Best GLP-1 for Perimenopause (2026): Verified Picks + Real Costs
Disclosure: Some links on this site are affiliate links. If you purchase through these links, we may earn a commission at no extra cost to you. Thank you for supporting our site.·For informational purposes only—not medical advice.
If you’re searching for the best GLP-1 for perimenopause, here’s your bottom line: it works, you’re not too late, and you have more affordable options than you probably think.
We spent 60+ hours verifying pricing, pharmacy sourcing, clinical evidence, and cancellation policies across four telehealth GLP-1 providers — specifically through the lens of what matters for women in perimenopause. Not generic weight loss advice. Not a list of brand names. A real answer to the question that brought you here.
The quick verdict:
- Best GLP-1 medication for most perimenopausal women: Tirzepatide (brand: Zepbound) — produces roughly 20% average weight loss in trials, works equally well regardless of reproductive stage. If you can’t access tirzepatide or prefer a longer track record: semaglutide (brand: Wegovy) at ~15% average weight loss.
- Best online program for most women paying cash: MEDVi — $179/mo to start for compounded semaglutide, no contract, 24/7 provider access, 100,000+ patients served. Refills lock at $299/mo.
- Best if a 3-month money-back guarantee matters to you: TrimRX — $199/mo, 100% medication refund if you follow the plan for 3 months and aren’t satisfied.
- Not for you if: You have a personal or family history of medullary thyroid cancer (MTC) or MEN2 syndrome, a history of pancreatitis, are pregnant or planning pregnancy, or have severe kidney/liver disease. (Source: FDA Wegovy Prescribing Information)
One honest thing before we go further: every provider below prescribes compounded GLP-1 medications, which are not FDA-approved as finished products. They contain the same active ingredient as brand-name Wegovy and Ozempic, but they’re prepared by compounding pharmacies rather than the original manufacturer. That’s how most women actually afford these medications — brand-name list prices can run $1,000+/month, and while manufacturers now offer cash-pay programs that may reduce costs for eligible patients (e.g., Wegovy and Zepbound have offered reduced cash pricing around $499/mo), many women either don’t qualify or find telehealth compounding more accessible. All four providers we reviewed use U.S.-licensed, FDA-registered compounding pharmacies. We’ll explain exactly what that means and how to verify safety in the section below.

GLP-1 Provider Comparison for Perimenopausal Women (Verified February 2026)
| MEDVi | TrimRX | Embody | SkinnyRX | |
|---|---|---|---|---|
| Starting Price (Semaglutide Inj.) | $179/mo | $199/mo | $99 first mo → $299/mo | $199/mo |
| Ongoing Price (Semaglutide Inj.) | $299/mo (locked) | $199/mo (starting) | $299/mo | $199–$299/mo |
| Tirzepatide Available | From $279/mo | From $349/mo | From $149 first mo → $399/mo | Tablets available |
| Oral/Tablet Options | From $249/mo | From $179/mo | Needle-free GLP-1 gum | Sublingual + tablets |
| Contract Required | No | No | No | No |
| Results Guarantee | 5-month (conditions apply) | 3-month 100% med refund | No formal guarantee | No formal guarantee |
| 24/7 Provider Access | Unlimited | Unlimited check-ins | 24/7 messaging | Patient portal |
| Lab Work | Included if needed (Quest) | Available | Not routinely required | Not routinely required |
| Pharmacy Partner | Belmar Pharmacy (U.S.-licensed) | U.S. FDA-registered | U.S.-licensed compounding pharmacy | U.S. FDA-registered |
| Trustpilot (Feb 2026) | 4.5/5 (~10K reviews) | 4.0/5 (~490 reviews) | Not rated here | 4.8/5 (~4,600 reviews) |
| Best For | Overall value + medical support | Budget + guarantee | Low first-month price + needle-free gum | Non-injection formats |
All providers offer compounded (not FDA-approved) GLP-1 medications. Prices are provider-stated and verified by WPG from official websites. Your actual cost may vary by medication type and dosage.
→ If your insurance covers brand-name Wegovy or Zepbound with a low copay, skip telehealth and use your insurance. The telehealth route below is for women paying out-of-pocket.
Which GLP-1 Provider Is Best for YOUR Perimenopause Situation?
We know that table has a lot of information. Here’s the simpler version — match yourself:
If you want the best overall value with real medical oversight → MEDVi
Lowest locked refill rate for injectable semaglutide ($299/mo includes everything). Over 100,000 patients. Partners with Belmar Pharmacy, one of the most established compounding pharmacies in the U.S. You get physician review, a personalized plan, metabolic report, and 24/7 messaging — which matters when you’re navigating GLP-1 side effects alongside perimenopause symptoms like sleep disruption and mood shifts. The 5-month results guarantee means you’re not trapped if it doesn’t work for you.
If a shorter money-back guarantee is your priority → TrimRX
Their 3-month satisfaction guarantee is the most accessible safety net in this comparison. If you follow the treatment plan for three consecutive months and aren’t satisfied, you may qualify for a 100% medication refund. Starting at $199/mo for compounded semaglutide with no membership fees.
If you want the lowest first-month price or a needle-free option → Embody
$99 gets you started on compounded semaglutide injection (then $299/mo ongoing). Embody also offers a needle-free GLP-1 gum option for women who’d rather skip self-injection — a genuine plus during perimenopause when you’re already managing a lot. Cash-pay, no insurance required (HSA/FSA accepted).
If you really don’t want to self-inject → SkinnyRX
The only provider here offering semaglutide in three formats: injectable, sublingual (under the tongue), and oral tablet. If needle anxiety is a real barrier — and for many women it is — SkinnyRX gives you alternatives.
If your insurance covers brand-name → Skip all of these
Check with your insurer first. If they cover Wegovy (semaglutide) or Zepbound (tirzepatide) with a copay you can sustain for 12+ months, that’s always the better option: FDA-approved, clinically tested at exact dosages, and covered by your plan.
Do GLP-1 Medications Actually Work for Perimenopausal Women?
Let’s not dance around this. You want to know: “Will this work for me, at my age, with my hormones?”
Yes. And the clinical evidence isn’t vague — it’s specific to your situation.
The study that matters most
In 2025, endocrinologists at Weill Cornell Medicine and NewYork-Presbyterian Hospital published a post-hoc analysis of 2,542 women from the SURMOUNT clinical trials (SURMOUNT-1, -3, and -4). They specifically broke out results by reproductive stage: premenopausal, perimenopausal, and postmenopausal.
The finding: Tirzepatide produced approximately 20% body weight reduction regardless of reproductive stage. Perimenopausal women lost just as much weight as younger women. The study also showed significant reductions in waist circumference and waist-to-height ratio — which matters because perimenopause shifts fat storage toward your midsection, and that visceral fat is the metabolically dangerous kind.
