What Happens When You Stop Taking GLP-1 — And What to Do About It
Here's what happens when you stop taking GLP-1 medication, straight from the clinical data: in the STEP 1 Extension trial, participants who stopped semaglutide regained about two-thirds of their prior weight loss within one year. Appetite comes back within one to two weeks. Blood sugar, blood pressure, and cholesterol improvements begin reversing within months. A January 2026 meta-analysis in the BMJ estimated that weight returns to pre-treatment levels in about 1.7 years.
That's the reality — and it's not a moral failure. It's biology. Obesity is a chronic condition, and GLP-1 medications treat it the way blood pressure drugs treat hypertension. Stop the treatment, and the condition tends to return.
But here's what most articles won't tell you: how you stop matters enormously. Tapering gradually instead of quitting cold turkey, building specific habits while still on medication, and — if cost is forcing your hand — switching to an affordable provider instead of quitting entirely can dramatically change your outcome. Below, I'll walk you through exactly what happens to your body week by week, what every major clinical trial actually found, and what to do based on your specific situation.
Medical note: Educational only — not medical advice. Always consult a licensed clinician.
The First Thing to Know: Are You Taking GLP-1 for Weight Loss or Diabetes?
This matters more than most articles acknowledge, and I want to get it out of the way before anything else.
If you take a GLP-1 for type 2 diabetes
(Ozempic, Mounjaro, or others prescribed for blood sugar control), stopping can cause your blood glucose to spike — sometimes dangerously. Do not stop without your prescriber's involvement. They'll need to adjust your diabetes management plan, potentially switching you to another medication. The Lancet eClinicalMedicine meta-analysis (November 2025) found that HbA1c rose by an average of 0.65% after GLP-1 discontinuation in people with type 2 diabetes. That's clinically significant.
If you take a GLP-1 for weight management
(Wegovy, Zepbound, or off-label Ozempic/Mounjaro), the primary risk is weight regain and the return of appetite — not an acute medical emergency. It's still worth planning, but you're not in immediate danger.
If you take it for both
Treat your situation as higher-stakes and keep your care team in the loop.
With that safety note established, let's get into what actually happens to your body.
What Happens to Your Body After Stopping GLP-1: The Week-by-Week Timeline
This is what most people are really searching for — not vague warnings about "weight regain," but a clear picture of when each change happens and what it feels like. I built this timeline by synthesizing data from the STEP 1 Extension trial, the SURMOUNT-4 trial, the January 2026 BMJ meta-analysis, FDA prescribing information, and statements from named physicians at major medical centers.
A quick note: individual experiences vary. This timeline represents what the research shows happens on average.
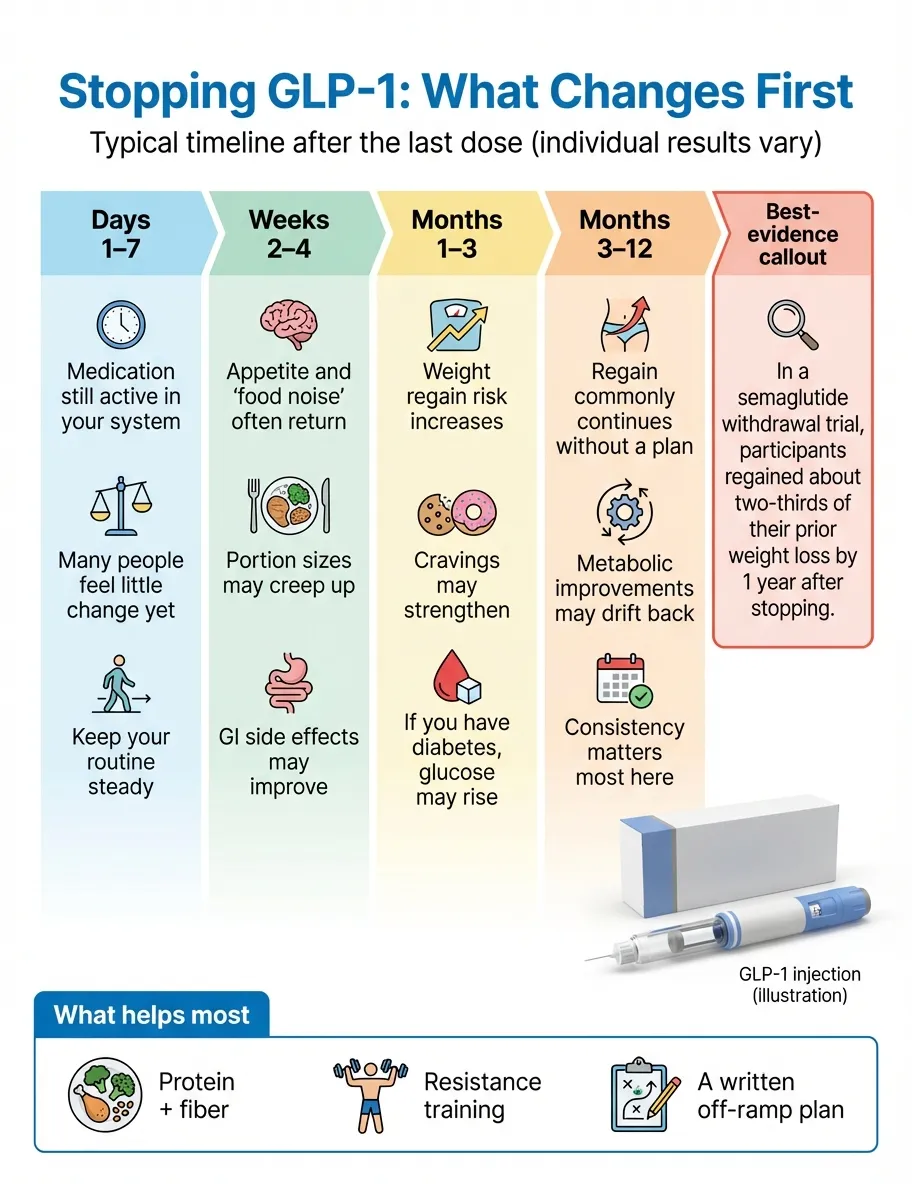
| Timeframe | What's Happening in Your Body | What You'll Likely Feel | What the Evidence Shows |
|---|---|---|---|
| Days 1–7 | Drug levels start declining. Semaglutide (Wegovy/Ozempic) has a half-life of about 7 days. Tirzepatide (Zepbound/Mounjaro) has a half-life of about 5 days. The medication is still active in your system. | Probably nothing noticeable yet. Most people feel normal during the first week. | FDA prescribing information: semaglutide half-life approximately 1 week; tirzepatide approximately 5 days. |
| Weeks 1–2 | GLP-1 receptor stimulation decreases. Gastric emptying begins speeding up. Ghrelin (the hunger hormone) starts rising. | Appetite begins returning. You may notice you're thinking about food more. Portions that satisfied you last week might leave you wanting more. | As medication levels fall (half-life ~1 week for semaglutide; ~5 days for tirzepatide), many people notice hunger and "food noise" returning. |
| Weeks 2–4 | The drug is largely clearing your system (full clearance takes ~5 weeks for semaglutide). Appetite regulation is reverting toward your pre-medication baseline. | Noticeably hungrier. "Food noise" — that constant background hum of thinking about food — starts coming back. Cravings for calorie-dense foods may resurface. One real upside: GI side effects like nausea and constipation resolve. | Appetite suppression fades as drug levels decline. Dr. Laura Choi, Houston Methodist: "What people refer to as 'withdrawal' may be that returning to your hunger levels pre-medication feels worse than how it used to feel." |
