Disclosure: Some links on this site are affiliate links. If you purchase through these links, we may earn a commission at no extra cost to you. Thank you for supporting our site.·For informational purposes only—not medical advice.
Best Supplements to Take With GLP-1 Medications: What Actually Helps, What to Skip, and When to Get Labs Instead
Bottom line: The best supplements for GLP-1 users are the ones that solve real gaps caused by eating less and managing side effects — not trendy “GLP-1 boosters” or megadose vitamin stacks. For most people on Ozempic, Wegovy, Mounjaro, or Zepbound, protein comes first. A solid multivitamin helps if your food variety has dropped. Fiber and hydration matter when constipation shows up. And targeted nutrients like vitamin D, B12, magnesium, or iron make sense when your symptoms, diet, or blood work actually point to them.
Not everyone on a GLP-1 needs all of these. And some supplements can make your side effects worse.
This guide is based primarily on FDA prescribing information for Wegovy and Zepbound, NIH Office of Dietary Supplements fact sheets, NIDDK and NCCIH guidance, CDC folic acid recommendations, and peer-reviewed nutrition reviews for GLP-1 users — including a 2025 narrative review on dietary supplementation during GLP-1 therapy published in Current Developments in Nutrition.¹ Every recommendation below includes an evidence confidence rating so you know how strong the science is.
What we found in building this page: most supplement guides either give you a shallow listicle with affiliate links, or a clinical deep-dive that takes 20 minutes to read and still doesn’t tell you what to actually do. We built this to do both — give you the answer fast, then back it up with everything you need to decide with confidence.
We may earn a commission if you use our provider links. This does not influence our recommendations. See our full methodology.

The Short Answer: What Most GLP-1 Users Should Consider
If you take nothing else from this page, here’s where the evidence points:
The Core Stack (Strongest Evidence)
Protein supplement — whey or plant-based — to preserve lean muscle mass. This is priority number one during active weight loss. Current guidance often lands around 0.8–1.6 g/kg/day, or for many adults roughly 80–120 g/day, paired with resistance training.¹ ²
Multivitamin — if your food variety or total intake has clearly dropped. Not a magic pill, but genuine insurance against the micronutrient gaps that come from eating significantly fewer calories.³
Fiber supplement — psyllium husk, 5–10 g/day, ramped up gradually — if constipation has shown up. The NIDDK recommends 22–34 g of fiber daily for adults.&sup4;
Vitamin D — worth discussing with your doctor or testing when risk factors are present (obesity, limited sun exposure, restricted diet).&sup5;
Electrolytes and hydration — especially if you’re experiencing nausea, vomiting, or diarrhea. Dehydration is more common than most people realize on GLP-1s.
Sometimes Helpful, Not Always Necessary
- • Omega-3 / fish oil — if you eat little fish&sup6;
- • Magnesium — if constipation or cramps are an issue&sup7;
- • Collagen peptides — a well-tolerated protein add-on when nausea makes shakes hard
- • Probiotics — for persistent GI symptoms
- • B12 — especially if you’re also on metformin&sup8;
- • Iron — only if labs confirm you’re low
What to Skip
Berberine, herbal blood-sugar-lowering supplements, garcinia cambogia, and any “natural GLP-1 booster” or OTC diet pill. These can create unpredictable blood sugar effects or worsen the GI side effects you’re already managing. The NCCIH states that most supplements marketed for weight loss have not been proven safe or effective.&sup9;
The bottom line: Start with the smallest stack that solves your biggest problem. Protein is usually where that starts. Then add based on symptoms, not marketing.
GLP-1 Supplement Comparison Table
The at-a-glance reference we wish existed when we started building this page. Bookmark it.
| Supplement | Why It Matters on GLP-1 | Best For | Not Ideal For | Evidence | When to Take |
|---|---|---|---|---|---|
| Protein (whey) | Preserves lean muscle during weight loss; high bioavailability | Most GLP-1 users with reduced appetite | Dairy-sensitive; severe nausea days | ⬤⬤⬤ | With meals or post-workout |
| Protein (plant) | Muscle preservation; gentler on sensitive stomachs | Dairy-free; GI-sensitive users | Those needing maximum leucine per serving | ⬤⬤⬤ | With meals or post-workout |
| Collagen peptides | Highly digestible protein add-on; supports skin, hair, joints | Nausea days; women wanting hair/skin support | Not a complete protein — add-on only | ⬤⬤○ | Mix into any beverage, any time |
| Multivitamin | Covers baseline micronutrient gaps from reduced intake | Low food variety; women of reproductive age | People with diverse, adequate diets | ⬤⬤⬤ | Morning with food containing fat |
| Fiber (psyllium) | Relieves constipation; feeds beneficial gut bacteria | Constipated users; low-fiber diets | Active diarrhea; without adequate water | ⬤⬤⬤ | Evening with full glass of water |
| Vitamin D | Supports bone health, immune function, mood | Those with confirmed low levels or risk factors | Without testing (dose should be individualized) | ⬤⬤⬤ | Morning with food containing fat |
| Vitamin B12 | Energy, nerve function, DNA synthesis | Metformin users; vegans; fatigue | Those with confirmed normal levels | ⬤⬤○ | Morning, with or without food |
| Magnesium (glycinate) | Muscle relaxation, sleep, 300+ enzyme reactions | Cramps, poor sleep, general depletion | Kidney issues; active diarrhea | ⬤⬤○ | Evening (promotes relaxation) |
| Magnesium (citrate) | Same as above + mild laxative effect | Constipation-focused use | Diarrhea-prone users | ⬤⬤○ | Evening |
| Omega-3 / Fish oil | Heart health, inflammation, hormone balance | Low fish intake; women’s reproductive health | Fish allergy; blood thinner users (ask doc) | ⬤⬤○ | With a meal containing fat |
| Iron | Oxygen transport; prevents anemia | Menstruating women; confirmed low ferritin | Men; those with normal levels (test first!) | ⬤⬤○ | Afternoon with vitamin C; away from calcium |
| Electrolytes | Prevents dehydration from GI side effects | Nausea/vomiting; heavy exercise; hot climate | As a substitute for adequate water intake | ⬤⬤○ | Throughout the day |
| Probiotics | May ease GI side effects; supports gut microbiome | Persistent bloating, diarrhea, or constipation | As a cure-all (set realistic expectations) | ⬤○○ | Follow label instructions |
| Creatine monohydrate | Supports muscle mass and exercise performance | Active exercisers doing resistance training | Those not exercising (works best with training) | ⬤⬤○ | Any time of day, 3–5 g |
| Ginger | Reduces nausea | Injection day; dose escalation periods | Long-term daily use without need | ⬤⬤○ | Before meals on nausea days |
How to read this table: Evidence strength reflects the underlying research for that use case and broader nutrition/weight-loss literature. Important context: most supplements do not yet have direct GLP-1-specific trial data.¹ ⬤⬤⬤ Strong = supported by RCTs, meta-analyses, or expert-consensus guidelines. ⬤⬤○ Moderate = observational studies, expert consensus, or strong mechanistic evidence. ⬤○○ Emerging = preliminary evidence or logical plausibility but limited direct research.
