Disclosure: Some links on this site are affiliate links. If you purchase through these links, we may earn a commission at no extra cost to you. Thank you for supporting our site.·For informational purposes only—not medical advice.
GLP-1 and PCOS: What the Research Actually Shows and How to Choose
By the WPG Research Team | Last verified: February 2026 | Sources: 2023 International PCOS Guideline, 8+ PCOS-specific clinical trials, FDA prescribing information — see full source list below
GLP-1 medications like semaglutide (Ozempic, Wegovy) and tirzepatide (Mounjaro, Zepbound) are not FDA-approved for PCOS. But the research on GLP-1 and PCOS is hard to ignore. In a 2024 meta-analysis of randomized controlled trials, GLP-1 receptor agonists reduced BMI by 2.42 points, waist circumference by 5.16 cm, and total testosterone by 33% in women with PCOS and obesity. The 2023 International Evidence-Based PCOS Guideline — the most authoritative clinical resource in the world for this condition — now says GLP-1 RAs “could be considered” alongside lifestyle changes for managing weight in adults with PCOS.
That's not hype. That's peer-reviewed data from multiple continents, backed by a guideline endorsed by the Endocrine Society, ASRM, and 37 other medical organizations.
But here's what most articles won't tell you: GLP-1s aren't a blanket solution for every type of PCOS. They work best for a specific metabolic profile. They carry real risks — especially if you're planning pregnancy. And the compounded market is a minefield of fraudulent products that the FDA has been actively cracking down on since 2025.
We built this guide to give you everything you need in one place: what the evidence actually shows, which symptoms improve (and which don't), who should and shouldn't consider a GLP-1, the fertility safety rules you can't afford to get wrong, how to avoid getting scammed, and what to do next. Every claim is cited to its source. No fluff. No generic advice.
If you already know GLP-1s are right for you and need to compare providers, skip straight to our Best GLP-1 Providers for PCOS comparison (verified pricing, updated monthly).
*For educational purposes only — not medical advice.*
Quick Decision Box: Should You Consider a GLP-1 for PCOS?
| Your Situation | What to Know |
|---|---|
| PCOS + BMI over 30 + insulin resistance | You're the strongest candidate based on current evidence. GLP-1s address the metabolic root of your symptoms. |
| PCOS + trying to conceive within 3 months | Stop or don't start a GLP-1. Semaglutide (Wegovy): stop ≥2 months before planned pregnancy. Tirzepatide: discuss timing with your clinician. Consider metformin as a bridge. |
| PCOS + trying to conceive in 6–12 months | “Treat and transition” approach: use GLP-1 to improve metabolic health, then stop before trying. Semaglutide: ≥2 months before. Tirzepatide: discuss timing with your clinician. |
| PCOS + type 2 diabetes | GLP-1s are FDA-approved for T2D. Insurance coverage is more likely. Talk to your endocrinologist. |
| Lean PCOS (BMI under 25) without insulin resistance | Evidence is essentially nonexistent for this population. GLP-1s target metabolic features you may not have. |
| History of medullary thyroid carcinoma (MTC) or MEN2 | Contraindicated. Do not use GLP-1 medications. |
| History of pancreatitis | Use caution. Discuss alternatives with your provider (labeled warning/precaution, not a contraindication). |
Why Are So Many Women With PCOS Turning to GLP-1s?
This isn't a trend that came from nowhere.
Prescriptions for GLP-1 medications among women with PCOS rose from 2.4% in 2021 to 17.6% in 2025 — more than sevenfold — according to a review of 120 million patient records by health data firm Truveta, reported by Reuters in December 2025.
Why the explosion? Because PCOS and metabolic dysfunction are deeply intertwined — and for decades, women with PCOS had almost nothing that actually worked.
Here's the reality most PCOS women know firsthand: insulin resistance is common in PCOS, affecting an estimated 65–70% of women with the condition (higher in those with obesity, lower in lean PCOS). Between 40% and 80% of women with PCOS have obesity, depending on the population studied (Cleveland Clinic). The condition creates a metabolic environment where losing weight is dramatically harder than it is for women without PCOS. The standard treatments — metformin for insulin resistance, birth control pills for cycle regulation — are helpful for some, but neither was designed to produce meaningful weight loss. Metformin's weight loss effect is modest at best (typically 1–3% of body weight). Birth control masks symptoms without addressing the metabolic root.
If you feel like you've tried everything and your body still won't cooperate, you're not broken. Your biology is working against you in ways that standard advice (“just eat less and move more”) doesn't account for. PCOS women have been shown to have impaired levels of appetite-regulating hormones like ghrelin and leptin, which can contribute to increased hunger that has nothing to do with willpower.
GLP-1 receptor agonists represent the first real pharmaceutical advancement for the metabolic management of PCOS in years. The American Society for Reproductive Medicine (ASRM) now includes them as an option for managing obesity in women with PCOS. That's not a fringe opinion — it's a guideline-level recommendation from one of the most respected reproductive medicine bodies in the world.
How Do GLP-1s Actually Work for PCOS?
This is where it gets important — and where most articles oversimplify.
Every site will tell you “GLP-1s help with weight loss, and weight loss helps PCOS.” That's true, but it's incomplete. Here's the fuller picture of what's happening in your body.
The Insulin-Androgen Loop (Why PCOS Makes Weight Loss So Hard)
PCOS, for most women, runs on a vicious cycle:
Insulin resistance → excess insulin → ovaries overproduce testosterone → irregular ovulation, acne, hair growth, weight gain → weight gain worsens insulin resistance → cycle repeats.
This is why “just eat less” fails for so many women with PCOS. Your body is trapped in a feedback loop that's hormonally driven, not a willpower problem.
How GLP-1s Break the Loop
GLP-1 receptor agonists intervene at multiple points in this cycle — not just one:
1. They improve insulin sensitivity. GLP-1s stimulate insulin release in a glucose-dependent manner and reduce hyperinsulinemia. Less excess insulin means the ovaries get less of the signal to overproduce androgens. This is the mechanism that makes GLP-1s different from just “a weight loss drug” for PCOS. (Source: PMC 10532286)
2. They promote significant weight loss. Through appetite reduction via brain signaling (GLP-1 receptors in the hypothalamus) and slowed gastric emptying. Even 5–10% body weight reduction can meaningfully improve PCOS symptoms.
3. They reduce “food noise.” Many patients with PCOS describe this as life-changing. The constant background chatter about food — what to eat, when to eat, the cravings that won't quit — goes quiet. As one patient described to the PCOS Nutrition Center: these medications made her feel like a “normal” person regarding hunger and cravings for the first time.
4. They may have direct reproductive effects. Preclinical studies suggest GLP-1 RAs can directly improve reproductive function by reversing high luteinizing hormone (LH) levels and reducing serum testosterone and free androgen index — independent of weight loss (Bednarz et al., 2022). This is still being studied in humans, but it's a promising signal.
5. They reduce chronic inflammation. PCOS is an inflammatory condition. GLP-1s have demonstrated anti-inflammatory effects on adipose tissue and vascular endothelium, reducing atherothrombosis markers in PCOS patients (PMC 10532286).
6. They improve liver health. Non-alcoholic fatty liver disease is common in PCOS. In one trial, liraglutide reduced liver fat by 44% in women with PCOS over 26 weeks (Frøssing et al., 2018).
Why This Matters More for PCOS Than General Obesity
Women with PCOS aren't just dealing with weight. They have higher baseline insulin levels than weight-matched women without PCOS, impaired appetite hormones, and a hormonal cascade that makes every pound harder to lose and easier to gain. GLP-1s address this specific metabolic profile in ways that diet alone — and even metformin alone — often can't match.