| Months 1–3 | Weight regain begins. Your body preferentially puts on fat (not muscle). Blood sugar and blood pressure start trending back toward pre-treatment levels. | The scale starts moving. Clothes feel different. This is when many people feel discouraged or frustrated. It's also when the emotional toll is heaviest. | BMJ (January 2026): average regain of approximately 1 pound per month. STEP 1 Extension: significant regain is evident by 3 months post-discontinuation. |
| Months 3–6 | Weight regain accelerates. Most cardiometabolic improvements are now reversing. Cholesterol levels are trending back. | The trajectory feels relentless. Some people describe feeling like they've "lost control" — but this is your body's biology, not a character flaw. | SURMOUNT-4: more than 50% of tirzepatide-related weight loss rebounded within 52 weeks. STEP-10: over 40% of lost weight regained within just 28 weeks. |
| Months 6–12 | Approximately two-thirds of lost weight has returned (in semaglutide trials). Prediabetic status may re-emerge. Blood pressure and HbA1c are approaching pre-treatment levels. | Weight regain may begin slowing or plateauing. Most people retain a net weight loss of about 5% from their original starting weight — which still has clinical significance. | STEP 1 Extension (2022): participants on semaglutide regained two-thirds of prior weight loss at 1 year. SURMOUNT-4 post-hoc (JAMA Internal Medicine, 2025): 82.5% of participants who stopped tirzepatide regained ≥25% of their weight loss within 1 year. |
| 12–18+ months | Weight approaches pre-treatment levels. Most cardiometabolic markers have fully reverted. | For many people, it feels like being back to square one. But those who built strong exercise and nutrition habits while on medication tend to retain more progress. | BMJ (January 2026): estimated return to pre-treatment weight within ~1.7 years; cardiometabolic markers within ~1.4 years. |
Important context behind these numbers
These are averages. Some people regain more. Some regain less. A few manage to maintain most of their weight loss through aggressive lifestyle changes — but they're the exception, not the rule.
The weight you regain is mostly fat. This is one of the most underappreciated consequences. While on GLP-1 medication, you lost a mix of fat and some muscle. But regained weight is disproportionately fat. Even at the same number on the scale, your body composition — and metabolic health — may be slightly worse. This is why resistance training during and after GLP-1 use is so important.
Semaglutide causes more rebound than liraglutide. In a systematic review and meta-analysis published in Lancet eClinicalMedicine (November 2025), semaglutide discontinuation was associated with an average weight regain of ~8.21 kg compared to ~4.29 kg with liraglutide (study-level averages; follow-up periods varied). The likely explanation: semaglutide's stronger central appetite suppression creates a more dramatic rebound when removed.
There's a silver lining. Even with weight regain, some cardiovascular markers — particularly C-reactive protein (an inflammation marker) and certain cholesterol measures — stayed slightly improved in the STEP 1 Extension trial. If you lost a significant amount of weight, you're likely to retain at least modest health benefits even after some regain.
How Long Does GLP-1 Stay in Your System After Your Last Dose?
Understanding your medication's half-life helps you anticipate when changes will start. "Half-life" means the time it takes for half the drug to leave your body. After about five half-lives, the medication is essentially gone.
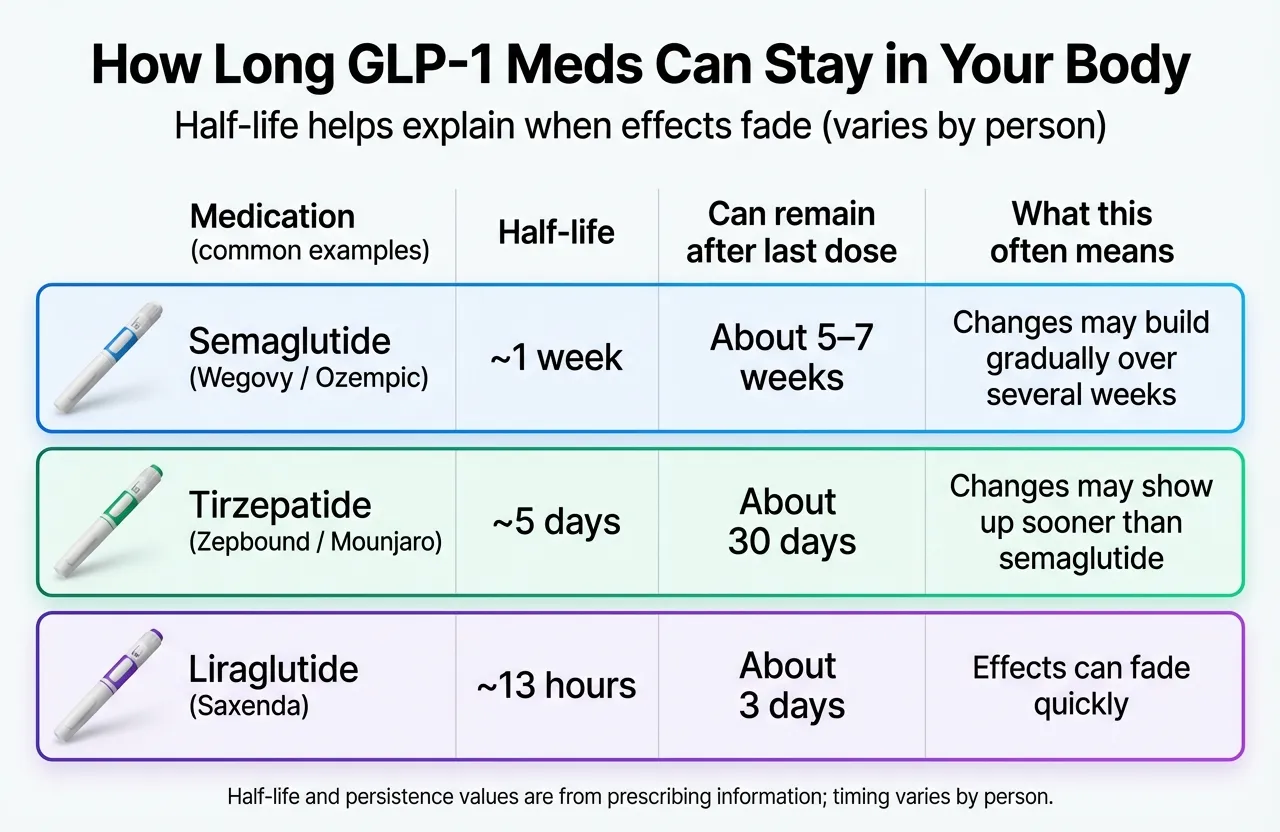
| Medication | Brand Names | Half-Life | Still in Circulation After Last Dose | When Appetite Changes Typically Begin |
|---|---|---|---|---|
| Semaglutide (injection) | Wegovy, Ozempic | ~7 days | ~5 weeks | 1–2 weeks after last dose |
| Semaglutide (oral) | Wegovy tablet, Rybelsus | ~7 days | ~5 weeks | 1–2 weeks after last dose |
| Tirzepatide | Zepbound, Mounjaro | ~5 days | ~25–30 days | 1–2 weeks after last dose |
| Liraglutide | Saxenda, Victoza | ~13 hours | 3–4 days | Within days of last dose |
Sources: FDA prescribing information for Wegovy, Zepbound, and Saxenda via DailyMed.
