GLP-1 Tips and Tricks for Beginners: The 30-Day Starter Playbook
If you just got prescribed a GLP-1 medication — or you’re about to — here’s the bottom line on GLP-1 tips and tricks for beginners: eat protein first at every meal (25–35g), drink 80–100 oz of water daily, take your first shot on a day you can rest, start strength training now (not later), and don’t panic about nausea. It peaks around days 2–4 and fades by week 2 for most people.
That’s the short version. But you probably have about 40 more questions — What do I eat? What do I avoid? How do I actually do the injection? Is this constipation normal? Am I losing muscle? How do I not waste $200–500 a month?
We built this page to answer every single one of them. No fluff, no filler, no scare tactics. Just the practical playbook we wish existed when we started covering GLP-1 medications — organized in the order your brain actually needs the information.
This guide applies to all GLP-1 medications — Wegovy, Ozempic, Zepbound, Mounjaro, Rybelsus, and compounded semaglutide or tirzepatide. Always follow your prescriber’s specific instructions when they differ from general guidance.
Every tip below is grounded in FDA prescribing information, published clinical data, or consensus clinical practice. This is educational content, not medical advice. When in doubt, contact your clinician.
Disclosure: Some links on this site are affiliate links. If you purchase through these links, we may earn a commission at no extra cost to you. Thank you for supporting our site.·For informational purposes only—not medical advice.
What Are the 10 Most Important GLP-1 Tips for Beginners?
Before we go deep, here’s the Pareto version — the 20% of actions that drive 80% of your results. If you only read one section, read this.
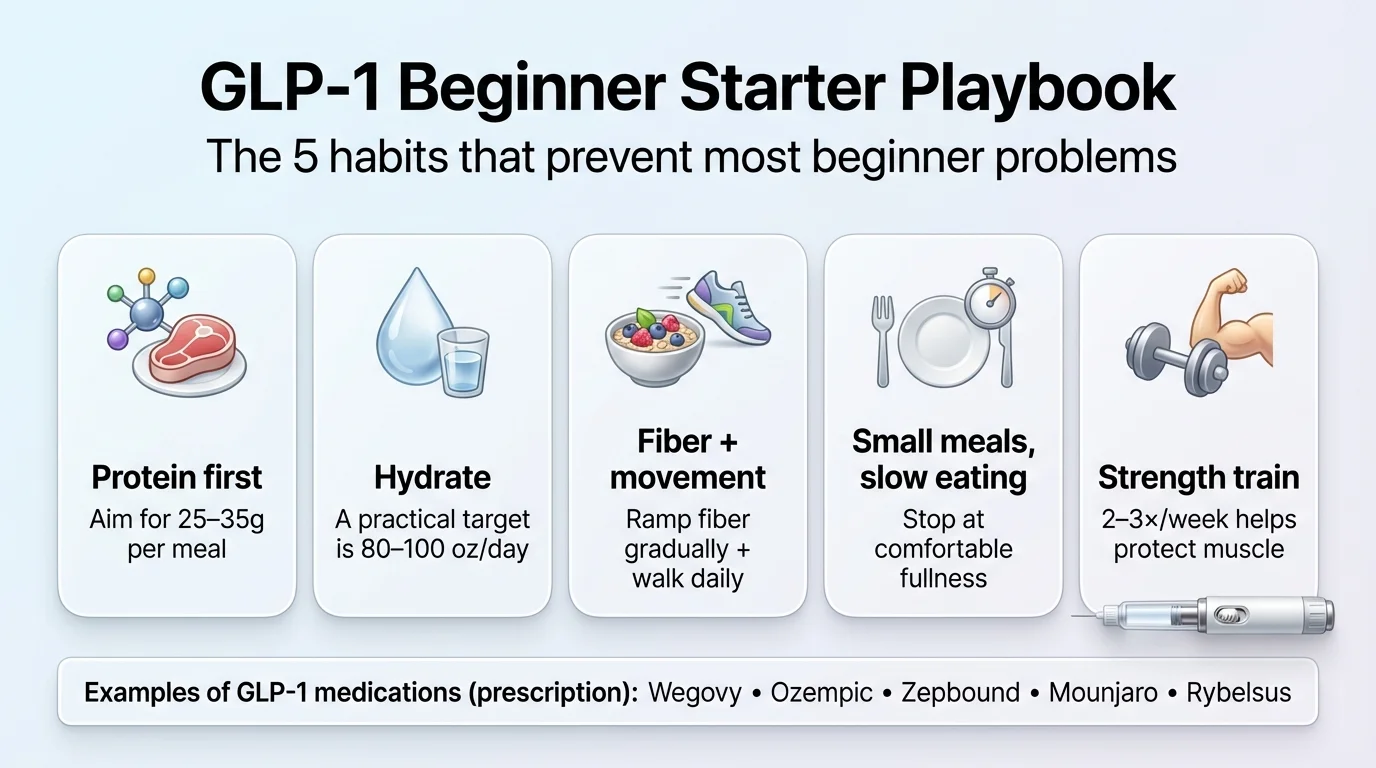
1. Protein first, every meal. Aim for 25–35g per meal. Protein preserves muscle, keeps you full, and stabilizes blood sugar. Eat it before vegetables, and eat vegetables before carbs. This single habit changes everything.
2. Hydrate aggressively. GLP-1s suppress thirst alongside hunger. You won’t feel thirsty even when dehydrated. Set a target of 80–100 oz of water daily and use reminders. Dehydration makes every side effect worse — nausea, headaches, constipation, fatigue.
3. Prevent constipation from day one. Don’t wait for it to happen. Start fiber (25–35g/day, ramped up gradually), drink your water, walk daily, and have Miralax on hand. Constipation is the side effect most beginners underestimate.
4. Plan your injection day strategically. Pick a day when you can rest the next day. Many people choose Thursday or Friday evening — if side effects hit, you have the weekend. Take it at the same time each week.
5. Eat small, eat slow. Your fullness signals are amplified on GLP-1s. Eat 4–5 smaller meals instead of 3 large ones, and take 15–20 minutes per meal. Overeating on a GLP-1 feels significantly worse than overeating without one.
6. Strength train 2–3 times per week. This is not optional. When you lose weight — by any method — you lose some muscle. Resistance training combined with high protein intake is the only proven way to minimize that loss. Start before or on day one, not after you’ve already lost muscle.
7. Go low-fat on injection day and dose increases. Fatty foods sit in your stomach longer. GLP-1s already slow digestion. The combination is why new users get blindsided by nausea after a burger on shot day. Stick to lean protein, simple carbs, and easy-to-digest foods for 24–48 hours around your injection.
8. Track three things (and only three). Weekly weight trend (not daily), daily protein consistency (did you hit your target?), and side effects with what you ate. That’s it. You don’t need to count every calorie — you need to see patterns.
9. Never adjust your dose without your prescriber. “Microdosing,” splitting pens, or skipping dose escalation steps based on internet advice is how people get inconsistent results or unnecessary side effects. Your prescriber sets the schedule for a reason.
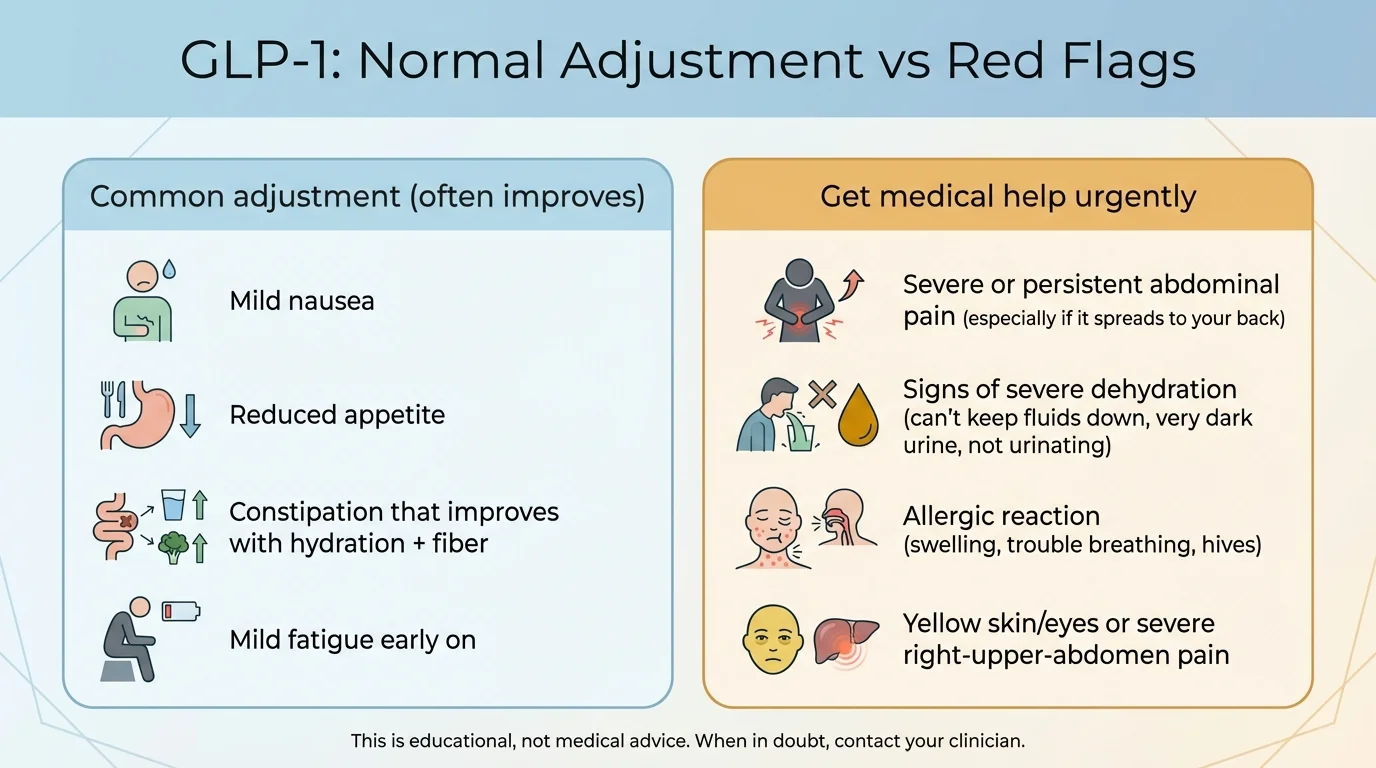
10. Learn the difference between normal adjustment and a red flag. Mild nausea for a few days? Normal. Severe abdominal pain radiating to your back? Call your doctor immediately. We cover the full list in the Red Flags section below.