There's something else worth naming: the psychological weight of PCOS. Many women with this condition have spent years being told they just need to try harder, exercise more, eat less. They've done all of that. The weight didn't budge — or it came right back. That's not a character flaw. That's insulin resistance and impaired satiety signaling doing what those conditions do. GLP-1s don't replace discipline. They level a playing field that was never level to begin with.
What the 2023 International PCOS Guideline Says About GLP-1s
If you're going to cite one source when talking to your doctor about this, make it this one.
The 2023 International Evidence-Based Guideline for the Assessment and Management of PCOS — developed through engagement of 3,000+ health professionals and 100+ multidisciplinary experts across 71 countries, with partners including ASRM, the Endocrine Society, ESHRE, and the European Society of Endocrinology — is the most comprehensive clinical guideline ever produced for PCOS. Published through Monash University and endorsed by 39 societies and organizations worldwide.
The guideline's recommendation:
GLP-1 RAs “could be considered” for weight management in adults with PCOS, alongside lifestyle modifications. This is a conditional recommendation — meaning the evidence is supportive but not yet strong enough for a firm directive.
Three guideline cautions people miss:
- Contraception is recommended when GLP-1s are used in women of reproductive age, because pregnancy data is limited and GLP-1s are not proven safe during pregnancy.
- Gradual dose escalation is recommended to minimize gastrointestinal side effects.
- Shared decision-making is essential — the guideline emphasizes discussing weight regain risk after stopping, limited long-term safety data in PCOS specifically, and individual goals.
The fertility caveat that's critical to understand:
The guideline states that anti-obesity agents for reproductive outcomes (meaning using them specifically to improve fertility) should be used only in research settings. In other words: GLP-1s can help your metabolic health, which may indirectly improve fertility — but they're not positioned as a fertility treatment, and you can't be on them when you conceive.
(Source: Teede et al., 2023. International Evidence-Based Guideline for the Assessment and Management of PCOS. Monash University.)
What the Clinical Trials Actually Show
This is where we go beyond “it may help” and into real numbers. We reviewed every PCOS-specific GLP-1 study we could find. Here's what the data says.
PCOS-Specific Clinical Trial Results
| Study | Drug & Dose | Who Was Studied | Duration | Key Results for PCOS |
|---|---|---|---|---|
| Jensterle et al., 2017 | Liraglutide 1.2mg/day vs. Metformin 1000mg 2x/day | Women with PCOS + obesity, previously on metformin | 12 weeks | Liraglutide reduced BMI by 1.1 kg/m² vs. 0.1 for metformin |
| Frøssing et al., 2018 | Liraglutide 1.8mg/day vs. placebo | 72 overweight women with PCOS | 26 weeks | Body weight ↓ >5%, liver fat ↓ 44%, visceral fat ↓ 18%, free testosterone ↓ 19% |
| Elkind-Hirsch et al., 2020 | Liraglutide 3mg/day vs. placebo | Women with PCOS + obesity | 32 weeks | Superior weight loss, reduced hyperandrogenism, improved cardiometabolic markers |
| Liao et al., 2023 | Liraglutide + Metformin vs. Metformin + OCP | 60 overweight PCOS patients | 12 weeks | GLP-1 combo showed greater reductions in BMI, waist circumference, fasting glucose, and ovulation rate |
| Carmina et al., 2023 | Semaglutide 0.5mg weekly | 27 obese women with PCOS unresponsive to lifestyle modification | 3–6 months | ~80% achieved ≥5% weight loss. Mean loss: 7.6 kg. BMI ↓ 3.1. Menstrual regularity improved in responders. |
| Prediabetes Remission Trial | Exenatide + Metformin vs. each alone | 153 prediabetic women with PCOS | 12 weeks | Prediabetes remission: 64% (combo), 56% (exenatide), 32% (metformin) |
| 2024 Meta-Analysis (4 RCTs) | GLP-1 RAs vs. placebo | 176 participants with PCOS | Variable | BMI ↓ 2.42, waist ↓ 5.16 cm, triglycerides ↓, total testosterone ↓ 33%. No significant change in HOMA-IR. |
(Sources: PMC 10532286, ScienceDirect meta-analysis, ClinicalTrials.gov NCT05819853, Cureus scoping review)
What This Data Means in Plain English
The evidence consistently shows GLP-1s reduce weight, BMI, and waist circumference in women with PCOS — and they do it more effectively than metformin alone. The testosterone reduction (about 33%) is clinically meaningful: that's the hormone driving your acne, excess hair growth, and hair thinning. Menstrual regularity improves in most women within 3–6 months.
But let's be honest about the limitations:
- These are small studies. The largest meta-analysis included only 176 participants across 4 trials.
- Most trials lasted 12–26 weeks. We don't have strong long-term PCOS-specific data yet.
- No large-scale randomized controlled trial specifically for PCOS has been completed. Several are underway (NCT04876027, NCT03919929, NCT05702905).
- The insulin resistance finding is mixed — HOMA-IR didn't reach statistical significance in the meta-analysis, even though fasting glucose consistently improved.
- We don't have head-to-head comparisons of different GLP-1s specifically for PCOS.
The evidence is strongest for overweight or obese women with PCOS and insulin resistance who haven't responded adequately to lifestyle changes alone. If that's you, the data is genuinely encouraging. If you're lean with PCOS and no metabolic features, the evidence simply doesn't exist yet.
Which PCOS Symptoms Do GLP-1s Actually Help?
Not every PCOS symptom responds equally. Here's an honest breakdown of what we know.
| PCOS Symptom | Does a GLP-1 Help? | Evidence Strength | What to Expect |
|---|---|---|---|
| Weight / BMI | ✓ Yes, significantly | Strong (multiple RCTs) | 5–15%+ body weight loss typical. ~80% of patients in one trial lost ≥5%. |
| Insulin Resistance | ✓ Yes | Moderate | Fasting glucose improves consistently. HOMA-IR results are mixed statistically. |
| High Testosterone | ✓ Yes | Moderate–Strong | ~33% reduction. This drives improvements in acne and excess hair growth. |
| Irregular Periods | ✓ Yes, for most | Moderate | Regularity improves within 3–6 months in the majority of patients. |
| Fertility | ✓ Likely (indirect) | Emerging | Weight loss + better insulin = restored ovulation. Stop medication before conception. |
| Acne | ● Possibly | Indirect | Via testosterone reduction. No direct acne-specific PCOS trials. |
| Excess Hair Growth | ● Possibly | Indirect | Via testosterone reduction. Hair growth cycle is slow — expect months, not weeks. |
| Hair Loss / Thinning | ⚠ Complicated | Insufficient data | Rapid weight loss itself can trigger telogen effluvium (temporary shedding). Monitor carefully. |
| NAFLD (Fatty Liver) | ✓ Yes | Moderate | Liraglutide reduced liver fat by 44% in one PCOS trial. |
| Cardiovascular Risk | ✓ Yes | Moderate | Improved lipid profiles, reduced inflammation, better atherothrombosis markers. |
| Mood / Energy | ● Possibly | Anecdotal + indirect | Many patients report improved energy and reduced brain fog. Likely metabolic improvement. |
| Ovarian Cysts | ● Possibly | Limited | Some evidence of decreased ovarian volume (Nylander et al.). |
What GLP-1s Won't Fix
Let's be direct about this: GLP-1 medications won't cure PCOS. There is no cure. They won't permanently fix the hormonal imbalance. Most women regain weight within about a year of stopping (though lifestyle changes made during treatment help). They won't replace healthy eating and exercise — they work best alongside those habits. And they won't treat lean PCOS effectively if there's no metabolic component to target.
