefer bedtime to sleep through early nausea.
For Oral Semaglutide (Rybelsus, Oral Wegovy)
Morning only. You must take it on an empty stomach, so first thing when you wake up is the only practical option. Keep the bottle and a small glass of water on your nightstand.
GLP-1 and Surgery: Do You Stop Before a Procedure?
This is a critical safety topic that most GLP-1 guides either skip entirely or oversimplify. GLP-1 medications slow gastric emptying — meaning food stays in your stomach longer than normal. During procedures requiring general anesthesia or deep sedation, this creates a risk of pulmonary aspiration (inhaling stomach contents into your lungs while sedated).
What Current Guidance Says
A multi-society review including the American Gastroenterological Association found that most patients can continue GLP-1 medications before elective surgery and endoscopy. However, patients with significant GI symptoms (active nausea, vomiting, bloating, or reflux) may need modifications — such as a 24-hour liquid diet before the procedure or an adjustment to the anesthesia plan.
Some institutions and the American Society of Anesthesiologists take a more conservative approach: Daily GLP-1s (Saxenda, Rybelsus): Hold on the day of surgery. Weekly GLP-1s (Ozempic, Wegovy, Mounjaro, Zepbound): Hold for at least 1 week before surgery. Some institutions recommend 2-3 weeks.
What You Should Do
- Tell your surgeon and anesthesiologist that you are taking a GLP-1 medication. Name the specific drug and dose. Don't assume they'll see it in your chart.
- Follow your surgical team's instructions — they may have specific protocols that differ from general guidance.
- If you're having any procedure requiring sedation — including colonoscopies, endoscopies, dental surgery under sedation — mention your GLP-1 use.
- Your surgical team may prescribe an extended fasting period or a liquid diet the day before.
Sources: AGA multi-society guidance on perioperative GLP-1 use; ASA consensus guidance (2024); FDA Wegovy prescribing information (2025 revision).
Who Should NOT Take GLP-1 Medications?
GLP-1 medications are safe for most people when prescribed appropriately. But there are clear situations where they should not be used. For a deeper dive, see our full GLP-1 contraindications guide.
Absolute Contraindications
- Personal or family history of medullary thyroid carcinoma (MTC) — all GLP-1 medications carry a black box warning about thyroid C-cell tumors found in rodent studies. The risk in humans is unconfirmed but the contraindication exists.
- Multiple endocrine neoplasia syndrome type 2 (MEN2)
- Known allergy to the active ingredient or any component of the medication
- Pregnancy — GLP-1 medications are not recommended in pregnancy. Semaglutide (Wegovy): stop at least 2 months before a planned pregnancy. Tirzepatide (Zepbound/Mounjaro): the U.S. label advises discontinuing when pregnancy is recognized — discuss timing and washout with your clinician if you are planning pregnancy. Use reliable birth control while taking any GLP-1 medication. If you become pregnant while taking one, contact your provider immediately.
- Breastfeeding — data varies by medication and is limited; discuss risks and benefits with your prescriber before using any GLP-1 while breastfeeding
Use With Caution (Provider Must Evaluate)
- History of pancreatitis
- History of gallbladder disease or gallstones
- Gastroparesis or severe GI motility disorders
- Severe kidney disease (dehydration from side effects can worsen kidney function)
- Diabetic retinopathy (rapid blood sugar improvement can temporarily worsen eye damage)
- Type 1 diabetes (GLP-1s are not approved for T1D)
- Active eating disorder (these medications profoundly suppress appetite and can worsen restrictive patterns — providers should screen for this)
Sources: FDA prescribing information (black box warnings); StatPearls NCBI overview; ADA 2025 Standards of Care; AGA guidelines.
Do GLP-1 Medications Interact With Other Drugs?
A few interactions matter enough to flag:
Insulin and sulfonylureas: Taking a GLP-1 with insulin or sulfonylureas increases your risk of hypoglycemia (low blood sugar). Your provider may need to reduce those doses when starting your GLP-1.
