Disclosure: Some links on this site are affiliate links. If you purchase through these links, we may earn a commission at no extra cost to you. Thank you for supporting our site.·For informational purposes only—not medical advice.
GLP-1 Plateau: Why Your GLP-1 Isn't Working Anymore (and What to Do Next)
By the WPG Research Team | Last verified: February 2026 | Sources: STEP & SURMOUNT clinical trials, FDA prescribing information, Endocrine Society guidelines — see full source list below
Your GLP-1 plateau is not a failure. It's a predictable biological event that happens to the majority of people on semaglutide, tirzepatide, and every other GLP-1 medication on the market — and it has specific, fixable causes.
Here's the bottom line: if you were losing weight and it stopped, the medication almost certainly hasn't “quit working.” Something shifted — your metabolism adapted, your dose needs adjusting, your body composition changed, or one of about a dozen other identifiable factors kicked in. We'll walk you through every one of them.
*For educational purposes only — not medical advice.*
What to do right now:
- Don't panic. Stalls and plateaus are common during GLP-1 weight loss — especially as weight loss naturally slows over time. You're in the majority, not the exception.
- Take our 60-Second Plateau Test (below) to identify your most likely cause and get a matched next step.
- Follow the 7-Step Fix Plan — in order — to restart your progress with the least effort and cost.
- If you're at max dose and still stalled, the single highest-impact move may be switching from semaglutide to tirzepatide (dual GLP-1/GIP mechanism). We'll show you the clinical data and exactly how to evaluate that decision.
One thing we won't do: tell you “it's perfect for everyone” or pretend every plateau has an easy answer. Some don't. But the vast majority are breakable once you identify the right lever to pull — and that's exactly what this guide is built to help you do.
Safety Note
If you're experiencing severe abdominal pain, persistent vomiting, signs of dehydration, or any symptoms that feel like a medical emergency — stop reading and contact your healthcare provider or call 911. Plateaus are frustrating. They're not emergencies. But some symptoms that coincide with stalls are.
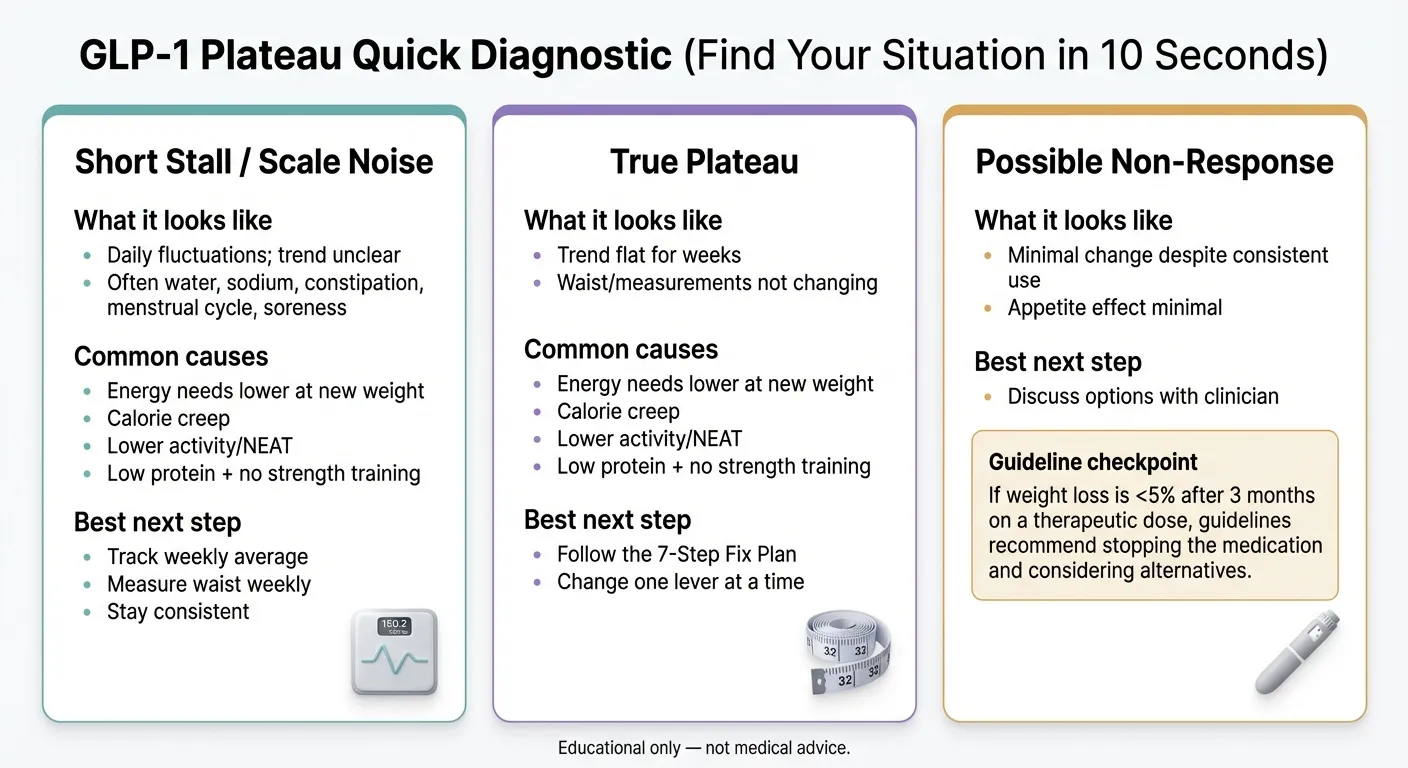
60-Second GLP-1 Plateau Test: Find Your Cause and Next Step
Before you read 8,000 words, answer a few quick questions. We built this diagnostic based on clinical trial patterns, published obesity medicine guidelines, and the most common plateau presentations reported by patients and providers.
This tool is educational and not a medical diagnosis. Use it to prepare for a conversation with your clinician.
*Educational only — not medical advice.*
If your situation doesn't fit neatly into one category — that's common. Most plateaus involve 2–3 overlapping factors. Keep reading. The full guide below covers every cause, every fix, and the decision framework for when it's time to switch medications.
What Exactly Is a GLP-1 Plateau?
A GLP-1 plateau is a sustained period — generally 4 or more consecutive weeks — where your weight does not decrease despite consistent medication use and reasonable adherence to nutrition and activity habits.
That's it. Simple definition. But here's what it is not: it is not proof that the medication stopped working. It is not proof that something is wrong with you. And it is not the end of your weight loss journey.