Think of GLP-1s as a powerful tool for managing the metabolic engine driving your PCOS symptoms. Not a cure. Not a shortcut. A tool — and potentially a very effective one.
GLP-1 vs. Metformin for PCOS: The Honest Comparison
This is the comparison most women with PCOS want, so let's do it properly.
| Factor | GLP-1 Medications | Metformin |
|---|---|---|
| Weight Loss | Significant: 5–15%+ body weight | Modest: 1–3% at best |
| Insulin Sensitivity | Improves (glucose-dependent insulin release) | Improves (reduces hepatic glucose output) |
| Testosterone Reduction | ~33% in meta-analysis | Modest reduction |
| Menstrual Regularity | Improves for most within 3–6 months | Improves for some |
| Fertility | Indirect improvement. Semaglutide: stop ≥2 months before planned pregnancy. Tirzepatide: discuss timing with clinician. | Safer closer to conception. Stop at pregnancy confirmation. |
| Cost Without Insurance | $200–$1,000+/month (brand) or $99–$399 (telehealth/compounded) | $4–$30/month (generic) |
| How You Take It | Weekly injection (semaglutide/tirzepatide) or daily (liraglutide) | Oral pill, 1–2x daily |
| Common Side Effects | Nausea (~44%), vomiting (~24%), dizziness (~15%). Usually fade after 4–8 weeks. | GI distress, diarrhea, B12 deficiency. Can be ongoing. |
| Long-Term Safety Data | Limited for PCOS (<5 years) | Extensive (decades) |
| Insurance Coverage for PCOS | Inconsistent. Better if you also have obesity or T2D. | Usually covered. |
| Guideline Status | “Could be considered” for weight management (2023 guideline) | “Should be considered” in adults with PCOS and BMI ≥25 for metabolic outcomes (2023 guideline) |
Our Take
If weight loss is the primary goal and metformin hasn't delivered: GLP-1s are likely more effective. The data isn't close.
If cost is a major barrier: Metformin costs a fraction of what GLP-1s cost. Don't underestimate the value of a $10/month medication that still improves insulin sensitivity.
If you're planning pregnancy soon: Metformin gives you a safer timeline. You don't need a multi-month washout period.
If you're prediabetic with PCOS: The combination of both may be the strongest option. In one trial, exenatide plus metformin achieved a 64% prediabetes remission rate versus 32% for metformin alone.
The sequential approach worth knowing about: One study found that using metformin after stopping a GLP-1 helped minimize weight regain over two years. They may work best in sequence — GLP-1 for the heavy lifting, metformin as a maintenance bridge.
MEDVI
Semaglutide & tirzepatide available
Which GLP-1 Medication Is Best for PCOS?
There's no single “best” answer — because no head-to-head trials comparing different GLP-1s specifically for PCOS exist yet. But we can lay out what's known for each.
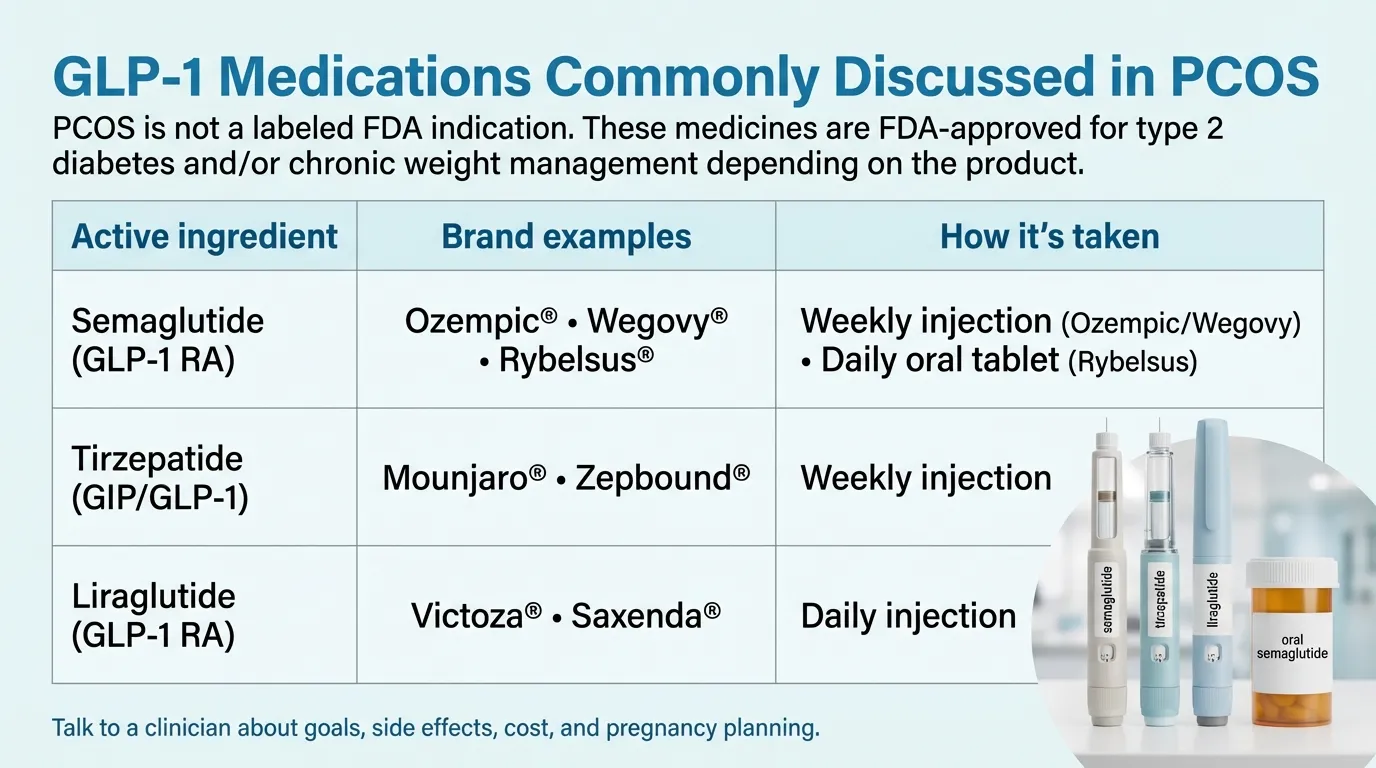
*PCOS is not a labeled FDA indication. These medicines are FDA-approved for type 2 diabetes and/or chronic weight management depending on the product.*
| Semaglutide | Tirzepatide | Liraglutide | Exenatide | |
|---|---|---|---|---|
| Brand Names | Ozempic, Wegovy, Rybelsus | Mounjaro, Zepbound | Saxenda, Victoza | Byetta, Bydureon |
| Type | GLP-1 RA | Dual GIP/GLP-1 RA | GLP-1 RA | GLP-1 RA |
| How Often | Weekly injection (Rybelsus is daily oral) | Weekly injection | Daily injection | Twice daily or weekly |
| PCOS Studies | 2+ trials (semaglutide specifically) | Very limited PCOS data | Most studied for PCOS (5+ trials) | 2–3 PCOS studies |
| Weight Loss (general) | ~15% body weight | ~20–25% body weight (highest in class) | ~8% body weight | ~5–7% body weight |
| FDA Approved For | T2D (Ozempic), Obesity (Wegovy) | T2D (Mounjaro), Obesity (Zepbound) | T2D (Victoza), Obesity (Saxenda) | T2D only |
| Oral Option? | Yes (Rybelsus) | Not yet | No | No |
| Typical Brand Cost | $900–$1,350/mo | $1,000–$1,200/mo | $1,300–$1,400/mo | $700–$900/mo |
| Birth Control Flag | No known interaction with OCs. Stop ≥2 months before planned pregnancy (Wegovy PI). | May reduce oral contraceptive effectiveness. Barrier method or non-oral contraceptive recommended for 4 weeks after initiation and each dose escalation (Zepbound PI). | Stop before planned pregnancy (Saxenda PI). | Limited pregnancy data. |
If We Had to Pick (and Why)
For most women with PCOS: Semaglutide is the most practical choice. It has the broadest availability, the most accessible pricing through telehealth, a once-weekly injection schedule, and an oral option (Rybelsus) if you can't tolerate injections. The PCOS-specific data is growing.