Lead author Dr. Beverly Tchang, an endocrinologist specializing in obesity medicine at Weill Cornell, noted that these findings are likely applicable to other GLP-1 medications as well. (Source: Tchang et al., published in Obesity, 2025)
The HRT combination evidence
A 2024 study published in the journal Menopause found that postmenopausal women taking both semaglutide AND hormone replacement therapy (HRT) lost significantly more weight than women on semaglutide alone — roughly 30% more at every checkpoint (3, 6, 9, and 12 months). (PubMed: 38446869)
A separate Mayo Clinic analysis found similar results with tirzepatide + HRT, with the combination group showing greater weight loss at every timepoint. (Mayo Clinic News Network)
This doesn’t mean HRT boosts GLP-1 effectiveness — it may be that HRT improves sleep, mood, and energy, which indirectly supports weight loss. But the signal is consistent: if you’re already on HRT or considering it, GLP-1 therapy may work even better alongside it.
You’re not a small group — you’re the biggest user demographic
RAND Corporation data from 2025 found that women aged 50–64 had the highest GLP-1 use overall, with 20% reporting current or past use. Women aged 30–49 were more than twice as likely as men to use GLP-1s. And yet — the RAND researchers explicitly warned that perimenopausal women have been “largely ignored” in GLP-1 clinical research. (RAND Corporation, August 2025)
You’re not an edge case. You’re the primary market. The research is catching up to what women already figured out.
The basic efficacy numbers
~15%
Semaglutide (Wegovy)
Average body weight loss over 68 weeks. 86% lost at least 5%; 69% lost at least 10%. (Source: STEP 1 trial; Wilding et al., NEJM 2021)
~20–22%
Tirzepatide (Zepbound)
Average body weight loss. Up to 90% achieved clinically meaningful weight loss of 5%+. (Source: SURMOUNT-1 trial; Jastreboff et al., NEJM 2022)
These numbers are from FDA-approved formulations at full therapeutic doses, combined with lifestyle modifications. Individual results vary. Compounded formulations have not undergone the same clinical trials, though they contain the same active pharmaceutical ingredients.
How GLP-1 Medications Work During Perimenopause (And Why It Matters)
What GLP-1 actually is
GLP-1 (glucagon-like peptide-1) is a hormone your body naturally produces in your gut after you eat. It does three things: tells your brain you’re full, slows how quickly food leaves your stomach, and helps your pancreas manage blood sugar.
GLP-1 medications (semaglutide, tirzepatide, liraglutide) mimic this hormone — but they last much longer in your body than the natural version. The result: you feel genuinely full with less food, your blood sugar stays more stable, and the constant “food noise” many women describe — that background hum of thinking about food — goes quiet.
Tirzepatide goes a step further. It’s a dual-action drug that activates both GLP-1 and GIP receptors, which is why trials show slightly greater weight loss. GI side effects are common with both medications, but in the SURMOUNT-5 head-to-head trial, drug discontinuation due to GI events was lower with tirzepatide (2.7%) than semaglutide (5.6%), and vomiting occurred less often with tirzepatide — though tolerability is individual and other side effects can vary between the two.
Why this matters MORE during perimenopause
Here’s the part most GLP-1 articles skip. During perimenopause, declining estrogen triggers a chain reaction that makes weight loss significantly harder:
Insulin resistance increases
Your cells become less responsive to insulin, so your body produces more. Elevated insulin promotes fat storage — especially around the midsection.
Metabolism drops 250–300 cal/day
Not because you’re lazy. Because your hormonal architecture physically changed — and many women move less without realizing it.
Visceral fat accumulates
Before perimenopause, women store fat in hips and thighs. After, it shifts to the belly — wrapping around organs and driving inflammation.
Appetite regulation breaks
Estrogen helps regulate leptin and ghrelin. When estrogen fluctuates unpredictably, so do your hunger signals.
GLP-1 medications directly address all four of these mechanisms. They improve insulin sensitivity, reduce appetite, target visceral fat, and stabilize blood sugar. That’s why they’re not just “another weight loss drug” for perimenopausal women — they’re working with the specific biology that changed.
A 2024 study in Biochemical Pharmacology even found direct interactions between GLP-1 and estrogen pathways in regulating fat metabolism — suggesting these medications may be particularly well-suited to the hormonal environment of perimenopause. (Source: Model et al., Biochemical Pharmacology, 2024;230:116623)
Semaglutide vs. tirzepatide: the quick comparison
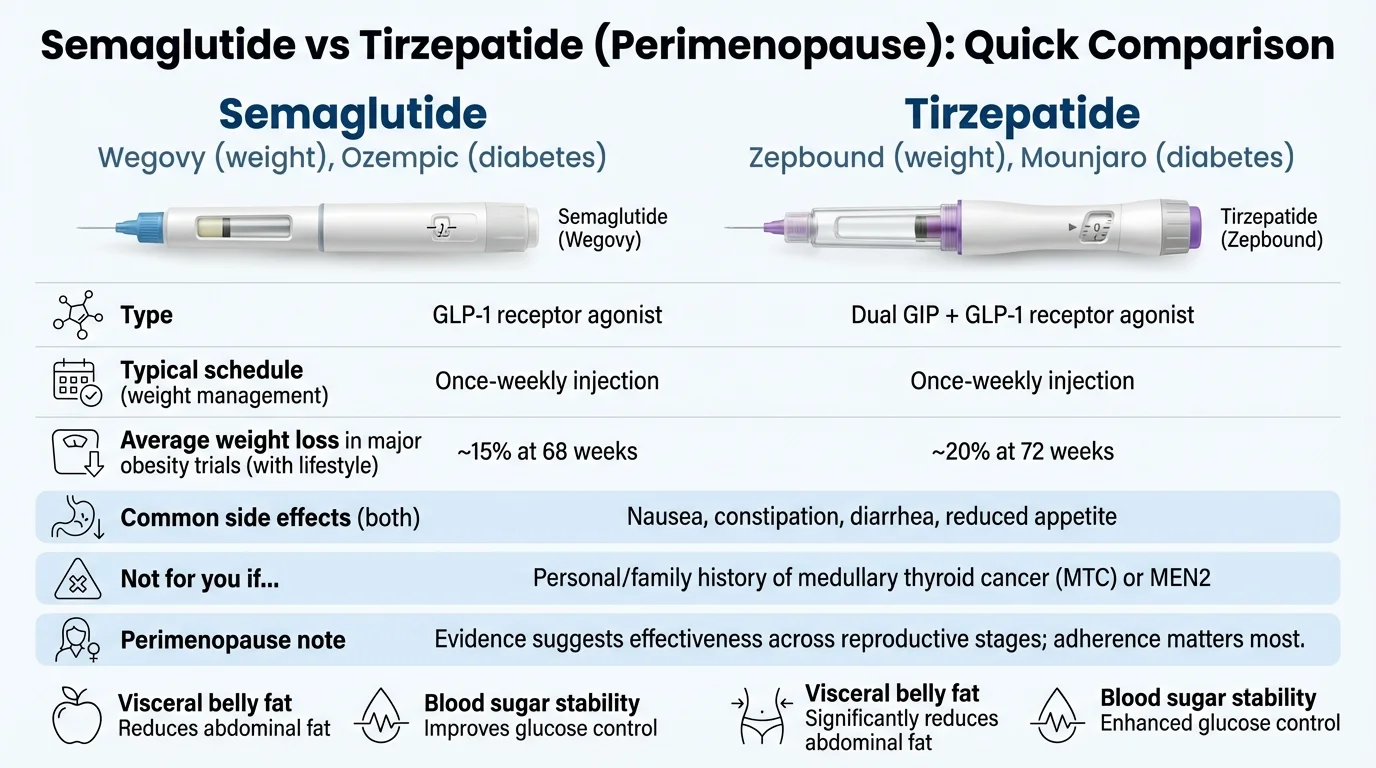
| Semaglutide | Tirzepatide | |
|---|---|---|
| How it works | GLP-1 receptor agonist (single action) | GLP-1 + GIP receptor agonist (dual action) |
| Brand names (weight loss) | Wegovy | Zepbound |
| Brand names (diabetes) | Ozempic | Mounjaro |
| Average weight loss | ~15% body weight (68 weeks) | ~20–22% body weight (72 weeks) |
| Dosing | Weekly injection (or daily oral) | Weekly injection |
| GI side effects | Common (nausea, constipation) | Common; lower discontinuation rate in SURMOUNT-5 |
| Track record | Longer (approved 2021 for weight loss) | Newer (approved 2023 for weight loss) |
| Cost (compounded, typical) | $179–$299/mo | $279–$399/mo |
| Best for | Proven track record, lower cost | Maximum weight loss, dual mechanism |
Both are effective for perimenopausal women. Tirzepatide tends to produce greater weight loss. Semaglutide costs less and has more long-term safety data. Your provider can help you decide based on your goals, budget, and health history.
