GLP-1 for Prediabetes: What Works, What’s Approved, and What to Do Next
Disclosure: Some links on this site are affiliate links. If you purchase through these links, we may earn a commission at no extra cost to you. Thank you for supporting our site.·For informational purposes only—not medical advice.
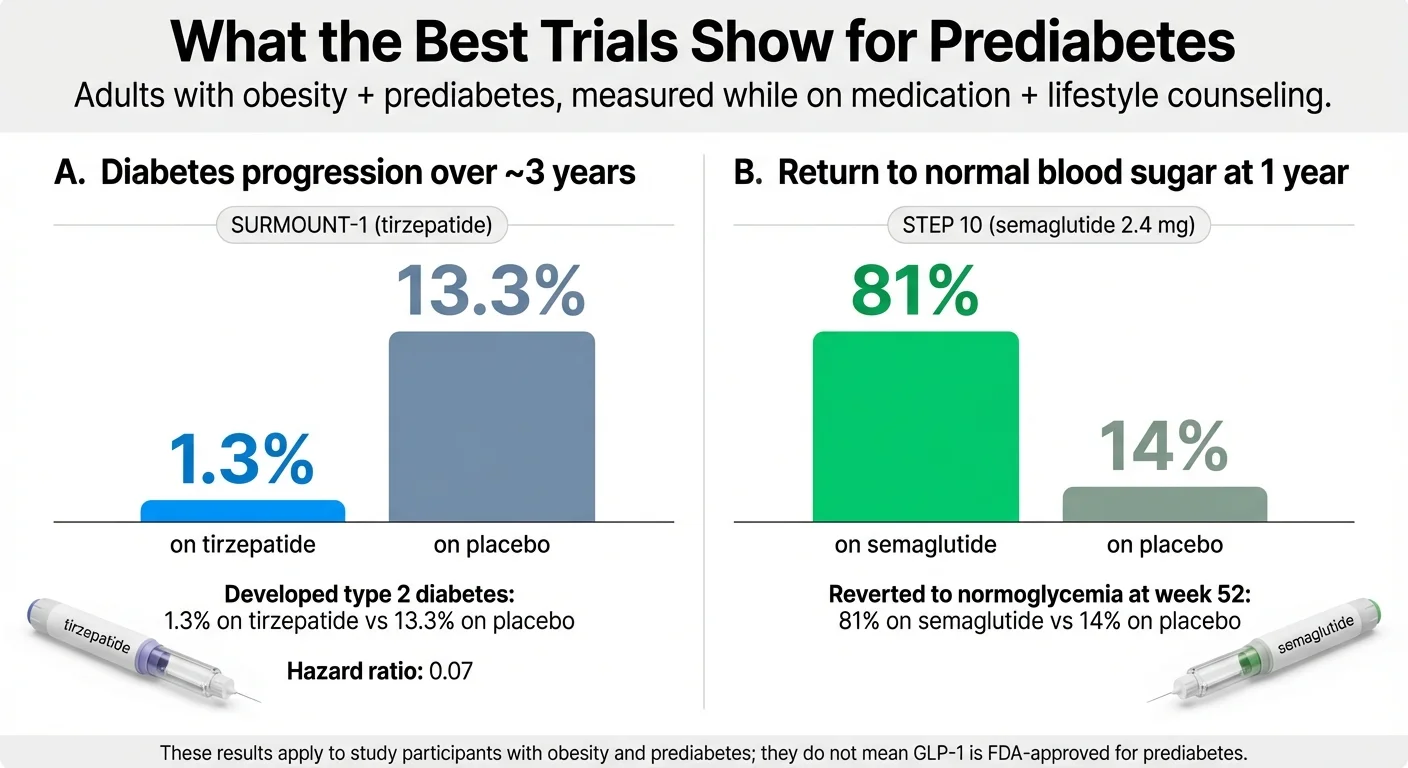
GLP-1 medications are not FDA-approved specifically to treat prediabetes. But the clinical evidence is hard to ignore — in one 3-year trial, tirzepatide (the drug behind Mounjaro and Zepbound) reduced the risk of progressing from prediabetes to type 2 diabetes by about 93%: just 1.3% of people on tirzepatide developed diabetes versus 13.3% on placebo (Jastreboff et al., NEJM, 2025). In a separate trial, 81% of people with prediabetes on semaglutide returned to normal blood sugar at one year, compared to 14% on placebo (McGowan et al., Lancet Diabetes Endocrinol, 2024).