Beginner Quick-Fix Table
| Problem | Likely Cause | What to Do in the Next 24 Hours | Red Flag → Contact Prescriber |
|---|---|---|---|
| Nausea | Normal GI adjustment, eating too fast or too much fat | Small bland meals, ginger tea/chews, stay hydrated, avoid greasy food | Can’t keep any fluids down for 12+ hours |
| Constipation | Slower GI motility + dehydration | 80+ oz water, fiber-rich foods, 20-min walk, Miralax if needed | No bowel movement for 5+ days with pain |
| Fatigue | Calorie reduction, dehydration, body adjusting | Eat enough protein, hydrate, sleep 7–9 hours | Extreme fatigue lasting 3+ weeks |
| Heartburn | Slower gastric emptying + acidic/spicy foods | Avoid eating 3 hrs before bed, elevate head, OTC antacid | Chest pain, difficulty swallowing |
| “Sulfur burps” | Delayed gastric emptying, food sitting longer | Smaller meals, avoid carbonation, eat slowly, peppermint tea | Persistent vomiting with burps |
| Appetite too low | Medication working as intended (sometimes too well) | Eat by the clock, not by hunger. Protein shakes count. | Eating under 800 calories/day consistently |
What Are GLP-1 Medications — and Which Ones Count?
GLP-1 receptor agonists are medications that mimic a hormone your gut naturally produces after you eat. That hormone — glucagon-like peptide-1 — helps regulate appetite, blood sugar, and digestion. The medications amplify that signal, so you feel full sooner, think about food less, and your body processes glucose more efficiently.
You’ve probably heard the brand names: Ozempic, Wegovy, Mounjaro, Zepbound. Here’s what’s actually what.
Beginner Cheat Sheet: Which Medication Is Which
| Generic Name | Brand Name(s) | Type | FDA-Approved For | How You Take It | Frequency |
|---|---|---|---|---|---|
| Semaglutide | Wegovy (injection) | GLP-1 agonist | Weight management (adults and adolescents 12+); cardiovascular risk reduction; MASH with fibrosis | Injection | Weekly |
| Semaglutide | Wegovy (tablets) | GLP-1 agonist | Weight management (adults only); cardiovascular risk reduction | Oral tablet | Daily |
| Semaglutide | Ozempic | GLP-1 agonist | Type 2 diabetes | Injection | Weekly |
| Semaglutide | Rybelsus | GLP-1 agonist | Type 2 diabetes | Oral tablet | Daily |
| Tirzepatide | Zepbound | Dual GLP-1/GIP agonist | Weight management; obstructive sleep apnea in adults with obesity | Injection | Weekly |
| Tirzepatide | Mounjaro | Dual GLP-1/GIP agonist | Type 2 diabetes | Injection | Weekly |
| Liraglutide | Saxenda | GLP-1 agonist | Weight management | Injection | Daily |
Three Things Beginners Mix Up
1. Ozempic and Wegovy are the same molecule (semaglutide) at different doses for different conditions. Ozempic maxes at 2mg for diabetes. Wegovy goes up to 2.4mg for weight management.
2. Tirzepatide (Mounjaro/Zepbound) is a dual agonist — it targets both GLP-1 and GIP receptors. Clinical trials showed higher average weight loss compared to semaglutide alone, though individual results vary widely. Learn more in our semaglutide vs. tirzepatide comparison.
3. Oral GLP-1s exist. Rybelsus (for diabetes) has been around for years. Wegovy tablets are now FDA-approved for adults (weight management and cardiovascular risk reduction). The dosing rules for oral versions are strict — you take them on an empty stomach with a small sip of water and wait 30 minutes before eating. See our oral vs. injectable comparison.
Clinical context: In the STEP 1 trial, semaglutide 2.4mg produced an average of roughly 15% body weight loss over 68 weeks. In SURMOUNT-1, tirzepatide 15mg produced approximately 22%. These are averages — some people lose more, some less. The medication is a tool, not a guarantee.
Sources: FDA prescribing information for Wegovy, Ozempic, Zepbound, Mounjaro; Wilding et al., NEJM 2021 (STEP 1); Jastreboff et al., NEJM 2022 (SURMOUNT-1)
What Should You Do Before Your First Dose?
The 48 hours before your first injection matter more than most guides let on. A little preparation here prevents a lot of misery in week one.
Confirm with Your Prescriber
- Your specific medication, dose, and escalation schedule
- Any contraindications that apply to you — FDA labeling for all GLP-1 agonists includes warnings about medullary thyroid carcinoma (MTC) risk in patients with a personal or family history of MTC or Multiple Endocrine Neoplasia syndrome type 2 (MEN2)
- Pancreatitis and gallbladder disease risk (noted in all GLP-1 labeling)
- If you’re on insulin or sulfonylureas, whether doses need adjustment (hypoglycemia risk increases)
- If you’re planning pregnancy — GLP-1 labeling includes fetal harm warnings; discontinue well before conception
- If you take oral birth control — tirzepatide (Zepbound/Mounjaro) labeling specifically advises switching to a non-oral contraceptive method or adding a barrier method for 4 weeks after initiation and 4 weeks after each dose escalation, because GLP-1 agonists may reduce oral contraceptive absorption
- If you have any upcoming surgeries or procedures — GLP-1s delay gastric emptying, which creates aspiration risk under anesthesia. Current multi-society guidance (including ASA) says most patients can continue, but your surgical team may require precautions. Always inform your surgeon and anesthesiologist.
Stock Your Kitchen
- Protein staples: Greek yogurt, eggs, rotisserie chicken, canned tuna, cottage cheese, protein shakes, string cheese
- Fiber basics: berries, oats, chia seeds, lentils (start increasing fiber intake NOW so your gut adjusts before the medication adds slower digestion)
- Easy bland foods for nausea days: crackers, applesauce, toast, chicken broth, bananas
- Ginger tea, ginger chews, or ginger candies (evidence supports ginger for nausea management)
Set Yourself Up
- Buy a large water bottle and set phone reminders to drink
- Choose your injection day and time (same day, same time, every week)
- Get a food journal or tracking app ready (simple — you’re tracking protein and side effects, not every macro)
- Have OTC remedies on hand: Miralax (constipation), Gas-X (bloating), antacid (heartburn), electrolyte packets
- Take “before” measurements: weight, waist circumference, and photos. You’ll want these at day 30.
- Start bodyweight exercises or resistance training THIS WEEK — muscle preservation starts before the medication, not after
If you’re still figuring out which provider or medication is right for you, our eligibility assessment takes about 2 minutes and matches you with vetted telehealth options based on your state, budget, and insurance status.
How Do You Take a GLP-1 Injection Correctly?
If you’ve never self-injected anything, the idea sounds much worse than the reality. The needle is tiny — 4mm to 5mm — and most people say it hurts less than a finger prick. After the second or third time, it becomes routine.
Important: Always follow your specific prescribing instructions. This is general guidance, not a substitute for what your provider told you.
Step-by-Step Injection Guide
- 1Wash your hands thoroughly with soap and water.