MEDVi Review: Best Overall for Perimenopausal Women
One-sentence verdict: MEDVi offers the strongest combination of price, medical oversight, and patient volume for women using compounded GLP-1s during perimenopause — and their locked refill pricing means no surprises as your dose increases.
Who it’s best for
Women who want everything bundled — medication, physician review, personalized plan, metabolic report, and 24/7 provider access — at a predictable monthly cost. If you’re navigating GLP-1 therapy alongside perimenopause symptoms (and potentially HRT), having unlimited messaging with a clinical team isn’t a luxury. It’s how you avoid unnecessary ER visits and anxiety spirals over normal side effects.
What you actually get
- Physician review of your health history and goals
- Personalized treatment plan with dosing guidance
- Metabolic report
- Compounded GLP-1 medication shipped to your door (semaglutide or tirzepatide)
- 24/7 messaging + unlimited appointments with your care team
- No contract. Month-to-month billing. Cancel 72+ hours before your billing date.
Verified pricing (February 2026)
| Medication | First Month | Ongoing Refills |
|---|---|---|
| Compounded Semaglutide (injectable) | $179 | $299/mo |
| Compounded Tirzepatide (injectable) | $279 | Varies by dose (~$399–$499) |
| Compounded Semaglutide (tablets) | $249 | Varies |
| Brand-Name Ozempic (limited availability) | $1,999 | $1,999/mo |
Prices from medvi.org. “Locked” refill pricing applies to compounded semaglutide injections. Tirzepatide refills increase with dose escalation.
The results guarantee
MEDVi advertises “lose weight or your money back.” The fine print: you must follow the program for at least 5 months, document your adherence, and a 25% consultation fee is deducted from any refund. It’s not a month-one safety net — it’s designed for patients who genuinely commit and don’t see results. For routine cancellations, the key is canceling before the pharmacy processes your next order.
State availability
Available in 49 states (not North Dakota). Some states require a video consultation before prescribing (Kansas, Indiana, Mississippi, New Mexico, Oklahoma, West Virginia). Alabama and California patients can only receive injectable forms, not tablets. (Source: ConsumerAffairs MEDVi listing)
What real patients say
Reviewers commonly mention steady weight loss of 5–6 lbs/month, responsive medical support, and fast shipping. One verified ConsumerAffairs reviewer (Melany, November 2025) described losing 31 pounds on the semaglutide program and noted that family and friends commented on her “more youthful appearance” and that her confidence was restored.
Multiple Trustpilot reviewers highlight 24/7 doctor accessibility as a major differentiator, with one writing that online medication management “doesn’t feel dangerous” because MEDVi providers “are careful — order labs and schedule face-time appointments.”
Sources: ConsumerAffairs, Trustpilot
The honest downside (and why it’s not a dealbreaker)
MEDVi’s billing cycle starts from your sign-up date, not your medication delivery date. Several reviewers mention this caused initial confusion — they expected billing to begin when meds arrived, but the clock starts when you enroll. It’s a process thing, not a quality thing. How to avoid the surprise: When you sign up, note your enrollment date. That’s your billing date going forward. If you need to cancel, do it at least 72 hours before that date.
Everything else — the medication quality, provider access, and pricing transparency — checks out. With ~10,000 Trustpilot reviews averaging 4.5/5 stars and over 100,000 patients served, MEDVi has the track record to back up their claims.
Who MEDVi is NOT for
- Women whose insurance covers brand-name Wegovy or Zepbound with a low copay (use your insurance)
- Women in North Dakota (not available)
- Women who exclusively want brand-name, FDA-approved medications (MEDVi’s core offering is compounded)
Check If You Qualify for the MEDVi Program
Free eligibility check takes about 5 minutes. No commitment required. If approved, medication ships directly to your door — most patients have it in hand within 3–7 days.
Affiliate link. We may earn a commission at no extra cost to you. See our ranking methodology and full disclosure.
TrimRX Review: Best Budget Option with a Money-Back Guarantee
One-sentence verdict: TrimRX pairs competitive $199/mo pricing with the most accessible results guarantee in this comparison — making it a smart pick if you want a financial safety net while trying GLP-1 therapy for the first time.

What you get
- Compounded semaglutide from $199/mo or tirzepatide from $349/mo
- Free home delivery
- Unlimited check-ins with licensed providers
- No membership fees on top of medication cost
- 3-month results guarantee: follow the plan for 3 consecutive months, and if you’re not satisfied, you may be eligible for a 100% refund of medication costs
The honest downside (and the reframe)
Some BBB complaints mention billing confusion and difficulty canceling. A handful of reviewers report being charged for multiple months at once without realizing they’d signed up for a multi-month plan. Before you provide payment info, confirm in writing: “Am I signing up for monthly billing or a multi-month package?” Ask that one question and you avoid the issue entirely.
TrimRX’s 3-month guarantee is genuine value — most providers don’t offer anything comparable. And at $199/mo with no membership fee, the total financial commitment to “try it and see” is lower than almost any other route to GLP-1 therapy.