That’s a dramatic signal. And it’s why more doctors — and more people with prediabetes — are having this conversation right now.
But there’s a catch. Because GLP-1s aren’t approved for prediabetes on their own, getting one prescribed (and covered by insurance) usually depends on whether you also qualify under obesity or weight management criteria. And the cost without insurance can run anywhere from $149 to over $1,000 a month.
We built this guide to answer every question that follows: Does the science hold up? Who actually qualifies? How much will it cost you specifically? Is it safer than waiting? And what’s the smartest next step — whether that’s a GLP-1 (also written GLP 1), metformin, or a lifestyle change program?

If You’re Short on Time, Start Here
| Question | Quick Answer |
|---|---|
| Is any GLP-1 FDA-approved for prediabetes? | No. But several are approved for obesity/overweight — which many people with prediabetes also have. |
| Can GLP-1s prevent type 2 diabetes? | Clinical trials show 72–93% reduced risk in people with prediabetes + obesity. |
| Who benefits most? | People with prediabetes who also have obesity (BMI ≥30) or overweight (BMI ≥27) with a related health condition. |
| Biggest downside? | Cost and access. Insurance rarely covers it for prediabetes alone. Side effects (mostly GI) are common but usually manageable. |
| Best first step? | Know your numbers (A1C, BMI, comorbidities), then talk to your doctor with specific questions. We give you the list below. |
Now, the full picture.
What Is Prediabetes — and Why Is Everyone Suddenly Talking About GLP-1s?
If you just got lab results that say “prediabetes,” you’re not alone. CDC estimates that more than 2 in 5 U.S. adults — 115.2 million people — have prediabetes. And 8 in 10 of them don’t know it.
Here’s what it means in simple terms: your blood sugar is higher than normal, but not high enough to be type 2 diabetes. Specifically:
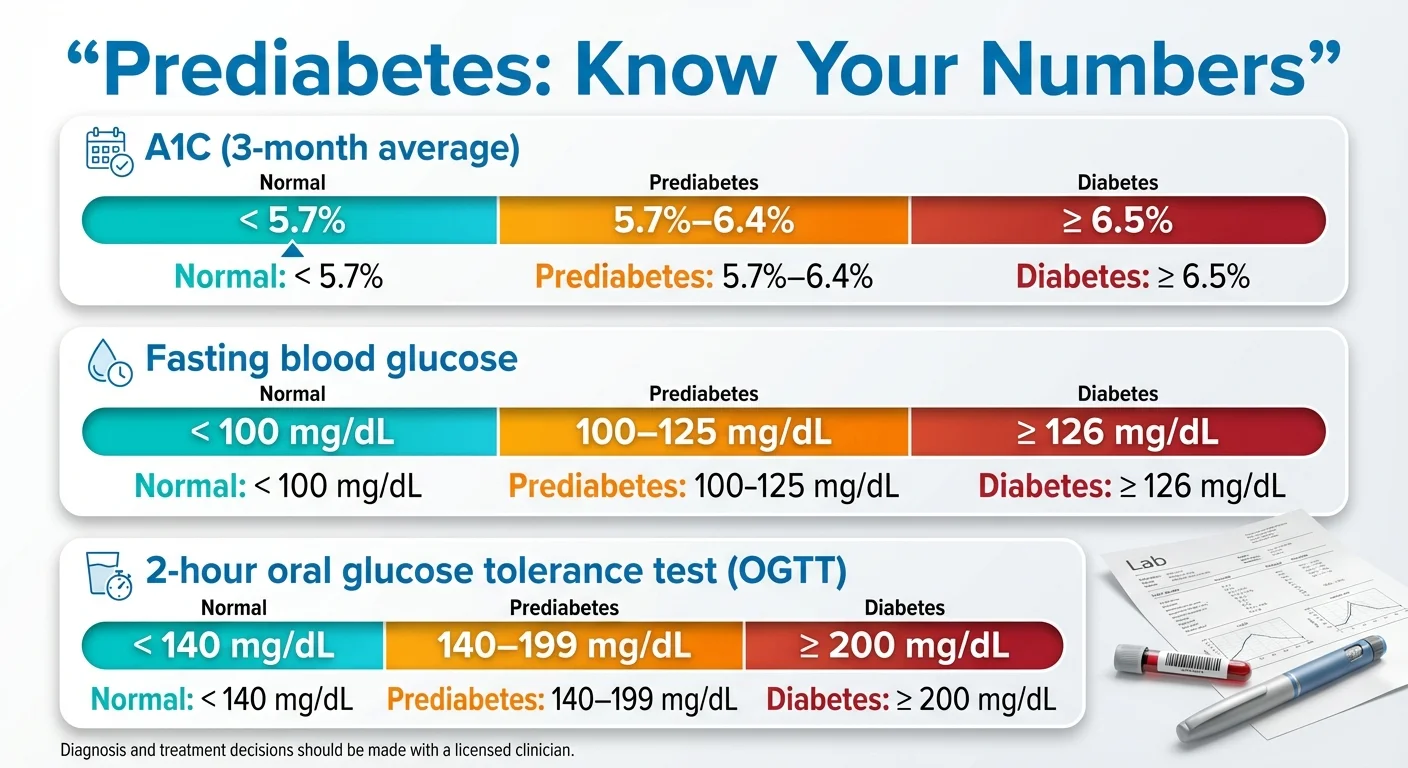
| Test | Normal | Prediabetes | Type 2 Diabetes |
|---|---|---|---|
| A1C (3-month blood sugar average) | Below 5.7% | 5.7% – 6.4% | 6.5% or higher |
| Fasting blood sugar | Below 100 mg/dL | 100 – 125 mg/dL | 126 mg/dL or higher |
| Oral glucose tolerance test (2-hour) | Below 140 mg/dL | 140 – 199 mg/dL | 200 mg/dL or higher |
Source: American Diabetes Association, Standards of Care 2025
Prediabetes matters because without intervention, a significant portion of people with prediabetes will develop type 2 diabetes. But here’s the important part: prediabetes is reversible. This is the window where your insulin system is struggling but not broken — and the right intervention can pull you back.
The Traditional Playbook
For decades, the standard approach has been:
