How to Start GLP-1 for Weight Loss: Step-by-Step Guide
Disclosure: Some links on this site are affiliate links. If you purchase through these links, we may earn a commission at no extra cost to you. Thank you for supporting our site.·For informational purposes only—not medical advice.
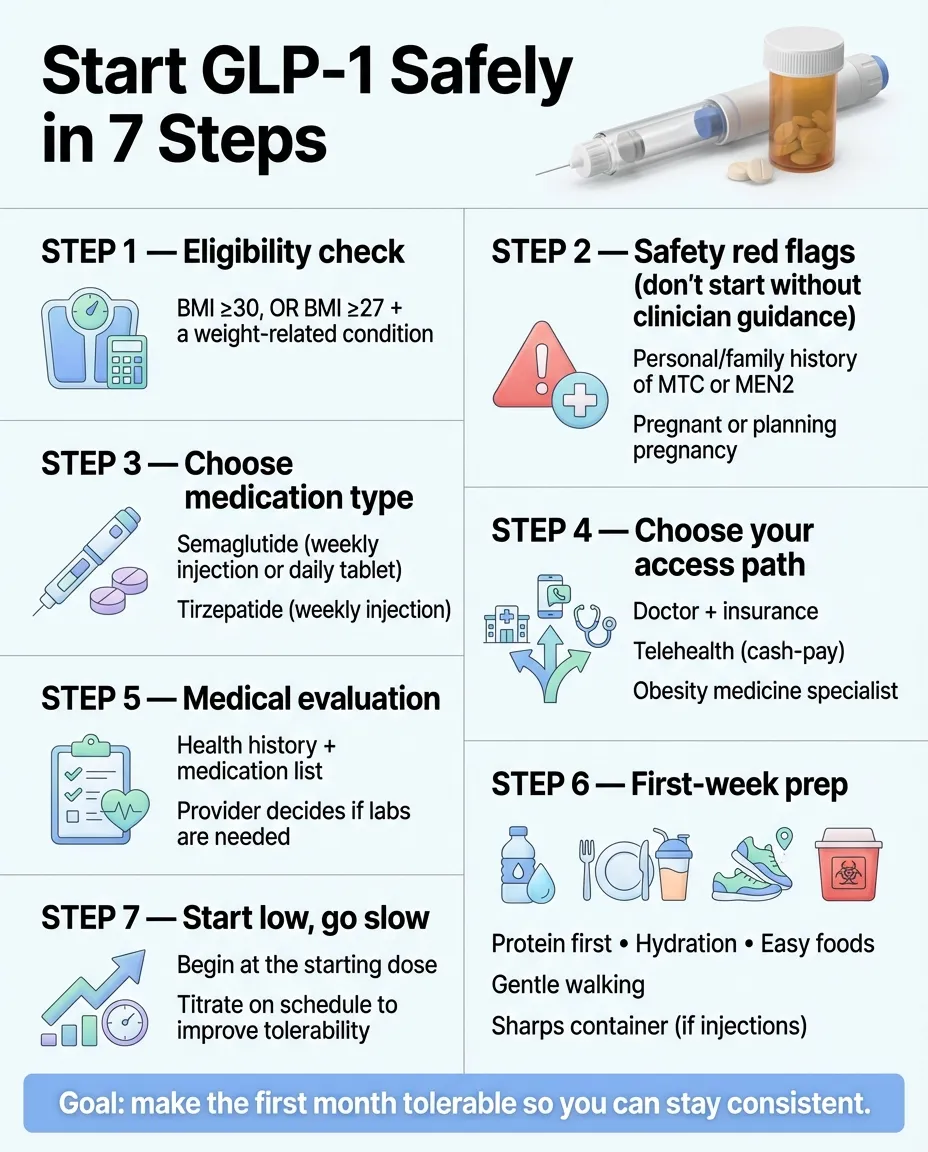
Here’s how to start GLP-1 for weight loss: confirm you’re eligible (BMI ≥30, or ≥27 with a condition like high blood pressure, high cholesterol, or type 2 diabetes), choose your access path (your doctor, a vetted telehealth provider, or insurance), complete a medical evaluation, get prescribed, then start at the lowest dose and follow a simple first-week plan. Most people can go from “thinking about it” to first dose in hand within a week — sometimes faster.
If you’ve been sitting on 14 open browser tabs researching this for days (or weeks), we built this guide to replace all of them. We’ll walk you through eligibility, which medication to choose, exactly what the first month feels like, side effects and how to handle them, real costs with no spin, and the fastest safe ways to get started — including telehealth options like MEDVi that let you start from home for $179.
One thing we won’t do: pretend this is all sunshine. The first 2–4 weeks can be rough, and about half of people stop GLP-1 within the first year — often because of side effects, cost, or lack of support (Yale Medicine). But the people who prepare, start slow, and have real clinical support? They see results that no diet has ever given them. This guide is designed to put you in that group.
Your GLP-1 Start Plan at a Glance
| Step | What You Do | Time It Takes |
|---|---|---|
| 1. Check eligibility | BMI ≥30 (or ≥27 + health condition). No history of MTC or MEN2. If you’ve had pancreatitis, discuss with your clinician first. | 2 minutes |
| 2. Pick your medication | Semaglutide (Wegovy) or tirzepatide (Zepbound) — both work. Your provider helps decide. | Part of your consult |
| 3. Choose your path | Doctor/insurance, telehealth (cash-pay), or obesity specialist | 10 minutes of research |
| 4. Complete medical eval | Health history, medications, goals. Some paths require labs. | 15–30 minutes |
| 5. Get prescribed + shipped | Provider reviews, writes Rx, medication delivered or picked up | 1–5 days |
| 6. Prep your body | Protein up, hydration up, stock easy foods, clear your schedule for dose day | 3–7 days before |
| 7. Start low, go slow | First injection at the lowest dose. Follow the first-week playbook below. | Week 1 begins |
What Is GLP-1 and Why Does It Work So Well?
GLP-1 stands for glucagon-like peptide-1. It’s a hormone your gut releases after you eat, and it tells your brain you’re full, slows your digestion, and helps regulate blood sugar. GLP-1 medications — technically called GLP-1 receptor agonists — work by mimicking that natural hormone, but at levels far higher than your body produces on its own.
The result: your appetite quiets down. The constant mental chatter about food (what doctors call “food noise”) fades. You feel satisfied with smaller portions. And because you’re eating less without white-knuckling it, you lose weight — steadily, and for many people, significantly.
This isn’t a stimulant. It’s not an appetite suppressant in the old-school sense. It works with your biology, not against it.
The clinical data is striking
- In the landmark STEP 1 trial, people on semaglutide 2.4 mg lost an average of 14.9% of their body weight over 68 weeks — vs. 2.4% with placebo (NEJM, 2021).
- The newer STEP UP trial showed semaglutide at 7.2 mg achieved 20.7% average weight loss over 72 weeks, with one-third of participants losing over 25% (Novo Nordisk, 2025).
- Tirzepatide (Zepbound) showed up to 22.5% weight loss at the highest dose in the SURMOUNT-1 trial (NEJM, 2022).
- The SELECT trial found semaglutide reduced the risk of heart attack, stroke, and cardiovascular death by 20% in people with obesity and heart disease (NEJM, 2023).
- Real-world data backs this up: patients using semaglutide 2.4 mg lost an average of 17.6% at 12 months (PMC, 2024).