Why this matters practically
If you're on semaglutide, the drug sticks around for over a month after your last injection. That's why the first week or two may feel relatively normal — the medication hasn't fully cleared yet. The real appetite shift tends to hit around weeks 2–4.
If you're on liraglutide (Saxenda), the transition is much faster. With a half-life of just 13 hours, the drug clears within days. Expect appetite changes sooner.
Why Does Weight Come Back? (It's Biology, Not Willpower)
If you stop blood pressure medication, your blood pressure goes back up. If you stop a GLP-1, your weight tends to go back up. Same principle. But it helps to understand why, because it removes the shame.
Your hunger hormones rebound
GLP-1 medications suppress ghrelin (the hormone that makes you hungry) and enhance satiety signals. When the drug leaves, ghrelin surges back — and your brain's hunger centers light up like they've been starved. Many people describe the return of "food noise" as genuinely distressing. As one researcher at the Perelman School of Medicine put it: the brain becomes more sensitive to hunger cues after the medication is removed.
Your metabolism adapted to your lower weight
During weight loss, your body reduces its resting metabolic rate — essentially burning fewer calories to protect itself from what it perceives as a threat. GLP-1 medications partly override this. Remove the medication, and you're left with a lower metabolism but a returned appetite. That mismatch drives regain.
Your body defends a "set point"
There's growing evidence that the body has a biological weight range it actively tries to maintain. GLP-1 medications override this set point. When you stop, your body's defense mechanisms kick back in — increased hunger, decreased energy expenditure, hormonal shifts that all push you back toward your previous weight.
The regained weight is disproportionately fat
You lost some muscle during weight loss (inevitable no matter the method), but regained weight comes back primarily as fat. At the same body weight, you may have less muscle mass and more fat than before you started — which makes your metabolic profile worse.
"Even if their lifestyle modifications such as diet and exercise are perfect — there will almost always be weight regain," said Dr. Maria Cecilia Asnis, Medical Director of the Center for Weight Management at Stamford Health, drawing on more than a decade of clinical experience. "That's because we're no longer addressing what's going on inside of the body."
The Key Point
None of this is a character judgment. This is your body's biology reasserting itself. The same biological drives that contributed to weight gain before you started medication are still there. The medication was managing them; without it, you have to manage them another way.
What Do the Studies Actually Show? Every Major GLP-1 Discontinuation Trial
I'm going to lay out the data from the key clinical trials — not cherry-picked, not exaggerated. This is what researchers found when they tracked people who stopped taking GLP-1 medications.
| Study | Drug | Time on Drug | Follow-Up After Stopping | Weight Lost on Drug | Weight Regained | Net Loss at Follow-Up | Key Takeaway |
|---|---|---|---|---|---|---|---|
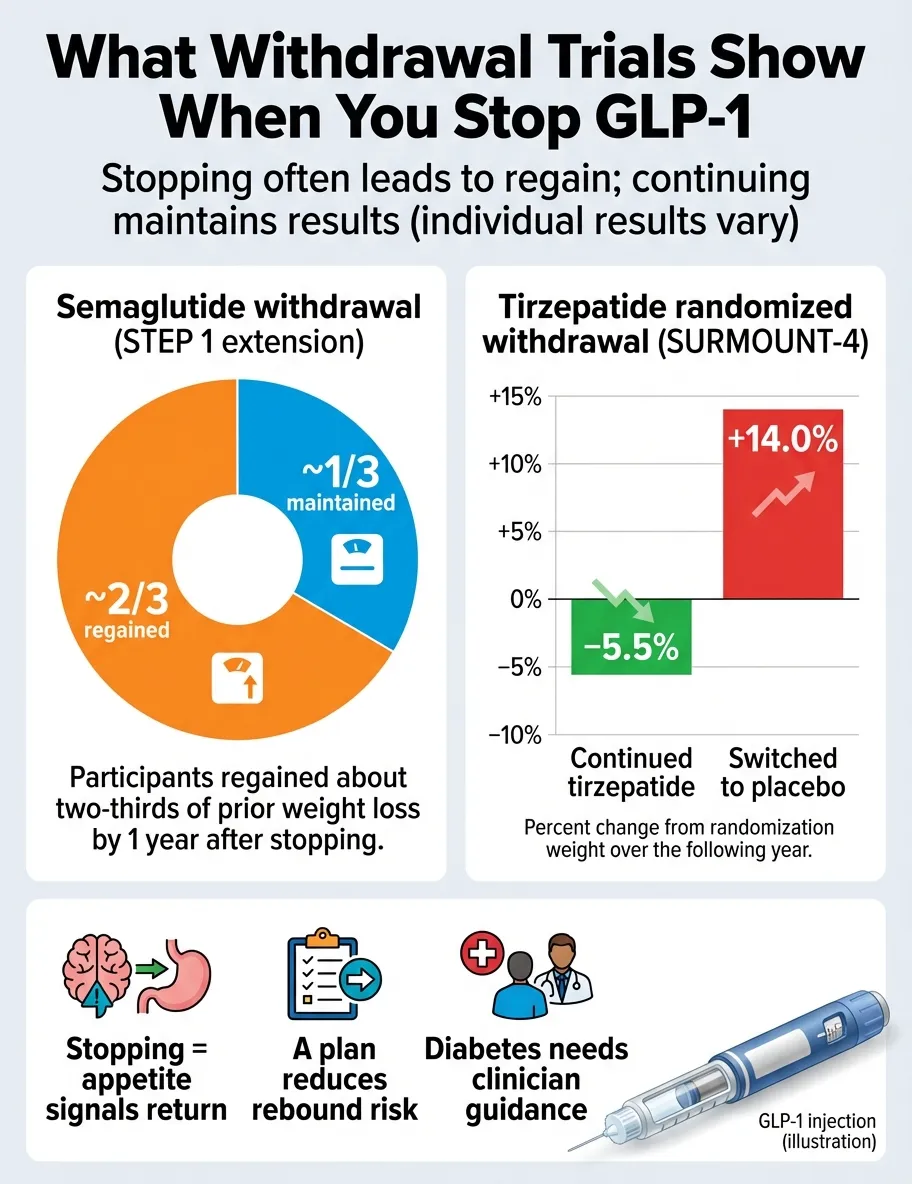
| STEP 1 Extension (Wilding et al., Diabetes Obes Metab, 2022) | Semaglutide 2.4 mg | 68 weeks | 1 year | ~15% body weight | ~2/3 regained | ~5% net loss | The landmark trial. Two-thirds of weight returned. Cardiometabolic markers reverted, though CRP and some cholesterol metrics stayed slightly improved. |
| JAMA 2021 (Rubino et al.) | Semaglutide 2.4 mg | 20 weeks | 48 weeks | ~11% body weight | ~7% regained | ~4% net loss | Continued lifestyle intervention may have slowed regain slightly. |
| SURMOUNT-4 (Aronne et al., JAMA, 2024) | Tirzepatide | 36 weeks | 52 weeks | ~21% body weight | ~14% regained (>50% of loss) | Significant net loss retained | Tirzepatide shows a similar rebound pattern. Continuing treatment maintained and even augmented weight loss. |
| STEP-10 | Semaglutide | Variable | 28 weeks | Variable | >40% in just 28 weeks | — | Faster rebound than expected, even in short follow-up. |
| BMJ Meta-Analysis (West et al., January 2026) | GLP-1 class (all) | Various | Various | Various | ~1 lb/month average | Pre-treatment level by ~1.7 years | Weight-loss drugs cause regain 4x faster than stopping behavioral interventions (diet/exercise programs) alone. |
| Lancet eClinicalMedicine (November 2025) | GLP-1 class (all) | Various | Various | Various | 5.63 kg (obesity); 2.03 kg (T2D) | — | Semaglutide causes more rebound than liraglutide (~8.21 kg vs ~4.29 kg). Greater regain with longer follow-up periods. |
| Lancet 2017 (le Roux et al.) | Liraglutide 3.0 mg | 1 year | 2 more years | ~8% body weight | Partial regain | ~6% maintained at 3 years | Liraglutide shows slower, less dramatic regain than semaglutide. |
What this table tells us
The pattern is consistent across every trial and every GLP-1 medication: stopping leads to significant weight regain. No trial found otherwise.