For maximum weight loss: Tirzepatide (Mounjaro/Zepbound) produces the highest weight loss in the class through its dual GIP/GLP-1 mechanism. But the PCOS-specific evidence is thin, and if you're on oral birth control, you need to know about the interaction (barrier method required — see the fertility section below).
If your doctor wants the most PCOS-specific research: Liraglutide (Saxenda/Victoza) has the longest track record in PCOS clinical trials. The daily injection is a drawback for adherence, but the evidence base is the deepest.
Are GLP-1s Right for You? The Decision Framework
Not every woman with PCOS should take a GLP-1. Here's how to think through it.
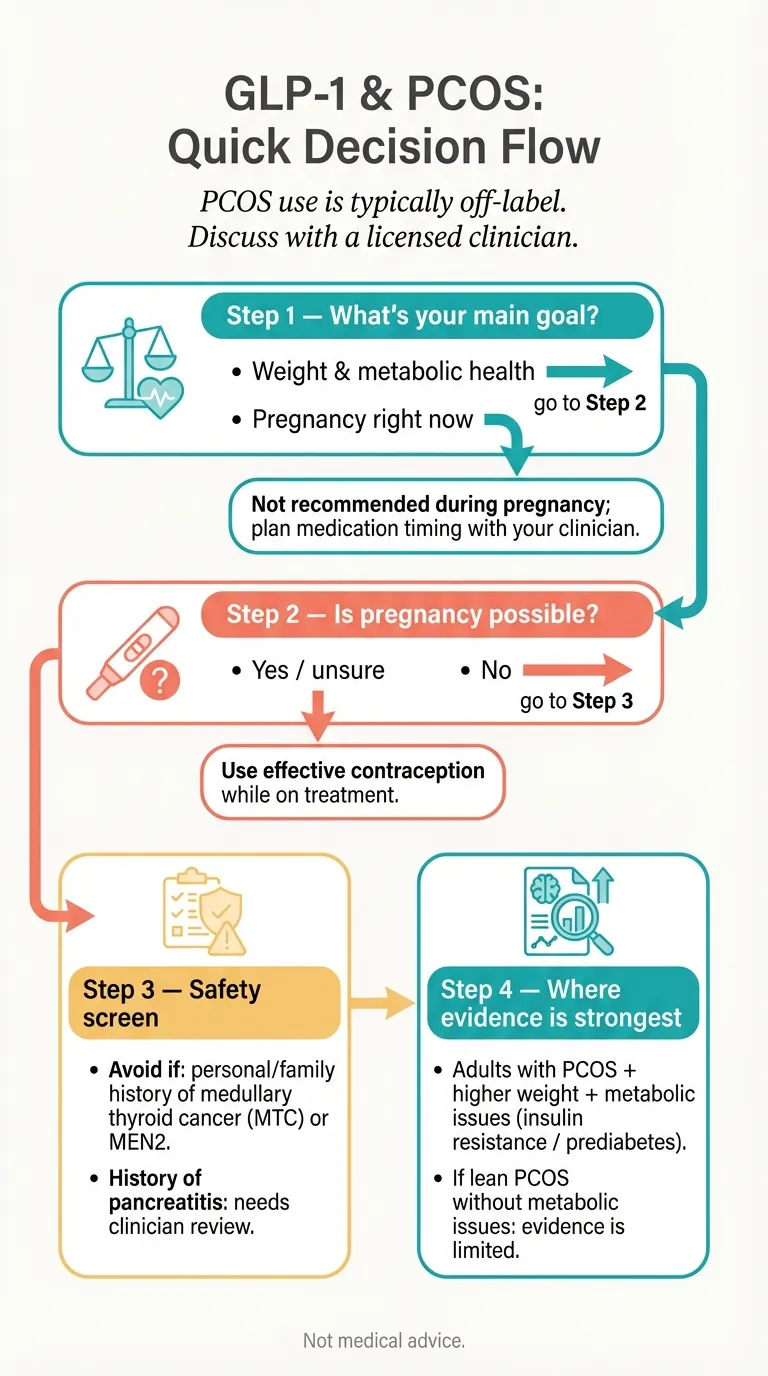
*PCOS use is typically off-label. Discuss with a licensed clinician.*
You're Likely a Good Candidate If:
- You have PCOS with insulin resistance (high fasting insulin, high HOMA-IR, acanthosis nigricans, elevated fasting glucose)
- Your BMI is over 30 — or over 27 with metabolic complications
- You've genuinely tried lifestyle modifications for 3+ months and haven't seen adequate results
- Metformin hasn't produced meaningful improvement (or you can't tolerate it)
- You're NOT pregnant or actively trying to conceive within the next 2–3 months
- You can commit to the medication for at least 3–6 months (this isn't an overnight fix)
- You're prepared to maintain lifestyle changes alongside the medication
GLP-1s Are Probably NOT Right for You If:
- You have lean PCOS without insulin resistance — the evidence simply doesn't support GLP-1 use in this population.
- You're trying to get pregnant within 2–3 months — semaglutide requires ≥2 month washout; for other GLP-1s, discuss timing with your clinician. See our fertility section below.
- You have a history of medullary thyroid carcinoma or MEN2 — this is a labeled contraindication per FDA prescribing information.
- You have a history of pancreatitis — GLP-1s carry a pancreatitis warning/precaution. Use caution and discuss alternatives with your provider.
- You have active diabetic retinopathy — semaglutide specifically carries this caution.
- Cost is a complete barrier and no telehealth or compounded option is accessible to you.
The Gray Zone — Worth Discussing With Your Doctor:
- BMI 25–30 with PCOS and insulin resistance: some providers prescribe, but the research is thinner here.
- You're on metformin and it's partially working: adding a GLP-1 or switching may be worth exploring.
- You want to optimize fertility in 6+ months: the “treat, improve, wash out, conceive” approach is increasingly common, but it requires careful planning with your provider.
Side Effects: What Actually Happens and When
Let's replace fear with data.
The Most Common Side Effects (With Real Numbers From the Wegovy Label)
- Nausea: ~44% of users. The most common complaint. Usually worst in the first 2–4 weeks.
- Diarrhea: ~30%.
- Vomiting: ~24%. Often triggered by eating too much or too fast while your body adjusts.
- Constipation: ~24%.
- Abdominal pain: ~20%.
- Dizziness: ~8%.
- Reduced appetite: Expected. This is part of how the medication works.
- Discontinuation rate: In pivotal trials, 6.8% of patients discontinued semaglutide due to adverse reactions. (Source: Wegovy prescribing information, FDA)
The Side Effect Timeline
Weeks 1–4: This is the hardest period. Side effects peak. Start at the lowest dose. Eat smaller, more frequent meals. Stay hydrated. Most doctors start semaglutide at 0.25 mg weekly.