The medications you’ll hear about
- Semaglutide — Wegovy (FDA-approved for weight loss), Ozempic (approved for diabetes, same drug), and the Wegovy tablet (oral semaglutide 25 mg, FDA-approved December 2025, launched January 2026). Weekly injection or daily tablet.
- Tirzepatide — Zepbound (weight loss), Mounjaro (diabetes). Weekly injection. Works on both GLP-1 and GIP receptors (dual action).
Both are legitimate, well-studied medications. We’ll help you understand which one makes more sense for you below.
If you’re looking for ways to increase GLP-1 naturally (through food, fiber, protein timing, etc.), that’s a different goal. This page focuses on GLP-1 medication for weight loss.
Step 1: Do You Qualify for GLP-1 Medication?
You probably do. Most adults with significant excess weight qualify.
The standard eligibility criteria (per FDA labeling)
- BMI ≥30 (obesity) — no additional conditions required, OR
- BMI ≥27 with at least one weight-related health condition. Per FDA labeling, examples include hypertension, dyslipidemia, and type 2 diabetes. Your clinician or insurer may also consider conditions like sleep apnea, PCOS, or pre-diabetes.
Quick BMI reference
| Height | Weight at ~BMI 30 | Weight at ~BMI 27 |
|---|---|---|
| 5’2” | 164 lbs | 148 lbs |
| 5’4” | 175 lbs | 157 lbs |
| 5’6” | 186 lbs | 167 lbs |
| 5’8” | 197 lbs | 177 lbs |
| 5’10” | 209 lbs | 188 lbs |
| 6’0” | 221 lbs | 199 lbs |
If you’re close to these numbers and have any of the conditions listed above, you likely qualify. Your provider makes the final determination — but the bar is lower than most people think.
Who Should NOT Start GLP-1 (Red Flags)
Per FDA prescribing information (Wegovy PI, Zepbound PI):
- Personal or family history of medullary thyroid carcinoma (MTC) or MEN2 — this is a hard contraindication.
- History of pancreatitis — not an automatic disqualifier, but requires careful discussion with your clinician.
- Pregnant, planning pregnancy soon, or breastfeeding — GLP-1 medications are not recommended. Stop at least 2 months before planned conception (semaglutide).
- Severe gastrointestinal conditions like gastroparesis (severely delayed stomach emptying).
- Currently on insulin or sulfonylureas — not a contraindication, but doses need adjustment to avoid dangerously low blood sugar.
Step 2: Which GLP-1 Should You Start? (Semaglutide vs. Tirzepatide)
Short answer: both work. Your provider will recommend one based on your health profile. Here’s what separates them.
| Semaglutide (Wegovy / Ozempic) | Tirzepatide (Zepbound / Mounjaro) | |
|---|---|---|
| Mechanism | GLP-1 receptor agonist | Dual GIP + GLP-1 agonist |
| FDA-approved for weight loss | Wegovy (injection), Wegovy tablet (oral) | Zepbound (injection) |
| How you take it | Weekly injection or daily tablet | Weekly injection |
| Average weight loss (trials) | 15–21% of body weight | 15–22.5% of body weight |
| Starting dose | 0.25 mg/week (injection) | 2.5 mg/week |
| Time to maintenance dose | ~16–20 weeks (injection) | Depends on target dose — 5 mg after 4 weeks; higher doses reached with ≥4 weeks per step |
| Availability | Widely available, including compounded versions | Available, some supply variability |
| Oral option? | Yes (Wegovy tablet, FDA-approved Dec 2025) | Not currently |
| Best for | People who want an oral option, broad availability, strong long-term data | People who want potentially higher weight loss, dual-mechanism approach |
Pick this if you’re…
- Needle-averse: Ask your provider about oral semaglutide (Wegovy tablet). It’s the first GLP-1 tablet approved for weight loss and showed 13.6% average weight loss at 64 weeks in the OASIS 4 trial. Take it daily on an empty stomach with no more than 4 oz of water, then wait 30 minutes before eating, drinking, or taking other medications.
- Focused on maximum weight loss: Tirzepatide edges out semaglutide slightly in head-to-head comparisons at the highest doses. But the difference matters less than consistency and adherence.
- Budget-conscious and going cash-pay: Compounded semaglutide is more widely available and typically cheaper through telehealth programs. Many providers (including MEDVi) offer both semaglutide and tirzepatide.
- Already taking diabetes medication: Tell your provider. They need to coordinate doses — particularly if you’re on insulin or sulfonylureas.
Our honest take:
Don’t overthink this decision. Both medications are effective and well-studied. The “best” GLP-1 is the one you can access, afford, and stick with consistently. Talk to your provider, pick one, and start.
What about Ozempic, Mounjaro, Rybelsus, and Saxenda? Ozempic and Mounjaro are FDA-approved for type 2 diabetes (not weight loss), though they contain the same active ingredients as Wegovy and Zepbound. Doctors sometimes prescribe them off-label for weight. Rybelsus is an older oral semaglutide (lower dose, smaller effect). Saxenda (liraglutide) is a daily injection with more modest weight loss. For most people starting in 2026, Wegovy/Zepbound (or their compounded equivalents) are the primary options. Read our semaglutide vs tirzepatide comparison for a detailed breakdown.
Step 3: How to Choose Your Provider Path (Doctor vs. Telehealth vs. Insurance)
This is where most people stall. There are three realistic paths to get GLP-1 prescribed. Each has tradeoffs in speed, cost, and safety.
| Your Doctor + Insurance | Vetted Telehealth (Cash-Pay) | Obesity Medicine Specialist | |
|---|---|---|---|
| Best for | People whose insurance covers Wegovy/Zepbound | People who want to start fast, no insurance coverage | People who want in-depth, in-person care |
| Speed to first dose | 2–8 weeks (scheduling, labs, prior auth) | 2–5 days (online eval → medication shipped) | 1–4 weeks |
| Typical monthly cost | $0–$50 copay if approved; $1,000+ if denied | $179–$399/month all-in (compounded) | Copay + medication cost (varies) |
| Medication type | Brand-name FDA-approved | Compounded semaglutide/tirzepatide (most common) | Brand-name or compounded |
| Support level | Varies (often limited follow-up) | 24/7 messaging + unlimited visits (MEDVi) | Typically strong, multidisciplinary |
| Main downside | Prior auth delays, denials common | Compounded meds are NOT FDA-approved products | Scheduling, availability, may not accept all insurance |
One path you should NEVER take
Do not buy GLP-1 from sites that don’t require a prescription, sell “research peptides,” or offer “compounded semaglutide” without a legitimate medical evaluation. The FDA has issued multiple warnings about unapproved GLP-1 products associated with dosing errors, contamination, and hospitalizations. If a site doesn’t require your medical history and a licensed prescriber’s review, walk away.
If you’re choosing telehealth: what “good care” actually looks like
- A real medical screening (health history, medication list, not just “enter your credit card”)
- A named, licensed prescriber who reviews your case
- A named pharmacy partner (not “our proprietary blend”)
- Clear pricing — what does month 1 cost? What do refills cost? Are consults extra?
- Cancellation policy transparency — can you stop anytime?
- Follow-up support — can you message a provider about side effects?
- LegitScript certification — you can verify any provider’s website here
We evaluated dozens of telehealth GLP-1 providers against these criteria. For a fast, affordable start with strong support, MEDVi consistently scores highest on our evaluation — $179 first month (medication included), 24/7 provider access, LegitScript certified, and pharmacy partners you can actually verify (Belmar Pharma Solutions, Beluga Health). They’re available in 49 states and offer both injectable and oral tablet options.