Plateaus happen across every weight loss intervention ever studied — surgery, medication, dietary approaches, all of them. The body adapts. That's what bodies do. GLP-1 receptor agonists are the most effective weight loss medications in modern medicine, and they still can't override basic metabolic adaptation forever.
The key distinction most articles miss:
Scale noise (1–3 weeks)
Water retention, sodium intake, bowel regularity, hormonal fluctuations. This is not a plateau. This is Tuesday.
True plateau (4+ weeks)
No measurable change in weight and body measurements (waist, hips). This signals something needs to be addressed.
Non-response
Medication never produced meaningful weight loss even after adequate time on a therapeutic dose. The Endocrine Society guidelines use <5% body weight loss after 3 months at therapeutic dose as the threshold to consider a change.
Knowing which category you're in changes everything about what to do next.
How Long Do GLP-1 Plateaus Last?
Most temporary stalls (scale noise) resolve on their own within 1–3 weeks without any changes.
True plateaus — where intervention is needed — vary:
- With the right intervention, most people see renewed weight loss within 2–6 weeks.
- Without intervention, plateaus can become permanent. The body settles at a new equilibrium and stays there.
- The most common window for hitting your first real plateau is between months 3–9 of GLP-1 treatment. Clinical trial data from the STEP trials (semaglutide) and SURMOUNT trials (tirzepatide) both show that weight loss velocity naturally decelerates during this period for the majority of participants.
Here's what most people get wrong about plateau timing: they either react too fast (changing everything after a 10-day stall) or too slow (waiting months hoping it resolves on its own while paying $200+/month for a medication that isn't producing results).
The Sweet Spot
4 weeks of confirmed plateau → take action using the fix plan below → give each intervention 2–4 weeks to show results before escalating to the next step.
The worst thing you can do during a plateau is nothing. The second worst thing is panic and make five changes at once — because then you won't know what worked. The fix plan below is designed to give you the right moves in the right order, so you can isolate the variable that actually matters for your situation.
Why Weight Loss Slows Down on GLP-1s (Even When You Do Everything Right)
Let's kill one myth right now: you probably didn't “do something wrong.”
Your body is a dynamic system. When you lose weight — by any means — your body recalibrates. It's not sabotaging you. It's doing exactly what evolution designed it to do: resist further energy loss when resources appear scarce.
Your metabolism adjusts downward
Every pound you lose reduces your daily calorie burn by roughly 7–10 calories. Lose 30 pounds, and your body now needs 210–300 fewer calories per day than it did before you started. That deficit that was producing steady weight loss? It shrunk — or disappeared entirely.
This is called metabolic adaptation (sometimes “adaptive thermogenesis”), and it's been documented extensively in weight loss research. A key modeling study by Hall (published in Obesity) found that plateaus are a mathematically predictable consequence of energy balance dynamics across all weight loss interventions (Hall KD, Obesity 2018, PMC).
Your appetite recalibrates
GLP-1 medications suppress appetite by slowing gastric emptying and signaling satiety to your brain. But your body pushes back over time. Hunger hormones (ghrelin, in particular) can partially reassert themselves. The appetite suppression you felt in month one is often stronger than what you feel in month six — not because the drug “wore off,” but because your hormonal system is fighting for equilibrium.
Your movement changes (and you don't notice)
This is the sneaky one. As you lose weight, your body unconsciously reduces something called NEAT — non-exercise activity thermogenesis. That's the fidgeting, the standing, the taking-the-stairs, the general restlessness that burns hundreds of calories a day. Research shows NEAT can drop significantly during weight loss without any conscious awareness. You feel like you're doing the same things. You're not — your body is conserving energy behind the scenes.
The math catches up
At a higher weight, there was a gap between what you ate and what you burned. That gap was your weight loss. As your weight dropped, the gap closed. Eventually, intake and expenditure met — and the scale stopped moving.
This isn't failure. It's physics. And it's addressable once you understand which lever to pull.
Body composition compounds the effect
Your body composition is changing the equation too. As you lose weight, you lose both fat and lean muscle mass — unless you're actively working to prevent it with resistance training and adequate protein. Muscle is metabolically “expensive” tissue; it burns more calories at rest than fat does. Lose muscle, and your basal metabolic rate drops even further than the weight loss alone would predict. This creates a compounding plateau effect that gets harder to break the longer it continues unchecked. We'll cover exactly how to address this in the fix plan.
Why Your GLP-1 Feels Like It “Stopped Working”: 12 Causes Ranked
Not all plateaus are created equal. Here are the 12 most common causes, ranked by how frequently they show up and how fixable they are. For each one: what it looks like, how to check, and the fix.
1. You're not at an effective dose yet
What it looks like: You started recently, you're still on a lower titration dose, and weight loss has been slow or minimal.
The check: Look at your prescribed titration schedule. Semaglutide's maintenance dose is 2.4mg (for Wegovy) and tirzepatide goes up to 15mg (Zepbound/Mounjaro). Many people don't reach a therapeutically effective dose for 12–20 weeks.
The fix: Patience — and follow your titration schedule. If your provider is keeping you on a low dose longer than the prescribing information recommends without a clear medical reason, ask about it.
2. Your dose needs adjustment
What it looks like: You were losing weight, you've been on the same dose for a while, and progress has stalled.
The check: Have you been at your current dose for 4+ weeks with no further weight loss? Is there room to increase?
The fix: Contact your prescribing provider. Dose escalation — moving up to the next step per the titration schedule — is the first-line pharmaceutical response to a plateau. Both the Wegovy and Zepbound prescribing information outline specific dose escalation protocols.
3. Calorie creep (the silent plateau killer)
What it looks like: You're “eating the same” — but you're probably not.
The check: Track everything you eat and drink for 7 full days. Pay special attention to liquid calories (coffee drinks, smoothies, alcohol, juice), cooking oils, sauces, and snack portions.
The fix: Most people find 200–400 extra daily calories hiding in places they didn't expect. Once you see them, you can make informed choices.
Practical tip: Focus your audit on the four biggest “stealth calorie” categories: beverages (a large coffee drink can pack 300–500 calories), cooking fats (a heavy pour of olive oil = 300 calories), “healthy” snacks eaten in large quantities (nuts, granola, dried fruit), and condiments/sauces (ranch, mayo, sweetened dressings).
4. Protein is too low
What it looks like: Appetite returns faster than expected between meals. Muscle loss is accelerating. Energy is low.
The check: Track your daily protein intake. Are you consistently hitting 0.7–1 gram per pound of your goal body weight?