But there's nuance worth noting. Most people retain some net weight loss (typically 3–5% from their original starting point). That amount, while it might feel disappointing, is still considered clinically meaningful — even 3% weight loss can improve diabetes risk, blood lipids, and blood pressure.
The more weight you lost on the drug, the more you'll regain — but paradoxically, you'll also retain the greatest absolute net loss. Losing 20% and regaining 14% still leaves you 6% lighter than where you started.
And the January 2026 BMJ finding is worth sitting with: drug-related weight regain happens roughly four times faster than regain after stopping a diet or exercise program. The medications create more dramatic biological shifts, so the reversal is more dramatic too.
Should You Stop Taking GLP-1? A Decision Framework
The answer depends entirely on why you're considering stopping. Here's a framework based on the most common reasons.
If You're Stopping Because of Cost
You're not alone — and this is not a trivial problem. Cost is the single biggest reason people discontinue GLP-1 therapy. List prices are around $1,000/month for Ozempic and about $1,349/month for Wegovy injectable, though manufacturer cash-pay programs and the new Wegovy pill (starting at $149/month self-pay) have changed the landscape — verify current pricing before making a stop/continue decision. A JAMA Network Open study found that 84.4% of non-diabetic users discontinued within two years (median time to discontinuation: 176 days), and income level was a strong predictor of persistence.
Before you stop entirely, consider switching providers. Online telehealth platforms offer GLP-1 prescriptions at significantly lower cost than brand-name pricing. Staying on a lower dose from an affordable provider is almost always a better outcome than stopping entirely.
A few options worth exploring:
- Manufacturer programs: NovoCare (for Wegovy) and LillyDirect (for Zepbound) offer reduced pricing for eligible patients
- Insurance appeals: Your prescriber can submit prior authorization with clinical justification — denials can sometimes be overturned
- Telehealth providers: Several offer GLP-1 treatment plans with pricing that's a fraction of brand-name pharmacy costs
If switching isn't an option and you truly must stop, taper gradually rather than quitting cold turkey (more on that below).
If You're Stopping Because of Side Effects
GI side effects — nausea, vomiting, diarrhea, constipation — are the second most common reason people quit. In clinical trials, about 3–4% of participants stopped specifically because of GI issues.
Before stopping entirely, talk to your prescriber about:
- Dose reduction: A lower dose may be tolerable while still providing some benefit
- Slower titration: Increasing the dose more gradually often reduces side effects
- Switching medications: Some people who can't tolerate semaglutide do well on tirzepatide, or vice versa. The side effect profiles differ.
If side effects are truly intolerable at any dose, stopping is reasonable. The good news: GI side effects resolve quickly once the medication clears your system. That's the one clear upside of discontinuation.
If You've Reached Your Goal Weight
This is the most psychologically tricky situation. You hit your target. The instinct is to "be done." And your insurance might even stop covering the medication once you're no longer classified as obese.
But the clinical evidence is unambiguous: stopping after reaching your goal weight still leads to substantial regain, regardless of lifestyle habits. "Reaching your goal weight on a GLP-1 is like reaching your target blood pressure on medication — the medication is what got you there," as obesity medicine physicians frequently explain.
Your options:
- Stay on a maintenance dose (lower dose, reduced cost, ongoing benefit)
- Taper gradually while building aggressive lifestyle habits
- Set a "restart threshold" with your doctor: "If I regain X pounds, we go back on medication"
Whatever you choose, have a written plan. Don't wing it.
If You're Planning a Pregnancy
GLP-1 medications should be discontinued before pregnancy. Wegovy labeling recommends stopping at least 2 months before planned conception (to allow full drug clearance given semaglutide's long half-life). For tirzepatide, discuss timing with your clinician; the drug has a ~5-day half-life and can remain in the body for about 25–30 days after the last dose.
Work with both your OB/GYN and your prescribing provider to create a transition plan. The time between stopping medication and conceiving is a vulnerable window for weight regain — having nutrition and exercise habits established beforehand makes a real difference.
If Your Insurance Stopped Covering It
Coverage denials are frustratingly common, particularly for weight management (as opposed to diabetes) indications.
- Appeal: Your provider can submit a prior authorization. Include clinical documentation of weight-related comorbidities.
- Switch providers: Telehealth platforms may offer lower out-of-pocket costs. Compare GLP-1 providers
- Manufacturer programs: Check NovoCare and LillyDirect eligibility
If the Medication Isn't Working for You
Approximately 10% of patients have no meaningful weight loss response to GLP-1 medications, according to Dr. John Morton at Yale New Haven Health. This isn't your fault — it's a medication mismatch.
Options include switching between medications (semaglutide ↔ tirzepatide), adjusting doses, or exploring other interventions. Stopping a medication that isn't working is completely reasonable.
How to Stop Taking GLP-1 Safely: Tapering vs. Cold Turkey
This is one of the most important sections of this guide, and it's where most other resources fall short.
Why "cold turkey" is the worst option
"If a person abruptly stops GLP-1s, they may regain between 50% and 80% of the weight they lost," said Dr. Duffy of ThedaCare Weight Wellness Solutions. The reason: appetite spikes immediately while your metabolism is still running slow. It's a "perfect storm" for rebound weight gain.
For people with type 2 diabetes, cold turkey carries an additional risk: blood sugar can spike unpredictably without the medication's glucose-regulating effects. If you have diabetes, never stop a GLP-1 without medical supervision.