MEDVi isn’t the only good option — Eden offers predictable flat pricing, and BreezeMeds serves all 50 states. But for most people who want a reliable, well-supported start without weeks of insurance runaround, MEDVi is where we’d point you. See our full provider comparison for the complete analysis.
Affiliate disclosure: We earn a commission if you sign up through our links. We recommend MEDVi because it meets our evaluation criteria — not because of the commission.
MEDVi
$179 first month — medication, provider access & shipping included
Compounded vs. brand-name: the distinction you need to understand
- Brand-name (Wegovy, Zepbound): FDA-approved products with standardized manufacturing. The clinical trial data is based on these. Gold standard for regulatory certainty.
- Compounded: Custom-prepared by licensed compounding pharmacies. The final product is NOT FDA-approved. The FDA has warned that some products marketed as “compounded semaglutide” may use different salt forms that are not the same active ingredient. More affordable — which is why most telehealth programs use them.
Our take: If you go compounded, the pharmacy and provider matter enormously. Ask your provider which pharmacy fulfills your prescription, and verify it’s a licensed 503A or 503B facility. Programs that name their pharmacy partners (and are LegitScript certified) are safer bets. Read our compounded semaglutide safety guide for the full analysis.
Step 4: How to Prepare Your Body Before Your First Dose
You don’t need to overhaul your life. But 5–7 days of simple prep makes your first weeks significantly easier — less nausea, less fatigue, less constipation. These aren’t random tips. They’re based on what obesity medicine dietitians and clinicians consistently recommend (Ohio State University, UCHealth).
The GLP-1 Readiness Checklist
Start eating protein first, every meal.
Aim for 25–30 grams per meal. GLP-1 crushes your appetite — if you’re not already prioritizing protein, you’ll lose muscle along with fat. Chicken, fish, eggs, Greek yogurt, cottage cheese, lean beef, tofu.
Increase fiber gradually.
Target 25 grams/day. Start now, not after your first dose — a sudden fiber increase on top of slowed digestion is a recipe for misery.
Build a hydration habit.
GLP-1 suppresses thirst alongside hunger. Goal: 80–100 ounces daily. Get a large water bottle and keep it where you can see it.
Start walking.
20–30 minutes daily. Walking helps with GI motility (less constipation), mood, and establishing the exercise habit before medication changes your appetite.
Begin basic strength training.
Even bodyweight exercises 2–3 times per week helps preserve muscle mass during weight loss. This is the single most important thing most new GLP-1 users skip.
Clear your schedule for injection day.
Take your first dose on a weekend or a day you can rest. Most people feel fine, but if you’re in the 30–40% who get nausea, you’ll want a low-pressure day.
Stock your kitchen.
Easy-on-the-stomach foods for week 1: bananas, rice, plain toast, broth, crackers, ginger tea, ginger chews. Avoid stocking up on greasy, heavy, or spicy foods.
Get a sharps container.
For safe needle disposal after injections. Available at any pharmacy for a few dollars.
Step 5: Starting Dose and Titration (Why “Low and Slow” Is Non-Negotiable)
Every GLP-1 medication starts at a dose too low to produce significant weight loss. That’s by design. The starting dose is about teaching your body to tolerate the medication so you can eventually reach the therapeutic dose without unbearable side effects.
Do not skip doses. Do not jump ahead. Do not let impatience convince you to escalate faster than your provider prescribes.
Semaglutide (Wegovy) Titration Schedule
Per the FDA-approved prescribing information:
| Weeks | Dose | Purpose |
|---|---|---|
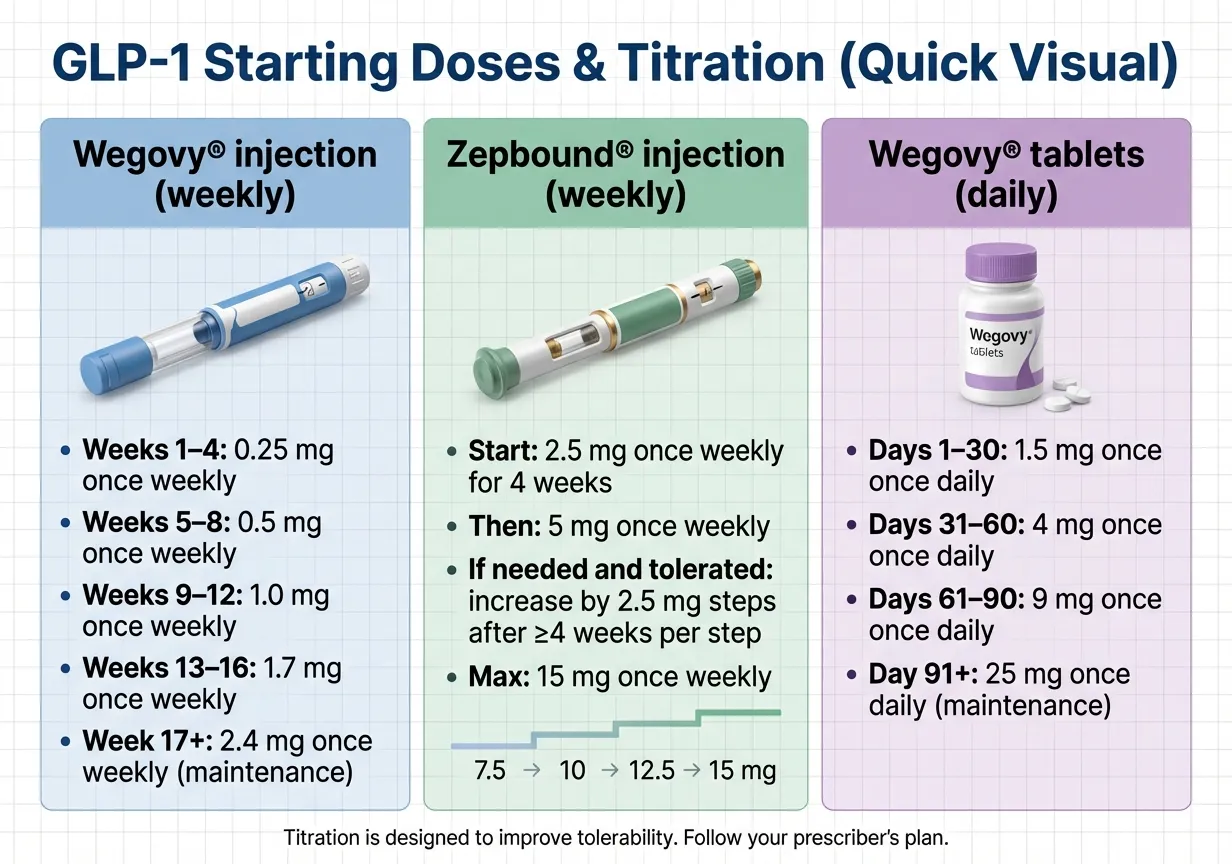
| 1–4 | 0.25 mg/week | Adjustment — minimal weight loss expected |
| 5–8 | 0.5 mg/week | Still titrating |
| 9–12 | 1.0 mg/week | Some weight loss begins |
| 13–16 | 1.7 mg/week | Approaching therapeutic range |
| 17+ | 2.4 mg/week | Maintenance / therapeutic dose |
Tirzepatide (Zepbound) Titration Schedule
| Weeks | Dose | Purpose |
|---|---|---|
| 1–4 | 2.5 mg/week | Adjustment |
| 5–8 | 5.0 mg/week | Dose increase #1 |
| 9–12 | 7.5 mg/week (optional) | May maintain at 5 mg if tolerating well |
| 13–16 | 10.0 mg/week | Continued titration |
| 17–20+ | 12.5–15 mg/week | Full therapeutic range (if needed) |
Your provider may slow the schedule if side effects are significant — and that’s the right call. Faster escalation = more nausea = higher chance of quitting. Patience during titration is what separates people who succeed long-term from people who stop after month two.