Oral birth control (especially with tirzepatide): Tirzepatide (Mounjaro, Zepbound) can reduce the effectiveness of oral hormonal contraceptives because it slows gastric emptying, affecting pill absorption. The FDA prescribing information recommends switching to a non-oral contraceptive method or adding a barrier method for 4 weeks after starting tirzepatide and for 4 weeks after each dose increase.
Hormone replacement therapy (HRT): Because GLP-1/GIP medicines can slow gastric emptying, absorption of oral HRT components — especially oral progesterone used for endometrial protection — may be less predictable. The British Menopause Society advises considering non-oral options (for example, transdermal estrogen and a non-oral progestogen strategy such as an LNG-IUD) or close monitoring when starting or increasing incretin therapy. Discuss this with your prescriber.
Warfarin and blood thinners: Monitor INR more frequently when starting or adjusting GLP-1 therapy.
Oral medications in general: Because GLP-1s slow stomach emptying, the absorption timing of other oral medications may shift. If you take critical medications like thyroid hormones or blood pressure pills, discuss timing with your provider. For oral semaglutide specifically — the 30-minute empty-stomach window means you cannot take other medications at the same time.
Sources: FDA prescribing information (Mounjaro/Zepbound, Wegovy, Ozempic); Drugs.com interaction checker; British Menopause Society advisory (2025).
How to Avoid Unsafe GLP-1 Products
The surge in GLP-1 demand has created a parallel market of risky products. In fall 2025, the FDA issued warning letters to companies compounding or manufacturing GLP-1 products with misleading claims. Here's how to protect yourself.
The “Is This Legit?” Checklist
You have a prescription from a licensed healthcare provider (MD, DO, NP, or PA)
Your medication comes from a state-licensed pharmacy (verify at your state board of pharmacy website)
The label matches what your provider prescribed — correct drug name, correct dose, correct pharmacy
The medication arrived at the proper temperature (cold, with adequate ice packs for injectables)
The pharmacy name and address on the label are real (you can call them and verify)
Red Flags That Should Stop You