Do You Actually Need Supplements on a GLP-1?
Honestly? Not automatically. And we say that as a site that recommends supplements.
The real issue for most GLP-1 users isn’t that the medication is “stripping nutrients from your body.” It’s simpler than that: you’re eating a lot less food, and less food means fewer nutrients. Clinical studies show people on GLP-1 medications naturally eat significantly fewer calories.¹&sup0; When your appetite drops that much, hitting your targets for protein, fiber, vitamins, and minerals through food alone gets genuinely difficult.
GI side effects compound the problem. Nausea can make healthy cooking feel impossible. Constipation changes what you’re willing to eat. Vomiting and diarrhea can deplete electrolytes. And food monotony — eating the same few “safe” foods that don’t trigger symptoms — can narrow your nutrient profile even further.
Important Distinction
GLP-1 medications are not the same as bariatric surgery. Some pages confuse the two and imply broad malabsorption, which overstates what the current evidence shows. GLP-1s primarily reduce intake and slow gastric emptying. The biggest driver of deficiency risk is simply eating less.¹¹ That means food-first is still the best strategy. Supplements are backup, not the foundation.
Quick Self-Check: Where Do You Fall?
You’re probably fine with food-first if you’re eating 3+ varied meals daily, hitting protein goals, no significant GI issues, and lab work looks normal.
Foundational support probably makes sense if your appetite is way down, you’re eating fewer than 3 meals most days, food variety has dropped, or you’ve lost significant weight.
Talk to your doctor and get labs if you’re exhausted, losing hair, experiencing numbness or tingling, can’t keep food down, have lost a large amount of weight quickly, or are on metformin alongside your GLP-1.
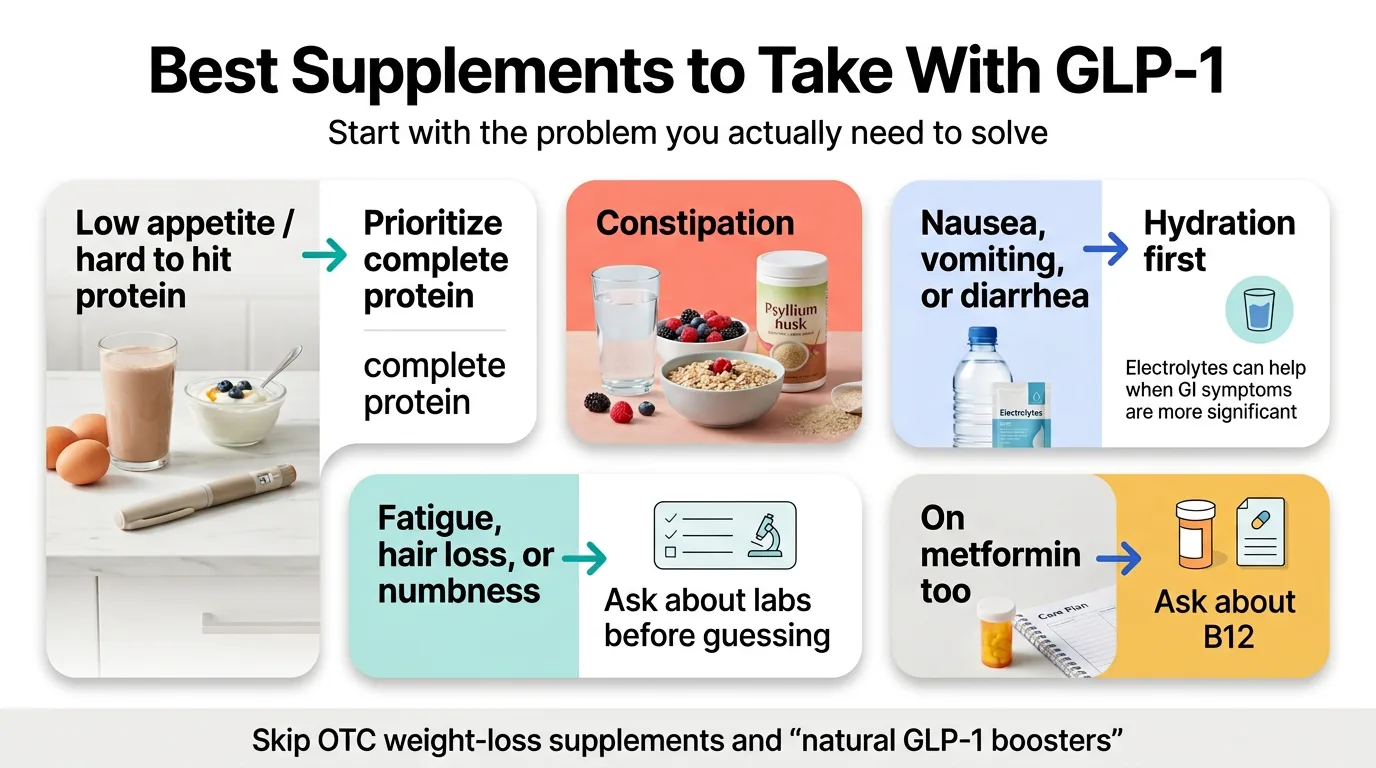
Find Your Situation: If You’re X, Start With Y
Your needs depend on what you’re actually experiencing — not a generic recommendation list.
If you can’t hit protein goals → start with protein. This is the most common gap and the most consequential one. Protein preserves the lean muscle mass that GLP-1-related weight loss tends to strip away.²
If you’re constipated → start with fiber + water. Not random pills. Fiber plus adequate hydration is the evidence-based first move. Magnesium citrate can help too, but fiber is the foundation.&sup4;
If you’re nauseated → focus on hydration and tolerance first. On high-nausea days, your priority is keeping fluids down and getting basic nutrition in. Ginger supplements can help. Simplify your supplement routine to just the essentials.