What if you miss a dose?
Semaglutide injection (per Wegovy label):
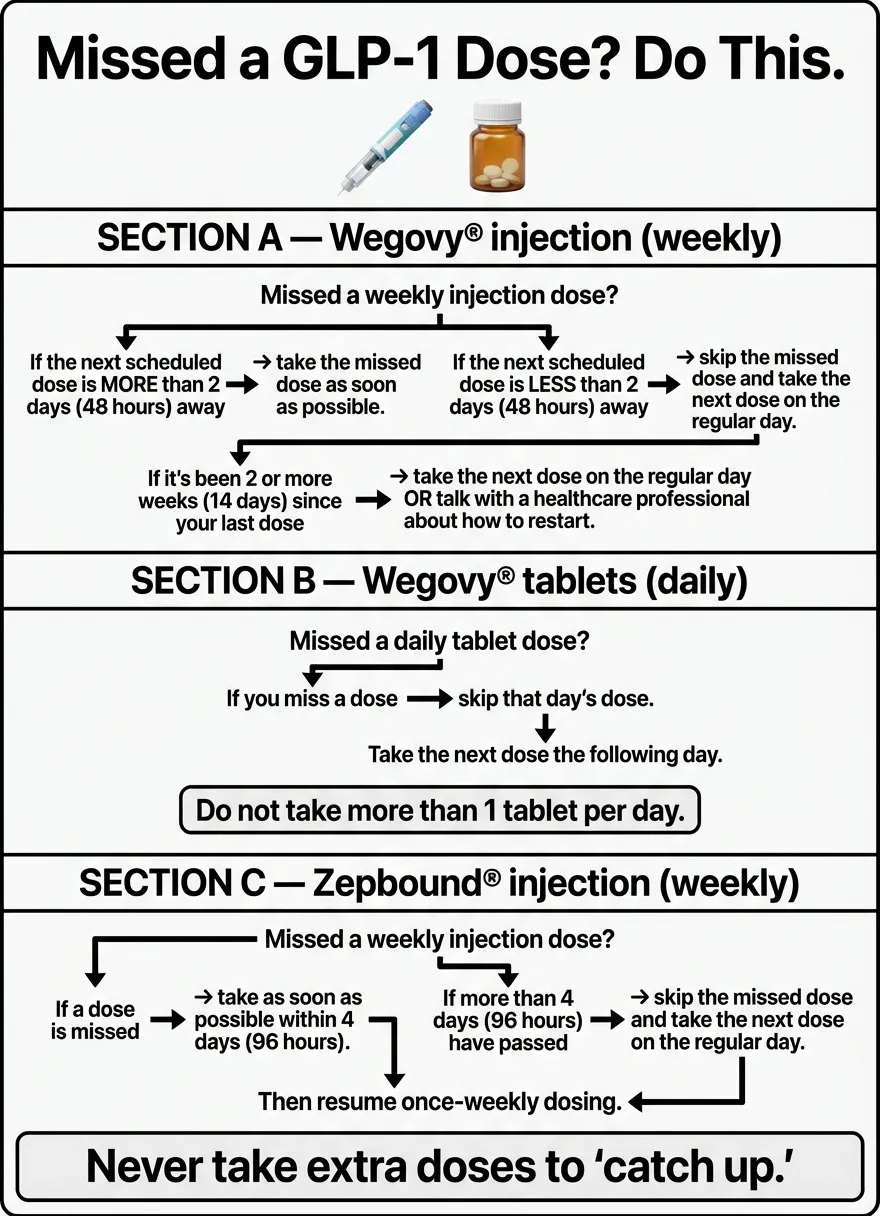
If you miss a dose and your next scheduled dose is more than 2 days away (48+ hours), take it as soon as you remember. If your next dose is 2 days or less away, skip the missed dose and resume on your regularly scheduled day. If you miss 2 or more consecutive doses, resume dosing as scheduled — or your provider may reinitiate dose escalation.
Semaglutide tablets (per Wegovy label):
If you miss a dose, skip it and take your next dose the following day. Do not take more than one tablet per day.
Tirzepatide (per Zepbound label):
If missed within 4 days of the scheduled day, take it as soon as possible. If more than 4 days late, skip and resume on the regular schedule.
What about “microdosing” GLP-1?
You’ll see this term online. It usually means staying on a very low dose long-term instead of titrating up. There’s no clinical evidence supporting this approach, and with compounded vials (vs. prefilled pens), the dosing-error risk is real. The FDA has specifically flagged dosing errors with compounded semaglutide. Only adjust doses under your provider’s direction.
Step 6: Your First GLP-1 Injection (It’s Easier Than You Think)
If the needle is what’s holding you back, here’s the truth: GLP-1 needles are tiny. They’re subcutaneous (just under the skin, into fat — not into a vein or muscle). Most people compare it to a quick pinch. After the second or third time, it becomes a 30-second routine.
Important: Devices differ
GLP-1 medications come in several device types: single-use prefilled pens, multi-dose pens, and vials with syringes. Each works differently. The steps below are general guidance — always follow the specific Instructions for Use (IFU) that come with your device and your prescriber’s instructions.
General injection steps (for most prefilled pens)
- Wash your hands.
- Choose your injection site: abdomen (at least 2 inches from your belly button), outer thigh, or upper arm. Rotate sites each week.
- Clean the area with an alcohol swab. Let it dry.
- Prepare the pen per your device’s IFU (some require needle attachment and dose dialing; others are preset).
- Pinch a fold of skin. Insert the needle subcutaneously per your IFU directions.
- Inject the dose. Hold for the time specified in your IFU (typically 5–10 seconds).
- Remove the needle. Don’t rub the site.
- Dispose of the needle in a sharps container. Never reuse.
If you’re using a compounded vial + syringe
This requires more care. You’re drawing medication from a vial with an insulin syringe, and dosing errors are the biggest risk. Never guess on the amount. Your pharmacy should provide specific instructions for your concentration and prescribed dose. If anything is unclear — call them before injecting.
- Confirm the concentration (mg/mL) with your provider and pharmacy
- Use the correct syringe type (insulin syringes, typically)
- Clean the vial top with alcohol before each draw
- Store properly — refrigerate per instructions
Needle-free option
If injections are truly a dealbreaker, ask your provider about oral semaglutide (Wegovy tablets, FDA-approved December 2025). It’s a once-daily tablet swallowed whole on an empty stomach with no more than 4 oz of water — wait 30 minutes before eating, drinking, or taking other oral medications. In the OASIS 4 trial, it showed 13.6% mean weight loss at 64 weeks (NEJM, 2025). Read our oral vs injectable semaglutide comparison for more details.
What to Expect: Your First Week on GLP-1
Your first week is about adjustment, not dramatic results. Here’s what’s actually going to happen.
Day 1–2: Injection Day and After
You took the dose. Now what? You might feel nothing at all — many people don’t notice anything the first day. Or you might feel:
- Mild nausea (usually 4–8 hours after injection)
- A subtle sense of fullness, even without eating much
- Slight fatigue or a “foggy” feeling
Eat small, bland meals. Drink water. Don’t test the medication with a large dinner out. Keep it boring and easy.