The fix: Protein preserves muscle mass (keeps metabolic rate up), has the highest thermic effect of any macronutrient (your body burns more calories digesting it), and is the most satiating macronutrient. Most people on GLP-1s are dramatically under-eating protein. Use our GLP-1 protein calculator to find your target.
5. Constipation and water retention are masking real fat loss
What it looks like: The scale is stuck. You feel bloated. Bowel movements are irregular.
The check: GLP-1 medications slow gastric emptying — that's literally how they work. A common side effect is constipation. If you haven't had a regular bowel movement in several days, the scale is lying to you.
The fix: Increase fiber intake gradually. Prioritize fluids. Magnesium citrate can help. Critically — measure your waist and hips weekly in addition to weighing yourself. If your measurements are still dropping, you're still losing fat even when the scale won't confirm it.
6. Missed or inconsistent doses
What it looks like: You've missed a dose or two, or your injection timing has been inconsistent.
The check: Be honest with yourself. Weekly injections need to be within the same 1–2 day window each week for consistent blood levels.
The fix: Set a recurring alarm. Same day, same time, every week. If you missed a dose, follow the guidance in your prescribing information. Don't double up.
7. You lost muscle mass (body composition shift)
What it looks like: You've lost significant weight but haven't been doing resistance training. You feel weaker.
The check: Body-composition studies show that some of the weight lost on GLP-1 therapies includes lean mass. “Lean mass” is not the same as “muscle” — but the principle holds: losing metabolically active tissue lowers your resting calorie burn (Willoughby et al., PMC 2018).
The fix: Resistance training, 2–3 times per week, with progressive overload. This is the single most important behavioral intervention for GLP-1 users. Pair with adequate protein.
8. Activity and NEAT dropped without you knowing
What it looks like: Your formal exercise is the same, but you're unconsciously moving less throughout the day.
The check: Compare your daily step count and total active minutes from your first month to now. Most people see a meaningful decline.
The fix: Set a daily step target (8,000–10,000). Stand more. Take phone calls while walking. NEAT can account for 200–500 calories per day, and it's the component that drops most silently during weight loss.
9. Sleep debt or chronic stress
What it looks like: Your routine is solid, your nutrition is dialed in, and the scale still won't move — but you're sleeping poorly or under chronic stress.
The check: Are you consistently getting 7–9 hours of quality sleep? Are you in a high-stress period?
The fix: Sleep deprivation elevates ghrelin (hunger hormone), suppresses leptin (satiety hormone), increases cortisol, and promotes abdominal fat retention. These aren't “wellness tips” — they're physiological mechanisms that directly counteract GLP-1 medication effectiveness. Fix sleep first.
10. Other medications working against you
What it looks like: You started or changed another medication around the time the plateau began.
The check: Several common medication classes are associated with weight gain: certain antidepressants (particularly mirtazapine, paroxetine, and some TCAs), beta-blockers, insulin and sulfonylureas, some anticonvulsants, certain antipsychotics, and systemic corticosteroids.
The fix: Do not change any medication without your doctor's guidance. But do bring this up at your next appointment. Ask: “Could any of my current medications be contributing to my weight loss plateau?”
11. An underlying medical condition
What it looks like: The plateau coincides with other symptoms — fatigue, hair thinning, cold intolerance, mood changes, menstrual irregularities.
The check: Significant weight loss can trigger or unmask thyroid dysfunction, worsen PCOS symptoms, or reveal insulin resistance patterns.
The fix: See your physician. Request a comprehensive panel: TSH, Free T4, Free T3, fasting insulin, HbA1c, and basic metabolic panel. If there's an underlying condition, no amount of dose adjustment or dietary changes will fully resolve it.
12. Product quality or legitimacy issues
What it looks like: You've been on the medication for an adequate time at what should be a therapeutic dose, and you've never experienced meaningful appetite suppression or weight loss.
The check: Where did you get your medication? The FDA has issued warnings about counterfeit Ozempic and unapproved GLP-1 products in the U.S. supply chain.
The fix: If you have any doubt about authenticity or quality, switch to a verified provider. A reputable telehealth provider that uses licensed U.S. pharmacies is a straightforward path.
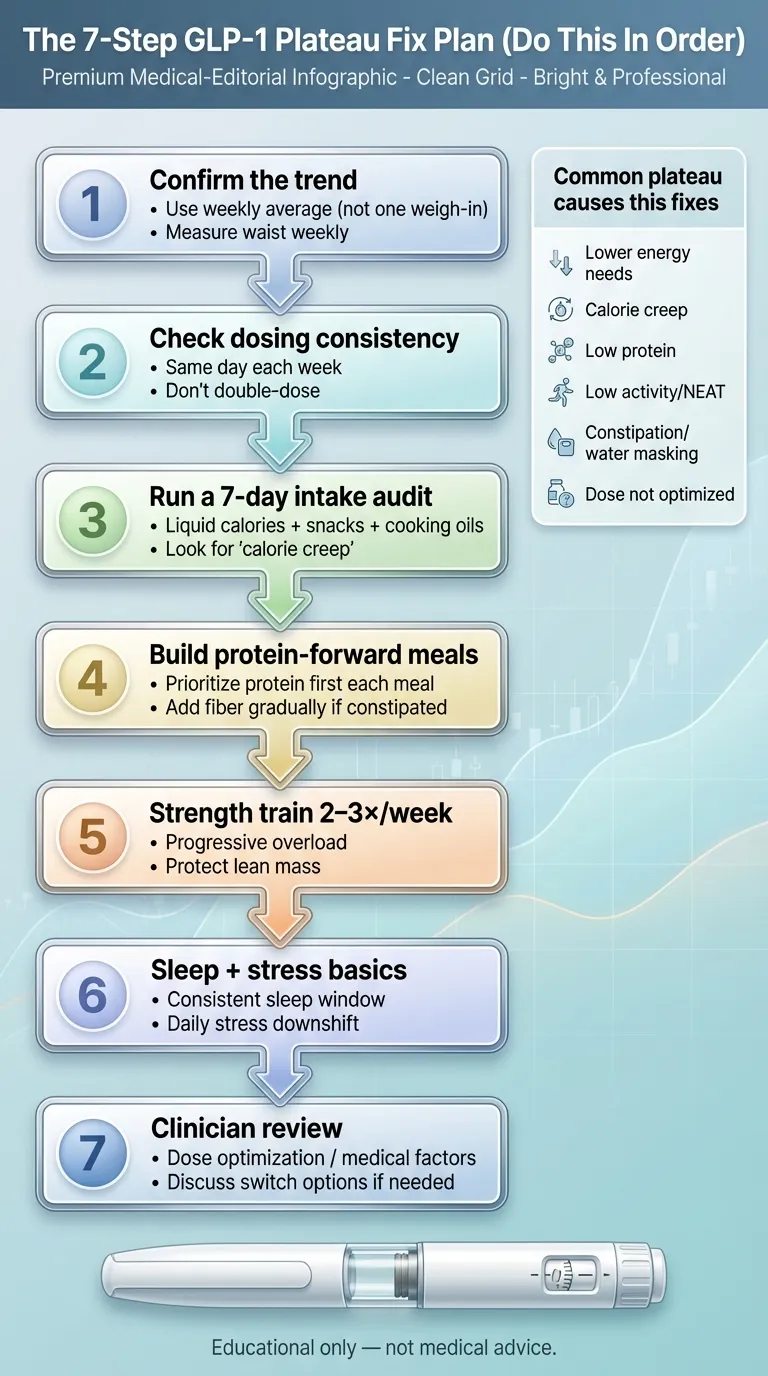
The 7-Step GLP-1 Plateau Fix Plan
Do these in order. Not all at once — in order. Each step either resolves the problem or reveals the next layer.