If you’re losing hair or feel wiped out → think labs, not bottles. Iron, ferritin, vitamin D, B12, zinc, and thyroid function can all be tested with simple blood work. Supplement after you know what’s low.
If you’re on GLP-1 + metformin → B12 deserves extra attention. The NIH Office of Dietary Supplements notes that metformin can reduce B12 absorption and significantly lower serum B12 concentrations.&sup8;
If you’re on tirzepatide and oral birth control → read the women’s health section. Tirzepatide may reduce the efficacy of oral hormonal contraceptives after initiation and dose escalation.¹²
If you’re on a budget → prioritize these three: Multivitamin + protein + vitamin D (if your doctor confirms you need it). These three cover the most ground for the lowest cost.
Protein on GLP-1: The Supplement Most People Need First
We’re putting this section first because, frankly, it’s the most important. If you only address one nutritional gap during GLP-1 treatment, make it protein.

Why Protein Matters More on GLP-1
When you lose weight — whether through GLP-1s, bariatric surgery, or calorie restriction — your body doesn’t only burn fat. It also breaks down muscle. Peer-reviewed nutrition guidance for GLP-1 users is clear: protein intake combined with resistance training is the best evidence-based strategy for preserving lean body mass during GLP-1 therapy.¹ ²
Muscle isn’t just about looking toned. It’s your metabolic engine. It keeps your bones strong. It keeps you functional as you age. Losing too much of it during weight loss is one of the biggest long-term risks of rapid weight reduction.
How Much Protein Do You Actually Need?
The standard RDA for the general population is 0.8 g per kg of body weight daily. During active weight loss on GLP-1 therapy, higher protein is commonly advised. Current guidance often lands around 0.8–1.6 g/kg/day, or for many adults roughly 80–120 g/day, paired with resistance training.¹ ²
| Your Weight | Moderate Target (1.0 g/kg) | Higher Target (1.4 g/kg) |
|---|---|---|
| 150 lbs (68 kg) | 68 g/day | 95 g/day |
| 180 lbs (82 kg) | 82 g/day | 115 g/day |
| 200 lbs (91 kg) | 91 g/day | 127 g/day |
| 220 lbs (100 kg) | 100 g/day | 140 g/day |
When your appetite is suppressed and you’re eating two small meals a day, hitting 100+ grams of protein through food alone is genuinely hard for many people. That’s where supplementation makes a real difference.
Whey vs. Plant-Based vs. Collagen
Whey protein has the best bioavailability and the highest leucine content (the amino acid that triggers muscle protein synthesis). If you tolerate dairy well, it’s the gold standard for muscle preservation. Look for products that are third-party tested and deliver 20–30 g protein per serving.
Plant-based protein (pea protein, rice protein blends) is a solid choice for dairy-free users or those with sensitive stomachs. You may need slightly more per serving (around 30 g) to match whey’s muscle-building effect, but modern blends have closed the gap significantly.
Collagen peptides are a useful add-on but should not be your primary protein source. Collagen is not a complete protein. Its real advantage for GLP-1 users: it’s almost universally well-tolerated, tasteless, dissolves into any hot or cold beverage, and provides 10–15 g per serving without the GI distress that shakes can cause on nausea days.
Common Protein Mistakes on GLP-1
- Waiting until dinner. If you eat most of your protein in one meal, your body can’t use it all efficiently. Spread it across the day — 20–30 g per meal or snack.
- Relying on “healthy” but protein-light meals. A salad with grilled chicken sounds good, but if the chicken portion is small because your appetite is low, you might be getting 15 g when you need 30.
- Thinking protein powder = bodybuilder territory. It’s not. It’s a practical tool for anyone who can’t eat enough. Period.
Multivitamins on GLP-1: When They Help and When They Don’t
A multivitamin is not magic, and it’s not necessary for everyone. But when you’re consistently eating less food with less variety, it serves as genuine insurance against the micronutrient gaps you can’t see or feel yet.
Who Benefits Most
- People whose total calorie intake has dropped significantly
- Anyone eating a narrow rotation of “safe” foods due to GI sensitivity
- Women of reproductive age (higher needs for folic acid, iron, B vitamins)
- People experiencing repeated nausea that limits meal quality
- Anyone who wants one product instead of five separate bottles
What to Look For
Choose a basic multivitamin that fits your needs and avoids megadoses. Look for one that includes vitamin D and B12 at reasonable levels. If you’re a woman who could become pregnant, make sure you’re getting 400 mcg of folic acid daily — this is the CDC recommendation and is supported by the U.S. Preventive Services Task Force for preventing neural tube defects.¹³ ¹&sup4;
Avoid megadose formulas that blast 5,000% of daily values. More is not better with vitamins — especially fat-soluble ones (A, D, E, K) that accumulate in your body.
When a Multivitamin Isn’t Enough
If you have symptoms — fatigue, hair loss, numbness, brain fog — a multivitamin alone may not fix the problem. Those symptoms warrant blood work to identify specific deficiencies, which may need higher targeted doses than a multivitamin provides.
Fiber, Hydration, and Electrolytes: The Constipation Section
Constipation is one of the most common GLP-1 side effects, and it’s one of the most fixable.
Why Constipation Happens on GLP-1
GLP-1 medications slow gastric emptying — that’s part of how they work to make you feel full. But that same mechanism slows your entire digestive tract, which can lead to constipation. Combine that with eating less food (and therefore less fiber), and things can slow to a crawl.