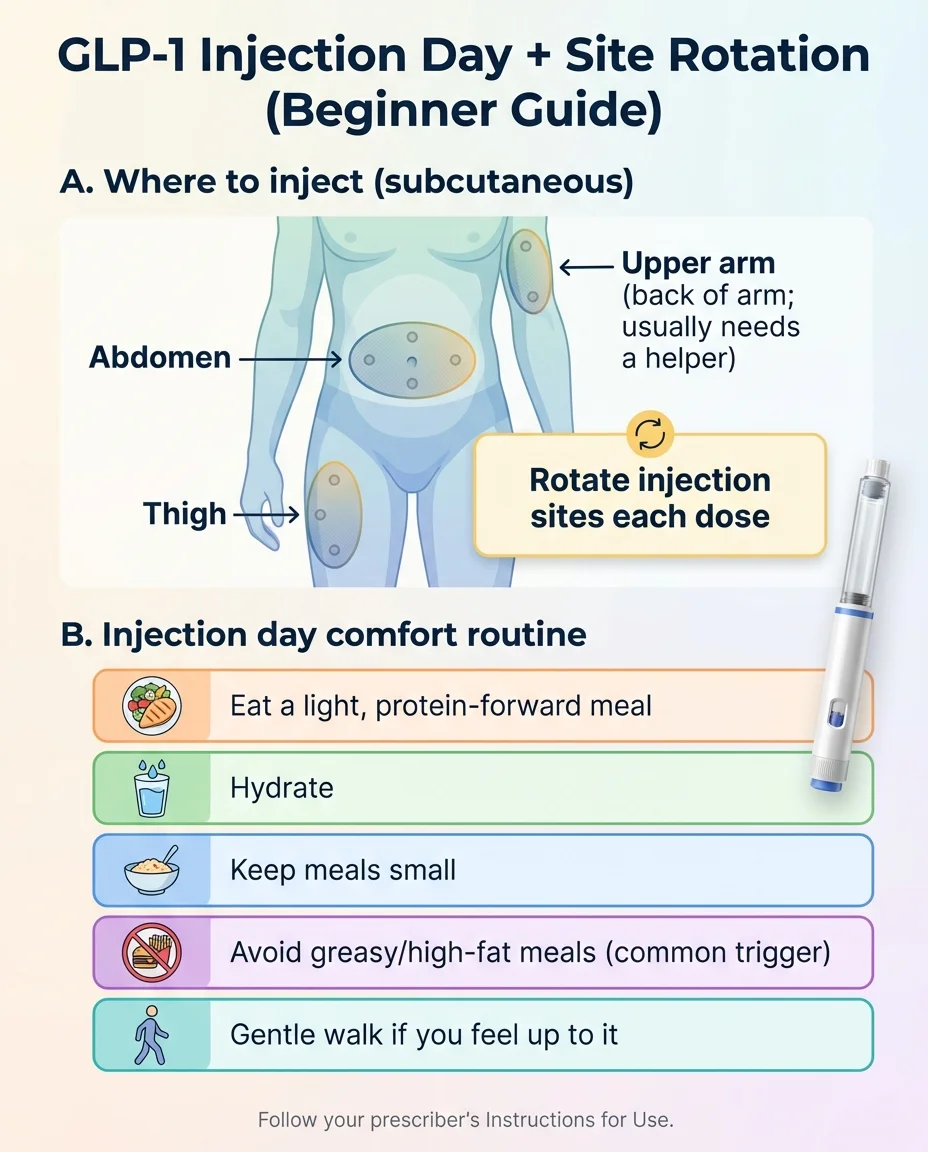
- 2Choose your injection site. Three options: abdomen (at least 2 inches from your belly button), front of your thigh, or back of your upper arm. The abdomen tends to be the easiest and least sensitive for most people.
- 3Clean the site with an alcohol swab. Let it dry completely — injecting through wet alcohol stings.
- 4
Identify your device type (this changes the steps):
- • Single-dose pens (needle is built in — you do NOT attach one): Wegovy injection, Mounjaro (single-dose pen), and Zepbound (single-dose pen). Follow the “Instructions for Use” that came with your device.
- • Multi-dose pens (you attach a new pen needle each time): Ozempic and, if prescribed, the Mounjaro KwikPen or Zepbound KwikPen. Attach a new needle before each injection, and remove it after.
- • Not sure which you have? Check the carton or the Instructions for Use that came with your medication. Don’t guess.
- 5If your device requires it, follow the first-use checks/priming steps in your Instructions for Use. Multi-dose pens typically require priming before first use.
- 6Pinch the skin gently at your injection site. Insert the needle at a 90-degree angle straight in.
- 7Press the injection button. Hold it down for the full count specified by your brand — usually 5–10 seconds. You want all the medication delivered.
- 8Remove the needle straight out. Don’t rub the injection site.
- 9Dispose of the needle in a sharps container. Never reuse needles.
Injection Site Rotation
Rotate your injection site every week. Don’t use the same exact spot within 1 inch for at least a week. A simple rotation: abdomen this week → left thigh next week → right thigh the week after → back to abdomen.
Why it matters: Repeated injection in the same spot can cause lipodystrophy — lumps or hardened tissue under the skin that can affect medication absorption.
Pro Tips From Real Users
- • Take your shot at bedtime. Many people find that sleeping through the first 6–8 hours after injection means they sleep through the worst of any nausea.
- • If needles make you anxious, press an ice cube to the site for 20–30 seconds first. It numbs the area. You can also use OTC lidocaine cream.
- • Relax the muscle. Tensing up makes it hurt more. Take a slow breath, exhale, and inject on the exhale.
- • Don’t watch. Seriously. The auto-injector pens just require you to press and hold. Look away if it helps.
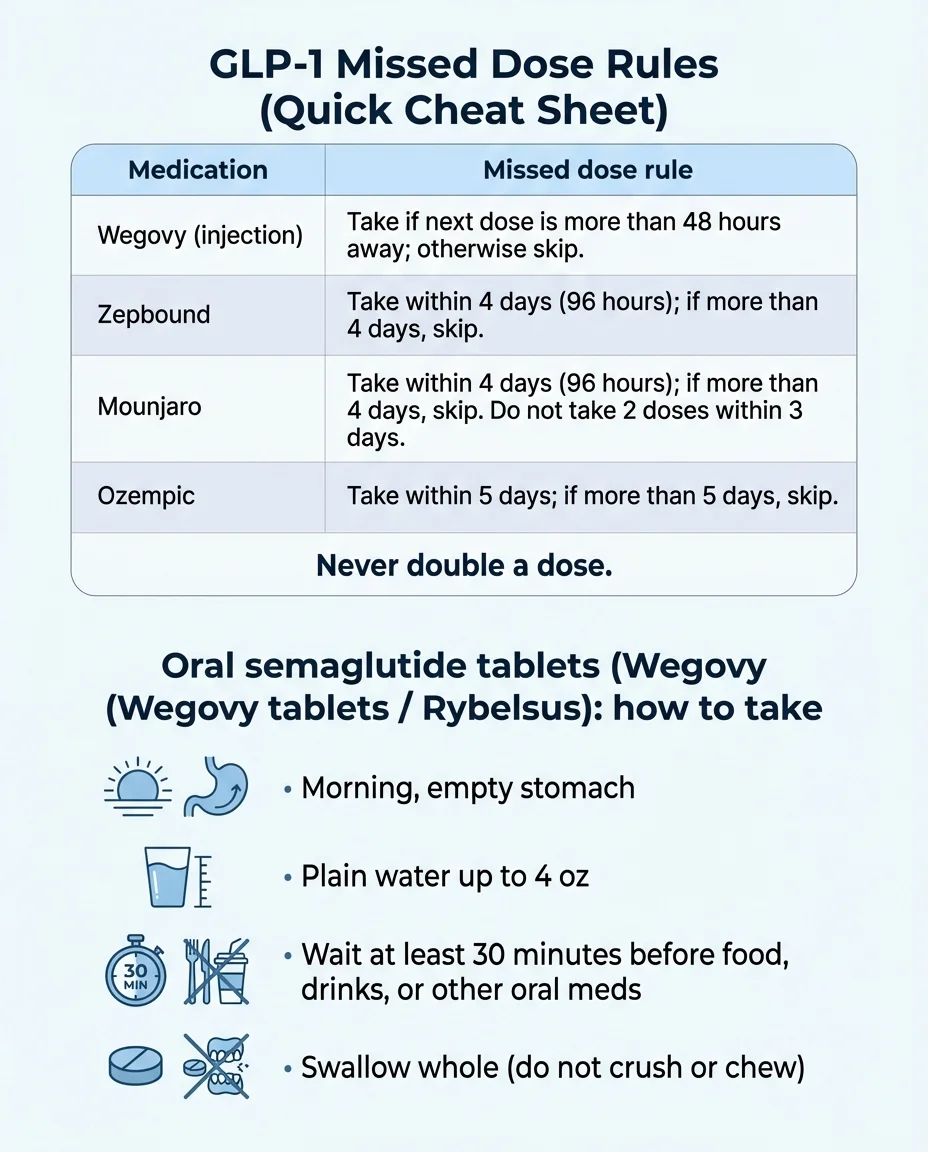
Oral GLP-1 Rules (Rybelsus, Wegovy Tablets)
If you’re on an oral form, the timing rules are strict and non-negotiable:
- Take it first thing in the morning on a completely empty stomach
- Swallow whole with no more than 4 oz (half a glass) of plain water
- Wait at least 30 minutes before eating, drinking anything else, or taking other oral medications
- Do not crush, chew, or split the tablet
The reason: the medication needs an acidic stomach environment with minimal food or liquid to absorb properly. Breaking these rules significantly reduces how much medication your body actually gets. For a deep comparison, see our oral vs. injectable semaglutide comparison.