*Educational only — not medical advice.*
Confirm It's Real (The 4-Week Rule)
Don't react to a bad week. Or even two bad weeks. Weigh yourself at the same time each day (morning, after bathroom, before food). Track the weekly average, not any single day. Measure your waist and hips once a week.
The rule: If your weekly average weight and your body measurements haven't changed in 4 consecutive weeks, it's a real plateau. Before that, it's noise. If you can only do one thing: take waist measurements. The scale lies constantly. The tape measure doesn't.
Audit Your Adherence
Simple question: have you missed any doses in the last 4 weeks? Has your injection timing been consistent? If yes — fix it. Set a phone alarm. Use a medication tracking app. Consistency in dosing directly impacts blood levels, which directly impacts efficacy.
No judgment here. Life gets busy. But inconsistent dosing is the simplest plateau cause to fix and the one people most often overlook.
Run a 7-Day Intake Audit
Not a “diet.” An audit. For 7 days, log everything that goes in your mouth. Use an app like MyFitnessPal, Cronometer, or even a simple notes file. The goal isn't perfection — it's awareness.
You're looking for:
- Liquid calories you forgot about (lattes, smoothies, juice, alcohol, creamer)
- Cooking fats that don't get counted (olive oil is 120 calories per tablespoon)
- Snack portions that grew without you noticing
- Protein total — is it actually at 0.7–1g per pound of goal body weight?
Most people discover a 200–500 calorie discrepancy they didn't know existed. That's often the entire deficit that was driving their weight loss — gone.
Lock In Protein and Fiber Targets
These aren't suggestions. They're the two nutritional levers with the most evidence for GLP-1 users.
Protein Target
0.7–1g per pound of goal body weight, daily. Preserves muscle, highest thermic effect, keeps you fuller longer.
Fiber Target
25–35g per day from whole food sources. Supports gut health, reduces constipation, adds satiety volume.
Add Resistance Training (Non-Negotiable)
Resistance training is the single most important behavioral intervention for someone on GLP-1 medication. GLP-1 users who don't do resistance training lose substantially more lean mass as a proportion of total weight lost.
Simplest possible starting point: Pick 5 compound movements (squat, hinge, push, pull, carry), do 3 sets of 8–12 reps of each, twice per week. When it stops being challenging, add weight or reps. That's it.
This step alone has broken more plateaus than any dose adjustment. Muscle tissue burns roughly 6 calories per pound per day at rest, compared to 2 calories per pound for fat tissue. Build 5 pounds of muscle while losing fat, and you've permanently raised your daily calorie burn.
Address Sleep and Stress
If steps 1–5 are solid and you're still stalled, this is where most people find their answer.
Sleep: Aim for 7–9 hours per night. Sleep deprivation doesn't just make you tired — it actively works against your medication by increasing ghrelin, decreasing leptin, elevating cortisol, and impairing insulin sensitivity. One study found that sleep restriction reduced the proportion of weight lost as fat by 55%.
Stress: Chronic cortisol elevation promotes visceral fat storage and can directly counteract the appetite-suppressing effects of GLP-1 agonists. 10 minutes of daily stress management (deep breathing, walking, meditation) has measurable physiological effects on cortisol.
Medication Strategy Review With Your Provider
If you've worked steps 1–6 honestly for 4–6 weeks and you're still stalled, it's time for a clinical conversation. This is not the first step — it's the seventh — because most plateaus resolve before you get here.
If you're NOT at max dose: Dose escalation is the first pharmaceutical move.
If you ARE at max dose of semaglutide: This is where switching to tirzepatide becomes the conversation. Tirzepatide activates both GLP-1 and GIP receptors. If you've reached the maximum benefit from your current medication after optimizing lifestyle factors, adding an entirely new receptor pathway may restart weight loss.
What to say to your provider (use this script):
“I've been at [dose] for [X weeks] and my weight loss has completely stalled. I've audited my nutrition, I'm hitting [X grams] of protein daily, I'm doing resistance training [X times per week], my sleep is [7+ hours / needs work], and I've tracked my food intake for the past week — it's consistent with what was working before. I'd like to discuss whether a dose adjustment or a switch to tirzepatide is appropriate for my situation.”
Bringing data to your provider transforms the conversation from “I'm frustrated” to “here's the clinical picture — what do you recommend?”
MEDVI
Semaglutide from $179/mo · Tirzepatide available
Should You Switch From Semaglutide to Tirzepatide?
This is the question behind many GLP-1 plateau searches — and the answer depends entirely on your specific situation.
The short version
If you've maxed out your semaglutide dose and completed steps 1–6 above with no results, switching to tirzepatide is often the highest-impact pharmaceutical move available. The reason is mechanistic, not marketing: tirzepatide does something semaglutide doesn't.
The science (in plain English)
Semaglutide (Ozempic, Wegovy) activates one receptor: GLP-1. It slows gastric emptying and signals satiety through a single pathway.
Tirzepatide (Mounjaro, Zepbound) activates two receptors: GLP-1 and GIP (glucose-dependent insulinotropic polypeptide). This dual mechanism affects appetite, fat storage, insulin sensitivity, and energy expenditure through pathways that semaglutide doesn't touch.
Think of it this way: semaglutide pushes one button really well. Tirzepatide pushes that same button and a second one. If your body adapted to the first button, the second one is new territory.