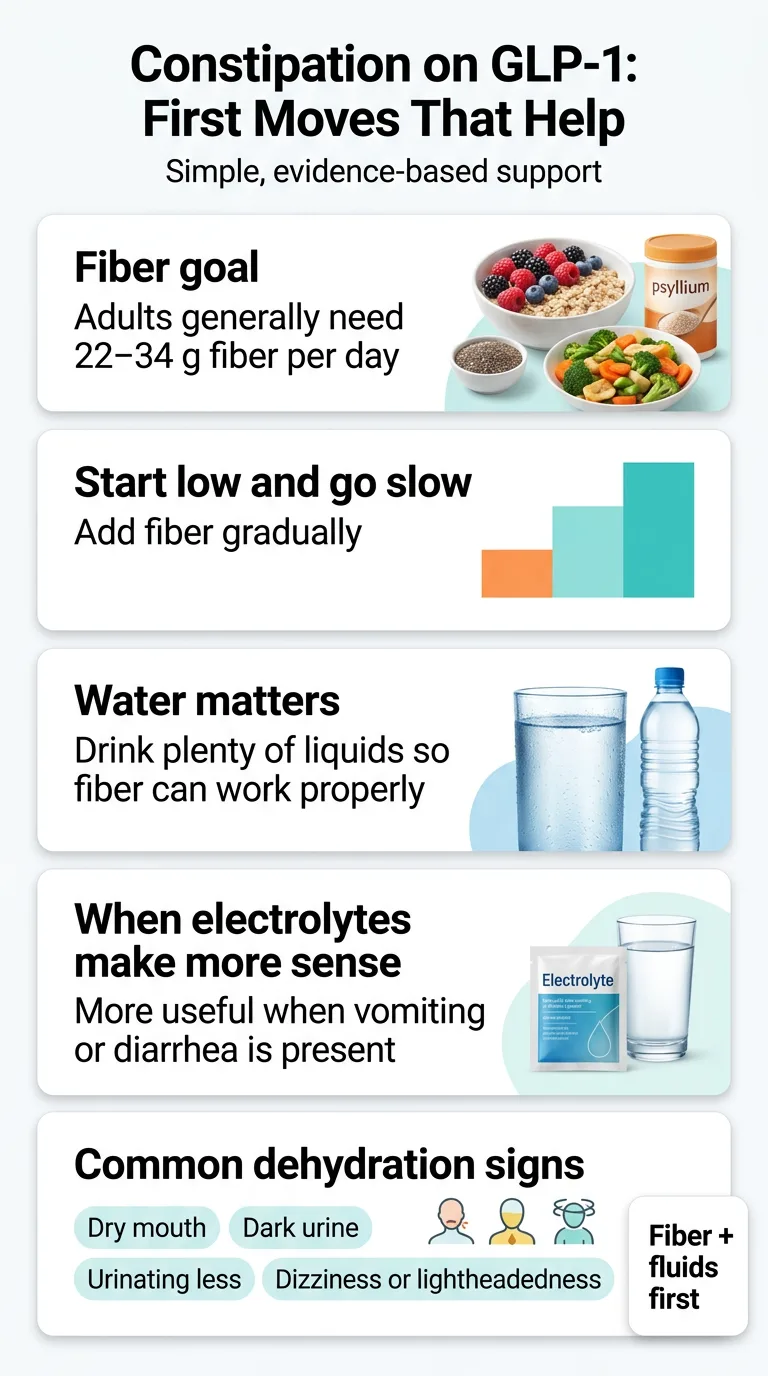
The Fix Is Boring but Effective: Fiber + Water
The NIDDK recommends 22–34 g of fiber daily for adults, added gradually, with plenty of fluids so fiber can work properly.&sup4; Most Americans get far less than that on a good day. On a GLP-1 with suppressed appetite, you might be getting even less.
Psyllium husk is the most-studied fiber supplement and what we recommend starting with. Begin at 5 g/day (one serving), increase gradually over 2–3 weeks to 10–15 g/day, and drink at least a full glass of water with each serving. Important: fiber without adequate water can make constipation worse, not better.
Other options: partially hydrolyzed guar gum (PHGG) for less bloating, and inulin for prebiotic benefits. Avoid the temptation to jump to laxatives before giving fiber and hydration a real try.
How Much Water Do You Actually Need?
A good baseline for most GLP-1 users: aim for 80–100 ounces of fluid daily. That sounds like a lot, but GLP-1 medications can suppress thirst signals along with hunger signals. You may not feel thirsty even when you need fluids. The NIDDK lists thirst, dry mouth, low urination frequency, dark urine, and lightheadedness among signs of dehydration.¹&sup5;
When Electrolytes Help
If you’re experiencing nausea, vomiting, or diarrhea — common during dose escalation — you’re not just losing water. You’re losing sodium, potassium, and magnesium. An electrolyte drink or powder can help maintain balance. Plain water is usually enough for mild symptoms. Electrolyte supplementation makes more sense when GI symptoms are moderate to significant.
Magnesium on GLP-1: Useful for Some, Wrong for Others
Magnesium shows up in every GLP-1 supplement list, and for decent reasons — it’s involved in over 300 enzymatic reactions and many adults don’t get enough. But the conversation around magnesium and GLP-1 needs more nuance than it usually gets.
When Magnesium May Make Sense
- Constipation: Magnesium citrate has a mild laxative effect
- Muscle cramps: Common during weight loss and may indicate depletion
- Sleep issues: Magnesium glycinate in particular has calming properties
- General depletion: If your diet is narrow and you’re not getting magnesium-rich foods
When Magnesium Can Backfire
The NIH Office of Dietary Supplements notes that higher-dose magnesium supplements frequently cause diarrhea, nausea, and abdominal cramping.&sup7; If you’re already dealing with GLP-1 GI side effects, adding a poorly chosen magnesium supplement can make things significantly worse.
Avoid magnesium oxide — it’s the cheapest form, poorly absorbed, and more likely to cause GI distress. If your main goal is constipation relief, magnesium citrate is the better choice. For general supplementation and sleep support, magnesium glycinate is well-absorbed and well-tolerated. Dose: 200–400 mg/day.
Don’t self-experiment if you have kidney issues, already have diarrhea, or are experiencing severe GI symptoms. Talk to your doctor.
Omega-3, Collagen, Probiotics, and Greens Powders: Which “Extras” Are Actually Worth It?
This is where we prevent this page from feeling like “buy everything.” These supplements have their place, but they’re situational add-ons, not essentials for everyone.
Omega-3 / Fish Oil
If you eat fatty fish 2–3 times a week, you probably don’t need a supplement. If you don’t — and many GLP-1 users eat less fish simply because they eat less of everything — omega-3 supplementation (1,000–2,000 mg combined EPA/DHA daily) is a reasonable consideration. The NIH Office of Dietary Supplements notes that omega-3 benefits vary by individual and condition.&sup6; For women of reproductive age, omega-3s play a role in hormone balance and reproductive health.
Collagen
Collagen peptides are a useful add-on, not a foundation. They provide supplemental protein (typically 10–15 g per serving) in a form that’s almost universally well-tolerated — no flavor, no GI distress, dissolves into coffee or water. That makes collagen a practical tool on nausea days when a full protein shake feels impossible. Collagen also provides amino acids that support skin elasticity, hair strength, and joint health — all relevant concerns during significant weight loss. Just remember: it’s not a complete protein. Use it alongside whey or plant-based protein, not instead of them.