Day 3–4: The Appetite Shift
This is when most people first notice the medication working. The food noise gets quieter. You look at a plate of food and feel satisfied with half of it. You forget to think about snacking.
Important: you still need to eat. Don’t skip meals because you’re not hungry. Eat for nutrition — especially protein. A protein shake is a good safety net on low-appetite days.
Day 5–7: Settling In
Side effects (if you had them) typically peak around day 2–3 and start improving by day 5. Constipation may show up around now — this is where your prep (hydration + fiber + walking) pays off.
Weight change in week 1 is mostly water and reduced food volume. Expect 1–3 lbs. Don’t obsess. Weekly weigh-ins are more useful than daily.

What to Expect: Your First 30 Days on GLP-1
Week 1–2: The Adjustment Phase
You’re on the lowest dose. This isn’t the “weight loss dose” — it’s the “get your body used to it” dose. Side effects are most likely during this window: nausea, constipation, maybe some fatigue or headache. Don’t be discouraged by slow weight loss.
Week 3–4: Building Momentum
Appetite suppression becomes more consistent. Behavioral changes emerge naturally — smaller portions feel normal, cravings weaken, snacking drops. Many people report 4–8 lbs lost by end of month 1 (varies widely by starting weight and individual biology).
Energy often improves as your body adapts. Some people describe a sense of calm around food they’ve never experienced before. That’s the “food noise” turning off.
At the 4-week mark, your provider will typically discuss the first dose increase. The titration continues — and with each step up, the appetite effects strengthen.
What real users say about their first month
“My weight has been a constantly increasing problem until I found Medvi. My cholesterol and blood pressure were too high. My A1C was still in the prediabetic range.” — ConsumerAffairs review, Oct 2025
“Everyone seems to be extremely supportive and that’s so important when it comes to weight loss. No judgments — they just want me to get to a healthy me.” — Trustpilot review, Feb 2026
“I was pre-diabetic with high cholesterol when my doctor suggested [GLP-1 medication]. In less than a year, I’ve lost 92 pounds, and my A1C is back in the normal range. I no longer need blood pressure medication.” — Patient testimonial
Individual results vary. Testimonials are not guarantees of outcomes.
GLP-1 Side Effects: What’s Normal, What’s Fixable, and When to Call Your Doctor
Let’s be direct: side effects are real. The most common ones are gastrointestinal, and they tend to show up during the first few weeks and during dose increases. For most people, they’re manageable and temporary. For a smaller number, they’re the reason they stop.
Common Side Effects and How to Handle Them
| Side Effect | How Common | What to Do | When It Improves |
|---|---|---|---|
| Nausea | Very common (~40% early on) | Eat small, frequent meals. Avoid greasy food. Ginger tea/ginger chews. Eat slowly. | 1–3 weeks after each dose level |
| Constipation | Common (20–30%) | 80+ oz water daily. 25g fiber/day. Walk 30 min/day. Miralax if needed. | 2–4 weeks |
| Diarrhea | Less common | Stay hydrated. BRAT diet. Contact provider if persistent. | 1–2 weeks |
| Fatigue | Common early | Rest. Hydrate. Make sure you’re eating enough calories and protein. | 1–2 weeks |
| Headache | Less common | Hydration first. OTC pain relief. Usually linked to not drinking enough. | Days |
| Reflux/heartburn | Occasional | Avoid eating close to bedtime. Smaller meals. Elevate head when sleeping. | Varies |
| Injection site reaction | Uncommon | Rotate sites. Use room-temp medication. | Usually mild and brief |
When to Call Your Provider Immediately
These are not “wait and see” situations:
- Severe, persistent vomiting — can’t keep fluids down for 24+ hours
- Severe abdominal pain — especially if it radiates to your back (possible pancreatitis)
- Signs of dehydration — dark urine, dizziness, rapid heart rate, not urinating
- Allergic reaction — swelling of face/throat, difficulty breathing, severe rash
- Gallbladder symptoms — sharp pain in upper right abdomen after eating
The Honest Numbers on Quitting
Here’s the uncomfortable stat: about half of people stop GLP-1 within the first year. The biggest reasons are side effects, cost, and insufficient follow-up support (SteadyMD, 2024).
The people who succeed long-term tend to have three things in common:
- They started with a provider who offers real follow-up (not a one-and-done prescription).
- They expected the first 2–4 weeks to be an adjustment period — not instant results.
- They built the habits (protein, hydration, movement) that make the medication work best.
That’s exactly what this guide is designed to set you up for. For a deeper dive, see our complete guide to GLP-1 pros and cons.
What to Eat on GLP-1 (The Practical Diet Guide)
You don’t need a special diet plan. But what you eat matters more on GLP-1 — because you’re eating less, every bite carries more weight for nutrition, muscle preservation, and side-effect management.
The 3 Rules (Keep It Simple)
Protein first, every meal.
Aim for 25–30 grams per meal, 80–100 grams per day minimum. Without adequate protein, a significant portion of your weight loss is muscle — which tanks your metabolism, strength, and energy.
Fiber for function.
25 grams daily. This prevents constipation (the most persistent side effect) and keeps your gut moving. Fruits, vegetables, beans, lentils, oats, chia seeds.
Hydrate relentlessly.
80–100 ounces of water per day. GLP-1 suppresses your thirst along with your hunger. You won’t feel thirsty, but your body still needs the fluid.
Foods That Work Well on GLP-1
- Lean proteins: chicken, fish, eggs, cottage cheese, Greek yogurt
- Non-starchy vegetables: broccoli, spinach, bell peppers, zucchini, asparagus
- Complex carbs (moderate): sweet potato, quinoa, brown rice, oats
- Healthy fats (small portions): avocado, olive oil, nuts, seeds
- Comfort foods for nausea days: ginger tea, bone broth, bananas, plain crackers, toast
- Protein shakes: your safety net when appetite is very low
Foods That Make Side Effects Worse (Especially Early On)
- Greasy and fried foods — the single biggest nausea trigger on GLP-1
- Large portions — your stomach is processing food more slowly
- Sugary drinks and processed sweets — empty calories when every calorie counts
- Alcohol — worsens nausea, adds empty calories, impairs blood sugar regulation
- Spicy food — can worsen reflux and nausea, particularly in the first 2–4 weeks
A Simple Eating Pattern That Works
Think of your plate in thirds: one-third protein, one-third vegetables, one-third complex carb or healthy fat. Eat 3 small meals and 1–2 protein-rich snacks. Eat slowly — put the fork down between bites. Stop when you’re satisfied, not stuffed. On days when you have zero appetite, at minimum have a protein shake and some fruit.
Exercise on GLP-1: What Actually Matters
Exercise isn’t optional. It’s what separates people who lose fat and keep muscle from people who lose both.
The Two Non-Negotiables
Walking: 150 minutes per week.
That’s 30 minutes, 5 days a week. Walking improves GI motility, boosts mood, supports cardiovascular health, and establishes the baseline activity habit. You don’t need a gym membership. You need shoes and a door.
Resistance training: 2–3 sessions per week.
This is the most important thing most GLP-1 users skip. Resistance training protects your muscle mass, which protects your metabolism, which protects your long-term results. Bodyweight exercises count. Resistance bands count. Light dumbbells count.
A Simple Starter Plan
- Weeks 1–2: 15–20 minute walks daily. Get the habit started while your body adjusts.
- Weeks 3–4: 30-minute walks + 2 bodyweight sessions per week (squats, push-ups, lunges, planks, resistance band rows).