Why tapering appears to work better
There are no official tapering guidelines from drug manufacturers — GLP-1 medications are designed as lifelong treatments, so the labels don't address discontinuation protocols.
But emerging evidence supports a gradual approach. Research presented at the European Congress on Obesity in 2024 found that patients who tapered off semaglutide over approximately 9 weeks maintained a stable body weight for 26 weeks after complete discontinuation. That's a meaningful difference compared to the rapid regain seen with abrupt stopping.
Two common tapering approaches:
Reverse titration
Step down through the dose levels in the opposite order you titrated up. If you're on semaglutide 2.4 mg, drop to 1.7 mg for a few weeks, then 1.0 mg, then 0.5 mg, then 0.25 mg.
Dose stretching
Keep the same dose but increase the interval. Go from weekly injections to every 10 days, then every two weeks, then every three weeks.
The typical taper takes 4–12 weeks depending on your dose and individual response.
An important caveat
I want to be honest about the evidence here. The tapering research is still early. Most of what clinicians recommend is based on clinical experience and biological plausibility, not large randomized controlled trials. Dr. Robert Kushner, an obesity medicine specialist, notes that tapering "is the strategy that is most commonly done in the office setting" — but the manufacturers themselves provide no guidance because the drugs weren't designed to be stopped.
What to monitor during your taper
- Weight: Weekly weigh-ins. Note the trend, not individual fluctuations.
- Appetite: Track hunger levels and food noise. Are cravings manageable or overwhelming?
- Blood sugar: Essential if you're diabetic or prediabetic. Check with your provider on monitoring frequency.
- Blood pressure: Can start climbing as weight returns.
- Your relationship with food: Are you stress-eating? Binge-eating? Losing the structure you built while on medication?
If any of these metrics move in a concerning direction, don't wait. Call your prescriber. Restarting medication is always an option.
The bottom line on stopping
If you must stop, taper. If cost is the reason, switch providers before you stop. The worst option is quitting cold turkey with no plan.
Do GLP-1 Drugs Cause "Withdrawal"?
Short answer: no — not in the clinical sense. GLP-1 medications are not addictive and don't cause the kind of withdrawal you'd experience with, say, opioids or benzodiazepines.
But — and this matters — the return of symptoms can feel like withdrawal. Dr. Laura Choi at Houston Methodist puts it well: "I think the word withdrawal could apply, but it's more about losing the benefits. Losing the benefits of these medications — if you were enjoying those — can feel like withdrawal because then your sense of how you feel every day can drastically revert to where it was pre-medicine."
What people commonly experience after stopping
Increased appetite and food cravings — The most universal experience. The "food noise" that GLP-1 medications quieted comes roaring back. Many people describe this as the hardest part.
Faster digestion — Food moves through your stomach more quickly again, which means you feel hungry sooner after meals.
Mood changes — Some people report increased irritability, anxiety, or low mood. This isn't well-studied but makes intuitive sense: watching the scale climb and feeling hunger return is emotionally difficult.
Blood sugar fluctuations — Primarily affects people with diabetes or prediabetes. Can manifest as fatigue, excessive thirst, frequent urination, and brain fog.
GI relief — Here's the positive: if you experienced nausea, constipation, bloating, or acid reflux on the medication, those symptoms typically resolve as the drug clears. For some people, this alone makes stopping worth it.
When to call your doctor (not normal "adjustment")
Most post-discontinuation symptoms are uncomfortable but not dangerous. However, contact your healthcare provider if you experience:
- Severe or persistent vomiting
- Blood sugar readings above your provider's threshold (if diabetic)
- Severe abdominal pain
- Signs of dehydration (dizziness, dark urine, rapid heartbeat)
- Symptoms of diabetic ketoacidosis (for T2D patients: nausea, confusion, fruity breath odor)
- Binge eating episodes you can't control
How to Keep Weight Off After Stopping GLP-1
I'll be straight with you: no lifestyle program fully replaces what GLP-1 medications do biologically. The BMJ meta-analysis confirmed that drug-related weight regain is 4x faster than regain after stopping behavioral interventions alone. But that doesn't mean there's nothing you can do. The strategies below won't guarantee you maintain every pound, but they can meaningfully reduce how much comes back.
Start BEFORE you stop
This is the single highest-leverage move. The time to build habits is while you're still on medication and your appetite is suppressed. Use the medication as a training ground — not a vacation from effort.
If you're planning to discontinue, spend the last 2–3 months on medication aggressively establishing:
- A consistent eating pattern (same approximate times each day)
- A protein-first approach at every meal (25–30g per meal minimum)
- A regular exercise routine you genuinely enjoy and will maintain
- Strategies for managing stress and emotional eating
Nutrition that mimics some of what GLP-1 does
You can't perfectly replicate a medication's effects with food, but certain patterns come close to producing natural satiety:
Protein at every meal. Protein is the most satiating macronutrient. Aim for lean meats, fish, eggs, Greek yogurt, legumes, and cottage cheese. The 25–30g per meal target isn't arbitrary — research on satiety consistently shows this threshold makes a measurable difference.
High-fiber foods. Fiber slows gastric emptying — which is exactly what GLP-1 medications do pharmacologically. Beans, lentils, vegetables, whole grains, and fruits all contribute. Target 25–35g of fiber daily.
Smaller, more frequent meals. Without the medication slowing your digestion, you'll get hungry faster. Eating every 3–4 hours (instead of trying to push through long gaps) can help prevent the desperate-hunger-driven overeating that accelerates regain.
Eliminate empty calories ruthlessly. Alcohol, sugary drinks, processed snacks — these are the first things to cut. When your appetite is back at full force, you don't have room in your calorie budget for things that don't keep you full.
Exercise — but the right kind
Resistance training is non-negotiable. I can't emphasize this enough. You lost muscle mass during weight loss (everyone does, regardless of method). Regained weight comes back as fat. The only way to counteract this body composition shift is progressive resistance training — lifting weights, bodyweight exercises, resistance bands — at least 2–3 times per week.
Cardio helps with overall health but is less effective for weight maintenance than most people think. It burns calories, but it also increases appetite. The real maintenance benefit of exercise comes from the muscle it builds and preserves.
There's also a direct physiological benefit: in one study, a year-long supervised exercise program increased postprandial GLP-1 response, with late-phase GLP-1 about 25% greater compared to a usual-activity control group. Your body produces its own GLP-1 — and exercise may help it produce more.
Sleep and stress management
These sound like generic wellness advice, but they're genuinely critical in this context:
- Poor sleep increases ghrelin (the hunger hormone) and decreases leptin (the satiety hormone). It's essentially the opposite of what GLP-1 medications do. Aim for 7–8 hours consistently.
- Chronic stress drives cortisol, which promotes fat storage and increases cravings for high-calorie comfort foods. Find stress management tools that work for you — exercise, meditation, therapy, whatever sticks.
Build an "if/then" plan for rebound hunger
Don't wait until you're standing in front of the refrigerator at midnight to figure out your strategy. Pre-commit:
- If hunger spikes in the evening → then I eat a pre-planned high-protein snack (not whatever's available)
- If I notice binge-like urges → then I call my provider to discuss options
- If I regain X pounds → then I restart medication or schedule an appointment
Write these down. Share them with your doctor. Make the decision in advance, when you're thinking clearly.