Probiotics
The research on probiotics for GLP-1 users is still emerging. Some evidence suggests they may help with bloating, diarrhea, and constipation. Multi-strain formulas with Lactobacillus and Bifidobacterium are the most studied. Approach probiotics as symptom-based support, not a universal recommendation.
Greens Powders
A greens powder is convenience, not a replacement for actual vegetables. If it helps you get more micronutrients on low-appetite days, fine. But don’t confuse it with real produce, and definitely don’t choose a greens powder instead of protein.
Supplements to Avoid on GLP-1 Medications
This section exists because honesty builds trust, and because getting this wrong can genuinely hurt you. Not everything marketed to GLP-1 users is safe to combine with these medications.

“Natural GLP-1 Boosters” and OTC Weight-Loss Supplements
If you’re already on a prescription GLP-1 medication, you do not need — and should not add — a “natural GLP-1 booster” or OTC weight-loss supplement. The NIH’s NCCIH states that most supplements marketed for weight loss have not been proven safe or effective.&sup9; The FDA has also issued specific warnings about illegally marketed, unapproved GLP-1-style products sold online.¹&sup6;
Avoid Stacking Blood-Sugar-Lowering Supplements
This is the most important safety point in this section. Supplements like berberine, chromium, garcinia cambogia, and herbal blood-sugar reducers (bitter melon, gymnema sylvestre, fenugreek, banaba) all have glucose-lowering properties. When combined with a GLP-1 medication that already affects blood sugar regulation, stacking these on top can create unpredictable glucose effects — particularly in people also using other diabetes medications. Don’t use these without your clinician’s explicit approval.&sup9;
High-Dose Vitamin C (>1,000 mg) and Zinc
Both can cause nausea and diarrhea independently. When you’re already managing GLP-1 GI side effects, mega-dose immune formulas containing these can make things miserable. Standard multivitamin doses are fine — it’s the high-dose supplements that are the problem.
OTC Diet Pills and Fat Burners
The safety of combining GLP-1 medications with OTC weight-loss products — including supplements containing stimulants, high-dose caffeine, or unregulated ingredients — is not established.&sup9;
The principle here is simple: Your GLP-1 medication is your weight-loss tool. You don’t need to stack more weight-loss products on top of it. Focus supplements on protecting your health during weight loss — nutrition gaps, muscle preservation, side-effect management — not on trying to accelerate fat loss.
Hair Loss, Fatigue, and Muscle Loss: Symptoms That Need More Than a Bottle
These three symptoms drive more GLP-1 supplement searches than almost anything else. And in all three cases, the instinct to “just buy something” is usually the wrong first move.
Hair Loss on GLP-1
Hair shedding can occur during GLP-1 treatment and appears to be associated at least in part with weight reduction. The Zepbound prescribing information specifically notes that hair-loss adverse reactions were associated with weight reduction.¹² This type of shedding — called telogen effluvium — is the same kind that can happen after surgery, childbirth, or severe illness.
Before You Buy a Hair Supplement, Ask Your Doctor to Check:
- ☐ Ferritin (not just hemoglobin — low ferritin is associated with hair thinning even before you’re technically anemic)
- ☐ Zinc
- ☐ Vitamin D
- ☐ Vitamin B12
- ☐ Thyroid panel (TSH, free T3, free T4)
What else supports hair during GLP-1 weight loss: Protein (hair is made of keratin, which requires amino acids), collagen peptides (provides amino acids for keratin synthesis), and biotin (may help, but the FDA warns biotin can interfere with certain laboratory tests¹&sup7; — tell your clinician if you take it before any blood work).
Timeline: Hair shedding during GLP-1 treatment can feel alarming, but for most people it’s temporary. Regrowth typically begins once weight stabilizes.
Fatigue on GLP-1
Persistent tiredness has multiple possible causes during GLP-1 treatment: eating too few calories, dehydration, low B12, low iron, low vitamin D, poor sleep quality, or simply your body adjusting to the medication. A multivitamin and adequate hydration help with the general causes. Targeted supplementation (B12, iron, vitamin D) helps when labs point to specific deficiencies. If fatigue is severe or worsening, that’s a “get labs” situation, not a “buy more supplements” situation.
Muscle Loss on GLP-1
This one has a clear, evidence-backed answer: protein + resistance training. There is no “muscle vitamin” that replaces this combination. Creatine monohydrate (3–5 g/day) has strong general evidence for supporting muscle mass and exercise performance, though it hasn’t been studied specifically in GLP-1 clinical trials.¹ It works alongside training, not instead of it. If you’re not doing any resistance training while on a GLP-1, that’s the single highest-leverage change you can make — higher impact than any supplement.
GLP-1 and Women’s Reproductive Health
This section addresses a gap that almost no other GLP-1 supplement guide covers. The use of GLP-1 medications among young women has increased significantly in recent years. Many are of reproductive age, and the intersection of GLP-1 use and reproductive nutrition is poorly understood by the general public.
Here’s the paradox: GLP-1 medications may actually improve some fertility markers — particularly for women with PCOS. But the dietary changes that accompany GLP-1 use can simultaneously deplete the nutrients reproductive health depends on: folic acid, iron, omega-3 fatty acids, vitamin D, choline, and B12.