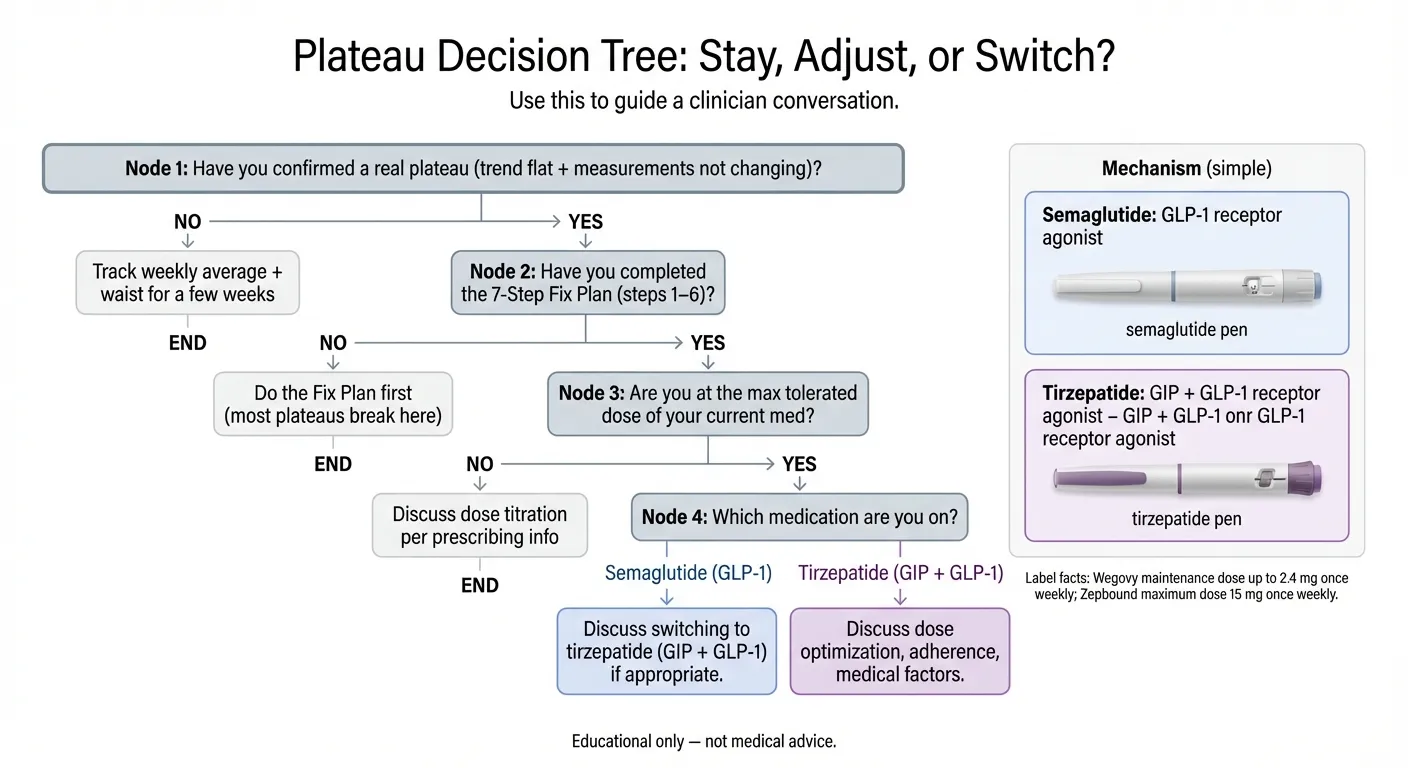
*Use this to guide a clinician conversation. Educational only — not medical advice.*
What the clinical data shows
| Factor | Semaglutide (Wegovy) | Tirzepatide (Zepbound) |
|---|---|---|
| Mechanism | GLP-1 receptor agonist | Dual GLP-1 + GIP receptor agonist |
| Avg. weight reduction (trials) | ~15% (STEP 1, Wilding et al., NEJM 2021) | ~21% (SURMOUNT-1 treatment-regimen estimand, Jastreboff et al., NEJM 2022) |
| Max dose | 2.4 mg/week | 15 mg/week |
| Head-to-head data | SURPASS-2 showed tirzepatide superior at every dose for weight loss in type 2 diabetes patients (Frías et al., NEJM 2021) | |
| Common side effects | Nausea, constipation, diarrhea (dose-dependent) | Similar GI profile; may vary during transition |
| Monthly cost (telehealth) | ~$149–$299/mo | ~$199–$399/mo |
Sources: STEP 1 (NEJM 2021), SURMOUNT-1 treatment-regimen estimand (NEJM 2022), SURPASS-2 (NEJM 2021), FDA prescribing information. Pricing ranges from major telehealth provider websites as of February 2026. Important caveat: STEP and SURMOUNT were separate trials with different patient populations, not a direct head-to-head comparison for weight loss in non-diabetic adults.
Who switching helps most
- People at maximum semaglutide dose (2.4mg Wegovy or equivalent) who have stalled for 6+ weeks after optimizing lifestyle factors
- People who experienced strong initial appetite suppression on semaglutide that has meaningfully diminished
- People whose providers have confirmed no underlying medical cause for the plateau
Who should NOT switch lightly
- People who haven't completed steps 1–6 of the fix plan
- People whose plateau is caused by caloric drift, insufficient protein, lack of resistance training, or sleep/stress issues
- People with a medical condition driving the plateau (thyroid, PCOS, medication interactions) — treat the root cause first
- People still in the titration phase who haven't reached a therapeutic dose
What the switch actually involves
- Your provider evaluates your plateau and confirms a medication change is appropriate
- You transition to tirzepatide starting at a lower dose and titrate up (you don't jump straight to max)
- The transition is generally smooth, though you may experience a brief return of early side effects (nausea, etc.) as your body adjusts
- Most telehealth providers can manage this transition within your existing subscription
If your current provider doesn't offer tirzepatide, can't facilitate the switch, or hasn't been responsive to your plateau concerns, it may be worth looking at providers who specialize in this specific situation. MEDVI, for example, offers both semaglutide and tirzepatide with included clinical consultations, which means the switch can be managed within one provider relationship.
When to Switch Providers (Not Just Medications)
Sometimes the medication isn't the problem. The provider is. Red flags that your current GLP-1 provider isn't serving you:
- “Just be patient” is their only response to your plateau, with no clinical reasoning or plan
- They can't prescribe what you need. If tirzepatide is appropriate and your provider doesn't offer it, that's a meaningful limitation.