Your GLP-1 Off-Ramp Checklist (Print This)
If you're planning to stop — or you've already been forced to by cost, side effects, or insurance — here's a step-by-step checklist to give yourself the best possible outcome. This isn't generic wellness advice. It's a sequenced plan based on what the clinical evidence and practicing physicians actually recommend.
1Clarify your reason for stopping
Write it down. "I'm stopping because ___." This matters because different reasons call for different responses. Cost? Explore cheaper providers before quitting. Side effects? Ask about dose adjustment or switching drugs. Goal weight? Discuss maintenance dosing. Pregnancy? Follow the 2-month pre-conception window. The reason shapes every other decision.
2Talk to your prescriber BEFORE your last dose
This isn't optional. Your provider needs to:
- Develop a taper schedule (if appropriate)
- Adjust other medications (especially for diabetes)
- Set monitoring expectations
- Establish a "restart threshold" — the weight or symptom level at which you'd go back on medication
If cost is preventing the conversation, many telehealth providers offer affordable consultations specifically for medication management.
3Set up your monitoring system
For the first 3 months after stopping, track:
- Weight: Once per week, same day, same conditions. Don't weigh daily — water fluctuations will drive you crazy.
- Appetite and food noise: Rate it 1–10 weekly. Is it stable, climbing, or manageable?
- Waist circumference: Monthly. Sometimes body composition shifts before weight does.
- Blood sugar (if diabetic): Per your provider's instructions, but likely more frequently during the transition.
- Blood pressure: Monthly at minimum.
- Mood and energy: Note any significant changes.
A simple journal or phone note works. The goal isn't obsessive tracking — it's early warning. If things trend badly at week 6, you can intervene at week 6 instead of realizing at month 6 that you've regained 30 pounds.
4Build your "maintenance anchors" before you stop
Do this while still on medication, when appetite is suppressed and habit-building is easier:
- Lock in your protein-first eating pattern. Every meal should lead with 25–30g of protein. This should feel automatic by the time you stop.
- Establish a resistance training routine. Two to three sessions per week. This is the single most impactful exercise choice for your situation.
- Set up your food environment. Stock the kitchen with high-protein, high-fiber options. Remove foods that trigger overeating. Make the default choice the healthy choice.
- Identify your high-risk scenarios. Late-night eating? Stress-triggered snacking? Social events? Know your patterns and have a plan for each.
5Create your "if/then" relapse plan
Pre-commit to specific actions before you need them:
- If I regain ___lbs within ___weeks → then I contact my prescriber to discuss restarting or adjusting my plan
- If food noise becomes unmanageable (rated 8+ for 2 consecutive weeks) → then I schedule a provider visit
- If I notice binge-like episodes → then I schedule a session with a therapist or counselor
- If blood sugar rises above ___mg/dL → then I call my endocrinologist immediately
Write these down. Share them with your provider. Decide now while you're thinking clearly — not later when you're standing in front of the refrigerator at midnight feeling desperate.
6Plan for the emotional component
This part gets overlooked in every clinical guide, but it's real. After months of feeling in control of your appetite, watching that control slip away is psychologically brutal. Some things that help:
- Reframe the narrative. Weight regain after stopping a GLP-1 is not failure. It's the expected biological response to discontinuing treatment for a chronic condition. You wouldn't call it "failure" if your blood pressure went up after stopping blood pressure medication.
- Tell someone. Whether it's a partner, friend, therapist, or online community — don't do this alone. Isolation amplifies shame.
- Set non-scale victories. Strength gains, energy levels, sleep quality, bloodwork improvements. The scale is one metric, not the only one.
- Give yourself permission to restart. Stopping medication doesn't have to be permanent. In a large real-world study, 36.3% of non-diabetic users who stopped GLP-1 therapy restarted within a year. That's not weakness — it's chronic disease management.
What Gets BETTER After You Stop? (Side Effects That Resolve)
Not everything about stopping is bad. If side effects were part of your experience on GLP-1 medication, here's what you can expect to improve:
Nausea typically resolves within 1–2 weeks of your last dose as the drug clears. For many people, this was the most disruptive side effect on the medication, and its departure is genuinely welcome.
Constipation and bloating improve as gastric emptying returns to normal speed. Food moves through your system faster again, which can feel like a relief after months of slowed digestion.
Acid reflux and heartburn (reported by some users, especially at higher doses) tends to diminish as the medication leaves.
Injection site reactions — redness, itching, or bumps at the injection site — resolve completely.
Energy and fatigue: Some people report feeling more energetic after stopping, particularly if the medication suppressed their appetite to the point where they were under-eating. When you're getting adequate nutrition again, energy may improve.
The tradeoff is real, though
The side effects that resolve are the same mechanisms that were helping you lose weight. Faster digestion means less satiety. No nausea means no natural portion control. The appetite-suppressing effects and the unpleasant GI effects are two sides of the same pharmacological coin.
If your side effects were severe enough that they were significantly impacting your quality of life, stopping or switching medications is completely valid. Quality of life matters. But if your side effects were mild to moderate and manageable, it's worth weighing them against the benefits — especially since most GI side effects diminish over time with continued use.
Missed Doses, Shortages, and Restarting GLP-1
Missing a dose or two isn't the same as permanently stopping — but there are important differences in how you handle it.
The two-week threshold
If you've missed roughly two weeks of doses, contact your prescriber before restarting at your previous dose. UCLA Health notes that after two missed doses (~14 days), some people experience significant GI side effects if they resume at the same dosage and may need a lower restart dose. Most clinicians recommend re-titrating (starting at a lower dose and working back up) if you've been off for more than 2 weeks.
Restarting after a longer break
If you've been off for a month or more, plan for a full re-titration from the starting dose. This is frustrating but necessary. The good news: the medication will work again. There's no evidence of "tolerance" that would make it permanently less effective.
In a large real-world cohort study, 36.3% of people without type 2 diabetes who discontinued GLP-1 therapy restarted within 1 year, and 46.4% restarted within 2 years. If that's you, there's nothing wrong with it. Chronic conditions often require treatment adjustments.
If you're dealing with a medication shortage
Drug shortages for GLP-1 medications have been a recurring issue. Supply has improved and the FDA has removed some GLP-1 products from shortage lists, but availability can still vary by dose, pharmacy, and location — check current local supply with your prescriber or pharmacy. If you can't fill your prescription:
- Contact your prescriber immediately — they may be able to switch you to an available alternative
- Do not try to "stretch" doses by cutting them in half or skipping weeks without guidance
- Consider the telehealth providers that may have better access to inventory
When weight starts coming back despite your best efforts
It happens. Even with perfect habits, biology is powerful. If weight is trending up and you've genuinely been consistent with nutrition and exercise, you have options:
Restarting GLP-1 medication is always on the table. The drugs work when restarted — there's no "tolerance" that makes them less effective the second time around. You'll need to re-titrate, but the weight loss effects return.