- Month 2+: Build from there. Increase walking duration or intensity. Add weight to your resistance exercises.
How Much Does GLP-1 Actually Cost? (Real Numbers, No Spin)
Cost is one of the top reasons people either don’t start or stop early. Here’s the full picture.
| Path | Monthly Cost | What’s Included | Notes |
|---|---|---|---|
| Brand-name list price | ~$1,350/month | Medication only | This is the sticker price. Almost nobody pays this. |
| Wegovy self-pay (NovoCare) | $149–$299/mo (tablet) or $199–$349/mo (injection) | Medication + home delivery | Dose-dependent pricing. Government beneficiaries excluded. (Wegovy cost info) |
| Zepbound self-pay | $299–$699/month | Medication | Vial and KwikPen options at different price points. (Zepbound savings) |
| Brand-name with insurance + savings card | As low as $25/month | Medication | Requires prior authorization. Government beneficiaries excluded. |
| MEDVi (compounded telehealth) | $179 first month, $299/mo ongoing | Medication + physician review + 24/7 support + shipping | No insurance needed. No hidden fees. |
| Other telehealth (compounded) | $200–$500/month | Varies widely | Check what’s actually included. Some charge separately for consults, shipping, or dose increases. |
The cost reality most people land on
If your insurance covers Wegovy or Zepbound with a low copay — that’s the cheapest path and uses FDA-approved products. Pursue it. If insurance denies you or you don’t have coverage, you now have two realistic options: brand-name self-pay programs from the manufacturers (NovoCare Pharmacy for Wegovy, Lilly’s program for Zepbound) or compounded telehealth programs. Read our complete GLP-1 cost guide for the full breakdown.
Watch out for bait-and-switch pricing
Some telehealth providers advertise a low starting price but charge more as your dose increases. Others charge separately for consultations, follow-ups, or shipping. Always ask: “What is my total monthly cost at the maintenance dose, including everything?” before you sign up.
The insurance prior authorization playbook
- Your provider submits a prior authorization request documenting your BMI, comorbidities, and prior weight loss attempts.
- Insurance reviews (this takes days to weeks).
- If approved: great, fill the prescription.
- If denied: appeal. Include documentation of prior failed diet/exercise programs and a letter of medical necessity.
- If the appeal fails: consider a manufacturer savings card, or switch to a cash-pay telehealth path.
Many people run the insurance process in parallel with telehealth — start cash-pay to avoid waiting, then switch to insurance if approval comes through.
How Long Does It Take to Lose Weight on GLP-1?
The honest answer: faster than any diet, but not overnight.
| Timeframe | What Typically Happens |
|---|---|
| Week 1–4 | Appetite decreases. Food noise quiets. 2–6 lbs lost (mostly water/food volume reduction). |
| Month 2–3 | Steady fat loss begins. Average ~5–10% of starting weight lost by month 3. Clothes fit differently. |
| Month 4–6 | Weight loss continues. Average ~10–15% of starting weight lost. Blood pressure, cholesterol, A1C may improve. |
| Month 6–12 | Approaching peak results. STEP 1 trial showed ~15% average loss at 68 weeks. Some people lose 20%+. |
| Month 12+ | Weight loss plateaus for most. Shift to maintenance. Dose may stay the same or be adjusted. |
Clinical reference: Patients on semaglutide 2.4 mg lost an average of 6% by week 12, 12% by week 28, and 14.9% by week 68 in the STEP 1 trial. Real-world data shows 17.6% at 12 months with consistent use (PMC, 2024).
Plateaus Happen. Here’s What to Do.
- Check protein intake. Are you consistently hitting 80–100 grams per day?
- Check hydration. Dehydration slows everything.
- Add or increase strength training. Muscle burns more calories at rest.
- Look at sleep. Poor sleep tanks hormones that regulate hunger and metabolism.
- Talk to your provider. A dose adjustment may be appropriate.
For a deeper dive on plateaus, see our GLP-1 plateau guide with the 7-step fix plan.
What Happens If You Stop Taking GLP-1?
We’re not going to soft-pedal this: weight regain after stopping is common and well-documented. The STEP 4 trial found that participants who switched from semaglutide to placebo regained about two-thirds of their lost weight within a year (JAMA, 2021).
This isn’t a failure of willpower. Obesity is a chronic condition driven by hormonal and neurological signals. When you remove the medication correcting those signals, the signals return.
What this means practically
- GLP-1 is increasingly viewed as a long-term or ongoing medication, not a “course of treatment” you finish.
- Some people successfully transition to a lower maintenance dose after reaching their goal.
- The lifestyle habits you build while on GLP-1 are your insurance policy.
The empowering reframe:
GLP-1 gives you a window. During that window, you have the clearest head around food you’ve ever had. Use it to build the habits, the routines, and the relationship with movement and nutrition that will serve you regardless of what happens with medication.
Read our complete guide on what happens when you stop GLP-1 for the full analysis.
Is GLP-1 Safe? What the Research Actually Shows
GLP-1 medications have been studied more rigorously than almost any weight-loss treatment in history. Here’s what the data says — sourced, not speculated.
- Semaglutide has been prescribed for type 2 diabetes since 2017 and for weight management since 2021 — millions of prescriptions worldwide.
- The STEP program (multiple large Phase 3 trials) consistently shows a safety profile where GI side effects are the main issue, and they’re typically mild-to-moderate (Frontiers in Endocrinology, 2022).
- The SELECT trial showed semaglutide reduced major adverse cardiovascular events by 20% in people with obesity and heart disease (NEJM, 2023).
- A 2025 Cochrane Review concluded that GLP-1 medications produce clinically meaningful weight loss, with GI adverse events as the primary concern (Cochrane, 2025).
- Serious adverse events (pancreatitis, gallbladder disease) are rare but documented. The FDA black box warning about medullary thyroid carcinoma is based on animal studies and has not been confirmed in humans.
The balanced view: No medication is risk-free. GLP-1s carry real (though mostly manageable) side effects and rare serious risks. For most people with obesity, the health risks of untreated obesity are significantly greater than the risks of GLP-1 treatment. Read our long-term effects of GLP-1 guide for the complete safety analysis.
How to Avoid GLP-1 Scams (Red Flags That Should Make You Walk Away)
As GLP-1 demand has exploded, so have sketchy providers and outright scams. The FDA has published specific warnings about unapproved products.
Red flags — if you see any of these, do not buy
- No prescription required. GLP-1 is a prescription medication. Period.
- “Research use only” or “not for human consumption” labels.
- No named prescriber. If you can’t find out who’s reviewing your health information, you’re not getting real medical care.
- No pharmacy disclosure. If they won’t tell you where your medication is made, that’s a problem.
- Prices too good to be true. If someone’s selling “semaglutide” for $50/month, ask what you’re actually getting.
- Guarantees of specific weight loss. No legitimate provider promises “lose 30 lbs in 30 days.”
- “Make GLP-1 at home” kits. Don’t. This is dangerous, unregulated, and illegal.
How to verify a provider
- Check their website on LegitScript’s verification tool.
- Look up the prescriber’s medical license in their state’s licensing database.
- Ask which pharmacy fills the prescription. Look up the pharmacy’s license.
- Check for real third-party reviews (Trustpilot, ConsumerAffairs, BBB — not just testimonials on their own site).
Our Evaluation Methodology (How We Built This Guide)
We believe you deserve to know how we formed our recommendations.