- No follow-up care. If you get a prescription and then hear nothing unless you initiate, you're using a refill service, not a clinical provider.
- No guidance beyond the medication. If they've never discussed protein intake, resistance training, or lifestyle optimization, you're getting half a treatment plan.
- They won't discuss switching when the clinical situation warrants it
| Feature | Refill-Only Services | Clinical-Support Providers |
|---|---|---|
| Medication access | Usually one option | Multiple medications (semaglutide + tirzepatide) |
| Provider check-ins | Minimal or none | Regular consultations included |
| Plateau support | “Wait and see” | Active management with dose/switch guidance |
| Nutrition guidance | None | Included or recommended |
| Cost range | $99–$199/mo | $179–$399/mo |
MEDVI falls into the clinical-support category — their program includes provider consultations, access to both semaglutide and tirzepatide, and the ability to manage medication transitions without starting a new patient intake elsewhere. Read our full MEDVI tirzepatide review for more details.
One real downside worth mentioning: Some users on review sites have reported that billing and cancellation communication wasn't as smooth as they expected. Our recommendation: if you sign up for any telehealth GLP-1 provider, set a calendar reminder before your renewal date and review the cancellation policy upfront. That said, the clinical quality of care — the part that actually matters for your plateau — is where MEDVI consistently earns strong reviews.
“The financial communication has been clear and honest…” — MEDVI review, Trustpilot
“To me this is a very excellent, responsible company!” — MEDVI review, ConsumerAffairs
We earn a commission if you sign up through our links, at no extra cost to you. This doesn't influence our evaluations — we recommend services based on their clinical value for the specific situations described in this guide. Full affiliate disclosure
MEDVI
Both semaglutide & tirzepatide · Provider consultations included
Safety & FDA Warnings: When a Plateau Is NOT the Problem
Most GLP-1 plateaus are frustrating but not dangerous. However, some symptoms that occur alongside weight changes need medical attention — not a plateau guide.

*Educational only — not medical advice.*
Contact your healthcare provider if you experience:
- Severe or persistent abdominal pain
- Persistent vomiting or inability to keep fluids down
- Signs of dehydration (dark urine, dizziness, rapid heart rate)
- Jaundice (yellowing of skin or eyes)
- Vision changes
- Signs of allergic reaction (swelling, difficulty breathing, rash)
These may or may not be related to your GLP-1 medication, but they require clinical evaluation. Don't self-diagnose with a web article — including this one.
Brand-Name vs. Compounded vs. “Research Peptides”: Know What You're Taking
This matters for plateaus more than most people realize. If your medication isn't what it should be, no amount of diet optimization or dose adjustment will help.
Brand-name GLP-1s (Wegovy, Ozempic, Zepbound, Mounjaro)
Manufactured by Novo Nordisk or Eli Lilly, dispensed through licensed pharmacies, FDA-approved. Consistent potency and purity. Highest cost, but you know exactly what you're getting.
Compounded GLP-1s
These products are not FDA-approved, and quality and ingredients can vary by pharmacy and formulation. The FDA has published updated concerns about unapproved GLP-1 drugs. If prescribed a compounded product, ask your prescriber which pharmacy is used, whether it's a state-licensed 503A pharmacy or an FDA-registered 503B outsourcing facility, and what exact ingredient form is being dispensed. Learn more in our compounded semaglutide safety guide.
“Research peptides” and unverified online sources
The FDA has explicitly warned consumers about products marketed as GLP-1 agonists that are labeled “for research use only” or sold without a prescription through unverified websites. These are not FDA-approved, not manufactured under pharmaceutical quality standards, and not monitored for potency or purity.
If you're experiencing a plateau and your medication came from an unverified source, the medication itself is the most likely culprit. Switch to a verified provider.
Semaglutide vs. Tirzepatide: Complete Comparison for Plateau Decisions
| Factor | Semaglutide (Ozempic / Wegovy) | Tirzepatide (Mounjaro / Zepbound) |
|---|---|---|
| Drug class | GLP-1 receptor agonist | Dual GIP + GLP-1 receptor agonist |
| FDA-approved for weight loss | Wegovy (yes) | Zepbound (yes) |
| How it works | Activates GLP-1 receptors → slows gastric emptying, increases satiety signaling to brain | Activates GLP-1 AND GIP receptors → same GLP-1 effects PLUS additional pathways affecting fat storage, insulin sensitivity, energy expenditure |
| Avg. weight loss (pivotal trials) | ~15% body weight (STEP 1, 68 weeks) | ~21% body weight (SURMOUNT-1, 72 weeks, 15mg) |
| Patients achieving ≥20% loss | ~32% (STEP 1) | ~57% at highest dose (SURMOUNT-1) |
| Titration schedule | 0.25mg → 0.5mg → 1mg → 1.7mg → 2.4mg (4 weeks each) | 2.5mg → 5mg → 7.5mg → 10mg → 12.5mg → 15mg (4 weeks each) |
| Max dose | 2.4 mg/week | 15 mg/week |
| Most common side effects | Nausea (44%), diarrhea (30%), vomiting (24%), constipation (24%) | Nausea (28%), diarrhea (23%), vomiting (13%), constipation (11%) — rates at 15mg per FDA label |
| Administration | Weekly subcutaneous injection | Weekly subcutaneous injection |
| Monthly cost (brand, no insurance) | ~$1,300–$1,600 | ~$1,000–$1,200 |
| Monthly cost (telehealth, compounded) | ~$149–$299 | ~$199–$399 |
| Best for plateau if… | You haven't maxed your dose yet; dose escalation may resolve it | You've maxed semaglutide and need a new mechanism to restart weight loss |
Side effect rates from FDA prescribing information (Wegovy label, Zepbound label). Trial data from published NEJM studies (SURMOUNT-1 treatment-regimen estimand). Pricing ranges reflect major telehealth providers as of February 2026 — verify current pricing directly before signing up.
The core takeaway: if you've exhausted the semaglutide pathway and your plateau persists after lifestyle optimization, tirzepatide's dual mechanism represents the most evidence-supported pharmaceutical escalation available today. Read our full semaglutide vs. tirzepatide comparison for more details.
Common Plateau Breakthrough Patterns We See
Across public forums (Reddit's r/Ozempic, r/semaglutide, r/tirzepatide), patient communities, and review platforms, the same breakthrough patterns show up again and again.