Switching to a different GLP-1 may help. Some people who plateau on semaglutide respond well to tirzepatide, and vice versa. Tirzepatide acts on both GLP-1 and GIP receptors, which may provide a different (sometimes stronger) response.
Oral weight-management medications as a bridge. Research is underway on whether medications like bupropion-naltrexone (Contrave) can help maintain weight loss during and after GLP-1 discontinuation. These oral agents aren't as powerful as injectable GLP-1s, but they may help manage appetite during the transition.
For significant obesity, bariatric surgery remains the most durable intervention. Patients typically experience 35–50% total body weight loss that is maintained long-term. If you've been on and off GLP-1 medications and keep experiencing regain, surgery may be worth discussing with your provider. It's not giving up — it's upgrading the tool.
Maintenance troubleshooting
"I'm doing everything right but still gaining." Your "everything right" may need recalibration. When you were losing weight, your calorie needs dropped. Post-medication, your appetite wants pre-loss calories but your body burns post-loss calories. You may need to track intake for a few weeks to find the new equilibrium.
"Cravings are overwhelming." Distinguish physical hunger from emotional eating. Physical hunger builds gradually and any food satisfies it. Emotional cravings hit suddenly and demand specific foods (usually high-sugar or high-fat). If it's emotional, address the emotion, not the food. If it's physical, you may be under-eating protein or fiber.
"I can't make myself exercise." Forget "should." Find movement you genuinely enjoy. Walking counts. Dancing counts. Playing pickleball counts. The best exercise for weight maintenance is the one you'll actually do three months from now. If you hate the gym, stop going to the gym and find something else.
"My partner/family isn't supportive." This is more common than people admit. If your household food environment works against you, have a direct conversation. If that's not possible, focus on what you can control: your meals, your snacks, your exercise routine. Consider working with a registered dietitian who can help you navigate shared kitchens and social eating.
What About Blood Sugar, Blood Pressure, and Heart Health?
Weight isn't the only thing that changes. GLP-1 medications improve a wide range of cardiometabolic markers — and most of those improvements reverse after stopping.
Blood sugar (if you have diabetes or prediabetes)
Blood glucose control deteriorates after discontinuation. The Lancet eClinicalMedicine meta-analysis found an average HbA1c increase of 0.65% in people with type 2 diabetes. Some people who were prediabetic before treatment and had normalized their glucose on GLP-1s saw prediabetes return.
If you have diabetes, your provider will need to monitor blood sugar closely and may need to add or adjust other diabetes medications.
Blood pressure
Returns to pre-treatment levels in most people. The STEP 1 Extension trial found that any blood pressure improvements from weight loss reversed within a year of stopping semaglutide.
Cholesterol and cardiovascular risk
Most cholesterol improvements reverse with weight regain. However, the STEP 1 Extension trial found a few bright spots: C-reactive protein (a marker of inflammation) and some cholesterol metrics stayed slightly improved even after weight regain. Researchers speculate this may be related to even modest amounts of retained weight loss providing some ongoing cardiovascular benefit.
The big picture: Wegovy is FDA-approved specifically for cardiovascular risk reduction in people with obesity and established heart disease. Stopping the medication may reverse those protective effects. If you're taking a GLP-1 partly for heart health, factor this heavily into your decision.
Special Situations
Pregnancy / Trying to Conceive
GLP-1 medications should be stopped before pregnancy. The Wegovy label specifically recommends discontinuation at least 2 months before planned conception to allow full drug clearance. For tirzepatide, discuss timing with your clinician — the drug has a shorter half-life (~5 days) but can still be present in the body for about a month after the last dose.
Work closely with your OB/GYN and prescribing provider. The gap between stopping medication and conceiving is a high-risk window for weight regain. Having strong nutrition and exercise habits established beforehand is critical.
Surgery or Anesthesia
Some anesthesiologists have raised concerns about GLP-1 medications and delayed gastric emptying during surgery (risk of aspiration). The American Society of Anesthesiologists has addressed this topic. If you have a planned surgery, discuss your GLP-1 medication with your surgical team well in advance. Your prescriber and anesthesiologist should coordinate on whether and when to pause the medication.
Eating Disorder History
If you have a history of disordered eating, the return of appetite and food noise after stopping a GLP-1 can be particularly destabilizing. Work with a therapist or counselor who specializes in eating disorders during the transition. The emotional dimension of discontinuation is real and deserves professional support — not just dietary advice.
Older Adults
JAMA Network Open data shows that older adults are more likely to discontinue GLP-1 medications. For this group, muscle loss (sarcopenia) is an especially serious concern. Regained weight is fat, not muscle — and age-related muscle loss plus treatment-related muscle loss can compound into meaningful functional decline. Resistance training is even more important for older adults on or coming off GLP-1 therapy.
The Truth About "GLP-1 Patches" and Supplement Lookalikes
If you've seen ads for "GLP-1 patches" or "natural GLP-1 boosters," you're not alone — this is one of the most common search queries we see. Let me be direct.
There are no FDA-approved GLP-1 receptor agonist patches as of early 2026. Some are in development, but nothing is available for prescription use. Products marketed as "GLP-1 patches" online are not the same class of medication and have not been evaluated for safety or efficacy by the FDA.
"Natural GLP-1" supplements (berberine, various fiber supplements, etc.) are not pharmacologically equivalent to GLP-1 receptor agonist medications. Some may have modest effects on blood sugar or satiety, but they are not substitutes for prescribed GLP-1 therapy. Don't let marketing convince you otherwise.
How to verify any GLP-1 product is legitimate:
- Is it an FDA-approved brand (Wegovy, Ozempic, Rybelsus, Zepbound, Mounjaro, Saxenda, Victoza)?
- Is it dispensed by a licensed pharmacy?
- Does it require a prescription?
- Is the active ingredient and concentration clearly labeled?
If the answer to any of these is "no," proceed with extreme caution.
Alternatives If You Can't Stay on GLP-1 (Or Don't Want To)
If GLP-1 medications aren't sustainable for you — whether because of cost, side effects, access, or personal preference — other options exist. None are as effective as GLP-1 receptor agonists for most people, but they're real tools with real evidence behind them.
Other FDA-approved weight management medications
- Bupropion-naltrexone (Contrave): An oral combination drug that reduces cravings and appetite. Less potent than injectable GLP-1s (typical weight loss of 5–10% vs. 15–20%), but it's oral, cheaper, and better tolerated by some people.
- Phentermine-topiramate (Qsymia): Another oral combination. Effective but carries cardiovascular and psychiatric considerations.
- Orlistat (Alli/Xenical): Works by blocking fat absorption. Modest weight loss, and the GI side effects (oily stool, urgency) deter many users.
- Wegovy tablet (oral semaglutide 25 mg): FDA-approved in December 2025 as the first oral GLP-1 for weight management. Available as of January 2026, with a self-pay starting price of $149/month. Discuss availability and dosing with your clinician — it's the same active ingredient as injectable Wegovy but a different formulation and dose.
- Rybelsus (oral semaglutide 7/14 mg): This is oral semaglutide approved for type 2 diabetes — not the same labeled indication or dosing as Wegovy for weight management. Weight loss can occur, but it's not indicated for that purpose.