Product is labeled “for research use only” or “not for human consumption”
It's called “GLP-1 drops” or “GLP-1 oral liquid” from an online retailer (these are not FDA-approved formulations)
No prescription was required
The pharmacy can't be verified through your state board
Spelling errors, incorrect addresses, or generic-looking labels
The price seems impossibly cheap compared to market rates
It arrived warm with no cold packing
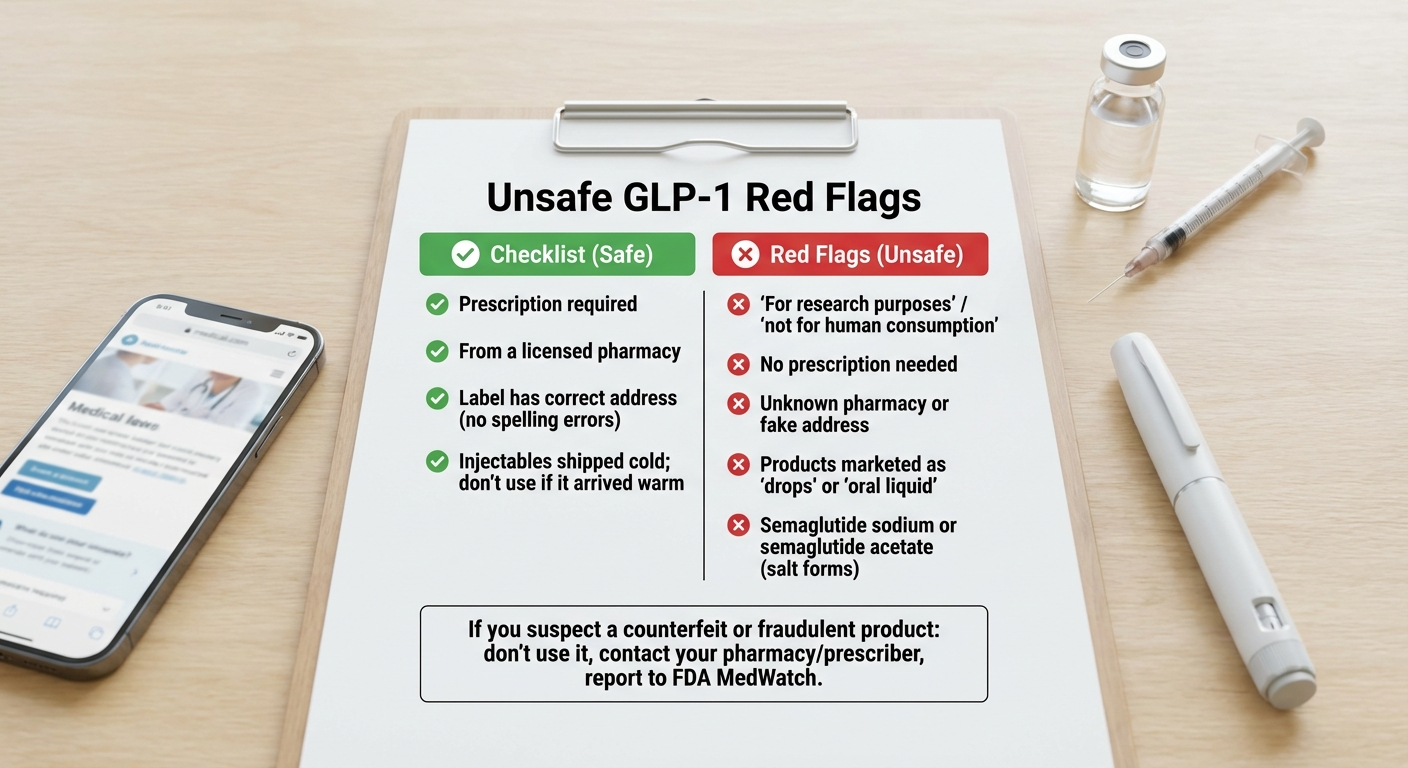
Red flags checklist: how to identify unsafe or counterfeit GLP-1 products.
Illustrations are for education; product appearance and packaging may vary.
If You Think Something Is Wrong
- Contact your prescriber and pharmacy immediately
- Do not inject or take the product
- Report to FDA MedWatch (fda.gov/medwatch or call 1-800-FDA-1088) — the FDA also recommends their BeSafeRx program for verifying online pharmacies
Sources: FDA concerns with unapproved GLP-1 drugs used for weight loss (fda.gov); FDA warning letters fall 2025; FDA BeSafeRx campaign.
What to Expect Week by Week on a GLP-1
Knowing what's coming makes the early weeks much less stressful. Here's a realistic timeline based on clinical trial data and real-world patient experience.
Week 1 — The Adjustment. First injection (or first tablet). Most people notice reduced appetite within 1-3 days. Some nausea is common — usually mild, usually manageable. Take your first dose on a day you can rest. Focus on hydration, small meals, and giving yourself grace.
Weeks 2-4 — Finding Your Rhythm. Nausea typically peaks somewhere in here, then starts fading. Appetite reduction becomes more consistent. You may notice constipation starting — now is the time to add fiber and increase your water intake if you haven't already. Weight loss begins: typically 2-5 pounds in the first month, mostly from reduced food volume and water shifts. Don't obsess over the scale yet.
Weeks 5-8 — First Dose Increase. Moving to the second dose level may bring a brief return of side effects (milder than week 1 for most people). Appetite suppression becomes more reliable. Energy may fluctuate — make sure you're eating enough. This is not a crash diet. Your body needs fuel. Start or continue resistance training to protect muscle mass.