Sources: FDA prescribing information for Wegovy, Ozempic, Mounjaro, Zepbound; manufacturer injection instructions
What Should You Eat on a GLP-1? (The Beginner’s Diet Guide)
This is the section most beginners need most — and where most other guides give you a vague “eat healthy” and call it a day. We’re going to be specific.
The GLP-1 Plate Method
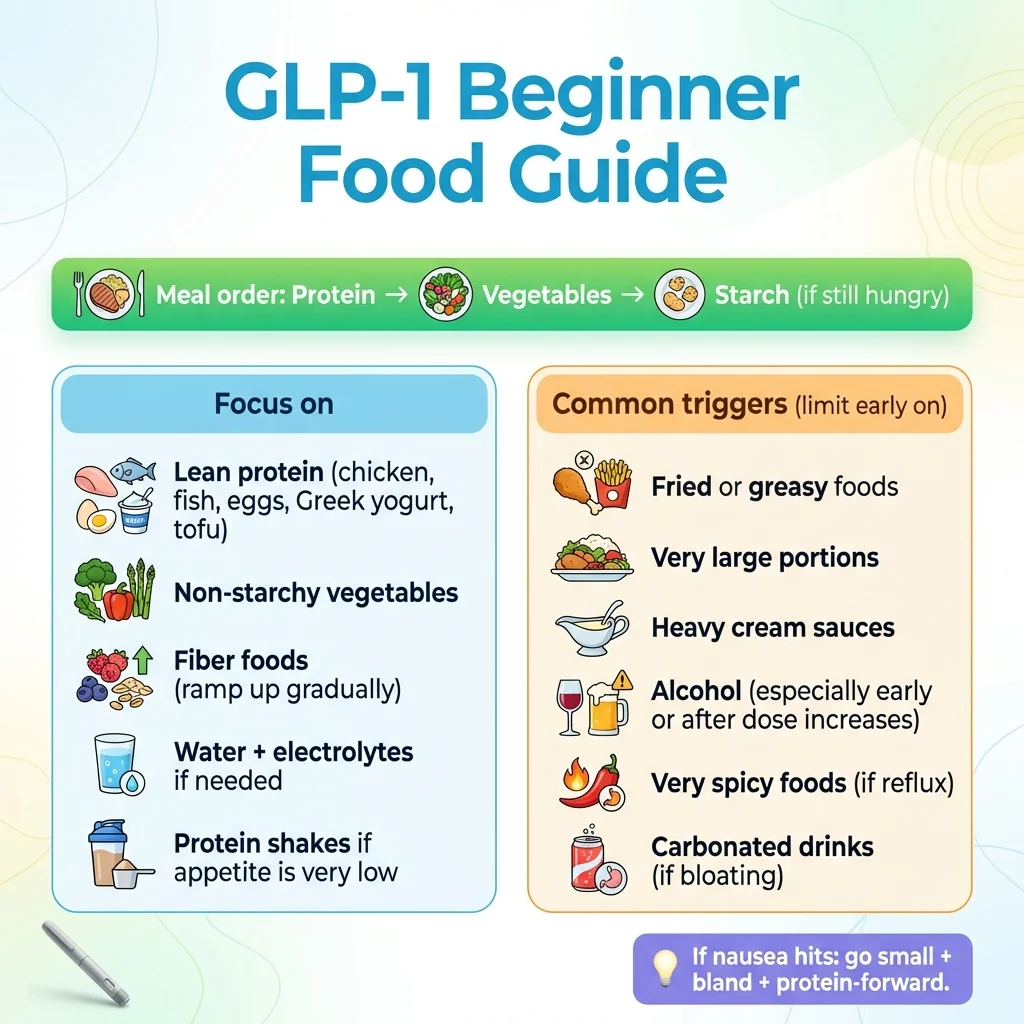
Think of every meal in this order:
- 1Protein first (always — this is the non-negotiable)
- 2Non-starchy vegetables next (fiber + nutrients)
- 3Healthy fats in moderation (avocado, olive oil, nuts)
- 4Starches and fruit last (only if you’re still hungry)
Why this order? GLP-1s slow gastric emptying — food sits in your stomach longer. Protein takes priority because you’re eating less overall, and every bite needs to count for muscle preservation and satiety. Vegetables provide fiber to keep your GI system moving. Fats and starches are where side effects get triggered if you overdo it.
How Much Protein Do You Actually Need?
Practical protein target: Many experts suggest aiming around 1.2–1.6 g/kg of body weight per day (often roughly 80–120g daily for many adults), split across meals — unless your clinician has you on a different plan, especially if you have kidney disease.
A joint advisory from the American Society for Nutrition, the Obesity Medicine Association, and The Obesity Society (Mozaffarian et al., 2025) specifically emphasized prioritizing protein intake for patients on GLP-1 therapy to prevent lean mass loss.
Protein-Per-Meal Quick Reference
| Food | Serving Size | Protein |
|---|---|---|
| Chicken breast (grilled) | 4 oz | ~35g |
| Cottage cheese (low-fat) | 1 cup | ~28g |
| Salmon (baked) | 4 oz | ~25g |
| Whey protein shake | 1 scoop | ~25–30g |
| Ground turkey (93% lean) | 4 oz | ~22g |
| Greek yogurt (plain, 2%) | 1 cup | ~20g |
| Tuna (canned in water) | 1 can (5 oz) | ~20g |
| Tofu (firm) | ½ block | ~20g |
| Lentils (cooked) | 1 cup | ~18g |
| Black beans (cooked) | 1 cup | ~15g |
| Eggs (whole) | 2 large | ~12g |
| String cheese | 2 sticks | ~14g |
If your appetite is very low: Protein shakes are your best friend. A scoop of whey in a smoothie with berries and Greek yogurt gets you 40–50g in something that goes down easy even on nausea days.
Foods to Eat vs. Foods to Avoid on GLP-1s
This isn’t about “good” and “bad” foods. It’s about what your body tolerates well on a GLP-1 — especially in the first few weeks — versus what tends to trigger side effects.
| Focus on These | Limit or Avoid (Especially Early On) | Why It Matters |
|---|---|---|
| Lean proteins: chicken, fish, eggs, Greek yogurt, cottage cheese, tofu | Fried foods: french fries, fried chicken, mozzarella sticks | High fat + slow digestion = nausea and bloating |
| Non-starchy vegetables: broccoli, spinach, zucchini, bell peppers | Greasy/rich foods: fast food, cream sauces, heavy cheese dishes | Fat sits in your already-slow stomach even longer |
| Whole grains in small portions: oats, quinoa, brown rice | Sugary foods and drinks: soda, candy, pastries, fruit juice | Blood sugar spikes, empty calories, works against the medication |
| Healthy fats (small amounts): avocado, olive oil, almonds | Highly spicy foods (at first): hot sauce, chili peppers | Worsens nausea and heartburn while your GI system adjusts |
| Fiber-rich foods (ramped up gradually): berries, chia seeds, lentils | Very large portions of anything | Your “full” signal is amplified — overeating causes vomiting |
| Probiotic foods: plain yogurt, kefir, sauerkraut | Alcohol (especially first 4 weeks and dose increase weeks) | Lower tolerance, amplified nausea, dehydration, empty calories |
| Water, herbal tea, electrolyte drinks | Carbonated beverages | Gas and bloating compound the GLP-1 digestive slowdown |
| Cold foods when nauseous: smoothies, yogurt, chilled chicken salad | Coffee on an empty stomach | Stomach acid + empty GLP-1 stomach = nausea spiral. Eat protein first, then coffee. |
What to Eat on Injection Day
- Before your shot: Eat a light, protein-forward meal. Think grilled chicken with rice, or eggs with toast. Nothing heavy, nothing greasy.
- Shot day evening (if you inject at night): Keep it simple. Soup, a protein shake, crackers with cottage cheese.
- Next day: Lighter meals, extra hydration. This is not the day to try the new Thai place.
- Dose increase weeks: Treat these like your first injection all over again — go bland, go small, go easy.