Critical Pregnancy Safety Information
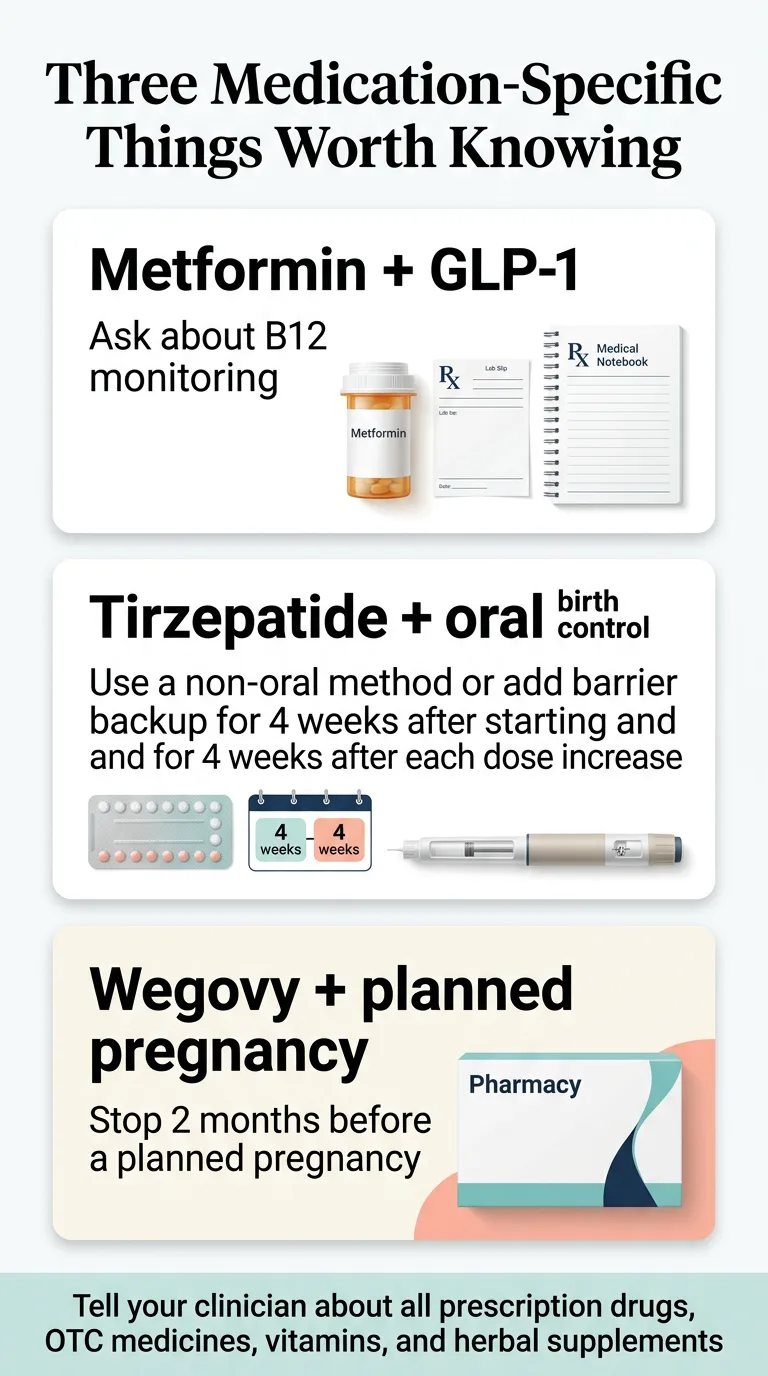
- Semaglutide (Wegovy/Ozempic): Discontinue at least 2 months before a planned pregnancy because of the long half-life. When pregnancy is recognized, discontinue Wegovy.¹&sup8;
- Tirzepatide (Zepbound/Mounjaro): Discontinue when pregnancy is recognized. May cause fetal harm based on animal studies.¹²
- Tirzepatide and oral birth control: May reduce efficacy of oral hormonal contraceptives for 4 weeks after starting and 4 weeks after each dose increase. Backup or non-oral contraception is advised.¹²
Key Nutrients for Reproductive Health During GLP-1 Use
Folic acid (400 mcg daily): The CDC and USPSTF recommend this for all people who could become pregnant.¹³ ¹&sup4; Folic acid is the only form of folate proven to help prevent neural tube defects.
Iron: Menstruation + reduced food intake = elevated risk. Get your ferritin tested. Supplement only if needed.
Omega-3 (EPA/DHA): Supports hormone balance. May be harder to get enough of when dietary fat intake drops.
Vitamin D: Low levels are common among people with overweight or obesity. Worth testing and supplementing if low.
Choline: Often missing from standard multivitamins. Important for reproductive and fetal health. Look for it specifically on the label.
For Women Who Want a Simplified, Reproductive-Health-Focused Routine
FullWell’s Women’s Nutritional Support for GLP-1 Users combines a women’s multivitamin (with folic acid, choline, and 23+ nutrients), balanced omegas, and collagen peptides in one bundle. Formulated by a registered dietitian with 20 years of clinical fertility nutrition experience. The manufacturer states every lot undergoes independent third-party testing.
Best for: Women on GLP-1 whose intake variety is down and who want a simplified routine with reproductive health coverage.
Not best for: Men, people who prefer food-first plus separate protein, people on a tight budget, or anyone who doesn’t need a women-focused formula.
See the FullWell GLP-1 Women’s Support BundleDoes It Change for Ozempic vs. Wegovy vs. Mounjaro vs. Zepbound?
Short answer: the core supplement logic is mostly the same across all GLP-1 and GLP-1/GIP medications. They all reduce appetite, slow gastric emptying, and create similar nutritional challenges. But there are two medication-specific considerations worth knowing:
Delayed Gastric Emptying and Oral Medications
All GLP-1 medications slow stomach emptying, which can theoretically affect how quickly oral medications and supplements are absorbed. The Wegovy prescribing information specifically states that this delay may affect oral-medication absorption and advises patients to tell their clinician about all prescription drugs, OTC medications, vitamins, and herbal supplements.¹&sup8; In practical terms: this is usually not a major issue for standard supplements, but it’s worth mentioning to your pharmacist or doctor — especially if you’re on time-sensitive oral medications.
Tirzepatide and Oral Contraceptives
Tirzepatide (the active ingredient in Mounjaro and Zepbound) may reduce the efficacy of oral hormonal contraceptives during initiation and dose escalation. The FDA-approved prescribing information recommends backup or non-oral contraception for 4 weeks after starting tirzepatide or after each dose increase.¹² If you’re on tirzepatide and relying on the pill for birth control, this is a conversation to have with your prescriber now.
What About GLP-1 Plus Metformin?
Many people with Type 2 diabetes are prescribed a GLP-1 medication alongside metformin. This combination deserves its own mention because of one specific nutrient interaction: the NIH’s Office of Dietary Supplements notes that metformin can reduce vitamin B12 absorption and significantly lower serum B12 concentrations.&sup8; Long-term use increases the risk.
When you combine metformin’s effect on B12 with the reduced food intake from a GLP-1, the risk of B12 deficiency goes up.
Symptoms That Should Push You Toward Testing
- Persistent fatigue that doesn’t improve with sleep
- Numbness or tingling in hands or feet
- Brain fog or difficulty concentrating
- Mood changes
- Balance problems
If you’re on both metformin and a GLP-1, ask your doctor to check B12 levels. If B12 supplementation is needed, common forms include cyanocobalamin and methylcobalamin — your provider can help you choose.&sup8;
When to Ask Your Doctor for Labs Instead of Guessing
We’ve said it throughout this guide, but it deserves its own section: sometimes the right move is not another supplement — it’s a blood test.