Weeks 9-16 — Approaching Therapeutic Dose. Most GI side effects have settled or become very mild. Appetite control feels more natural — less like fighting cravings, more like simply not being as hungry. Weight loss becomes more consistent and noticeable. This is where the real results begin to show.
Months 4-6+ — Maintenance Phase. You've reached or are approaching your maintenance dose. Weight loss continues but the rate gradually slows — this is completely normal biology, not a “plateau.” Your body is finding a new equilibrium. Average results in clinical trials: approximately 15% of body weight lost with semaglutide 2.4 mg (Wegovy) at 68 weeks; approximately 20%+ with tirzepatide 15 mg (Zepbound) at 72 weeks.
Sources: STEP 1 trial (semaglutide); SURMOUNT-1 trial (tirzepatide); real-world cohort data.
How Long Do You Need to Stay on a GLP-1?
This is the question everyone asks, and the honest answer is: probably long-term, if you want to keep the results.
Clinical trials consistently show that when patients stop GLP-1 medications, most regain a significant portion of the weight they lost — usually within 1-2 years. A BMJ analysis found that weight regain tends to be faster after stopping GLP-1s compared to after stopping traditional lifestyle programs. This isn't a moral failing. It's biology. The medications work by changing your hunger and satiety signals. When you stop them, those signals return to their pre-treatment state.
The American Diabetes Association's 2025 Standards of Care recommend continuing GLP-1 therapy long-term for patients who are benefiting — the same way we continue blood pressure or cholesterol medication long-term.
That said: this is a conversation between you and your provider. Some patients maintain results with lower “maintenance doses.” Some transition to other strategies with medical supervision. What doesn't work is stopping abruptly and hoping for the best.
Sources: BMJ systematic review and meta-analysis; ADA 2025 Standards of Care; STEP 4 trial (semaglutide withdrawal data).
What Are the Long-Term Safety Concerns? (What We Know and What We Don't)
You deserve an honest answer here, not corporate reassurance and not fear-mongering. So here's where the evidence actually stands.
What the Evidence Strongly Supports as Safe
Cardiovascular health: The SELECT trial (the largest GLP-1 cardiovascular outcomes trial to date) found that semaglutide reduced major cardiovascular events — heart attack, stroke, cardiovascular death — by 20% in overweight or obese adults with existing heart disease. This is a proven benefit, not just an absence of harm.
Suicidal ideation: The FDA reviewed reports of suicidal thoughts and actions with GLP-1 medicines and reported that their evaluation did not find evidence of a causal relationship, while continuing to monitor safety data. In early 2026, the FDA also asked manufacturers to remove certain warning language from some GLP-1 labels based on its review.
General short-to-medium term safety: Established across 5+ years of clinical use and trials involving tens of thousands of patients.
What Requires Ongoing Monitoring
Thyroid C-cell tumors: Found in rodent studies at high doses. No confirmed causal link in humans after years of widespread use. But this is why every GLP-1 carries a black box warning, and why patients with a personal or family history of medullary thyroid carcinoma should not use them.
Pancreatitis: Individual case reports exist, but large-scale analyses have not shown a statistically significant increase over the general population rate. Still — if you get severe abdominal pain radiating to your back, stop the medication and go to the ER.
Gallbladder events: Modestly increased risk of gallstones — but this tracks with rapid weight loss from any cause, including bariatric surgery. It's the weight loss, not the drug specifically.
Muscle loss: Up to 25-40% of weight lost can be lean muscle mass without intervention. This is mitigated significantly by adequate protein intake (60-100g/day) and resistance training. If you do nothing else, do those two things.
Bone density: Rapid weight loss from any method can reduce bone density. Particularly relevant for postmenopausal women and older adults. Monitor with your provider.