The coffee rule worth repeating: You can still drink coffee. Just eat something with protein first — even a hard-boiled egg or a few bites of Greek yogurt. Coffee on an empty GLP-1 stomach triggers a nausea-acid combo that ruins your morning.
For a detailed nausea meal plan, see our GLP-1 nausea food guide.
Sources: Cleveland Clinic GLP-1 diet guide; Ohio State Health & Discovery; Mozaffarian et al. (2025), nutritional priorities for GLP-1 therapy (ACLM, ASN, OMA, TOS joint advisory); FDA prescribing information
How Do You Handle GLP-1 Side Effects? (The Side Effect Solver)
Let’s normalize this: GI side effects are common, especially during dose escalation, and typically improve over time. How common? Here’s what FDA labeling actually reports:
How Common Are Side Effects? (FDA Label Data)
| Side Effect | Wegovy Injection (Adults) | Zepbound (Adults, Dose Range) |
|---|---|---|
| Any GI adverse reaction | 73% | — |
| Nausea | 44% | 25–29% |
| Diarrhea | 30% | 19–23% |
| Vomiting | 24% | 8–13% |
| Constipation | 24% | 11–17% |
| Fatigue | 11% | 5–7% |
| GERD | Reported (≥5%) | 4–5% |
These numbers look scary, but context matters: most cases were mild to moderate, occurred during dose escalation, and resolved as the body adjusted. Only about 5–7% of patients discontinued treatment due to GI side effects.
Nausea (Most Common — Up to ~44% with Wegovy, ~25–29% with Zepbound)
What it feels like: Mild to moderate queasiness, usually worst on days 2–4 after injection, often fading by end of week 1 at each dose level.
What helps:
- • Small, frequent meals (4–5 per day instead of 3)
- • Ginger — tea, chews, or candies (evidence-backed for nausea)
- • Avoid greasy, fatty, or heavily spiced foods
- • Eat before drinking coffee or acidic beverages
- • Take your injection at bedtime to sleep through the peak
- • Cold foods often settle better than hot when nauseous
- • Stay hydrated — dehydration makes nausea worse
What to avoid: Large meals, lying down immediately after eating, skipping meals entirely (empty stomach makes it worse).
Red flag: You cannot keep any fluids down for 12+ hours, or you’re vomiting repeatedly. Contact your prescriber.
Constipation (~24% with Wegovy, ~11–17% with Zepbound)
Why it happens: GLP-1s slow everything down in your GI tract. Add reduced food intake (less fiber, less volume) and reduced thirst signals, and things stop moving.
What helps:
- • 80–100 oz of water daily (non-negotiable)
- • 25–35g of fiber daily from food (fruits, vegetables, beans, oats, chia seeds — increase gradually)
- • Daily walking (20+ minutes — movement stimulates the gut)
- • Probiotic foods or supplements
- • Miralax (osmotic laxative) if dietary changes aren’t enough — it’s gentle and generally safe for regular use
- • Fiber supplement (psyllium husk) if you can’t get enough from food
What to avoid: Waiting until it’s a problem. Prevent it from day one.
Red flag: No bowel movement for 5+ days with pain or bloating. Contact your prescriber.
Diarrhea (~30% with Wegovy, ~19–23% with Zepbound)
What helps: BRAT foods (bananas, rice, applesauce, toast), hydrate with electrolytes, avoid high-fat foods and dairy temporarily.
Red flag: Bloody stool, signs of severe dehydration (dizziness, dark urine, rapid heartbeat).
Heartburn/Acid Reflux (Reported at ≥5% with Wegovy, ~4–5% with Zepbound)
What helps: Don’t eat within 3 hours of lying down, elevate the head of your bed, avoid spicy/acidic foods and alcohol, OTC antacids.
Red flag: Chest pain or difficulty swallowing.
Fatigue (Common in first 1–2 weeks at each dose)
What helps: Ensure you’re eating enough (under-eating causes fatigue faster than the medication), stay hydrated, prioritize sleep (7–9 hours), check that you’re getting adequate calories — GLP-1 fatigue is often calorie deficiency fatigue.
Red flag: Extreme exhaustion lasting more than 3 weeks at a stable dose.
Headache (Common in first few days)
What helps: Almost always dehydration. Drink more water. Electrolytes help. OTC pain relief with provider approval.
Red flag: Severe or persistent headache that doesn’t respond to hydration and OTC remedies.
Appetite Suppression That’s “Too Strong”
This sounds like a good problem until you realize you haven’t eaten 800 calories in three days and you feel terrible.
What helps: Eat by the clock, not by hunger signals. Set meal reminders. Protein shakes count as meals. Even small amounts of nutrient-dense food matter — a handful of almonds, a cheese stick, a few spoonfuls of yogurt.
Red flag: Consistently eating under 800 calories for multiple days, signs of malnutrition (extreme weakness, hair loss, dizziness, fainting).
Hair Thinning (Uncommon, typically months 3–6)
What helps: This is usually from rapid weight loss (telogen effluvium), not from the medication directly. Adequate protein, a daily multivitamin, and biotin can help. It’s almost always temporary — hair regrows once weight stabilizes.
Red flag: Significant patchy hair loss. See a dermatologist.
For more side effect management, see our complete GLP-1 side effects guide and GLP-1 SOS side effect relief hub.
Sources: FDA prescribing information (adverse reactions sections); Wharton et al. (2022) GLP-1RA side effect management; Cleveland Clinic; STEP and SURMOUNT trial adverse event data
Red Flags Beginners Should Never Ignore
Most GLP-1 side effects are uncomfortable but not dangerous. These are the exceptions. If you experience any of the following, stop the medication and contact your healthcare provider immediately — or go to urgent care/the ER if symptoms are severe.
Severe persistent abdominal pain, especially radiating to your back. This could indicate pancreatitis. FDA labeling for all GLP-1 agonists includes warnings about acute pancreatitis. Do not “wait it out.”
Signs of gallbladder problems. Sudden pain in the upper right abdomen, fever, jaundice (yellowing of skin or eyes), clay-colored stools. FDA labeling notes increased occurrence of cholelithiasis (gallstones) with GLP-1 use.
Severe dehydration. You can’t keep fluids down, you feel dizzy when standing, your urine is very dark or you’re not urinating, your heart is racing. Dehydration from vomiting/diarrhea on GLP-1s can escalate quickly.
Allergic reaction. Difficulty breathing, swelling of face/tongue/throat, hives, rapid heartbeat. Rare but serious.
Vision changes. New blurring, floaters, or vision loss — particularly if you have diabetes. GLP-1 medications can worsen diabetic retinopathy in some cases.
Lump or swelling in your neck. FDA labeling carries a boxed warning about thyroid C-cell tumors observed in animal studies. Report any neck lumps, hoarseness, difficulty swallowing, or shortness of breath.
Thoughts of self-harm or significant mood changes. Suicidal behavior and ideation are listed in post-marketing reports in GLP-1 labeling. If you or someone close to you notices significant mood changes, contact your prescriber.
Severe hypoglycemia (if you’re also on insulin or sulfonylureas). Shakiness, confusion, sweating, rapid heartbeat, loss of consciousness. GLP-1s combined with certain diabetes medications increase this risk.
The vast majority of people on GLP-1s will never experience any of these. But knowing them means you’ll act fast if something feels wrong — and that makes all the difference.
For more detail, see our GLP-1 contraindications guide.
Sources: FDA prescribing information for Wegovy, Zepbound (boxed warnings, warnings and precautions sections); ASA consensus guidance on preoperative GLP-1 management
What Exercise Should You Do on a GLP-1? (The Muscle Protection Plan)
Here’s an uncomfortable truth that most GLP-1 tip lists gloss over: when you lose weight by any method, a meaningful portion of that loss can come from lean mass — not just fat. Estimates vary, but in some clinical data, lean soft tissue has accounted for roughly 26–40% of weight lost. GLP-1s aren’t special in this regard — similar ratios apply to calorie restriction, bariatric surgery, and other weight loss approaches.
But here’s the good news: you can shift that ratio dramatically with two things — high protein intake and resistance training. A 2025 study presented at the European Congress on Obesity found that patients who combined GLP-1 medication with supervised strength training and adequate protein preserved significantly more lean mass while still losing fat at the same rate.
Strength Training: Non-Negotiable
Minimum effective dose: 2 sessions per week, hitting all major muscle groups. Three sessions is better. Focus on compound movements — exercises that work multiple muscle groups at once:
| Day | Sample Exercises | Sets × Reps |
|---|---|---|
| Day 1 (Upper body + core) | Push-ups (or knee push-ups), dumbbell rows, overhead press, plank | 3 × 10–12 each |
| Day 2 (Lower body + core) | Goblet squats, lunges, glute bridges, dead hangs or farmer’s carries | 3 × 10–12 each |
| Day 3 (optional full body) | Bodyweight circuit: squats, push-ups, step-ups, rows, core work | 2–3 rounds |
No gym? No problem. Resistance bands, a pair of dumbbells, or just your body weight will get the job done. The goal is progressive overload over time — gradually increasing weight, reps, or difficulty.