Affiliate link. We may earn a commission at no extra cost to you.
Embody Review: Low First-Month Price + Needle-Free Gum Option
One-sentence verdict: Embody gets you into GLP-1 therapy at $99 for your first month of compounded semaglutide injection (then $299/mo ongoing), and it’s one of the few programs offering a needle-free GLP-1 gum option for women who’d rather not self-inject.
What you get
- • Compounded semaglutide injection at $99 first month, $299/mo ongoing
- • Compounded tirzepatide injection from $149 first month, $399/mo ongoing
- • Needle-free GLP-1 gum option for needle-averse patients
- • Cash-pay, no insurance required (HSA/FSA accepted)
- • 24/7 messaging with your care team
- • Broad U.S. availability (confirm your state during intake)
The honest downside (and the reframe)
Embody doesn’t routinely require lab work before prescribing, which gets you started faster but removes a safety checkpoint. Most obesity medicine specialists recommend baseline labs (metabolic panel, thyroid, A1C) before starting GLP-1 therapy. Our suggestion: If you go with Embody, ask your personal doctor for recent labs or bring them to your first consultation.
Embody’s shipped options are compounded GLP-1 medications, not FDA-approved finished drugs, and a licensed provider decides whether treatment is appropriate. As with any telehealth compounding program, set realistic expectations for shipping timelines and confirm current pricing, pharmacy details, and state eligibility during intake.
Affiliate link. We may earn a commission at no extra cost to you.
SkinnyRX Review: Best for Non-Injection Formats
One-sentence verdict: SkinnyRX is the only provider in this comparison offering semaglutide in three delivery formats — injectable, sublingual, and tablet — making it the strongest pick if needle anxiety is a real barrier.

What you get
- • Injectable semaglutide from $199/mo
- • Sublingual semaglutide (daily, under the tongue)
- • Oral semaglutide tablets
- • Tirzepatide tablets
- • Branded Zepbound available (~$1,400/mo)
- • Overnight shipping from FDA-registered pharmacies
- • All 50 states
The honest downside (and the reframe)
SkinnyRX has strong Trustpilot reviews (4.8/5 from ~4,600 ratings) but limited presence on some other review platforms like ConsumerAffairs (only 2 reviews at time of writing). They’re a newer entrant in the telehealth GLP-1 space. The upside: their multi-format approach is genuinely differentiated, and Trustpilot feedback consistently highlights responsive customer support. If you’ve been avoiding GLP-1s because of needles, having sublingual and tablet options may be the thing that gets you started.
Affiliate link. We may earn a commission at no extra cost to you.
Tirzepatide vs. Semaglutide for Perimenopause: Which Should You Choose?
This is the medication-level decision most women get stuck on. Let’s make it simple.
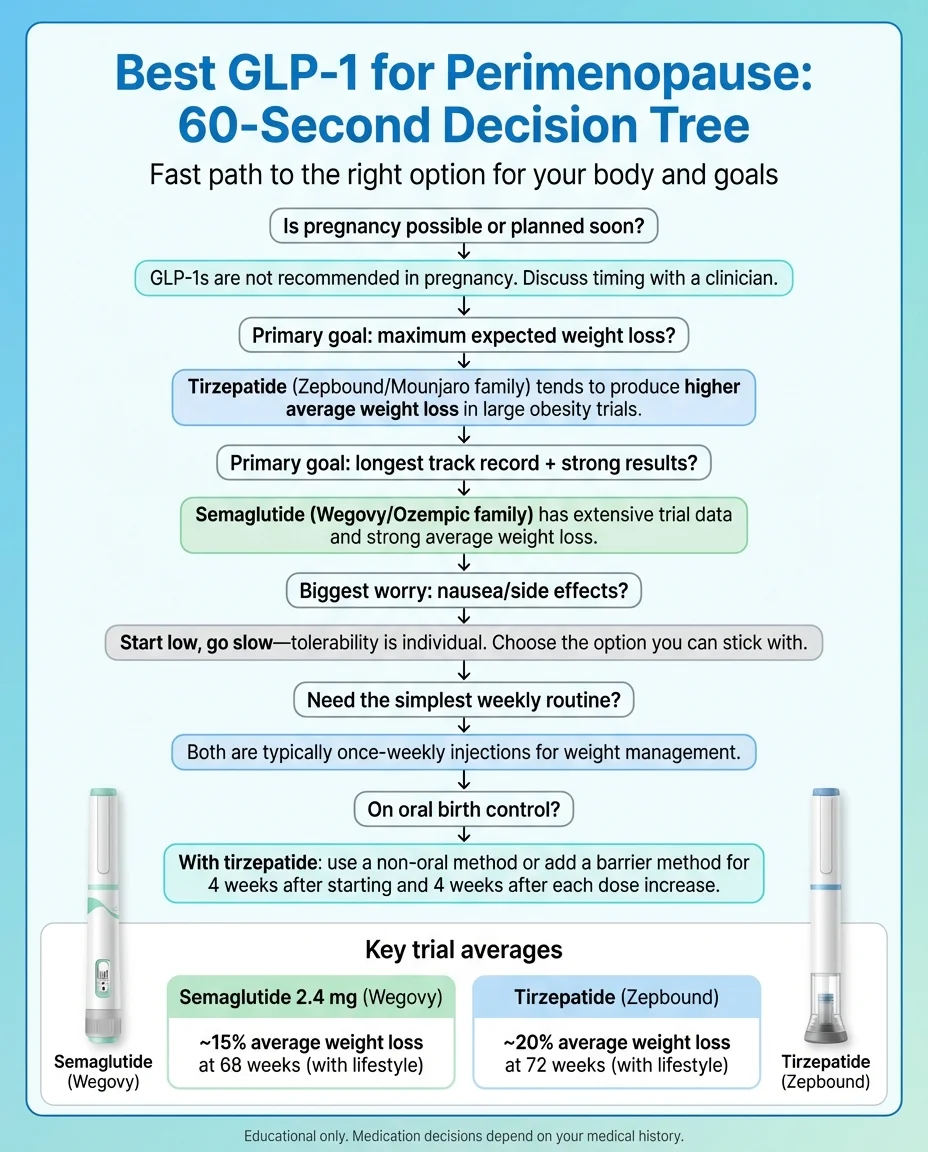
If maximum weight loss is your priority → Tirzepatide
Tirzepatide’s dual GLP-1/GIP mechanism consistently outperforms semaglutide in clinical trials. In one head-to-head comparison, tirzepatide users lost an average of 20.2% body weight compared to 13.7% for semaglutide at 72 weeks. That’s not a marginal difference — for a 200-pound woman, that’s roughly 40 pounds vs. 27 pounds.
The SURMOUNT post-hoc analysis confirmed this advantage holds for perimenopausal women specifically. And interestingly, some studies suggest the GIP receptor activation in tirzepatide may help preserve slightly more lean muscle mass compared to GLP-1-only medications — though the evidence on this is still emerging.