What We Genuinely Don't Know Yet
- Effects beyond 5-10 years of continuous use (the medications haven't existed long enough for this data)
- Long-term impact on the gut microbiome
- Whether lower maintenance doses can sustain full benefits with fewer potential risks
- The full picture of rare neuropsychiatric effects (mood changes, anxiety)
The honest bottom line: for most people, the known benefits of GLP-1 medications — significant weight loss, improved cardiovascular health, better metabolic markers — substantially outweigh the known risks. But no medication is risk-free, and long-term data is still being collected. Stay in communication with your provider, track how you feel, and don't ignore symptoms that seem off.
Sources: SELECT trial; STEP trials 1-5; SURMOUNT trials 1-4; PMC: Adverse Effects of GLP-1 Receptor Agonists; Pharmacy Times ADA Scientific Sessions coverage; FDA prescribing information.
How We Verified This Information
Every dosing schedule, storage rule, and safety recommendation in this guide has been verified against current FDA-approved prescribing information for each medication. Side effect data comes from FDA labels, NIH PubMed/PMC clinical reviews, and pivotal clinical trials including the STEP program (semaglutide), SURMOUNT program (tirzepatide), SELECT cardiovascular outcomes trial, and OASIS trials (oral semaglutide).
Drug interaction information was cross-referenced with FDA prescribing labels and the Drugs.com professional interaction database. Compounding safety information was sourced directly from FDA.gov safety communications, warning letters, and the FDA's BeSafeRx consumer guidance.
We have no financial relationship with any GLP-1 medication manufacturer. This safety guide page contains no affiliate links. Our provider comparison pages on other parts of this site do include affiliate links, which are clearly disclosed.
This page is updated when FDA prescribing information changes, new safety data is published, or new GLP-1 medications receive approval.
Last full verification: February 2026
Sources & FDA Labels
Every dosing, storage, and safety claim in this guide is verified against the FDA-approved prescribing information for each medication. Below are direct links to the official labels and key FDA resources referenced throughout this page.
- Wegovy (semaglutide injection + tablets): FDA prescribing information (injection); FDA prescribing information (tablets)
- Ozempic (semaglutide injection): Ozempic prescribing information
- Rybelsus (oral semaglutide): Rybelsus prescribing information
- Mounjaro (tirzepatide): Mounjaro prescribing information (Lilly)
- Zepbound (tirzepatide): Zepbound prescribing information (Lilly)
- Saxenda (liraglutide): Saxenda prescribing information
- Trulicity (dulaglutide): Trulicity prescribing information (Lilly)
- FDA: Concerns with unapproved GLP-1 drugs: FDA safety communication
- FDA: Suicidal behavior warning removal: FDA drug safety communication
All links verified February 2026. If any link is broken, the prescribing information can be found via DailyMed (dailymed.nlm.nih.gov) or Drugs@FDA (accessdata.fda.gov/scripts/cder/daf).
Frequently Asked Questions
Can you take GLP-1 "drops" instead of injections?
"GLP-1 drops" are not an FDA-approved formulation. Some online sellers market sublingual drops or "oral liquids," but these have not been reviewed by the FDA for safety, effectiveness, or quality. FDA-approved options are pre-filled injection pens and oral tablets (Rybelsus for diabetes; oral Wegovy for weight loss). If you're being offered "drops" — verify the source carefully before using them.
Which GLP-1 is best for weight loss?
In head-to-head clinical trial data, tirzepatide (Zepbound) produces the greatest average weight loss — over 20% of body weight at the highest dose. Semaglutide (Wegovy) averages about 15%. But “best” depends on your insurance coverage, medical history, cost, and individual response. Some people respond better to one than the other. Your provider can help you decide, and our provider comparison guide breaks down the options in detail.
Is it safe to take GLP-1 while trying to get pregnant?
No. All GLP-1 medications should be stopped before or during pregnancy. Semaglutide (Wegovy) should be discontinued at least 2 months before planned conception. For tirzepatide (Zepbound/Mounjaro), the U.S. label advises discontinuing when pregnancy is recognized — discuss pre-conception timing with your clinician. Use reliable birth control while on GLP-1 therapy.