Cardio: Helpful, but Secondary
Walking is the best starting point. Aim for 7,000–10,000 steps per day, built up gradually. Post-meal walks are especially valuable on GLP-1s — they help with digestion, blood sugar regulation, and reduce that “too full” feeling.
Target 150 minutes per week of moderate cardio per standard health guidelines. But if you have to choose between a 30-minute walk and a 30-minute strength session on a time-crunch day, choose the weights. Muscle preservation is harder to undo than missed cardio.
Exercise Timing Around Injection Day
- Injection day: Light activity only. A walk is fine. Don’t push it.
- Day after injection: If you feel okay, light strength training or walking. Listen to your body.
- Days 3–6: Your best training window. Schedule harder sessions here.
- Dose increase weeks: Treat it like your first week again — dial back intensity for 2–3 days.
- General rule: Avoid intense exercise within 60 minutes of injection. Increased blood flow can accelerate absorption and worsen nausea.
For the full protocol, see our GLP-1 muscle preservation guide.
Sources: Jastreboff et al. (2022), SURMOUNT-1 body composition data; ECO 2025 study on fat loss with lean mass preservation; Jensen et al. (2024), exercise + GLP-1 maintenance study; Mass General Brigham lean body mass review; American College of Sports Medicine guidelines
What Does the First 30 Days on a GLP-1 Look Like?
Nobody can tell you exactly how YOUR first month will go. But after reviewing clinical trial timelines, prescribing information, and thousands of real-world reports, here’s the pattern most beginners follow. Use this as a roadmap, not a rulebook.
First 48 Hours
What’s happening: Your body is meeting the medication for the first time. Semaglutide and tirzepatide have long half-lives, so effects build gradually.
What to expect: Most people feel relatively normal on injection day. By 12–24 hours, you might notice slightly reduced appetite. Some people feel mild nausea or fatigue by hour 24–48.
What to do: Eat your normal meals (lighter than usual). Hydrate aggressively. Don’t plan anything strenuous. Have ginger tea and bland food options ready just in case.
Week 1
What’s happening: Side effects — if they’re going to appear — usually peak between days 2–4. Your appetite is noticeably reduced. “Food noise” starts quieting for many people.
What to expect: Mild to moderate nausea (not everyone gets this), possible fatigue, possible constipation starting, reduced appetite. You probably won’t feel hungry at your usual meal times.
What to do: Small protein-forward meals 4–5 times a day. Hydrate. Walk daily. Track what you eat and how you feel — this data is gold for understanding your body’s patterns.
Weight change: 0–3 lbs, mostly from eating less food volume and water fluctuation. Don’t read too much into the scale yet.
Weeks 2–3
What’s happening: Side effects are fading for most people. Your new eating patterns are becoming more natural. You’re learning what “satisfied” feels like versus “full.”
What to expect: Better GI tolerance, clearer appetite signals, more energy, less food-obsessed thinking.
What to do: Refine your protein intake — are you consistently hitting 25–35g per meal? Establish your strength training routine if you haven’t already. Increase fiber gradually.
Weight change: 2–5 lbs from start. The trend matters more than any single weigh-in.
Week 4 (Dose Increase Week)
What’s happening: Most GLP-1 protocols call for your first dose increase around week 4. This often brings a milder version of week 1 side effects for a few days.
What to expect: A temporary return of nausea, possible fatigue, possibly reduced appetite. Usually less intense than the first dose.
What to do: Treat it like injection week 1 again. Go bland, go small, hydrate extra. Don’t schedule the dose increase during a vacation or big work week if you can help it.
Weight change: 4–8 lbs from start is typical, but highly variable. If you’re not losing, don’t panic — some people are slow starters.
The “Normal vs. Not Normal” Check
| Normal Adjustment (Ride It Out) | Contact Your Prescriber | Urgent Care / ER |
|---|---|---|
| Mild nausea for 2–4 days | Nausea lasting more than 7 days at a stable dose | Can’t keep fluids down for 12+ hours |
| Reduced appetite | Eating under 800 calories daily for 3+ days | Severe abdominal pain radiating to back |
| Mild fatigue for 1–2 weeks | Fatigue that doesn’t improve after 3 weeks | Signs of severe dehydration (confusion, no urine) |
| Constipation that responds to fiber/water | Constipation with severe pain for 5+ days | Allergic reaction (hives, swelling, breathing difficulty) |
| Occasional headache | Persistent headaches not helped by hydration | Vision changes, chest pain |
How Does Dose Escalation Work?
All GLP-1 medications start low and increase gradually. This is called titration — and it exists to minimize side effects and let your body adapt. Here’s what the schedule looks like for each medication.
Dose Escalation by Medication
| Medication | Week 1–4 | Week 5–8 | Week 9–12 | Week 13–16 | Week 17+ |
|---|---|---|---|---|---|
| Wegovy (semaglutide injection) | 0.25mg | 0.5mg | 1.0mg | 1.7mg | 2.4mg (maintenance) |
| Wegovy tablets (semaglutide oral) | Days 1–30: 1.5mg daily | Days 31–60: 4mg daily | Days 61–90: 9mg daily | Day 91+: 25mg daily (maintenance) | — |
| Ozempic (semaglutide) | 0.25mg | 0.5mg | 1.0mg (optional increase) | 2.0mg (if needed) | — |
| Zepbound/Mounjaro (tirzepatide) | 2.5mg | 5mg | 7.5mg | 10mg | 12.5mg → 15mg |
Key Things to Know
- Each dose increase can bring a temporary return of side effects — usually milder than the first dose. Plan accordingly.
- You don’t have to reach the highest dose. If you’re losing weight and tolerating a lower dose well, your prescriber may keep you there.
- If side effects are too much at a new dose, your prescriber can hold you at the current level for an extra 4 weeks before trying again. This is normal and common.
- Never adjust doses on your own. Splitting pens, “microdosing,” or skipping escalation steps without your prescriber’s guidance leads to inconsistent blood levels and unpredictable results.
If You Miss a Dose (Follow Your Label)
| Medication | What FDA Labeling Says |
|---|---|
| Wegovy injection | Take as soon as possible if next scheduled dose is more than 2 days (48 hours) away. Otherwise skip and resume on your regular day. |
| Wegovy tablets | If missed, skip that day’s dose and take the next dose the following day. Don’t double up. |
| Zepbound | Take within 4 days (96 hours) of the missed dose. If more than 4 days have passed, skip it and take the next scheduled dose. |
| Mounjaro | Take within 4 days (96 hours) of the missed dose. If more than 4 days, skip and resume schedule. Do not take 2 doses within 3 days of each other. |
| Ozempic | Take within 5 days of the missed dose. If more than 5 days, skip and resume your regular schedule. |
Never take two doses to make up for a missed one.
Sources: FDA prescribing information (dosage and administration sections) for Wegovy, Ozempic, Zepbound, Mounjaro
Lifestyle: Sleep, Alcohol, Travel, Surgery, and Social Situations
Hydration — The Habit That Fixes Half Your Problems
GLP-1s reduce your thirst signal alongside your hunger signal. You will not feel thirsty when you need water.
Target: 80–100 oz per day. More if you’re active or in a hot climate. How: Keep a large water bottle in your line of sight all day. Set phone reminders. Drink a full glass before every meal. Add lemon, cucumber, or electrolyte packets if plain water is unappealing.
Dehydration is the silent amplifier of almost every side effect — nausea, constipation, headaches, fatigue, dizziness. Fix your hydration and half your symptoms may resolve on their own. For more, see our GLP-1 constipation relief guide.
Sleep Matters More Than You Think
Poor sleep increases ghrelin (your hunger hormone) and decreases leptin (your fullness hormone), directly undermining what the GLP-1 is trying to do.
Target: 7–9 hours per night, consistent bedtime. Tips: No screens for 60 minutes before bed. Cool, dark room. Limit caffeine after 2 PM. If your GLP-1 causes insomnia or vivid dreams, try shifting your injection time.
Alcohol
Not forbidden, but understand the tradeoffs:
- Your tolerance is lower. Many GLP-1 users report feeling the effects of alcohol faster and stronger.
- Nausea is amplified. Alcohol + GLP-1 = a bad combination, especially in the first 4 weeks and dose increase weeks.
- Hypoglycemia risk increases, especially if you’re on diabetes medications too.
- Empty calories. A glass of wine is fine occasionally. But every drink is calories your reduced intake can’t afford.
If you choose to drink: Eat protein first. Limit to 1–2 drinks. Alternate with water. Avoid sugary mixers. Consider skipping it entirely during the first month and dose increase weeks.
Traveling With GLP-1 Medications
- Carry-on only. Never check your medication — cargo hold temperatures fluctuate.