The tradeoff: tirzepatide is newer (FDA-approved for weight loss in 2023 vs. 2021 for semaglutide) and costs more through compounding ($279–$399/mo vs. $179–$299/mo).
If you want the longest track record and lower cost → Semaglutide
Semaglutide has been studied in large-scale obesity trials since 2017 and has FDA approval for weight loss (as Wegovy) since 2021. We have more long-term safety data on semaglutide than tirzepatide. For women who prefer the comfort of a more established medication history, that matters.
It’s also significantly cheaper through compounding — as low as $179/mo for injectables at MEDVi. Over 12 months, the savings add up: roughly $1,200–$2,400 less than a tirzepatide regimen. And 15% average weight loss is not small. For most perimenopausal women dealing with 20–40 pounds of hormonal weight gain, semaglutide can get you to your goal.
If GI tolerability is a concern → The picture is nuanced
Both drugs cause nausea, constipation, and diarrhea — especially during dose escalation. In the SURMOUNT-5 head-to-head trial, fewer tirzepatide users discontinued due to GI events (2.7% vs. 5.6%), and vomiting was reported less often with tirzepatide. However, nausea rates were broadly similar between the two. Some researchers believe GIP activation may buffer certain GI effects, but tolerability is genuinely individual — some women do better on one versus the other. If you start one and can’t tolerate it, switching to the other is a reasonable conversation with your provider.
The practical decision
For most perimenopausal women paying cash through telehealth:
- Start with compounded semaglutide if budget matters and you want the most established option
- Choose tirzepatide if you can afford the higher price and want the strongest expected results
- Either works. The best GLP-1 is the one you can afford, tolerate, and stick with for 12+ months.
What Is GLP-1 Microdosing — and Does It Make Sense in Perimenopause?
GLP-1 microdosing means using a dose below the standard therapeutic level — typically staying in the 0.25–0.5mg range for semaglutide rather than titrating up to the maximum 2.4mg. The idea: get appetite control and metabolic benefits with fewer side effects.
What clinicians are seeing
Dr. Kathleen Jordan, Chief Medical Officer at Midi Health (a telehealth platform specializing in midlife women), has reported that “many women don’t need to go to the maximum dose when they’re using GLP-1s for weight loss.” Some practitioners find that perimenopausal women, who may only need to lose 15–30 pounds rather than 80+, respond well to lower doses that minimize muscle loss and GI side effects.
What the evidence says
Here’s the honest truth: there are no published clinical trials specifically studying GLP-1 microdosing. No national guidelines recommend it. The dose-response data from the STEP and SURMOUNT trials shows that higher doses produce greater weight loss — but they also produce more side effects.
Microdosing is essentially an off-protocol clinical judgment call made between a patient and their provider. It makes intuitive sense for some women, particularly those who have less weight to lose (15–30 pounds vs. 80+), are extremely side-effect sensitive, want to minimize muscle loss, or are combining GLP-1 therapy with HRT and lifestyle changes that provide additional metabolic support.
Our take
If microdosing interests you, bring it up with your provider. Ask: “Given my weight loss goals and my perimenopause status, do I need the maximum dose, or could we try staying at a lower maintenance level?” A good provider will work with you on dosing rather than following a rigid escalation protocol. Just understand that at lower doses, weight loss may be slower and more modest. That’s the tradeoff — and for some women, it’s the right one.
Can You Take GLP-1 Medications with HRT During Perimenopause?
This is one of the most common questions we see — and the answer is encouraging.
What we know
The 2024 Menopause journal study found that postmenopausal women on HRT + semaglutide lost approximately 30% more weight at every timepoint compared to semaglutide alone. A Mayo Clinic analysis found similar enhanced results with HRT + tirzepatide.
The proposed mechanism: HRT restores the hormonal environment (reducing insulin resistance, improving sleep, stabilizing mood, preserving muscle) while GLP-1s drive appetite control and fat loss. One researcher described it as “fixing the foundation and remodeling the house at the same time.”
Important: These are observational studies, not randomized controlled trials. We can’t say HRT causes better GLP-1 outcomes — it may be that women on HRT simply have better sleep, more energy, and more capacity for the lifestyle changes that support weight loss. But the signal is consistent and promising.
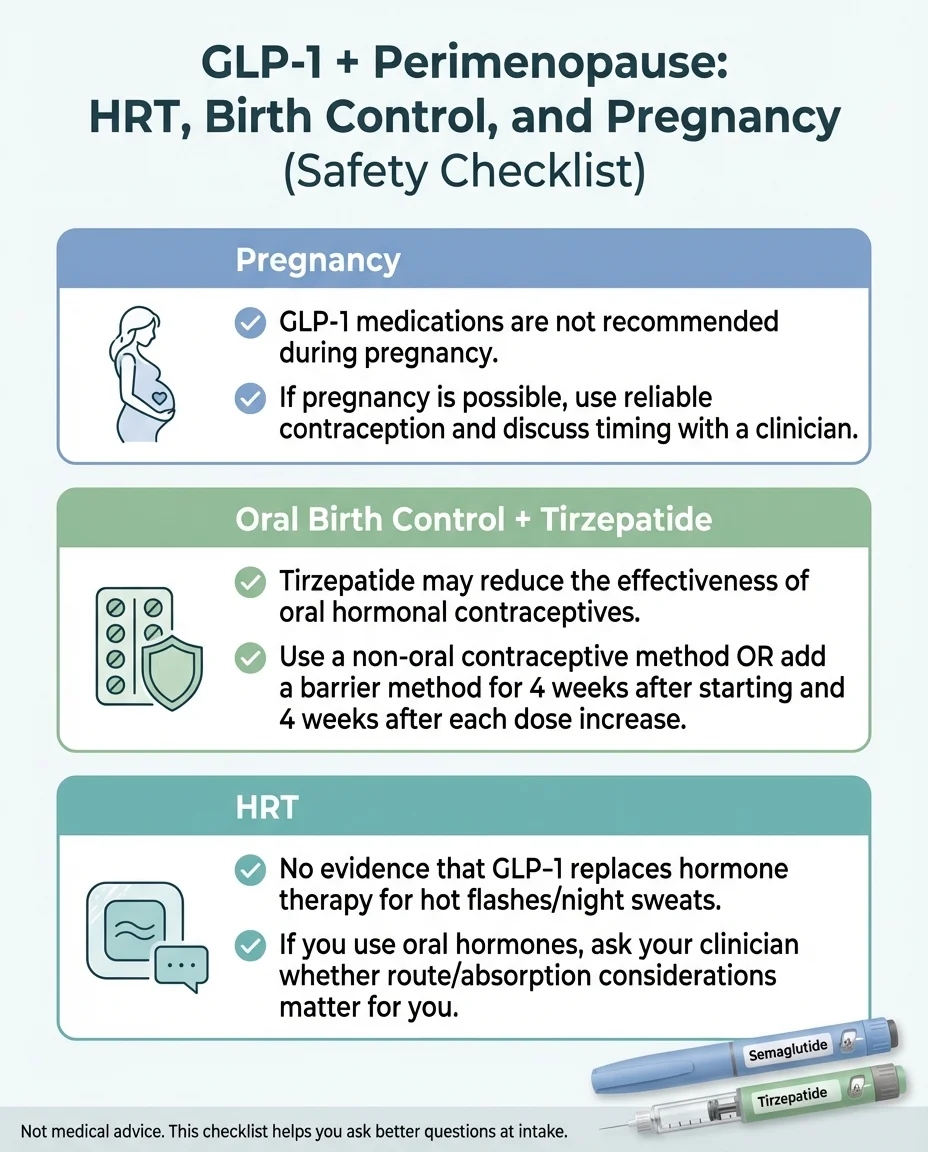
The caution most pages don’t mention
If you take oral hormone therapy or oral hormonal contraceptives and you start tirzepatide, read this carefully: tirzepatide slows gastric emptying, which can reduce the absorption of oral medications — including oral birth control pills. The FDA label for Zepbound (tirzepatide) specifically warns that oral hormonal contraceptives may be less effective, and recommends switching to a non-oral contraceptive method or adding a barrier method for 4 weeks after starting tirzepatide and for 4 weeks after each dose increase. (Source: FDA Zepbound Prescribing Information)
If you’re on oral HRT (estrogen/progesterone pills): Discuss with your provider whether switching to transdermal patches or topical forms might make sense while on a GLP-1, to ensure consistent absorption. This isn’t a dealbreaker — it’s a conversation to have at intake.