Only a clinician can determine which medication (if any) is appropriate for your situation. This is not a recommendation — it's an overview of what exists.
Structured behavioral programs
Programs that combine nutrition coaching, exercise programming, and behavioral support have the most evidence for long-term weight maintenance without medication. They're not glamorous, but they work — and the BMJ meta-analysis noted that weight regain after stopping behavioral interventions is 4x slower than regain after stopping medication.
Bariatric surgery
For people with BMI ≥ 35 (or ≥ 30 with obesity-related health conditions), bariatric surgery offers the most durable weight loss intervention available. Average sustained weight loss is 35–50% of total body weight. If you've been cycling on and off GLP-1 medications with recurring regain, it may be worth a conversation with a bariatric specialist.
Reddit Says… Separating Real Experiences from Your Forecast
You've probably read posts on r/Ozempic or r/Semaglutide from people who stopped and shared their experience. Some are terrifying ("I gained it all back in 4 months"). Some are encouraging ("I've kept the weight off for a year"). Both are real experiences — but neither is your forecast.
Why experiences vary so much:
- Duration on medication: Someone who was on a GLP-1 for 3 months has a very different trajectory than someone who was on it for 2 years
- Dose: Higher doses create stronger appetite suppression and potentially more dramatic rebound
- Lifestyle changes made during treatment: The person who used the medication period to build habits has a massive advantage over the person who didn't
- Why they stopped: Planned tapering vs. insurance suddenly cutting off coverage vs. running out due to a shortage
- Individual biology: Metabolic response, genetics, gut microbiome, hormonal profile — all vary enormously
Use other people's stories as data points, not predictions. Your outcome will depend on your specific circumstances and the choices you make during the transition.
How We Built This Guide
This guide was built using the following methodology:
Clinical evidence sources: Published randomized controlled trials (STEP 1 Extension, SURMOUNT-4, STEP-10), systematic reviews and meta-analyses (BMJ January 2026, Lancet eClinicalMedicine November 2025), and observational studies (JAMA Network Open, Epic Research).
Regulatory sources: FDA prescribing information for Wegovy, Ozempic, Zepbound, Mounjaro, Rybelsus, Saxenda, and Victoza, accessed via DailyMed.
Clinical perspective: Named physician statements from academic medical centers including Yale New Haven Health, Stamford Health, Houston Methodist, Mayo Clinic, Henry Ford Health, Scripps Clinic, and ThedaCare.
Evidence hierarchy: We prioritize randomized controlled trials and systematic reviews over observational data, and observational data over expert opinion. Where evidence is limited (e.g., tapering protocols), we explicitly note that guidance is based on clinical practice rather than trial data.
What this guide is not: This is not medical advice. It's a research synthesis for informational purposes. Always consult your healthcare provider before making changes to your medication regimen. We are not physicians.
Affiliate relationships: Some links on this page are affiliate links. If you sign up through them, we may earn a commission. This does not influence our editorial content, which studies we cite, or how we present the evidence.
Update schedule: This guide is reviewed against new research every 90 days. Pricing information is re-verified every 90 days.
References
- Wilding JPH, Batterham RL, Davies M, et al. Weight regain and cardiometabolic effects after withdrawal of semaglutide. Diabetes Obes Metab. 2022;24(8):1553-1564. [PMC full text]
- Aronne LJ, Sattar N, Horn DB, et al. Continued treatment with tirzepatide for maintenance of weight reduction in adults with obesity: the SURMOUNT-4 randomized clinical trial. JAMA. 2024;331(1):38-48. [PubMed]
- West HW, Patel R, Engel S, et al. Weight regain after cessation of anti-obesity medications: a systematic review and meta-analysis. BMJ. 2026;388:e080347. (January 2026)
- Horn DB, Linetzky B, Davies MJ, et al. Cardiometabolic parameter change by weight regain on tirzepatide withdrawal: a post hoc analysis of the SURMOUNT-4 trial. JAMA Intern Med. Published online November 24, 2025. [PubMed]
- Wegovy (semaglutide) prescribing information. Novo Nordisk; 2025. [FDA label]
- Zepbound (tirzepatide) prescribing information. Eli Lilly; 2025. [Lilly PI]
- Lancet eClinicalMedicine systematic review/meta-analysis (November 2025): Weight and cardiometabolic changes after GLP-1 RA discontinuation.
- Rodriguez PJ, Zhang V, Gratzl S, et al. Discontinuation and reinitiation of dual-labeled GLP-1 receptor agonists among US adults with overweight or obesity. JAMA Netw Open. 2025;8(1):e2457349. [Full text]
- UCLA Health. Missed a dose or more of your GLP-1 medication? Here's what to do. [UCLA Health]
- Holt et al. Exercise and postprandial GLP-1 response: year-long supervised exercise program showing ~25% increase in late-phase GLP-1 vs usual-activity control group.
- Wegovy tablet (oral semaglutide 25 mg) prescribing information. FDA approved December 22, 2025. [FDA label]
- Rubino D, Abrahamsson N, Davies M, et al. Effect of continued weekly subcutaneous semaglutide vs placebo on weight loss maintenance. JAMA. 2021;325(14):1414-1425.
Frequently Asked Questions About Stopping GLP-1
What to Do Next
If you've read this far, you now know more about GLP-1 discontinuation than most healthcare articles will tell you. Here's your action summary based on where you are right now:
If you haven't stopped yet and are considering it:
Talk to your prescriber before making any changes. Ask specifically about: (1) a tapering schedule, (2) whether a lower maintenance dose makes sense, (3) switching to a more affordable provider if cost is the driver. Get a written plan for monitoring and agree on a "restart threshold" — the specific weight or symptom level at which you'd go back on medication. Don't leave these decisions vague.
If cost is driving your decision:
This is the most solvable version of the problem. Affordable GLP-1 providers exist, and staying on a lower dose at reduced cost is almost always a better outcome than stopping entirely. Manufacturer discount programs (NovoCare for Wegovy, LillyDirect for Zepbound) are worth checking even if you've been denied before — eligibility criteria change.
If you've already stopped and are watching the scale climb:
First: don't panic. Panic leads to crash dieting, which leads to worse outcomes. Second: implement the maintenance anchors — protein-first eating, resistance training, sleep. Third: track your weight weekly and compare against your "restart threshold." If you're trending past it, call your provider. Restarting medication is always an option and is not a failure.
If you have diabetes:
Contact your provider before any medication changes. Full stop. Blood sugar management needs to be adjusted alongside any GLP-1 discontinuation, and the stakes of getting this wrong are higher.
If you're navigating this alone and feeling overwhelmed:
You're managing a chronic condition. That's hard under the best circumstances, and harder when the tools you were relying on are being taken away (by cost, by side effects, by insurance). Seek support — from your provider, from a registered dietitian, from a therapist, from an online community. The people who do best after stopping GLP-1 are the ones who don't try to do it in isolation.
This is a chronic condition. There's no "finishing" treatment — there's managing it. And managing it well means having a plan, building habits that last, knowing when to adjust, and using every tool available to you.
Medical Disclaimer: This content is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions about a medical condition or medication changes. Never disregard professional medical advice or delay seeking it because of something you have read on this website.