Weeks 4–8: Side effects significantly diminish for most people as the body adjusts.
Month 3+: Most patients tolerate the medication well. GI symptoms are uncommon. This is when you're seeing meaningful results.
Serious Risks (Low Probability, but You Need to Know)
Thyroid C-cell tumors: GLP-1 RAs carry an FDA black box warning based on rodent studies showing increased thyroid C-cell tumor incidence. It is unknown whether semaglutide causes thyroid C-cell tumors, including medullary thyroid carcinoma (MTC), in humans. Contraindicated if you have personal or family history of MTC or MEN2. (Source: Wegovy prescribing information, FDA)
Pancreatitis: Reported in post-marketing surveillance. Risk is low but real. If you experience severe, persistent abdominal pain — especially with vomiting — seek immediate medical care and discontinue the medication.
Gallbladder problems: Rapid weight loss increases gallstone risk. This isn't unique to GLP-1s — it happens with any significant weight loss.
Kidney injury: Possible through dehydration if you experience severe vomiting or diarrhea. Stay hydrated, especially early on.
PCOS-Specific Concerns
Hair thinning: This comes up a lot in PCOS forums. It's important to understand that rapid weight loss from any cause can trigger telogen effluvium (temporary excessive shedding). It's not a direct GLP-1 effect — it's a consequence of rapid caloric deficit. Usually resolves within 6–12 months. If you already have PCOS-related hair thinning, monitor closely with your provider.
Under-eating and malnutrition: When appetite drops dramatically, nutrient intake can suffer. Protein, iron, vitamin D, and B12 are especially important for PCOS women. Work with a dietitian if possible. Don't just eat less — eat well.
Fertility surprise: GLP-1s can restore ovulation in women who weren't ovulating. If you don't want to get pregnant, use reliable contraception. This brings us to the next critical section.
Fertility, Pregnancy, and Birth Control: The Rules You Can't Skip
This section exists because getting it wrong has real consequences.
The Core Rule
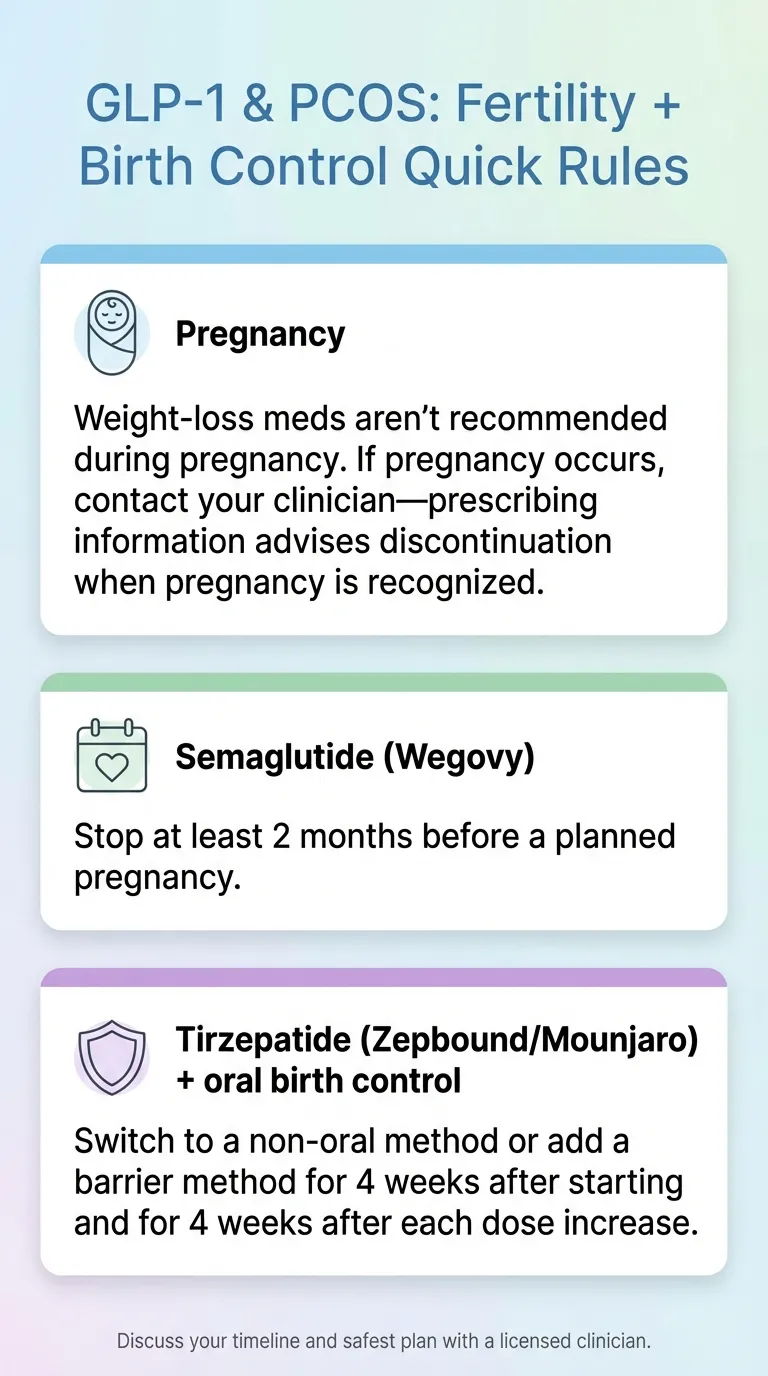
GLP-1 and GIP/GLP-1 drugs are NOT recommended during pregnancy. Prescribing information for these medications warns they may cause fetal harm and recommends discontinuation when pregnancy is recognized. Semaglutide (Wegovy) specifically recommends stopping at least 2 months before a planned pregnancy due to its long half-life.
*Discuss your timeline and safest plan with a licensed clinician.*
The Recommended Timeline
- Semaglutide (Wegovy): Stop at least 2 months before planned pregnancy. (Source: Wegovy prescribing information, FDA)
- Liraglutide (Saxenda): Discontinue before planned pregnancy. (Source: Saxenda prescribing information, FDA)
- Tirzepatide (Zepbound): Labeling advises discontinuation when pregnancy is recognized. No specific washout period is stated in the label — discuss timing before conception with your clinician.
The Birth Control Interaction Most People Miss
Tirzepatide (Mounjaro, Zepbound) may reduce the effectiveness of oral contraceptive pills. The prescribing information advises patients on oral hormonal contraceptives to switch to a non-oral method, or add a barrier method (condoms), for 4 weeks after starting tirzepatide and for 4 weeks after each dose escalation. (Source: Zepbound prescribing information, FDA)
If you're on the pill and starting tirzepatide, talk to your doctor about backup contraception. The 2023 International PCOS Guideline specifically recommends effective contraception when using GLP-1s in women of reproductive age.
Why “Ozempic Babies” Happen
It's not mysterious. Here's the chain of events:
- Woman with PCOS hasn't been ovulating regularly (a core feature of PCOS)
- Starts GLP-1 medication
- Loses weight, insulin resistance improves, androgen levels drop
- Ovulation resumes — sometimes before she notices her period is back
- Without contraception, pregnancy occurs
This has been documented across community forums, in news coverage, and confirmed by reproductive endocrinologists. Even a modest 5–10 pound weight loss can restore ovulation in some PCOS women. This is good news if you want a baby — but only if you time it correctly and stop the GLP-1 first.