Pattern 1 — The Medication Switch
The most common success story from people at max-dose semaglutide involves switching to tirzepatide and experiencing renewed weight loss. Posts consistently describe stalls of 6–12+ weeks on maximum semaglutide that broke within weeks of starting tirzepatide titration. The phrase that comes up repeatedly: “my body just needed a different tool.”
Pattern 2 — The Protein and Training Fix
People who tracked their food intake during a stall frequently discovered protein intake well below 100g/day. Adding deliberate protein targets and starting resistance training — even basic bodyweight exercises — is a recurring breakthrough story, often breaking stalls of 4–8 weeks.
Pattern 3 — The Medical Discovery
A meaningful subset of plateau posts describe concurrent symptoms (fatigue, hair thinning, cold sensitivity) that turned out to be thyroid dysfunction triggered by rapid weight loss. After treatment for the underlying condition, GLP-1 weight loss resumed.
The people who break through fastest aren't the ones with the most willpower or the best genetics. They're the ones who stop guessing and start diagnosing — who figure out which specific type of plateau they're dealing with and apply the matched fix instead of trying everything at once.
What to Expect After You Break Through Your Plateau
Once you identify the right lever and pull it, here's what the restart typically looks like:
Week 1–2
If the fix involves a behavioral change (protein, resistance training, sleep), you may not see scale movement immediately — but you might notice appetite changes, energy improvements, or measurement changes.
Week 2–4
Most people who've made the right intervention see the scale start moving again. The rate of loss is usually slower than your initial rate — 0.5–1.5 pounds per week. That's fine.
Week 4–8
If you switched medications (e.g., semaglutide to tirzepatide), this is typically when the new medication reaches a therapeutically effective dose through titration and the weight loss effect becomes clear.
Important mindset note
Your second round of weight loss after a plateau will feel slower than your first. That's not because the fix isn't working — it's because your body is smaller, your metabolic adaptation is real, and the initial rapid loss phase is behind you. Slower progress is still progress.
And here's the part nobody tells you: you'll probably hit another plateau later. That's not pessimism — that's biology. But now you have the diagnostic framework. You know the causes, you know the fixes, and you know the order to work through them. The second plateau is less scary than the first because you have a playbook.
How We Built This Guide (and How We Keep It Updated)
Transparency matters — especially for health content with affiliate links. Here's how this page was built and maintained:
- Clinical sources: We reference published, peer-reviewed clinical trial data (STEP, SURMOUNT, SURPASS trial programs), FDA prescribing information for all named medications, and guidelines from the Endocrine Society. Every clinical claim links to its source.
- The Plateau Diagnostic Framework was developed by cross-referencing documented plateau causes from clinical literature with the most common patterns reported by patients in public forums (Reddit, patient communities, review platforms). It's an editorial tool — not a medical diagnostic.
- Pricing and provider details are verified directly from provider websites and marked with “Last Verified” dates. We review and update pricing data monthly.
- Update schedule: This page is reviewed monthly for clinical accuracy, pricing changes, and new FDA guidance.
What this guide is NOT: Medical advice. We're not doctors. We're a research team that reads the clinical literature carefully, verifies claims, and presents the information in a way that helps you make better decisions with your actual healthcare provider. Always consult your physician before making changes to your medication or treatment plan. Read our editorial standards for more details.
FAQ: GLP-1 Plateau and “Not Working Anymore”
Can you plateau on Ozempic?
Yes. Plateaus on Ozempic (semaglutide) are well-documented in clinical trials and extremely common in clinical practice. The STEP trials showed that weight loss velocity naturally decelerates after the first few months for most participants. This is a feature of how the body adapts, not a flaw in the medication.
Can you plateau on Wegovy?
Yes — same active ingredient as Ozempic (semaglutide), higher max dose for weight loss. Plateaus occur on Wegovy just as they do on Ozempic. The higher max dose (2.4mg vs 1mg–2mg for Ozempic used off-label) gives more titration room, but plateaus are still common at any dose.
Can you plateau on Zepbound or Mounjaro?
Yes. Tirzepatide (the active ingredient in both) produces greater average weight loss than semaglutide in clinical trials, but plateaus still occur. The dual GLP-1/GIP mechanism means they may happen later or at a higher total weight loss percentage, but they are not eliminated.
How long does a GLP-1 weight loss plateau last?
Temporary stalls (1–3 weeks) resolve on their own. True plateaus (4+ weeks) typically require intervention. With the right steps, most people restart weight loss within 2–6 weeks. Without intervention, a plateau can become a new maintenance weight indefinitely.
Why did my appetite come back on semaglutide?
Partial appetite adaptation is normal over months. Your GLP-1 receptors can become less sensitive at a stable dose — a process called receptor desensitization. This does not mean the medication stopped working entirely. It means the appetite suppression effect moderated, which may require dose adjustment, lifestyle optimization, or a medication switch to address.
Why am I hungrier on tirzepatide now than when I started?
Same principle as semaglutide — your body adapts. The initial dramatic appetite suppression typically moderates over time. If you are on a stable dose and hunger is returning, talk to your provider about dose escalation (if there is room) or optimization of protein and meal timing to support satiety through complementary pathways.
Should I increase my dose if I stall?
If you are not at your maximum dose and you have been on your current dose for 4+ weeks, dose escalation is the standard first-line pharmaceutical response. But check the non-pharmaceutical factors first (steps 1–6 in the fix plan). Talk to your provider — do not adjust dosing on your own.
What if I'm still on a low dose and not losing?
You may not be at a therapeutically effective dose yet. The titration schedules for both semaglutide and tirzepatide take 4–5 months to reach the maximum dose. Give the process time. If you have been at a low dose for significantly longer than the prescribing information recommends, ask your provider why.
What if I'm at the max dose and not losing?
This is where the decision tree branches. First: complete the 7-step fix plan to rule out non-pharmaceutical causes. If everything checks out, the most evidence-supported next move is switching from semaglutide to tirzepatide (if you are on semaglutide) or discussing adjunctive approaches with your provider.
How do I know if I'm a GLP-1 non-responder?
The Endocrine Society obesity pharmacotherapy guidelines use a benchmark of less than 5% body weight loss after 3 months on a therapeutic dose as the threshold to consider changing approaches. If you achieved meaningful weight loss initially and then stalled, you are not a non-responder — you are plateauing. Different situation, different solutions.
What if I didn't lose weight on Wegovy at all?
True non-response does happen. Some people do not lose significant weight on Wegovy and may need to discuss alternative approaches with their physician. This is a fundamentally different situation from a plateau and should be managed directly with your healthcare provider.
Does constipation cause a fake plateau?