- TSA allows injectable medications and needles in carry-on. Bring your prescription label.
- Storage: Unopened pens: refrigerate (36–46°F). In-use pens: room temperature up to 86°F for the timeframe specified by your brand (ranges from 21 to 56 days). Use a small insulated travel case with a cool pack for longer trips.
- Time zones: Take your weekly shot at your usual time in your home time zone initially, then adjust gradually.
Before Surgery or Medical Procedures
This is a safety issue, not a preference. GLP-1 medications delay gastric emptying, which means food and liquid can remain in your stomach longer than expected. Under anesthesia, this creates aspiration risk — inhaling stomach contents into your lungs.
Current multi-society guidance (including ASA, AGA, ASMBS, and SAGES, released October 2024) says most patients can continue GLP-1 medications before elective surgery. However, people at higher risk for delayed stomach emptying — such as those during dose escalation, experiencing significant GI symptoms, or on higher doses — may be asked to follow additional precautions. These can include a 24-hour liquid diet before the procedure, modifications to the anesthesia plan, or in rare cases, rescheduling.
The non-negotiable part: Always tell your surgeon and anesthesiologist that you’re on a GLP-1 medication, even for procedures you consider “minor.” Follow the specific plan your surgical team gives you based on your individual risk.
Sources: Multi-society clinical practice guidance on perioperative GLP-1RA use (ASA, AGA, ASMBS, ISPCOP, SAGES, 2024); FDA prescribing information
Social Situations and Eating Out
You’re going to eat less in front of people who notice. A few things that help:
- You don’t owe anyone a medical explanation. “I’m not super hungry” or “I ate earlier” works fine.
- Restaurant strategy: Order appetizer portions or split an entrée. Focus on protein options. Ask for a to-go box at the start and pack half before you eat.
- Holidays and gatherings: Eat a protein-rich snack before you arrive. Focus on the socializing, not the buffet. Nobody is watching your plate as closely as you think.
What Happens If You Stop?
The data is clear: weight regain is common after stopping GLP-1 medications. Studies show roughly two-thirds of people regain most of the weight within a year of discontinuation.
The insurance policy: The muscle you built and the habits you established while ON the medication. People who maintained strength training and dietary habits fared significantly better than those who relied on the medication alone (Jensen et al., 2024).
If you’re considering stopping, discuss a tapering and maintenance plan with your prescriber rather than stopping cold turkey. For more, see our guide on what happens when you stop taking GLP-1.
“Supplements That Increase GLP-1” — What’s Legit vs. Hype
This question is all over the search results, so let’s be straight with you.
What People Mean When They Search This
Usually one of two things: “I want appetite control without a prescription medication” or “I’m already on a GLP-1 and want to boost my results.”
What Actually Has Evidence Behind It
These aren’t “GLP-1 supplements” — they’re dietary and lifestyle factors that support your body’s natural GLP-1 production. They won’t replace medication, but they can complement it:
- Protein at every meal. Protein stimulates GLP-1 release. This is well-established and one reason protein-first eating is so effective on GLP-1 medications.
- Fiber (especially soluble fiber). Fiber is fermented by gut bacteria into short-chain fatty acids that may promote GLP-1 secretion. Sources: oats, beans, lentils, chia seeds, berries.
- Probiotic and fermented foods. A healthy gut microbiome supports GLP-1 signaling. Yogurt, kefir, sauerkraut, kimchi.
- Healthy fats in moderation. Monounsaturated and omega-3 fats (olive oil, avocado, fatty fish) can stimulate GLP-1 release.
- Meal order. Eating protein and vegetables before carbohydrates leads to greater GLP-1 release than eating carbs first — same food, different order, different hormonal response.
- Regular exercise. Both aerobic and resistance exercise improve GLP-1 sensitivity.
- Adequate sleep. Sleep deprivation disrupts appetite hormone signaling, including GLP-1.
What to Avoid
Any product marketed as a “GLP-1 supplement” or “natural Ozempic.” There is no over-the-counter supplement that replicates what prescription GLP-1 agonists do. The mechanism isn’t comparable. These products are marketing, not medicine.
Anything claiming to be semaglutide or tirzepatide without a prescription. These are prescription medications. If someone is selling them without a legitimate medical evaluation, that is a red flag — full stop.
“Research peptides” or gray-market GLP-1 compounds. Unregulated, untested for purity or dose accuracy, and potentially dangerous. The FDA has issued specific warnings about unapproved GLP-1 products.
Can You “Make GLP-1 at Home”?
This question comes up in search results, so we’ll answer it directly: No, you cannot make prescription GLP-1 medications at home. These are complex molecules manufactured under strict pharmaceutical conditions.
What you can do is support your body’s own GLP-1 production through the diet and lifestyle strategies above. That’s real, evidence-based, and helpful — but it will not produce the same magnitude of effect as prescribed medication.
Supplements Worth Considering on GLP-1
Reduced food intake can create nutritional gaps. These supplements are commonly recommended by prescribers for GLP-1 patients:
| Supplement | Why It Helps | Notes |
|---|---|---|
| Daily multivitamin | Covers micronutrient gaps from reduced food intake | Choose a quality brand with iron and B12 |
| Vitamin D | Commonly deficient; supports bone health and immune function | 2,000–4,000 IU/day typical; test levels if possible |
| Magnesium citrate | Helps with constipation, muscle cramps, and sleep | 200–400mg at bedtime; start low |
| Fiber supplement | Psyllium husk (Metamucil) if dietary fiber is insufficient | Ramp slowly; take with plenty of water |
| Electrolytes | Prevents headaches, dizziness, and fatigue | LMNT, Liquid IV, or similar; especially first few weeks |
| Protein powder | Helps meet protein targets when appetite is very low | Whey, casein, or plant-based; 25–30g per scoop |
Always discuss supplements with your prescriber, especially if you take other medications. If you’re on oral semaglutide tablets, take supplements separately (30+ minutes after the tablet).
Sources: Ohio State Health & Discovery; NIH dietary supplement fact sheets; FDA safety communications on unapproved GLP-1 products
Brand-Name vs. Compounded GLP-1 Medications: What Beginners Need to Know
This is where a lot of beginners get confused — and where we see the most misleading information online. We’re going to give you the facts without spin.
What “Compounded” Means
Compounded medications are prepared by compounding pharmacies, often when there’s a shortage of the FDA-approved brand-name product. They are not FDA-approved — meaning they haven’t gone through the same rigorous testing for safety, efficacy, and manufacturing consistency that branded products have.
That doesn’t automatically mean they’re dangerous. But it does mean the regulatory framework is different, and buyers need to do more due diligence. For an in-depth look, see our guide on compounded semaglutide safety.
FDA’s Specific Concerns
- The FDA has warned about unapproved GLP-1 drugs used for weight loss, including products using semaglutide salt forms (like semaglutide sodium or semaglutide acetate) that are different active ingredients than what’s in FDA-approved products. These have not been shown to be safe or effective.
- The FDA has stated that companies cannot legally claim compounded products are “generic” versions of FDA-approved drugs or suggest they’re therapeutically equivalent.
- There have been reports of adverse events associated with compounded GLP-1 products.
How to Reduce Your Risk If Considering Compounded Options
If cost makes brand-name medications inaccessible and you’re exploring compounded alternatives with your healthcare provider:
- Verify the pharmacy is state-licensed and accredited (look for PCAB accreditation or state board of pharmacy licensing)
- Use the FDA’s BeSafeRx program to check online pharmacy legitimacy
- Ask your provider what form of semaglutide the pharmacy uses — base form versus salt forms matter
- Be wary of any provider or pharmacy using language that implies their compounded product is equivalent to the brand-name version
- Compounded products should still come with proper labeling, storage instructions, and a pathway to report adverse events
We are not in a position to tell you whether a compounded product is right for you — that’s a conversation with your prescribing provider. What we can tell you is that doing the due diligence above materially reduces risk.
Sources: FDA safety communication on unapproved GLP-1 drugs (fda.gov); FDA BeSafeRx program; FDA press announcements on compounded GLP-1 enforcement
How Much Do GLP-1 Medications Cost — and How Do You Afford Them?
Let’s talk numbers.
Brand-name retail pricing: Wegovy, Zepbound, Ozempic, and Mounjaro list at roughly $1,000–$1,400/month without insurance. Yes, really.
With insurance: Coverage is expanding rapidly. Many commercial plans now cover Wegovy and Zepbound for patients meeting BMI criteria (≥30, or ≥27 with a weight-related condition). Copays with insurance range from $0 to $500/month depending on your plan. Prior authorization is usually required.
Manufacturer savings programs: Both Novo Nordisk (Wegovy/Ozempic) and Eli Lilly (Zepbound/Mounjaro) offer copay assistance cards that can reduce out-of-pocket costs significantly for commercially insured patients.
Telehealth providers with flat monthly pricing: Many online providers offer GLP-1 programs at $150–$350/month, typically including the medication and medical supervision. Availability and medication options vary by state and current supply.