Questions to ask your provider
- • “I’m on [specific HRT]. Should we adjust my hormone delivery method while I’m on a GLP-1?”
- • “Do I need to use additional birth control while on tirzepatide?” (If you’re still menstruating)
- • “How should we coordinate my HRT management with my GLP-1 titration schedule?”
What Are the Side Effects of GLP-1s During Perimenopause?
We’re not going to sugarcoat this — but we’re also not going to scare you out of a decision that could genuinely change your health trajectory.
Common side effects (usually temporary)
Most side effects peak during the first few weeks and during dose increases, then fade:
- Nausea — the most reported side effect. Usually mild to moderate. Tends to improve significantly after 4–8 weeks.
- Constipation — common, and can feel worse during perimenopause when hormonal shifts already slow digestion.
- Diarrhea — less common than constipation, but happens during adjustment periods.
- Reduced appetite — this is technically the mechanism, not a side effect. But it can feel strange at first.
- Fatigue — usually temporary as your body adjusts.
Less common but important
- Pancreatitis risk — rare, but report severe abdominal pain immediately.
- Gallbladder issues — rapid weight loss can trigger gallstones in some people.
- Potential thyroid concerns — GLP-1 medications carry a boxed warning about thyroid C-cell tumors observed in rodent studies. Contraindicated for anyone with a personal or family history of medullary thyroid carcinoma (MTC) or MEN2 syndrome.
The perimenopause-specific concern you need to know about
GLP-1 medications reduce both fat AND muscle mass. On average, about 25–40% of weight lost on GLP-1s is lean mass (muscle). This is a real concern during perimenopause, when you’re already losing muscle from declining estrogen. The combination — hormonal muscle loss + medication-induced muscle loss — can accelerate sarcopenia (age-related muscle wasting) if you’re not proactive.
Even more concerning: if you stop the medication, clinical trial follow-up shows many people regain a large portion of weight — about two-thirds of prior weight loss within one year in the STEP 1 extension study (Source: Wilding et al., NEJM 2022). Building muscle and healthy habits while on the medication is your best insurance against regain.
The solution is not to avoid GLP-1s. The solution is to protect your muscle from day one:
- Strength training 2–3x per week — non-negotiable. Resistance exercise is the single most important thing you can do while on a GLP-1.
- Protein: aim for 25–30g per meal — most perimenopausal women under-eat protein. Your muscles need the building blocks.
- Adequate hydration — GLP-1s can reduce your thirst signals. Set reminders to drink.
- Work with your provider on slow titration — start low, go slow. Aggressive dose escalation can accelerate muscle loss.
How to minimize GI side effects
- • Start at the lowest dose and increase gradually
- • Eat smaller, more frequent meals
- • Avoid high-fat, greasy foods (especially during titration)
- • Increase fiber slowly — not all at once
- • Skip carbonated drinks (they worsen bloating when digestion is already slowed)
- • Stay hydrated even when you don’t feel thirsty
- • If nausea persists, ask your provider about prescription anti-nausea medication
How Much Do GLP-1s Cost — and Will Insurance Cover It?
Let’s be direct about money.
Brand-name pricing (without insurance)
| Medication | List Price (Cash) | Cash-Pay Program Price* |
|---|---|---|
| Wegovy (semaglutide for weight loss) | ~$1,349/mo | ~$499/mo (if eligible) |
| Ozempic (semaglutide for diabetes, off-label) | ~$900–$1,400/mo | Varies by program |
| Zepbound (tirzepatide for weight loss) | ~$1,060/mo | ~$299–$499/mo (vial program, if eligible) |
| Mounjaro (tirzepatide for diabetes) | ~$1,000–$1,200/mo | Varies by program |
*Manufacturer cash-pay programs have eligibility requirements and terms that change. Always verify current availability and your eligibility directly with the manufacturer.
The insurance reality
Most insurance plans cover GLP-1s for type 2 diabetes. Coverage for weight loss is a different story — many plans exclude it, require extensive prior authorization, or impose strict BMI and comorbidity requirements.
What to do: Call your insurance company and ask specifically: “Does my plan cover Wegovy or Zepbound for weight management? What are the prior authorization requirements?” Get a clear yes or no before assuming you need the telehealth route.
Compounded pricing (what most women actually pay)
| Provider | Semaglutide (Inj.) Start | Semaglutide (Inj.) Ongoing | Tirzepatide Start |
|---|---|---|---|
| MEDVi | $179/mo | $299/mo | $279/mo |
| TrimRX | $199/mo | $199/mo | $349/mo |
| Embody | $99/mo | $299/mo | $149/mo |
| SkinnyRX | $199/mo | $199–$299/mo | Tablets available |
HSA/FSA
Most of these providers state they accept HSA and FSA cards, but eligibility depends on your specific plan — confirm at checkout and with your plan administrator before assuming coverage.
The long-term math
GLP-1 treatment typically runs 12–24+ months for meaningful, sustained results. At $200–$300/month, that’s $2,400–$7,200 over 1–2 years. It’s real money. But consider the comparison: obesity-related medical expenses (diabetes management, cardiovascular care, joint problems) average $10,000–$20,000+ per year in the U.S. For many women, GLP-1 therapy is the less expensive path when measured against what untreated metabolic dysfunction costs over a decade.
Are Compounded GLP-1 Medications Safe?