The “Treat and Transition” Fertility Protocol
If you want to use a GLP-1 to get fertility-ready, here's what reproductive endocrinologists typically recommend:
- Use GLP-1 for 3–12 months to achieve metabolic improvement and weight loss
- Stop the GLP-1 before trying to conceive. Semaglutide: ≥2 months before planned pregnancy (per Wegovy labeling). Tirzepatide: labeling advises discontinuation when pregnancy is recognized — discuss your specific timeline with your clinician.
- Bridge with metformin during the transition period to minimize weight regain and maintain insulin sensitivity
- Monitor menstrual regularity — many women find cycles are more regular even after stopping
- Optimize nutrition — folate, iron, vitamin D, adequate protein
- Proceed with conception attempts once menstrual cycles have stabilized
If you're planning IVF, IUI, or ovulation induction, discuss the appropriate medication discontinuation timeline with your reproductive endocrinologist well in advance of starting treatment.
What Happens When You Stop Taking a GLP-1?
We'll be straight with you: most people regain weight after stopping. But context matters, and it's not as simple as “it all comes back.”
Clinical data shows weight tends to return toward pre-treatment levels within about a year of stopping GLP-1 therapy. However, more than half of patients in some studies maintained the achieved weight loss at one year post-discontinuation. The range is wide. Learn more in our complete guide to stopping GLP-1 medications.
The biggest predictor of what happens after stopping? Whether you built sustainable habits during treatment. If you used the medication as a window to establish healthy eating patterns, regular exercise, and a relationship with food that doesn't involve constant fighting — you're in a much better position.
Strategies to Minimize Regain
- Transition to metformin — one study showed this helped minimize weight regain over two years after stopping a GLP-1.
- Continue the nutrition and exercise habits you developed during treatment. The medication reduces appetite; the habits give that reduced appetite something to work with.
- Work with a dietitian during and after treatment. Especially important for PCOS women who need to balance macros carefully.
- Consider GLP-1s as long-term management — increasingly, obesity medicine specialists view these as appropriate for chronic use, similar to blood pressure medication for hypertension.
The PCOS Reframe
PCOS is a chronic condition. Managing it with medication long-term isn't “cheating” or “taking the easy way out.” It's treating a metabolic disorder with a tool that addresses the metabolic dysfunction driving your symptoms. Many women will need ongoing treatment — whether that's a GLP-1, metformin, lifestyle modifications, or some combination — for the long haul. That's okay. That's good medicine.
What to Expect: The PCOS GLP-1 Timeline
If you start a GLP-1, here's a realistic picture of what the journey looks like — week by week, based on clinical data and patient-reported experiences.
Week 1–2: The Adjustment Phase
You'll likely notice reduced appetite within the first few days. Some women describe the “food noise” quieting almost immediately — the constant background hum of thinking about food, planning meals, fighting cravings. That can feel dramatic. Side effects may start: nausea is most common. Eat smaller portions, avoid greasy or heavy foods, and stay hydrated. You're at the lowest dose during this phase.
Week 3–4: Side Effects Peak, Then Begin Fading
This is often the toughest stretch. Nausea may intensify as you adjust, especially if you titrate up. Weight loss typically starts — usually 2–5 pounds in the first month, mostly from reduced caloric intake. Some women report noticeable changes in blood sugar stability (fewer crashes, less afternoon fatigue). Energy may fluctuate.
Month 2–3: The Turning Point
For most women, this is when GI side effects fade significantly and the medication starts working in a more comfortable rhythm. Weight loss becomes more consistent. If you're tracking labs, fasting glucose and insulin levels may begin improving. Your body is adjusting to the new metabolic signaling. Second or third dose escalation typically happens during this window.
Month 3–6: Visible Results
This is the window where PCOS-specific improvements start showing. In clinical trials, menstrual regularity improved for most women within this timeframe. Testosterone levels drop measurably (that 33% reduction from the meta-analysis). You may notice less acne, fewer new coarse hairs, and improved skin quality. Weight loss continues — many women are down 10–20+ pounds by month 6, depending on starting weight and dose. Lab markers (A1C, lipids, liver enzymes) typically show improvement at the 3-month check.
Month 6–12: Maximizing Benefits
Weight loss may slow (this is normal — it's not a failure). Your body is recalibrating. The metabolic improvements continue to deepen. This is the window where the cumulative effects on hormones, ovulation, and inflammation are strongest. If you're planning a fertility timeline, month 6–12 is often when reproductive endocrinologists suggest transitioning to the washout phase.
The Plateau Reality
Almost everyone hits a plateau. It doesn't mean the medication stopped working. Your resting metabolic rate adjusts as you lose weight — your body resists further loss. This is normal physiology, not a medication failure. Your provider may adjust your dose. The focus should shift from the scale to metabolic markers, symptom improvement, and how you feel day-to-day. Read our complete GLP-1 plateau guide for the fix plan.
What to Track (PCOS-Specific)
Keep a simple log of:
- Weight and waist measurement (weekly)
- Period dates and regularity
- Acne severity
- Energy levels and mood
- Side effects
- Lab results at 3 and 6 months (compare to baseline)
This data is invaluable for your follow-up appointments and for deciding whether to continue, adjust, or transition.
Cost, Insurance, and How to Actually Get a GLP-1 for PCOS
Let's talk real numbers.
What GLP-1s Actually Cost
- Brand-name (Wegovy, Zepbound, Ozempic): $900–$1,400/month without insurance
- With insurance (if covered): Copays vary widely. $25–$150/month on good plans.
- Telehealth providers (compounded or membership models): $99–$399/month typically
- Metformin (for comparison): $4–$30/month generic
Will Insurance Cover GLP-1s for PCOS?
Honest answer: it's inconsistent. Here's what we've seen:
- If you have PCOS + obesity (BMI ≥30): Better chance of coverage under the obesity indication
- If you have PCOS + type 2 diabetes: Strongest chance of coverage, since GLP-1s are approved for T2D
- If you have PCOS alone without obesity or T2D diagnosis: Coverage is unlikely for GLP-1s specifically
Insurance tip: Ask your doctor to code for obesity (E66) or insulin resistance as the primary diagnosis, with PCOS as secondary. Request prior authorization with documentation of your BMI, fasting insulin levels, and documented failure of lifestyle modification and/or metformin.
Three Routes to Getting a Prescription
1. Through your own doctor — endocrinologist, OB/GYN, or primary care. Best if you have insurance coverage or want in-person care. Bring your labs (fasting insulin, fasting glucose, A1C, testosterone, lipid panel).
2. Through a telehealth provider — many platforms now prescribe GLP-1s and evaluate PCOS as a qualifying condition. Prices range from $99–$399/month including medication. This is often the most accessible option for women without a T2D diagnosis.
3. Through a weight management clinic — some offer package pricing that includes medication, lab monitoring, and nutritional counseling.
What to Ask Your Doctor (Scripts)
If you're nervous about the conversation, try these approaches:
“I have PCOS with insulin resistance, and I've been struggling with weight despite lifestyle changes. I've been reading about GLP-1 medications — the 2023 PCOS guideline says they could be considered alongside lifestyle modifications. Can we discuss whether this might be appropriate for me?”
“I've been on metformin for [X months/years] and it hasn't produced the metabolic improvement we were hoping for. Are GLP-1 receptor agonists something we should consider as a next step?”
“I'm planning pregnancy in [timeframe]. Could we discuss using a GLP-1 to optimize my metabolic health before conception, with a planned washout period?”
How to Avoid Scams: Compounded GLP-1 Safety
This is where we need to get serious, because the compounded GLP-1 market has become genuinely dangerous — and the FDA has been increasingly aggressive about it.