Signs That Justify Testing
- Persistent fatigue not explained by poor sleep
- Hair thinning or increased shedding
- Numbness, tingling, or pins-and-needles sensations
- Eating very few calories or limited food variety for weeks
- Repeated vomiting or diarrhea
- Rapid or significant weight loss
- Taking metformin alongside your GLP-1
- Any symptom that’s new, worsening, or doesn’t make sense
The Blood Test Checklist for GLP-1 Users
Print this list and bring it to your next appointment:
- ☐ Complete Blood Count (CBC) — screens for anemia and general health
- ☐ Comprehensive Metabolic Panel (CMP) — electrolytes, kidney function, glucose
- ☐ Vitamin D, 25-hydroxy — a common deficiency, especially with obesity&sup5;
- ☐ Vitamin B12 — especially if on metformin or experiencing fatigue&sup8;
- ☐ Iron panel (ferritin + serum iron + TIBC) — ferritin alone isn’t the full picture
- ☐ Thyroid panel (TSH, free T3, free T4) — if fatigue or hair loss
- ☐ Zinc — if hair loss or immune concerns
- ☐ HbA1c — if diabetic or pre-diabetic
When to test: Monitoring should be individualized based on your symptoms, intake, medication combinations, and your clinician’s judgment. Bring this checklist and discuss what makes sense for your situation.
Red Flags: When Supplements Are Not Enough
Supplements support your health during GLP-1 treatment. They don’t replace medical care. Contact your healthcare provider or seek care if:
- You cannot keep fluids down for more than 24 hours
- You have signs of significant dehydration (dark urine, dizziness, rapid heartbeat, confusion)¹&sup5;
- You experience severe or worsening abdominal pain
- Vomiting is frequent, persistent, or getting worse over time
- You develop new neurological symptoms (numbness, weakness, vision changes)
- Supplements feel like they’re just masking a problem that isn’t improving
Sometimes GI symptoms that don’t improve signal a need to adjust your GLP-1 dose or medication, not to add another pill. Your prescriber needs to know what’s happening.
Your Daily GLP-1 Supplement Routine
We’ve covered a lot. Here’s how to put it into practice with a simple, actionable daily schedule.
The Minimalist Routine (For Most People)
Morning, With Breakfast
- • Multivitamin (take with food containing some fat)
- • Vitamin D (if prescribed — with food containing fat)
- • Omega-3 / fish oil (with food)
Mid-Morning or Around Exercise
- • Protein shake — whey or plant-based (20–30 g)
- • Creatine (3–5 g, if doing resistance training — can mix into your shake)
- • Optional: collagen peptides stirred into coffee or water for extra protein
Afternoon, With Lunch
- • Second protein serving if needed to hit daily goals
- • Iron (if prescribed — take with vitamin C source, keep 2+ hours from calcium)
- • B12 (if taking separately from your multivitamin)
Evening
- • Magnesium glycinate (200–400 mg — promotes sleep)
- • Fiber supplement (with a full glass of water)
Injection Day Adjustment
Many users experience increased nausea on injection day and the 24–48 hours that follow. On those days, simplify:
- Keep: Multivitamin, protein (try collagen in a beverage if shakes are too heavy), electrolytes
- Delay if needed: Omega-3, magnesium, fiber, any supplement that triggers nausea
- Add: Ginger supplement (250 mg before meals) for nausea relief
Budget Routine
If cost is a factor, prioritize: 1. Protein powder, 2. Vitamin D (if your doctor confirms you need it), 3. Generic multivitamin. Add fiber if constipation is present. This covers the highest-impact bases for the lowest cost.
“Lost 16 lbs in 10 weeks — no side effects. Down two sizes. I wish I’d started sooner.”
— Verified MEDVi patient on ConsumerAffairs ★★★★★
Food Still Beats Pills When You Can Eat
Supplements are meant to supplement food, not replace it. When you can tolerate eating, prioritize these:
High-Protein Foods Usually Well-Tolerated on GLP-1
Greek yogurt, eggs, cottage cheese, rotisserie chicken, deli turkey, canned tuna/salmon, tofu, lentil soup, string cheese.
High-Fiber Foods That Tend to Be Gentle
Oatmeal, berries, cooked vegetables (carrots, sweet potatoes, green beans), chia seeds in smoothies, lentils.
Nutrient-Dense Foods Worth Prioritizing
Salmon (protein + omega-3), eggs (protein + choline + B12), leafy greens (folate + magnesium + iron), nuts and seeds (magnesium + zinc + healthy fats), fortified dairy (calcium + vitamin D).
Easy High-Protein Meal Ideas for Reduced-Appetite Days
- Scrambled eggs with cheese (15–20 g protein)
- Greek yogurt with berries and nuts (15–20 g protein)
- Protein shake blended with banana and peanut butter (30–40 g protein)
- Cottage cheese with fruit (20–25 g protein)
- Collagen peptides stirred into morning coffee + a boiled egg (20–25 g protein)
Every bite counts more when you’re eating less. Make your small meals work harder.
Final Takeaway
Most people on GLP-1 medications don’t need a giant supplement stack. They need a few smart choices matched to their actual situation.
Start with protein. It’s the gap that matters most for long-term health, and it’s the hardest to close through food alone when your appetite is suppressed. Add a multivitamin if your eating has narrowed. Add fiber and water if constipation shows up. Get labs if you have symptoms like fatigue, hair loss, or numbness — then supplement what’s actually low. Skip the hype. You don’t need “natural GLP-1 boosters,” megadose vitamins, or weight-loss supplements on top of your medication. Your GLP-1 is doing the weight-loss work. Your supplements should protect your health while it does.
And if something feels off, talk to your doctor. A blood test costs less than a month of random supplements and tells you infinitely more.
Frequently Asked Questions
What are the best supplements to take with GLP-1?
For most people: protein (to preserve muscle), a multivitamin (to cover micronutrient gaps), fiber (if constipated), vitamin D (if testing shows you're low), and electrolytes (if GI side effects are significant). Tailor beyond that based on your specific symptoms and lab results.
What vitamins should I take while on Ozempic?
The most commonly discussed are vitamin D, B12 (especially if also on metformin), and a general multivitamin to cover gaps from reduced food intake. If you're experiencing hair loss, ask your doctor to check iron, zinc, and ferritin as well.
Do I need a multivitamin on GLP-1?
Not universally, but it's a smart safety net if your food variety or total intake has dropped significantly. Choose one that avoids megadoses and includes vitamin D and B12 at reasonable levels.
What supplements should I avoid on GLP-1?