Sources we rely on
- FDA prescribing information (Wegovy, Zepbound) and FDA safety communications
- Published clinical trial data (STEP 1–5, STEP UP, SURMOUNT-1, SELECT, OASIS 4)
- Peer-reviewed journals (NEJM, JAMA, Cochrane Reviews, PMC)
- Major academic medical centers (Yale Medicine, Ohio State, Tufts, Mayo Clinic)
How we evaluate telehealth providers
We score providers on medical screening quality, pharmacy transparency, pricing clarity (including intro vs. renewal costs), cancellation policies, state availability, follow-up support quality, third-party review volume and ratings, and LegitScript certification status. We verify pricing and policies directly on provider websites and note the date of verification.
What we don’t do
- We don’t accept payment to rank providers higher.
- We don’t manufacture fake reviews or testimonials.
- We don’t make medical claims beyond what published research supports.
- We don’t imply expert review that hasn’t actually happened.
Your Next Step
You’ve done the research. You understand how GLP-1 works, what it costs, how to prepare, and what to expect. You know the side effects and how to manage them. You know the risks, the benefits, and the honest tradeoffs.
Now there’s really only one thing left to do: decide your path and start.
If you want to compare more providers first: See our full GLP-1 provider comparison — we’ve done the research so you don’t have to.
MEDVi
$179 first month — medication, provider access, 24/7 support included
Frequently Asked Questions: How to Start GLP-1
How do I start GLP-1 for weight loss?
Confirm you qualify (BMI ≥30, or ≥27 with a health condition), choose a provider path (doctor, telehealth, or insurance route), complete a medical evaluation, get prescribed, and start at the lowest dose. Most people can start within a week through telehealth.
Do I need a prescription to start GLP-1?
Yes, always. GLP-1 receptor agonists are prescription medications. Any legitimate path involves a licensed prescriber reviewing your health history before you receive medication. Run from anyone offering it without a prescription.
Can my primary care doctor prescribe Wegovy or Zepbound?
Yes, most PCPs can prescribe GLP-1 medications. However, not all are comfortable doing so, and some don’t have experience managing dose titration and side effects. If your PCP isn’t familiar with GLP-1 prescribing, ask for a referral to an obesity medicine specialist or consider a telehealth provider who specializes in it.
Can I get GLP-1 without a doctor?
No — and you shouldn’t try. The prescription requirement exists because GLP-1 medications have real contraindications and require clinical monitoring. But "without a doctor" often means "without weeks of in-person appointments." Telehealth providers offer licensed physician evaluations entirely online, often with approval within 24–48 hours.
What is the starting dose for GLP-1?
Semaglutide (Wegovy): 0.25 mg per week for the first 4 weeks, then gradually increased over ~16 weeks to the 2.4 mg maintenance dose. Tirzepatide (Zepbound): 2.5 mg per week for the first 4 weeks, then gradually increased. Always follow your provider’s titration schedule.
What if I miss a GLP-1 dose?
Semaglutide injection (Wegovy): if the next scheduled dose is more than 2 days away, take the missed dose as soon as possible. If it’s 2 days away or less, skip and resume on your regular schedule. Tirzepatide (Zepbound): if fewer than 4 days late, take it. If 4+ days, skip and resume on schedule.
How do I restart GLP-1 after stopping?
Contact your provider. If you’ve been off the medication for more than a few weeks, you’ll likely need to re-titrate from a lower dose to avoid rebound side effects. Don’t restart at your previous dose without medical guidance.
How do I give myself a GLP-1 shot?
Choose a site (abdomen, outer thigh, or upper arm), clean with alcohol, pinch a fold of skin, insert the pen needle at 90 degrees, inject, hold 5–10 seconds, remove. Rotate sites weekly. The needles are tiny and most people barely feel them after the first time.
Where do I inject GLP-1?
Abdomen (at least 2 inches from belly button), outer thigh, or upper arm. Rotate the injection site each week to avoid irritation or fat changes at one spot.
What should I eat the first week on GLP-1?
Small, bland, protein-focused meals. Avoid greasy, fried, and spicy foods. Good options: eggs, chicken, Greek yogurt, bananas, rice, toast, broth, ginger tea. Eat slowly and stop before you feel full.
What foods should I avoid on GLP-1?
Especially early on: greasy/fried foods (biggest nausea trigger), large portions, sugary drinks, alcohol, and very spicy foods. Your tolerance will improve over time, but the first few weeks call for boring, easy-to-digest eating.
How do I reduce GLP-1 nausea?
Eat small, frequent meals instead of large ones. Eat slowly. Avoid high-fat and greasy foods. Try ginger tea or ginger chews. Stay hydrated. Don’t eat until you feel overfull. If nausea is persistent, talk to your provider — they may slow your dose escalation or prescribe an anti-nausea medication.
How do I fix constipation on GLP-1?
Drink 80+ ounces of water daily (this is the #1 fix). Eat 25 grams of fiber per day. Walk for 30 minutes daily. Add a probiotic. If those don’t work, Miralax is generally safe — but confirm with your provider.
Is compounded semaglutide safe?
Compounded semaglutide is custom-prepared by licensed compounding pharmacies. The final product is NOT FDA-approved, and safety depends entirely on the pharmacy’s quality controls. The FDA has warned that some products marketed as "compounded semaglutide" may use different salt forms that are not the same active ingredient. Use compounded medications only from providers who name their pharmacy partners and have verifiable credentials (LegitScript certification, licensed 503A/503B pharmacy).
What does the FDA say about unapproved GLP-1 products?
The FDA warns consumers not to purchase GLP-1 products marketed without a prescription, labeled "for research use," or sold through unverified online sellers. These products may be counterfeit, contaminated, or incorrectly dosed. Always get GLP-1 through a licensed prescriber and a verified pharmacy.
Does Zepbound (tirzepatide) affect birth control pills?
Yes. Zepbound’s labeling warns that tirzepatide may reduce the effectiveness of oral hormonal contraceptives due to delayed gastric emptying. The FDA recommends switching to a non-oral contraceptive method or adding a barrier method for 4 weeks after starting Zepbound and for 4 weeks after each dose increase. This warning applies specifically to tirzepatide — studies on semaglutide have not shown the same effect.
How much does GLP-1 cost per month?
It depends on your path. With insurance coverage: as low as $25/month. Brand-name self-pay through manufacturer programs: $149–$449/month depending on medication, dose, and program. Compounded telehealth: $179–$399/month. MEDVi starts at $179 for month 1 with medication, provider access, and shipping included.
Does insurance cover GLP-1 for weight loss?
Some plans do, but coverage for weight-loss medications varies significantly. Most require prior authorization, documentation of BMI and comorbidities, and sometimes proof of prior weight loss attempts. Denials are common but can be appealed. Check with your insurer directly.
Do I have to take GLP-1 forever?
Not necessarily "forever," but long-term use is common and often recommended. Research shows significant weight regain after stopping. Some people transition to a maintenance dose. Others use the medication indefinitely, similar to blood pressure medication. Your provider can help you develop a long-term plan.
Can I increase GLP-1 naturally?
Your body produces GLP-1 naturally, and you can support higher levels through high-protein meals, fiber-rich foods, fermented foods, regular exercise, adequate sleep, and eating protein and fat before carbs at meals. However, natural strategies produce GLP-1 at much lower levels than medication. They’re excellent complements to treatment — not replacements for it.
Medical Disclaimer: This guide is for educational purposes and is not medical advice. Always consult with a licensed healthcare provider before starting any medication. GLP-1 medications are prescription drugs with contraindications and potential side effects that must be evaluated for your individual health profile.