What the FDA Has Found
Fraudulent products are real. The FDA has identified compounded semaglutide and tirzepatide products with false information on labels. In some cases, the pharmacies listed on the labels don't even exist. In other cases, real pharmacy names appear on products those pharmacies didn't actually compound. (Source: FDA, “Concerns with Unapproved GLP-1 Drugs Used for Weight Loss,” updated Feb 2026)
Dosing errors are causing hospitalizations. The FDA received multiple reports of adverse events — some requiring hospitalization — from dosing errors with compounded injectable semaglutide. Patients unfamiliar with vials and syringes have measured and self-administered incorrect doses, and healthcare providers have miscalculated doses due to varying concentrations. (Source: FDA Safety Alert on Compounded Semaglutide Dosing Errors)
“Semaglutide salts” are a red flag. The FDA has noted that some compounded products use salt forms (semaglutide sodium, semaglutide acetate) and states it is not aware of a lawful basis for their use in compounding. If your compounded product lists a semaglutide “salt” on the label, raise this with your provider immediately. (Source: FDA, “Concerns with Unapproved GLP-1 Drugs Used for Weight Loss”)
50+ warning letters in September 2025. The FDA sent warning letters to more than 50 companies — including major telehealth platforms like Hims & Hers — for marketing compounded GLP-1s with false or misleading claims. Companies cannot claim compounded drugs are “the same as” or “generic versions of” FDA-approved products.
“Animal grade” semaglutide has been found. The FBI's IC3 reported that a medical spa was selling compounded semaglutide made with “animal grade” semaglutide combined with B12 — completely incompliant with FDA regulations.
February 2026 update: The FDA announced plans to restrict the active pharmaceutical ingredients used in mass-marketed compounded GLP-1 drugs, established an import alert for GLP-1 APIs from unverified foreign sources, and is taking further steps to combat misleading direct-to-consumer advertising.

*Not medical advice. If unsure, ask your clinician or pharmacist.*
Your “Safe GLP-1 Online” Checklist
Before you order from any telehealth provider or online pharmacy, verify these. For a deeper dive, read our complete guide to compounded semaglutide safety.
Prescriber is licensed — verify their medical license through your state's medical board
Pharmacy is state-licensed — you can verify at your state's board of pharmacy website
You know if it's brand-name or compounded — ask explicitly. “Is this FDA-approved Wegovy/Ozempic, or is it a compounded product?”
If compounded: check the vial/pen details — what's the concentration? What are the dosing units? Were instructions provided?
The product requires a prescription — if anyone sells you a GLP-1 without a medical evaluation, that's a red flag
No “research peptide” language — products labeled “for research purposes” or “not for human consumption” are illegal when sold for human use
Check for red flags — spelling errors on labels, unfamiliar pharmacy names, suspiciously low prices, products shipped warm when they should be refrigerated
Ask the pharmacy directly — if a product has a pharmacy name on the label, call that pharmacy and ask if they made it
This is not paranoia. The FDA, FBI, and multiple state pharmacy boards have documented real harm from fraudulent GLP-1 products. Protecting yourself takes five minutes of verification.
How to Get Started: Your Action Steps
You've read the evidence. You understand the risks. You know whether you might be a candidate. Here's what to do next.
Step 1: Get Baseline Labs
Before starting any GLP-1, these labs give your provider (and you) a baseline to measure improvement:
- Fasting insulin
- Fasting glucose
- HOMA-IR (calculated from fasting insulin and glucose)
- Hemoglobin A1C
- Total and free testosterone
- DHEA-S
- Lipid panel (total cholesterol, LDL, HDL, triglycerides)
- Thyroid panel (TSH, free T4)
- Liver function tests (ALT, AST)
- Vitamin D, B12
Step 2: Talk to Your Doctor
An endocrinologist or OB/GYN with PCOS experience is ideal. Bring your labs. Be specific about what you've already tried and what your goals are — weight management, metabolic health, fertility planning, or all of the above.
Step 3: If Your Doctor Won't Prescribe
Some providers are cautious about off-label use. That's their right. A telehealth provider specializing in weight management or GLP-1 prescribing may be more willing to evaluate you, especially if you have documented PCOS with obesity or insulin resistance.
Step 4: Start Low, Go Slow
Every GLP-1 starts at the lowest dose and titrates up over weeks to months. For semaglutide, this means starting at 0.25 mg weekly and increasing every 4 weeks. Rushing titration is the fastest path to intolerable side effects. Learn more in our guide to taking GLP-1 safely.
Step 5: Pair With Lifestyle Changes
GLP-1s are most effective when combined with a low-glycemic, anti-inflammatory diet and regular exercise. The medication handles the appetite and insulin signaling. You handle the food quality and movement. This combination is more powerful than either alone.
Step 6: Monitor and Follow Up
Recheck labs at 3 and 6 months. Track your symptoms: period regularity, acne, energy levels, weight. If something's not working or side effects persist, your provider can adjust the dose or try a different medication.
MEDVI
Both semaglutide & tirzepatide available
How We Researched This Guide
This article is based on our review of:
- The 2023 International Evidence-Based Guideline for the Assessment and Management of PCOS (Teede et al., Monash University; endorsed by 39 medical organizations)
- 8+ PCOS-specific clinical trials and 3 meta-analyses from PubMed, PMC, ScienceDirect, and Oxford Academic
- FDA prescribing information for Wegovy (semaglutide), Zepbound (tirzepatide), and Saxenda (liraglutide)
- FDA safety communications and warning letters regarding compounded GLP-1 products (updated through February 2026)
- Active clinical trial registries at ClinicalTrials.gov for ongoing PCOS-GLP-1 research
- Patient experiences from PCOS community forums and clinician-reported outcomes
We update this article when new clinical trial results are published, when FDA status changes, or when significant pricing or access changes occur. All clinical claims are cited to their primary source.
We are not doctors. This is health information, not medical advice. Always consult a licensed healthcare provider before starting, stopping, or changing any medication. Read our editorial standards for more details.
Frequently Asked Questions About GLP-1 and PCOS
Are GLP-1s FDA-approved for PCOS?
No. As of February 2026, no GLP-1 medication is FDA-approved specifically for PCOS. However, several are approved for type 2 diabetes (Ozempic, Mounjaro, Victoza) and/or obesity (Wegovy, Zepbound, Saxenda), and doctors can prescribe them off-label for PCOS. The 2023 International PCOS Guideline says they "could be considered" for weight management in adults with PCOS. Multiple clinical trials specifically studying GLP-1s for PCOS are currently underway.
How do GLP-1s help PCOS specifically?
GLP-1s address the metabolic root of PCOS — insulin resistance — by improving insulin sensitivity, promoting significant weight loss, and reducing appetite. This cascade reduces excess androgen (testosterone) production by the ovaries, which in turn can improve menstrual regularity, reduce acne and excess hair growth, and potentially improve fertility. They also reduce chronic inflammation and cardiovascular risk factors elevated in PCOS. Evidence suggests they may have direct effects on reproductive hormones beyond what weight loss alone explains.
Which GLP-1 is best for PCOS?
There is no definitive "best" — no head-to-head PCOS trials have been done. Liraglutide has the most PCOS-specific research. Semaglutide is the most prescribed and accessible, with an oral option available. Tirzepatide produces the most weight loss overall. Your best choice depends on your symptoms, budget, and pregnancy plans.
Can you take GLP-1s and metformin together for PCOS?