This is the trust question — and you deserve a straight answer.
What “compounded” actually means
Compounding pharmacies take the same active pharmaceutical ingredient (semaglutide or tirzepatide) and prepare it into a finished medication. This is legal and common — compounding has existed for decades for medications where commercial versions are unavailable, in shortage, or cost-prohibitive.
What the FDA says
The FDA has issued cautions about compounded GLP-1 medications, citing risks including:
- Contamination during preparation
- Incorrect concentrations (too much or too little active ingredient)
- Temperature mishandling during shipping that can reduce effectiveness
- Use of salt forms (like semaglutide sodium) that differ from the approved drug
These are real risks — but they’re risks associated with poorly run compounding pharmacies, not with compounding as a practice.

How to protect yourself
- Verify the pharmacy is U.S.-licensed and FDA-registered. All four providers we reviewed use pharmacies that meet this standard.
- Ask about third-party testing. Reputable compounders test each batch for potency and sterility.
- Check shipping conditions. Medication should arrive properly refrigerated (for injectables) with cold packs.
- Avoid “research peptide” sites. If a website sells semaglutide without a prescription or provider consultation, walk away.
How to verify your compounded GLP-1 is what it claims
- Check the label. Your vial or pen should identify the compounding pharmacy by name, the active ingredient, the concentration, and an expiration date.
- Confirm semaglutide base vs. salt form. The FDA-approved form uses semaglutide base. Some compounders have used semaglutide sodium (a salt form), which the FDA has flagged as not interchangeable.
- Verify the pharmacy license. Every state pharmacy board maintains a public lookup. Search for the pharmacy name to confirm their license is active and in good standing.
- Understand 503A vs. 503B. A 503A pharmacy compounds individual prescriptions for specific patients. A 503B is an “outsourcing facility” registered with the FDA that can compound in larger batches under stricter federal oversight. Both are legal; 503B facilities undergo more frequent FDA inspections.
- Ask about third-party testing. Reputable compounders test each batch for potency (correct concentration) and sterility. If they can’t confirm this, that’s a red flag.
- Check shipping conditions. Injectable semaglutide and tirzepatide should arrive cold-shipped with gel packs or insulation. If it arrives warm, contact the pharmacy before using it.
Bottom line: Compounded ≠ unsafe. But quality depends entirely on the pharmacy. The providers we reviewed partner with pharmacies that meet federal and state licensing standards. For more detail, see our full guide: Is Compounded Semaglutide Safe?
Does GLP-1 Help with Other Perimenopause Symptoms (Beyond Weight)?
GLP-1 medications are FDA-approved for weight management and type 2 diabetes. They are not a replacement for hormone therapy when it comes to classic perimenopause symptoms like hot flashes, night sweats, and vaginal dryness. HRT remains the first-line treatment for vasomotor symptoms.
That said, several secondary benefits are emerging in the research:
- Improved insulin sensitivity — which can reduce the energy crashes and sugar cravings that intensify during perimenopause
- Reduced systemic inflammation — by shrinking visceral fat, which is itself highly inflammatory tissue
- Better cardiovascular markers — blood pressure, cholesterol, and triglycerides often improve
- Early evidence on hot flash reduction — some researchers hypothesize that GLP-1s modulate the hypothalamus, potentially reducing hot flash severity. This is preliminary — not a reason to choose GLP-1s for this purpose alone.
- Improved sleep — indirectly, through weight loss and reduced sleep apnea risk
- Reduced “food noise” — many women report this as life-changing, describing the mental relief of not constantly thinking about food
If weight is the perimenopause symptom that’s stealing your confidence, your energy, and your sense of self — addressing it can ripple outward in ways that affect everything else. That matters. It’s not vanity. It’s metabolic health.
The Perimenopause-Specific Risks Most GLP-1 Articles Don’t Mention
Bone density
Perimenopause already accelerates bone density loss due to declining estrogen. Rapid weight loss from any cause — including GLP-1s — can further reduce bone mineral density. If you have existing osteopenia or osteoporosis risk factors, discuss bone-protective strategies with your provider (weight-bearing exercise, adequate calcium/vitamin D, possible DEXA scan baseline).
Constipation compounding
GLP-1s slow gastric emptying. Perimenopause’s hormonal fluctuations also slow gut motility. The combination can make constipation significantly worse than what you’d experience from either factor alone. Build fiber intake gradually and stay ahead of it with hydration — don’t wait until it’s a problem.
Mood and “menofog”
Some women report mood changes on GLP-1s — this can be difficult to distinguish from the mood shifts, anxiety, and brain fog that perimenopause itself causes. Keep a simple symptom journal so you and your provider can identify what’s medication-related versus hormone-related. This is especially important if you’re adjusting multiple treatments simultaneously.
Fertility and pregnancy
If you’re in perimenopause and still menstruating, you can still get pregnant. GLP-1 medications are contraindicated during pregnancy. Use reliable contraception — and remember that oral hormonal contraceptives may be less effective while on tirzepatide. Semaglutide should be stopped at least 2 months before a planned pregnancy due to its long half-life. For tirzepatide, some manufacturer guidance recommends stopping about 1 month before a planned pregnancy — discuss exact timing with your clinician.
How to Start a GLP-1 in Perimenopause (Step by Step)
Choose your medication path
Brand-name (FDA-approved): If your insurance covers it, always try this first. Call your insurer. Compounded (telehealth): If insurance doesn’t cover weight management GLP-1s, this is the most common affordable route.
Check your eligibility
Most providers require a BMI of 30+ (or 27+ with a weight-related health condition like hypertension, high cholesterol, type 2 diabetes, or sleep apnea). You’ll complete a health questionnaire covering medical history, current medications, and goals.
Ask these questions at your intake
"I’m in perimenopause — how does that affect my treatment plan?" • "I’m on [specific medications/HRT] — are there interactions?" • "Do I need baseline labs?" • "What’s your approach to dose titration?" • "What’s the plan for muscle preservation?" • "What are the cancellation/refund terms?" • "Which compounding pharmacy fills my prescription, and are they U.S.-licensed?"
Build your muscle protection plan BEFORE you start
Commit to strength training 2–3x/week. Track protein intake: aim for 25–30g per meal, ~100g daily minimum. Consider creatine supplementation (emerging evidence supports it for perimenopausal women).
Track the right metrics
Don’t just weigh yourself. Track: waist circumference (most meaningful visceral fat indicator), protein intake, strength training frequency, side effects (type, severity, duration), energy and mood, and sleep quality.
What Happens When You Stop GLP-1 Medications?
We believe in setting expectations honestly. Most clinical data shows that when patients discontinue GLP-1 therapy, a significant portion of weight is regained — about two-thirds of prior weight loss within one year in the STEP 1 extension trial. (Source: Wilding et al., NEJM 2022) This is relevant for all patients, but especially for perimenopausal women navigating natural metabolic changes.