References
- Wilding JPH, et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity. N Engl J Med. 2021;384:989-1002. NEJM
- Jastreboff AM, et al. Tirzepatide Once Weekly for the Treatment of Obesity. N Engl J Med. 2022;387:205-216. NEJM
- Novo Nordisk. STEP UP trial results. January 2025. novonordisk.com
- Lincoff AM, et al. Semaglutide and Cardiovascular Outcomes in Obesity without Diabetes (SELECT). N Engl J Med. 2023;389:2221-2232. NEJM
- FDA. Wegovy (semaglutide injection and tablets) Prescribing Information. Revised 12/2025. FDA.gov
- FDA. Zepbound (tirzepatide) Prescribing Information. FDA.gov
- FDA. Concerns with Unapproved GLP-1 Drugs Used for Weight Loss. FDA.gov
- FDA. Alerts Regarding Dosing Errors with Compounded Semaglutide. FDA.gov
- Cochrane Review. GLP-1 drugs effective for weight loss. 2025. Cochrane.org
- Real-World Weight Loss Among Patients Initiating Semaglutide. PMC. 2024. PMC
- Rubino D, et al. Effect of Continued Weekly Subcutaneous Semaglutide vs Placebo on Weight Loss Maintenance (STEP 4). JAMA. 2021;325:1414-1425. JAMA
- Wharton S, et al. Oral Semaglutide at a Dose of 25 mg in Adults with Overweight or Obesity (OASIS 4). N Engl J Med. 2025;393:1079-1089. NEJM
- Novo Nordisk. FDA approves Wegovy tablet. December 22, 2025. novonordisk.com
- LegitScript Website Certification. legitscript.com
- UCHealth. Nutrition When Taking GLP-1 Weight Loss Drugs. uchealth.org
- Ohio State University. GLP-1 Nutrition Guidance. health.osu.edu
- Novo Nordisk. Wegovy Savings and NovoCare Pharmacy Pricing. novocare.com
- Eli Lilly. Zepbound Savings Options and LillyDirect Pricing. zepbound.lilly.com
- Yale Medicine. GLP-1 Medications for Weight Loss: How to Get Started. yalemedicine.org
Related Guides
- Best GLP-1 Telehealth Providers (Compared)
- Semaglutide vs Tirzepatide: Which Is Right for You?
- Is Compounded Semaglutide Safe?
- GLP-1 Cost With and Without Insurance
- The Pros and Cons of GLP-1 Medications
- Oral Semaglutide vs Injectable: Complete Comparison
- GLP-1 Plateau: Why It’s Not Working + Fix Plan
- GLP-1 Tips and Tricks for Beginners: The 30-Day Starter Playbook
Related Articles
GLP-1 in Massachusetts
MA insurers cut GLP-1 coverage in 2026. 7 telehealth providers shipping to MA from $149/mo, real pricing, insurance workarounds, Medicare GLP-1 Bridge, and verification checklist.
GLP-1 in West Virginia
7 GLP-1 providers verified for WV — real prices from $149/mo, Medicaid/PEIA truth, WV telehealth law requirements, and which path fits your budget.
GLP-1 in Georgia
7 GLP-1 telehealth providers shipping to Georgia compared with real prices — compounded from $149/mo, Wegovy pill from $149/mo, insurance navigation, and Medicaid rules.
GLP-1 in Kentucky
7 GLP-1 providers verified for Kentucky — real April 2026 prices from $179/mo, KY telehealth law, Medicaid status, compounded vs FDA-approved, and which path fits your situation.
GLP-1 in Michigan
Michigan cut GLP-1 coverage in 2026. Compare 7 legit paths — FDA-approved and cash-pay — with real prices, insurance guidance, and a free Michigan matching quiz.
GLP-1 in North Dakota
North Dakota is the first state to add GLP-1 to ACA plans, but large-group plans just lost it. See real prices and the best provider for your plan type. April 2026.
Browse All: GLP-1 Overview & Education
Explore all 22 guides in this topic.
★What Is GLP-1?
A complete beginner's guide to GLP-1 medications, how they work, and what to expect.
GLP-1s for Weight Loss
How GLP-1 receptor agonists promote weight loss through appetite reduction and metabolic changes.
Learn About GLP-1
Educational hub covering GLP-1 science, medications, eligibility, and treatment options.
History of GLP-1 Drugs
The complete timeline of GLP-1 drug development from discovery to modern weight loss treatments.
Semaglutide vs Tirzepatide
Head-to-head comparison of semaglutide and tirzepatide for weight loss effectiveness and cost.
Retatrutide vs Tirzepatide
Triple agonist vs dual agonist: trial data, side effects, availability, and what you can actually do today.
Willow vs Ozempic
Willow telehealth service vs FDA-approved Ozempic: real pricing, safety, eligibility, and regulatory differences compared.
GLP-1 in Massachusetts
MA insurers cut GLP-1 coverage in 2026. 7 telehealth providers shipping to MA from $149/mo, real pricing, insurance workarounds, Medicare GLP-1 Bridge, and verification checklist.
GLP-1 in West Virginia
7 GLP-1 providers verified for WV — real prices from $149/mo, Medicaid/PEIA truth, WV telehealth law requirements, and which path fits your budget.
GLP-1 in Georgia
7 GLP-1 telehealth providers shipping to Georgia compared with real prices — compounded from $149/mo, Wegovy pill from $149/mo, insurance navigation, and Medicaid rules.
GLP-1 in Kentucky
7 GLP-1 providers verified for Kentucky — real April 2026 prices from $179/mo, KY telehealth law, Medicaid status, compounded vs FDA-approved, and which path fits your situation.
GLP-1 in Michigan
Michigan cut GLP-1 coverage in 2026. Compare 7 legit paths — FDA-approved and cash-pay — with real prices, insurance guidance, and a free Michigan matching quiz.
GLP-1 in North Dakota
North Dakota is the first state to add GLP-1 to ACA plans, but large-group plans just lost it. See real prices and the best provider for your plan type. April 2026.
GLP-1 in Rhode Island
GLP-1 in Rhode Island: real prices from $129/mo, BCBSRI and Medicaid coverage checked, fastest online and local options compared. Updated April 2026.
GLP-1 in New Hampshire
NH Medicaid dropped GLP-1 weight-loss coverage in 2026. Here are 7 providers with real prices, local clinics, and a free matching quiz. Find your fit fast.
How to Get GLP-1 in New York
Every legit way to get GLP-1 in New York — telehealth, clinics, pills, shots, costs, insurance, Medicaid rules, and scam avoidance.
How to Get GLP-1 in Florida
Florida GLP-1 guide: telehealth law, real provider costs from $149/mo, insurance navigation, and how to verify any provider before paying.
How to Get GLP-1 in New Jersey
New Jersey GLP-1 guide: NJ telehealth rules, FDA-approved and compounded paths, NJ Medicaid coverage, insurance navigation, and verified provider costs.
How to Get GLP-1 in North Carolina
North Carolina GLP-1 guide: NC Medicaid reinstated coverage, Blue Cross NC options, State Health Plan exclusion, telehealth rules, and verified provider costs from $149/mo.
GLP-1 for Prediabetes
Can GLP-1 medications prevent type 2 diabetes? Evidence, costs, eligibility, and next steps for prediabetes.
Oral Semaglutide vs Injectable
Comparing oral and injectable semaglutide forms by effectiveness, convenience, and price.
What Happens When You Stop Taking GLP-1
What to expect when discontinuing GLP-1 medications including weight regain and withdrawal effects.