Yes. Several studies show combining GLP-1 RAs with metformin produces better outcomes than either alone for PCOS — including a 64% prediabetes remission rate for the combination versus 32% for metformin alone. The risk of hypoglycemia with this combination is low. Many providers now use this approach.
Can GLP-1s help with PCOS fertility?
Indirectly, yes. By improving insulin resistance and promoting weight loss, GLP-1s can help restore regular ovulation. However, GLP-1s are not recommended during pregnancy. Semaglutide (Wegovy) should be stopped at least 2 months before planned pregnancy. For tirzepatide, labeling advises discontinuation when pregnancy is recognized — discuss timing with your clinician. The 2023 PCOS guideline states that anti-obesity agents for reproductive outcomes should be used only in research settings.
How long does it take for GLP-1s to work for PCOS?
Most women notice appetite changes within the first 1–2 weeks. Initial weight loss typically begins within the first month. Menstrual regularity improvements usually appear within 3–6 months. Testosterone reduction and improvements in acne or excess hair growth may take 3–6 months or longer. Full metabolic benefits generally require at least 6 months of consistent use.
Do GLP-1s work for lean PCOS?
There is currently no clinical evidence supporting GLP-1 use in lean PCOS (BMI under 25) without metabolic features like insulin resistance. GLP-1s target metabolic dysfunction — if you don't have it, there's no mechanism for them to address. Discuss alternatives like inositol, metformin, or hormonal management with your doctor.
Do GLP-1s cause hair loss?
GLP-1s themselves don't directly cause hair loss. However, rapid weight loss from any cause can trigger telogen effluvium — a temporary form of excessive shedding that usually resolves within 6–12 months. If you already have PCOS-related hair thinning, monitor carefully and ensure adequate protein and nutrient intake. Work with your provider if shedding increases significantly.
Is compounded semaglutide safe?
It depends entirely on the source. The FDA has identified fraudulent compounded products with fake pharmacy labels, "animal grade" ingredients, and dosing that caused hospitalizations. Compounded drugs are not FDA-approved and do not undergo FDA review for safety, quality, or effectiveness. If you use a compounded product, verify the pharmacy's state license, confirm the product is legitimately compounded to a valid prescription, and follow dosing instructions carefully.
Why do people get pregnant on Ozempic?
Weight loss and improved insulin sensitivity can restore ovulation in women with PCOS who weren't ovulating before. This means pregnancy becomes possible — sometimes before the woman realizes her cycles have returned. This is why the 2023 PCOS guideline recommends effective contraception when using GLP-1s in women of reproductive age. If you don't want to become pregnant, use contraception while on a GLP-1.
Does Zepbound (tirzepatide) affect birth control pills?
Yes. The Zepbound prescribing information (FDA) advises patients on oral hormonal contraceptives to switch to a non-oral method, or add a barrier method (such as condoms), for 4 weeks after starting tirzepatide and for 4 weeks after each dose escalation. This applies to Mounjaro as well, since both contain tirzepatide. This is a detail most articles about PCOS and GLP-1s don't mention — but it's critical if you're relying on the pill for contraception.
Will I gain the weight back if I stop?
Most people do regain significant weight within about a year of stopping, though the amount varies. More than half of patients in some studies maintained their weight loss at one year. The biggest factor is whether you've built sustainable lifestyle habits during treatment. Transitioning to metformin after stopping a GLP-1 may help minimize regain. Many obesity medicine specialists now view GLP-1s as appropriate for long-term use in chronic metabolic conditions.
How much do GLP-1s cost for PCOS?
Brand-name GLP-1s cost $900–$1,400/month without insurance. Telehealth providers offering compounded or subscription models typically range from $99–$399/month. Insurance coverage varies — you're more likely to get coverage if you also have an obesity diagnosis (BMI ≥30) or type 2 diabetes.
What labs should I check before starting a GLP-1 for PCOS?
At minimum: fasting insulin, fasting glucose, HOMA-IR, A1C, total and free testosterone, DHEA-S, lipid panel, thyroid panel, liver function tests, vitamin D, and B12. These give your provider a baseline and help confirm you're a good candidate. Recheck at 3 and 6 months to track improvement.
Can GLP-1s cure PCOS?
No. There is no cure for PCOS. GLP-1s can significantly improve the metabolic and hormonal symptoms, but they manage the condition rather than eliminate it. Most benefits require ongoing treatment or firmly established lifestyle changes to maintain.
What supplements work alongside GLP-1s for PCOS?
Inositol (myo-inositol + D-chiro-inositol in a 40:1 ratio) is the most studied supplement for PCOS insulin resistance and may complement GLP-1 therapy. Vitamin D is commonly deficient in PCOS and worth supplementing if levels are low. Omega-3 fatty acids may help with inflammation. Always discuss supplements with your provider — especially when taking prescription medications — to avoid interactions and ensure they're appropriate for your specific situation.
Can I take Ozempic while breastfeeding with PCOS?
There is insufficient data on GLP-1 medications during breastfeeding. Most manufacturers and clinical guidelines recommend against their use while nursing. Discuss with your healthcare provider to weigh the risks and benefits for your specific situation. Metformin is generally considered compatible with breastfeeding if you need metabolic support during this period.
What's the difference between Ozempic and Wegovy for PCOS?
Ozempic and Wegovy both contain semaglutide — the same active ingredient. The difference is the FDA-approved indication and dosing range. Ozempic is approved for type 2 diabetes (maximum dose 2mg weekly). Wegovy is approved for chronic weight management (maximum dose 2.4mg weekly). For PCOS, your doctor might prescribe either depending on your diagnoses and insurance coverage. Functionally, they work the same way in your body.
How is Mounjaro different from Ozempic for PCOS?
Mounjaro (tirzepatide) is a dual-action medication that activates both GLP-1 and GIP receptors, while Ozempic (semaglutide) activates only GLP-1 receptors. In clinical trials for obesity, tirzepatide produced higher average weight loss than semaglutide. However, tirzepatide has less PCOS-specific research, and it may reduce the effectiveness of oral contraceptive pills — a critical consideration for PCOS women relying on the pill for contraception or cycle management. Both are prescribed off-label for PCOS.
What to Do Next
You now have an evidence-based overview of what clinical studies and guidelines currently say about GLP-1 medications and PCOS. Here's where you go from here.
If you're ready to explore GLP-1 providers: We've verified pricing, medication sources, prescriber credentials, and support options across 15+ telehealth platforms that serve women with PCOS.
If you want to talk to your own doctor first: Bring this article. Print the decision framework. Get baseline labs. Use the scripts above.
If you're not sure yet: That's completely fine. Bookmark this page. We update it when new research drops or FDA status changes. You'll know when you're ready.
MEDVI
Verified pricing, updated monthly
Related Guides
- Best GLP-1 Providers for PCOS (Verified Comparison)
- Semaglutide vs. Tirzepatide: Complete Comparison
- GLP-1 Plateau: Why It's Not Working Anymore + Fix Plan
- What Is GLP-1? Complete Guide
- What Is Semaglutide?
- What Is Tirzepatide?
- Is Compounded Semaglutide Safe?
- How to Take GLP-1 Safely
- Best GLP-1 Telehealth Providers (2026)
- Cons of GLP-1 Medications
This article is part of our GLP-1 and PCOS resource library at WeightLossProviderGuide.com. We exist to help you make informed decisions about GLP-1 medications with verified information, honest assessments, and transparent pricing.
Medical Disclaimer: This content is for informational purposes only and does not constitute medical advice. Always consult a licensed healthcare provider before starting, stopping, or changing any medication. GLP-1 medications are prescription drugs with potential risks and side effects.