This doesn’t mean you’ll be on medication forever (though some women choose to be). It means you need a plan:
- Discuss maintenance dosing. Some providers transition patients to lower maintenance doses rather than stopping completely.
- Lifestyle habits matter most after discontinuation. The strength training, protein intake, and eating patterns you build while on the medication become your long-term strategy.
- HRT may help. If you’re on hormone therapy, maintaining it may help preserve some of the metabolic improvements gained during GLP-1 treatment.
The goal isn’t dependency. It’s using the medication as a window to reset your metabolism, build new habits, and then transition with medical guidance — not cold-turkey.
Who Should NOT Use GLP-1 Medications
This is non-negotiable. Do not start GLP-1 therapy if:
- Personal or family history of medullary thyroid carcinoma (MTC) or MEN2 syndrome — boxed warning on all GLP-1 medications
- History of pancreatitis — discuss with your doctor; may be a contraindication
- Pregnant, breastfeeding, or planning pregnancy — semaglutide should be stopped at least 2 months before planned conception; tirzepatide guidance varies
- Severe kidney or liver disease — requires specialized monitoring beyond what most telehealth platforms provide
- Active or recent eating disorder — GLP-1s alter appetite regulation; discuss with a mental health provider first
- Diabetic retinopathy requiring close monitoring — may require in-person care rather than telehealth
If you have any of these conditions, the right move is to discuss options with an in-person healthcare provider who can monitor you appropriately.
How We Ranked “Best GLP-1 for Perimenopause” (Our Methodology)
We evaluated each provider across these criteria, weighted toward what matters most for perimenopausal women specifically:
- Total cost transparency — first-month pricing AND ongoing refill costs, including how prices change with dose escalation
- Clinical support quality — access to providers, frequency of check-ins, ability to message with questions (critical when managing GLP-1s alongside perimenopause)
- Medication options — availability of both semaglutide and tirzepatide, injectable and oral formats
- Pharmacy sourcing — named pharmacy partners, U.S. licensing, FDA registration status
- Patient review volume and quality — Trustpilot and ConsumerAffairs ratings, with attention to complaints that indicate systemic issues vs. individual experiences
- Guarantee/refund policy — what protection exists if it doesn’t work
- State availability — how many states are served and what restrictions apply
- Cancellation friction — how easy it is to stop if you need to
What we verified
- • Pricing from official provider websites (verified February 2026)
- • Pharmacy partners named on provider sites
- • Trustpilot and ConsumerAffairs ratings and review counts
- • BBB listings and complaint patterns
- • State availability from provider FAQs and third-party reviews
What we did not do
We did not personally enroll in and test all four providers. Our comparisons are based on published pricing, patient reviews, provider documentation, and third-party analysis. We’re transparent about that.
How we handle affiliate relationships
We earn commissions through affiliate links on this page. This does not affect our rankings. We rank based on value to the perimenopausal reader, not commission rates. Our methodology is published above. If a provider changed their pricing, support, or quality, we would update our rankings accordingly. See our full ranking methodology.
Frequently Asked Questions: GLP-1s and Perimenopause
Your 5-Step Quick-Start Checklist
Print this. Stick it on your fridge. Come back to it when you’re ready.
Check insurance first.
Call your plan and ask about Wegovy/Zepbound coverage. If they cover it with a low copay, start there.
If paying cash, pick your provider.
Use our comparison table above. MEDVi for best overall value. TrimRX for guarantee. Embody for a low first-month price or a needle-free gum option. SkinnyRX for non-injection.
Confirm you’re safe to start.
No MTC/MEN2 family history. No active pregnancy or plans. No pancreatitis history. Tell your provider EVERY medication you take — especially HRT and birth control.
Protect your muscle from day one.
Strength train 2–3x/week. Hit 25–30g protein per meal. This isn’t optional — it’s what separates women who thrive on GLP-1s from those who end up with less muscle than they started with.
Set realistic expectations.
Most women lose 1–2 pounds per week after the first month. The first few weeks may include nausea and adjustment. Meaningful results show up at 3–6 months. This is a marathon, not a sprint — but the science says you will get there.
Ready to Find the Right GLP-1 Program for You?
Most women start with MEDVi — $179 first month, no contract, 24/7 provider access, and medication shipped directly to your door. Free eligibility check takes about 5 minutes.
Affiliate link. We may earn a commission at no extra cost to you. This never affects our recommendations. Full disclosure.
Update + Verification Log
- • February 2026: Initial publication. All provider pricing verified from official websites. Clinical evidence current through January 2026. Trustpilot and ConsumerAffairs ratings verified.
- • Next scheduled review: March 2026 (pricing + provider status re-verification)
If you notice a pricing change or policy update before we do, contact us. We want this page to stay accurate.
You didn’t gain this weight because you stopped trying. Your hormones changed the rules — and that’s not a moral failure, it’s biology. GLP-1 medications give you a tool that works WITH that biology instead of against it. The clinical evidence says it works for women like you. The only question left is which path fits your life.
— The WPG Research Team
Sources cited in this article
- • Tchang et al., “Tirzepatide efficacy by reproductive stage,” Obesity, 2025
- • Wilding et al., “Once-Weekly Semaglutide in Adults with Overweight or Obesity,” NEJM, 2021 (STEP 1)
- • Wilding et al., “Weight regain and cardiometabolic effects after withdrawal of semaglutide,” Diabetes, Obesity and Metabolism, 2022 (STEP 1 extension)
- • Jastreboff et al., “Tirzepatide Once Weekly for Treatment of Obesity,” NEJM, 2022 (SURMOUNT-1)
- • Muskiet et al., “Tirzepatide vs. Semaglutide for Obesity Treatment,” NEJM, 2025 (SURMOUNT-5)
- • RAND Corporation, “GLP-1 Agonists in Perimenopause: Unique Risks and Potential Opportunities,” August 2025
- • Weight loss response to semaglutide with and without HRT, Menopause journal, 2024 (PubMed: 38446869)
- • Mayo Clinic News Network, “New study links combination of hormone therapy and tirzepatide to greater weight loss after menopause”
- • Model et al., “Interactions between GLP-1 and estrogens regulates lipid metabolism,” Biochemical Pharmacology, 2024
- • FDA Prescribing Information: Wegovy (semaglutide), Zepbound (tirzepatide)
- • ConsumerAffairs: MEDVi reviews (November 2025)
- • Trustpilot: MEDVi, TrimRX ratings (February 2026)
Medical Disclaimer: This content is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult with a qualified healthcare provider before starting any medication. GLP-1 receptor agonists carry a boxed warning regarding thyroid C-cell tumors. Compounded medications are not FDA-approved as finished products. Individual results vary.
• This guide is independently published by WeightLossProviderGuide.com. We are an affiliate site — not a medical provider, insurer, or pharmacy. Some links are affiliate links and we may earn a commission at no cost to you. This never influences our rankings or recommendations. See our full advertising disclosure and how we rank providers.