Can you exercise on a GLP-1?
Yes, and you should. Resistance training is especially important for preserving muscle mass during weight loss. Start gradually. Stay hydrated — even more important on GLP-1s. Your energy may be lower in the first few weeks; adjust intensity as needed and build up over time.
What if I threw up shortly after my injection?
If you vomited within 30 minutes of an injection, the medication was likely already absorbed (injectable GLP-1s absorb from fatty tissue, not the GI tract). Do not take another dose. If you vomited after taking an oral GLP-1 tablet, the dose may not have absorbed — but do not take another tablet that day. Wait until the next scheduled dose.
What happens if you inject too much GLP-1?
Overdose can cause severe nausea, severe vomiting, and potentially dangerous hypoglycemia. If you suspect an overdose — especially with compounded vial-and-syringe formulations where dosing errors are most common — contact Poison Control at 1-800-222-1222 or call your provider immediately.
Can you travel with GLP-1 medications?
Yes. Keep injectable medications in your carry-on luggage (never checked bags). TSA allows needles and injectable medications when properly labeled. Use an insulated travel case. Carry your prescription or a letter from your provider.
What if my medication package arrived warm?
Contact the pharmacy for guidance before using it. Many injectable GLP-1 products are intended to be kept refrigerated until use (each brand has a limited room-temperature window). The FDA has flagged this as a specific concern with compounded GLP-1 shipments.
Are there natural alternatives to GLP-1 medications?
No supplement or food has been proven to replicate the pharmacological effects of GLP-1 receptor agonists. Your body naturally produces GLP-1, and lifestyle factors like high-fiber diets, sleep, and exercise support healthy levels — but not at the therapeutic intensity of prescription medications. Be skeptical of anything claiming to be a "natural GLP-1."
Can you drink alcohol on a GLP-1?
There's no absolute prohibition, but use caution. Alcohol amplifies nausea and dehydration risk — both of which are already elevated on GLP-1s. Many patients find their alcohol tolerance drops significantly. Start with very small amounts. For diabetic patients, alcohol can cause dangerous blood sugar swings.
Do you need bloodwork before or during GLP-1 treatment?
Your provider should assess baseline labs before starting (typically A1c or fasting glucose, lipid panel, kidney and liver function). Ongoing monitoring depends on your health history — most providers want periodic check-ins on these markers plus your weight, blood pressure, and how you're feeling overall.
What if I'm on birth control pills?
Tirzepatide (Mounjaro, Zepbound) specifically can reduce the absorption of oral contraceptives due to slowed gastric emptying. The FDA recommends using a non-oral contraceptive method or adding a barrier method for 4 weeks after starting tirzepatide and after each dose increase. Discuss this with your prescriber.
What to Do Next
If you've read this far, you're already more prepared than most people who start GLP-1 medications. Here's a quick action plan:
If you already have a prescription and medication in hand:
Use the safety checklist at the top of this page. Follow the injection or oral instructions for your specific medication. Bookmark this page — it's designed to be a reference you come back to when questions come up.
If you're looking for a provider:
The quality of your prescriber matters. You want a provider who does real medical screening (not just a 2-minute questionnaire), monitors your progress, and is available when you have questions. We've reviewed the major GLP-1 telehealth providers and compared them on pricing, medical oversight, and patient experience — see our comparison here.
If you're comparing brand-name vs. compounded GLP-1s:
This is a nuanced decision with real safety implications. We've written a separate guide that covers the trade-offs, costs, and what to verify — read it here.
This page was created by the Weight Loss Provider Guide research team. All medical information has been verified against FDA prescribing information and peer-reviewed clinical literature. We are not doctors. We are researchers who believe people deserve clear, accurate, complete information about the medications they put in their bodies. If anything on this page conflicts with what your healthcare provider tells you — follow your provider's guidance.
Last updated: February 2026. Last verified against FDA prescribing information: February 2026.