Yes — and it is more common than most people realize. GLP-1 medications slow gastric emptying, which frequently causes constipation. If you have not had a regular bowel movement in several days, the scale can easily be 2–5 pounds higher than your actual fat mass. Track waist measurements alongside weight. If your waist is still shrinking, you are still losing fat — the scale just cannot see it yet.
Do I need to track calories on a GLP-1?
Not necessarily forever. But if you have hit a plateau, a 7-day food audit is one of the most revealing things you can do. Many people discover significant calorie creep they were not aware of. You do not need to track permanently — just long enough to recalibrate.
Does alcohol stall GLP-1 weight loss?
It can. Alcohol adds empty calories (7 calories per gram), impairs fat oxidation (your body prioritizes metabolizing alcohol over burning fat), disrupts sleep quality, and can increase appetite. One or two drinks a week is unlikely to cause a plateau on its own, but regular alcohol consumption is a common contributing factor.
Can stress stop GLP-1 weight loss?
Yes. Chronic stress elevates cortisol, which promotes visceral fat storage, increases appetite (particularly for high-calorie comfort foods), disrupts sleep, and can dampen the appetite-suppressing effects of GLP-1 agonists. Managing stress is not just a wellness recommendation — it is a physiological intervention.
Can antidepressants block GLP-1 weight loss?
Some can. Certain antidepressants — particularly mirtazapine, paroxetine, amitriptyline, and some other tricyclics — are associated with weight gain. If you started or changed an antidepressant around the time your plateau began, bring this up with your prescribing physician. Do not stop any antidepressant without medical guidance.
Does PCOS affect GLP-1 results?
Yes. PCOS (polycystic ovary syndrome) involves hormonal imbalances — including insulin resistance and elevated androgens — that can make weight loss more difficult on any treatment, including GLP-1s. Women with PCOS may experience slower initial weight loss and earlier plateaus. The good news: GLP-1 and GIP agonists actually improve several PCOS-related markers (insulin sensitivity, inflammation).
What labs should I ask for if I'm stalled?
A reasonable panel to request: TSH, Free T4, Free T3 (thyroid function), fasting insulin, HbA1c (metabolic health), comprehensive metabolic panel (liver/kidney function), and if applicable, sex hormones (testosterone, DHEA-S for PCOS evaluation). These help rule out medical causes of plateaus that no amount of dietary adjustment will fix.
What happens if I stop my GLP-1 — will I regain?
The clinical data is consistent: discontinuing GLP-1 medication typically results in significant weight regain. The STEP 1 trial extension showed that participants who stopped semaglutide regained approximately two-thirds of their lost weight over the following year. This is why stopping during a plateau is almost always the wrong move — the medication is still preventing regain even when it is not producing further loss.
Is it normal to lose fast at first, then slow down on GLP-1?
Completely normal. This pattern is so predictable that researchers have modeled it mathematically. Early weight loss is faster because you are losing water and glycogen stores alongside fat, the caloric deficit is largest at your highest weight, and the appetite suppression effect feels strongest when it is new. A slower rate of loss is not the same as a plateau — it is the expected trajectory.
What's the safest way to restart after missed doses?
Follow your specific medication prescribing information and your clinician's instructions. Never double-dose. Wegovy: if next dose is more than 48 hours away, take missed dose ASAP; if less than 48 hours, skip and resume schedule. Zepbound: take missed dose within 4 days (96 hours); if more than 4 days, skip and take next scheduled dose.
Can exercise alone break a GLP-1 plateau?
It depends on the cause. If your plateau is driven by muscle loss and declining metabolic rate, adding resistance training can absolutely be the fix on its own. If it is a dose ceiling issue or a medical factor, exercise alone will not be enough — but it will still help by preserving lean mass and supporting the other interventions.
Will I regain weight if I switch from semaglutide to tirzepatide?
When managed properly, no. The transition from one GLP-1 medication to another is designed to maintain therapeutic effect while adding new mechanisms. Most providers start tirzepatide at a lower dose and titrate up, but the appetite-suppression effect typically continues throughout the transition.
How to talk to your doctor about your GLP-1 plateau
Bring data, not just feelings. Write down: your current dose and how long you have been on it, your weight trend for the past 4–8 weeks, your average daily protein intake, your exercise routine, your sleep patterns, and any other symptoms. State the facts, state what you have tried, and ask a specific question like "Should we adjust my dose or discuss switching medications?"
Primary Sources and References
These are the sources we cite throughout this guide. Every clinical claim traces back to one of these:
- STEP 1 Trial: Wilding JPH, et al. “Once-Weekly Semaglutide in Adults with Overweight or Obesity.” New England Journal of Medicine, 2021. [DOI: 10.1056/NEJMoa2032183]
- SURMOUNT-1 Trial: Jastreboff AM, et al. “Tirzepatide Once Weekly for the Treatment of Obesity.” New England Journal of Medicine, 2022. [DOI: 10.1056/NEJMoa2206038]
- SURPASS-2 Trial: Frías JP, et al. “Tirzepatide versus Semaglutide Once Weekly in Patients with Type 2 Diabetes.” New England Journal of Medicine, 2021. [DOI: 10.1056/NEJMoa2107519]
- Wegovy Prescribing Information (FDA): accessdata.fda.gov
- Zepbound Prescribing Information (FDA): accessdata.fda.gov
- FDA Counterfeit Ozempic Warning: fda.gov
- FDA Unapproved GLP-1 Warning: fda.gov
- Endocrine Society Obesity Pharmacotherapy Guidelines: endocrine.org
- Plateau Physiology Modeling: Hall KD. “Modeling Metabolic Adaptations and Energy Regulation in Humans.” Obesity, 2018. PMC: PMC10705578
- Body Composition During Weight Loss: Willoughby D, et al. Nutrients, 2018. PMC: PMC8089287
- Metabolic Adaptation: Leibel RL, Rosenbaum M, Hirsch J. “Changes in Energy Expenditure Resulting from Altered Body Weight.” New England Journal of Medicine, 1995.
MEDVI
Clinical support + both medications available
Related Guides
- Semaglutide vs. Tirzepatide: Complete Comparison
- How to Prevent Muscle Loss on GLP-1 Medications
- GLP-1 Protein Calculator: Find Your Daily Target
- GLP-1 Constipation Relief: What Actually Helps
- Best GLP-1 Telehealth Providers (2026)
- MEDVI Tirzepatide Reviews
- What Happens When You Stop Taking GLP-1
- Best GLP-1 for PCOS
- How to Take GLP-1 Safely