- Lifestyle changes first — diet, exercise, weight loss. The landmark Diabetes Prevention Program (DPP) study showed that structured lifestyle changes reduced diabetes risk by 58% over roughly three years.
- Metformin if lifestyle alone isn’t enough — the same study showed metformin reduced risk by 31%. It’s the only medication the American Diabetes Association (ADA) specifically recommends for diabetes prevention in high-risk prediabetes.
That playbook still holds. But there’s a problem buried in the data.
Why GLP-1s Entered the Conversation
In the DPP study, only 38% of people in the lifestyle group maintained their weight loss long-term. Medication adherence with metformin was better (~70%), but the risk reduction was more modest.
Then the GLP-1 trial data started rolling in — and the numbers were different.
Tirzepatide in the SURMOUNT-1 extension trial: ~93% reduction in diabetes progression over three years in people with obesity and prediabetes. Semaglutide across the STEP program: 81% of people with prediabetes achieved normal blood sugar at one year.
Those results changed the conversation. And with the Wegovy pill (oral semaglutide 25mg) launching in January 2026 as the first oral GLP-1 for weight management, the practical barriers to access started shifting too.
Add Medicare now exploring expanded GLP-1 coverage through new payment models, and you start to see why more people with prediabetes are asking about GLP-1s right now.
Do GLP-1s Actually Work for Prediabetes? Here’s What the Trials Show
This is the section where we earn your trust or lose it. No cherry-picked headlines. Here’s what the research actually says — the good, the limitations, and the uncertainties.
The SURMOUNT-1 Long-Term Data (Tirzepatide)
This is the strongest single piece of evidence for GLP-1s in prediabetes.
The SURMOUNT-1 trial enrolled adults with obesity (or overweight with at least one comorbidity) who did not have type 2 diabetes. Among the 1,032 participants who had prediabetes at the start of the study, researchers extended the trial to 176 weeks (about 3.4 years) to see what happened to their blood sugar.
Results: Tirzepatide reduced the risk of progressing from prediabetes to type 2 diabetes by about 93% compared to placebo. Just 1.3% of participants on tirzepatide developed type 2 diabetes, versus 13.3% on placebo (hazard ratio 0.07). After a 17-week off-treatment period, the numbers were 2.4% vs. 13.7% — meaning most of the benefit held even briefly after stopping. Average weight loss was approximately 12–20% of body weight depending on dose.
Limitation: These were people with both prediabetes and obesity/overweight. We don’t know if the results apply equally to someone with prediabetes at a normal weight.