Berberine, chromium, garcinia cambogia, herbal blood-sugar-lowering supplements (bitter melon, gymnema, fenugreek), high-dose vitamin C and zinc supplements, and any OTC weight-loss or "fat burner" product. These can create unpredictable blood sugar effects or worsen GI side effects.
What is the best fiber supplement to take with GLP-1?
Psyllium husk is the most-studied and our first recommendation. Start at 5 g/day, work up gradually, and always take it with a full glass of water.
What is the best magnesium supplement to take with GLP-1?
Magnesium glycinate for general supplementation and sleep support. Magnesium citrate if constipation is your main concern (it has a mild laxative effect). Avoid magnesium oxide — it's poorly absorbed and more likely to cause diarrhea. Dose: 200–400 mg/day.
Can I take collagen while on GLP-1?
Yes. Collagen peptides are well-tolerated, easy to digest, and a practical way to add supplemental protein on days when shakes feel too heavy. They support skin, hair, and joint health during weight loss. Just don't rely on collagen as your primary protein source — it's not a complete protein.
Do I need electrolytes on GLP-1?
If you're experiencing significant nausea, vomiting, or diarrhea — especially during dose escalation — electrolytes can help prevent dehydration and mineral depletion. For mild symptoms, adequate water intake is usually sufficient.
What if I'm on GLP-1 and metformin?
Pay extra attention to vitamin B12. Metformin can reduce B12 absorption, and combined with GLP-1-related reduced food intake, the risk of deficiency increases. Ask your doctor to check B12 levels.
What if I'm on tirzepatide and birth control?
The Zepbound prescribing information notes that tirzepatide may reduce the efficacy of oral hormonal contraceptives after initiation and dose escalation. The FDA recommends backup or non-oral contraception for 4 weeks after starting or increasing the dose. Discuss this with your prescriber.
Are "natural GLP-1 supplements" legit?
Products marketed as "natural GLP-1 boosters" are not replacements for prescription GLP-1 medications. If you're already on a prescription GLP-1, adding supplements that also affect GLP-1 activity creates unpredictable effects and is generally not recommended. The NCCIH says most weight-loss supplements have not been proven safe or effective.
Can supplements replace real food on GLP-1?
No. Supplements fill gaps — they don't replace the full spectrum of nutrients, fiber, and satiety that real food provides. Food-first is always the better approach when you can tolerate eating. Supplements are your backup plan.
When should I ask for labs instead of guessing?
When you have persistent fatigue, hair loss, numbness or tingling, very restricted eating, repeated vomiting or diarrhea, rapid or significant weight loss, or when you're on metformin. See our full blood test checklist in the guide above.
How We Built This Guide
Primary Sources
- FDA prescribing information for Wegovy (semaglutide) and Zepbound (tirzepatide)
- NIH Office of Dietary Supplements fact sheets (B12, Magnesium, Omega-3, Vitamin D)
- NIDDK guidance on constipation, fiber, and hydration
- NCCIH guidance on weight-loss supplements
- CDC folic acid and MTHFR guidance
- U.S. Preventive Services Task Force: folic acid recommendation
- FDA warnings on unapproved GLP-1 products
- FDA safety communication on biotin interference with lab tests
- “Dietary supplement considerations during GLP-1 receptor agonist treatment” (Current Developments in Nutrition, 2025)
- “Bridging the nutrition guidance gap for GLP-1 receptor agonist users” (PMC, 2025)
- “Nutritional Priorities to Support GLP-1 Therapy for Obesity” (PMC, 2025)
Our Evidence Rating System
⬤⬤⬤ Strong: Supported by randomized controlled trials, meta-analyses, or expert-consensus guidelines
⬤⬤○ Moderate: Supported by observational studies, indirect evidence, or strong expert consensus
⬤○○ Emerging: Preliminary evidence or logical plausibility but limited direct research
Important context: the 2025 Current Developments in Nutrition narrative review notes that no clinical trials have directly evaluated most supplements specifically in GLP-1 receptor agonist users.¹ Our ratings reflect the best available evidence, not certainty.
This guide was written by the Weight Loss Provider Guide editorial team. We update it as new research emerges. Some links in this guide are affiliate links. If you purchase through them, we may earn a commission at no extra cost to you. We recommend products based on evidence and genuine value — not commission rates. Most of our recommendations are to general supplement categories, not specific brands.
References
- “Dietary supplement considerations during glucagon-like peptide-1 receptor agonist treatment: A narrative review.” Current Developments in Nutrition, 2025. ScienceDirect
- “Nutritional Priorities to Support GLP-1 Therapy for Obesity.” PMC, 2025. PubMed
- “GLP-1 Supplements to Support Your Weight Loss Journey.” U.S. News & World Report, March 2026. U.S. News
- “Eating, Diet, & Nutrition for Constipation.” NIDDK. NIDDK
- “Vitamin D — Health Professional Fact Sheet.” NIH Office of Dietary Supplements. ODS
- “Omega-3 Fatty Acids — Consumer Fact Sheet.” NIH Office of Dietary Supplements. ODS
- “Magnesium — Health Professional Fact Sheet.” NIH Office of Dietary Supplements. ODS
- “Vitamin B12 — Health Professional Fact Sheet.” NIH Office of Dietary Supplements. ODS
- “Tips: Know the Facts About Supplements Marketed for Weight Loss.” NCCIH. NCCIH
- “Bridging the nutrition guidance gap for GLP-1 receptor agonist users.” PMC, 2025. PMC
- Ibid.
- Zepbound (tirzepatide) Prescribing Information. FDA. FDA
- “MTHFR Gene Variant and Folic Acid Facts.” CDC. CDC
- “Folic Acid Supplementation to Prevent Neural Tube Defects.” USPSTF, 2023. USPSTF
- “Symptoms & Causes of Viral Gastroenteritis.” NIDDK. NIDDK
- “FDA’s Concerns with Unapproved GLP-1 Drugs Used for Weight Loss.” FDA. FDA
- “Biotin Interference with Troponin Lab Tests.” FDA. FDA
- Wegovy (semaglutide) Prescribing Information. FDA. FDA
Medical Disclaimer
This guide is for educational purposes only and does not constitute medical advice. Always consult your healthcare provider before starting any supplement, especially if you are pregnant, nursing, or taking other medications. Individual needs vary — what works for one person may not be appropriate for another.
Affiliate Disclosure
Some links in this article are affiliate links. If you purchase through them, we may receive a commission at no additional cost to you. Our recommendations are based on evidence, not commissions.
Related Guides
Last Updated: March 2026 | Evidence last reviewed against published studies through early 2026