HSA/FSA: Prescribed GLP-1 medications for weight loss are generally HSA and FSA eligible.
Medicaid: Coverage varies widely by state. Some state Medicaid programs cover anti-obesity medications; many don’t yet.
The Real Cost Conversation
The medication itself is one cost. But factor in: fewer takeout meals (you’re eating less), fewer snacks, potentially lower medical costs over time if weight-related conditions improve. We’re not saying it’s cheap — it’s not. But the net financial picture is more nuanced than the sticker price.
For a deep dive into pricing, see our complete GLP-1 cost guide.
How Do You Get Started Safely?
Whether you go through your primary care doctor, an endocrinologist, or a telehealth provider, a legitimate GLP-1 program should include:
- A real medical evaluation — health history, current medications, contraindication screening
- Lab work when appropriate (metabolic panel, A1C if relevant, thyroid function)
- A clear treatment plan with dose escalation schedule
- Follow-up appointments — at minimum at 4, 8, and 12 weeks
- Access to your prescriber for questions and side effect management
What Sketchy Programs Look Like
- No medical history review or contraindication screening
- No follow-up visits or check-ins
- Unclear or unnamed pharmacy sources
- Pricing that seems dramatically lower than everyone else (if it sounds too good to be true...)
- They can’t tell you exactly what medication, dose, and form you’re getting
- No mention of potential risks or side effects
Trust signal: If a program’s website is all before/after photos and no medical disclaimers, treat that as a yellow flag.
We help you compare providers so you don’t have to guess. See our provider comparison based on verified pricing, pharmacy sources, and program features. For the fastest options, see our fast shipping GLP-1 comparison.
Not Sure Where to Start?
Our eligibility quiz takes about 2 minutes and matches you with vetted telehealth providers based on your state, insurance status, budget, and medication preference. No pressure, no sales pitch — just the information you need to make a decision.
Check Your Eligibility & Find a ProviderFree assessment • No commitment • Takes ~2 minutes
The 10 Beginner Mistakes That Cause Plateaus or Quitting
We see these patterns over and over. Avoid them and you’re ahead of most people.
#1: Not eating enough protein. This is mistake #1 for a reason. Inadequate protein → muscle loss → slower metabolism → plateau → frustration → quitting.
#2: Ignoring constipation until it’s a crisis. Prevent it from day one. Don’t wait until you haven’t gone in a week.
#3: Overeating on “good days.” Your appetite fluctuates. On days you feel more hungry, it’s tempting to eat everything. The medication didn’t stop working — your body is just cycling. Stick to your routine.
#4: Drinking alcohol in the first month. The nausea combo isn’t worth it. Give your body a chance to adjust first.
#5: Expecting linear weight loss. Weight loss is not a straight line. It’s a jagged downward trend with plateaus, water retention spikes, and weeks where nothing happens. Look at the 4-week trend, not the daily scale.
#6: Not planning dose increase weeks. They sneak up on people. Mark your calendar. Stock bland food. Don’t schedule them during stressful periods.
#7: Skipping strength training. We know. You’re tired. You’re nauseous. But even two 20-minute sessions per week makes a measurable difference in body composition. The muscle you save now is muscle you don’t have to rebuild later.
#8: Not planning medication refills. Supply chain issues, prior authorization delays, and pharmacy stock-outs are real. Start the refill process a week before you need it.
#9: Trying internet “hacks” without your prescriber. Microdosing, dose-splitting, skipping escalation, combining supplements — run everything by your prescriber first. Your treatment plan exists for a reason.
#10: Comparing your timeline to someone else’s. That person on Reddit who lost 20 lbs in their first month has a completely different starting weight, metabolism, medication, dose, activity level, and genetic profile than you. Your pace is your pace.
What to Ask Your Prescriber (Copy These Questions)
Your prescriber visit is short. Don’t waste it on questions you can look up. Ask the things that only your prescriber can answer for YOUR situation:
- 1“What side effects should I expect with each dose increase — and when should I call you?”
- 2“What symptoms mean I should stop the medication and contact you immediately?”
- 3“Does this interact with any of my current medications?”
- 4“If I’m on tirzepatide, do I need backup contraception during dose escalation?”
- 5“I have [upcoming surgery/dental procedure/colonoscopy] — when should I stop the medication?”
- 6“Should I get bloodwork done before starting, and at what intervals after?”
- 7“What’s your approach if I hit a weight loss plateau — stay at this dose, increase, or investigate other factors?”
- 8“How long do you typically keep patients on this medication?”
- 9“If I experience nausea that’s affecting my daily life, what’s your protocol — hold the dose, adjust timing, or add an anti-nausea medication?”
- 10“What’s the plan if this medication isn’t covered by my insurance or becomes unavailable?”
Print this list. Bring it to your appointment. You’ll thank yourself.
Important Safety Information
GLP-1 receptor agonists are prescription medications with potential side effects. This guide is educational and should not replace professional medical advice.
- • Always follow your prescriber’s specific instructions — they know your medical history
- • GLP-1 medications are not appropriate for everyone. Contraindications include personal or family history of medullary thyroid carcinoma (MTC) or Multiple Endocrine Neoplasia syndrome type 2 (MEN 2)
- • If you experience any red flag symptoms, seek medical attention immediately
- • Do not share or adjust medication dosing without prescriber guidance
- • For complete safety information, refer to the FDA-approved prescribing information for your specific medication
Compounded medications are pharmacy-prepared formulations that are not FDA-approved and have not been reviewed by the FDA for safety, effectiveness, or quality.
How We Built This Guide
This page was compiled by the WPG Research Team using primary sources including FDA prescribing information (Wegovy, Ozempic, Zepbound, Mounjaro), published clinical trial data (STEP 1–4, SURMOUNT 1–2, SELECT), medical society guidelines (ASA, American Society for Nutrition, Obesity Medicine Association), FDA safety communications, and clinical guidance from Cleveland Clinic, Ohio State Health & Discovery, and Mass General Brigham.
All medical claims are cited to their source. Pricing and availability information is verified as of the date shown above and updated regularly.
This guide does not constitute medical advice. Always consult your healthcare provider before starting or changing any medication.
References
- FDA Prescribing Information: Wegovy (semaglutide) — accessdata.fda.gov
- FDA Prescribing Information: Zepbound (tirzepatide) — accessdata.fda.gov
- FDA Prescribing Information: Ozempic (semaglutide) — accessdata.fda.gov
- FDA Prescribing Information: Mounjaro (tirzepatide) — accessdata.fda.gov
- Wilding JPH et al. (2021). “Once-Weekly Semaglutide in Adults with Overweight or Obesity.” New England Journal of Medicine, 384(11), 989–1002. (STEP 1)
- Jastreboff AM et al. (2022). “Tirzepatide Once Weekly for the Treatment of Obesity.” New England Journal of Medicine, 387(3), 205–216. (SURMOUNT-1)
- Lincoff AM et al. (2023). “Semaglutide and Cardiovascular Outcomes in Obesity without Diabetes.” New England Journal of Medicine, 389(24), 2221–2232. (SELECT)
- Multi-Society Clinical Practice Guidance on Perioperative Use of GLP-1 Receptor Agonists (2024). ASA, AGA, ASMBS, ISPCOP, SAGES. Surgical Endoscopy, 39, 180–183.
- Mozaffarian D et al. (2025). “Nutritional Priorities to Support GLP-1 Therapy for Obesity.” Joint Advisory: ACLM, ASN, OMA, TOS. The American Journal of Clinical Nutrition.
- Jensen SBK et al. (2024). “Healthy Weight Loss Maintenance with Exercise, GLP-1 Receptor Agonist, or Both Combined.” The Lancet.
- FDA Safety Communication: “FDA’s Concerns with Unapproved GLP-1 Drugs Used for Weight Loss” — fda.gov
- FDA BeSafeRx: Online Pharmacy Safety — fda.gov/besaferx
- Cleveland Clinic: “GLP-1 Diet: What to Eat & Avoid” — clevelandclinic.org
- Ohio State Health & Discovery: “Nutrition Plan When on GLP-1 Medication” — health.osu.edu
- European Congress on Obesity 2025: Body composition study (fat loss with lean mass preservation under supervised care)
Frequently Asked Questions: GLP-1 Tips for Beginners
Frequently Asked Questions
Continue Your Research
How to Take GLP-1 Safely
Complete safety guide with dosing, interactions, and monitoring
Prevent Muscle Loss on GLP-1
Evidence-based muscle preservation protocol
Best GLP-1 Online Programs
Top telehealth providers compared and ranked
GLP-1 Cost With and Without Insurance
Full cost breakdown and affordability options
Is Compounded Semaglutide Safe?
FDA concerns, pharmacy verification, and safety checklist
What Happens When You Stop GLP-1
Evidence on weight regain and maintenance strategies