Source: Jastreboff et al., N Engl J Med 2025; 392(10):958-971; PMID 39536238
The STEP Trials (Semaglutide)
The STEP program tested semaglutide 2.4mg (the dose used in Wegovy) across multiple trials for obesity. A pooled analysis looked specifically at participants who had prediabetes at baseline.
Results: In the pooled STEP 1, 3, and 4 trials, people with baseline prediabetes who received semaglutide showed significantly higher rates of returning to normal blood sugar (normoglycemia) compared to placebo (Perreault et al., Lancet Diabetes Endocrinol, 2023).
STEP 10 went further — it was specifically designed for adults with obesity and prediabetes. At 52 weeks, 81% of participants on semaglutide achieved normoglycemia, versus 14% on placebo (McGowan et al., Lancet Diabetes Endocrinol, 2024).
The Liraglutide SCALE Data
Before semaglutide and tirzepatide dominated the headlines, liraglutide (Saxenda) was tested in a 3-year trial in adults with obesity and prediabetes.
Results: Liraglutide reduced new-onset type 2 diabetes by 79% compared to placebo over three years. But there was a catch — when people stopped the medication, some of the benefit faded over time.
Source: le Roux et al., The Lancet, 2017
The 2024 Meta-Analysis (All GLP-1s Combined)
A systematic review published in June 2024 pooled data from 12 randomized controlled trials involving 4,316 patients with prediabetes.
Results: GLP-1 receptor agonists significantly increased reversion to normal blood sugar (risk ratio 1.76 — a 76% higher likelihood than control groups) and reduced new-onset diabetes by 72% (risk ratio 0.28). They also improved A1C, fasting glucose, body weight, waist circumference, triglycerides, and LDL cholesterol. Gastrointestinal side effects were more common in the GLP-1 groups.
Conclusion from the researchers: “GLP-1RAs combined with lifestyle modification proved to be a more effective therapy for managing prediabetic patients than lifestyle modification alone, with a tolerable safety profile.”
Source: Salamah et al., Diabetol Metab Syndr, 2024
The OASIS 4 Data (Oral Semaglutide)
A post-hoc analysis of the OASIS 4 trial — which tested the new Wegovy pill (oral semaglutide 25mg) — found that 71.1% of participants with prediabetes at baseline achieved normal blood glucose, compared to 33.3% on placebo.
This matters because it shows the oral pill can move the needle for prediabetes too, not just the injection.
Source: Novo Nordisk, OASIS 4 post-hoc analysis, 2025
Evidence Summary Table
| Medication / Trial | Population | Duration | Key Prediabetes Result | Weight Loss |
|---|---|---|---|---|
| Tirzepatide (SURMOUNT-1 extension) | Obesity + prediabetes | 176 weeks | ~93% reduced progression to T2D (1.3% vs 13.3%); ~98% stayed diabetes-free on treatment | ~12–20% body weight |
| Semaglutide 2.4mg (STEP 10) | Obesity + prediabetes | 52 weeks | 81% achieved normal blood sugar (vs. 14% placebo) | ~13% body weight |
| Semaglutide 2.4mg (STEP pooled) | Obesity ± prediabetes | 52–68 weeks | Significantly higher normoglycemia rates vs. placebo | ~15% body weight |
| Oral semaglutide 25mg (OASIS 4) | Obesity ± prediabetes | 64 weeks | 71% normalized blood sugar (vs. 33% placebo) | ~13–17% body weight |
| Liraglutide (SCALE) | Obesity + prediabetes | 3 years | 79% reduced new-onset T2D | ~6–8% body weight |
| All GLP-1s (Salamah et al., 2024 meta-analysis) | 4,316 patients, 12 trials | Varied | RR 1.76 for normoglycemia; RR 0.28 for new T2D | Significant across studies |
None of these medications are FDA-approved for prediabetes specifically. Evidence strength is based on trial size, duration, and prediabetes-specific outcomes.
What’s Still Uncertain
We want to be straight with you about what the evidence doesn’t prove yet:
- Long-term durability after stopping. Most benefits were measured while people were on medication. Weight regain and blood sugar changes after discontinuation are real concerns (more on this later).
- Normal-weight prediabetes. Almost all trial participants had obesity or overweight. If you have prediabetes at a normal BMI, the evidence base for GLP-1s is much thinner.
- Lab improvements vs. hard outcomes. “Returned to normal A1C” is encouraging, but we have less long-term data on whether this translates to fewer heart attacks, fewer diabetes complications, and longer life.
- Trial populations vs. real world. Clinical trial participants tend to be more adherent and more closely monitored than the average person. Real-world results will vary.
Are GLP-1s FDA-Approved for Prediabetes?
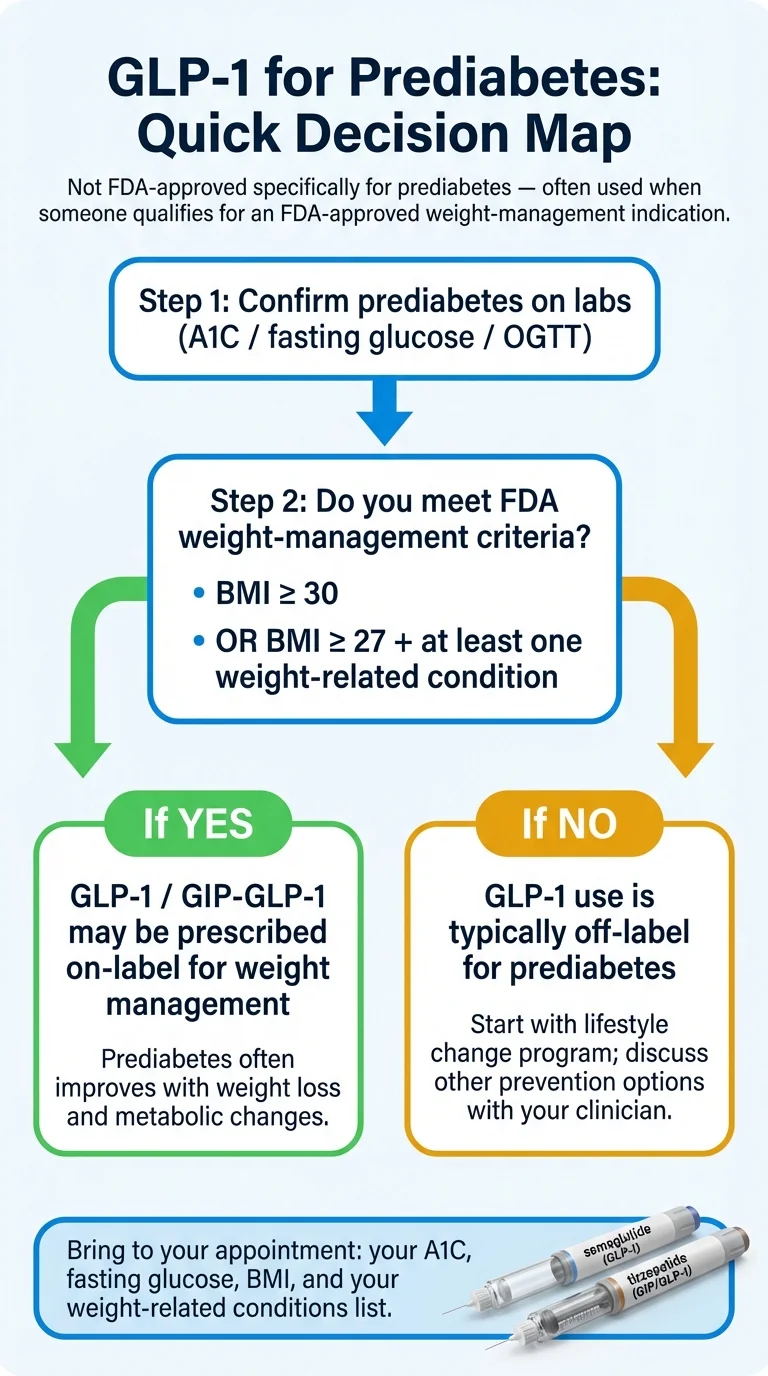
The short answer: No. No GLP-1 medication has been approved by the FDA specifically for the treatment or prevention of prediabetes.
But here’s the practical reality: many people with prediabetes also meet the criteria for an approved indication — particularly chronic weight management (if their BMI is 30 or higher, or 27+ with a weight-related condition) or cardiovascular risk reduction (for Wegovy specifically, in adults with obesity/overweight and established heart disease).
When your doctor prescribes a GLP-1 for prediabetes, they’re typically doing one of two things:
- Prescribing it on-label for obesity/overweight — and your prediabetes happens to benefit from the same treatment.
- Prescribing it off-label for prediabetes — which is legal and common in medicine, but may complicate insurance coverage.
Where Each Medication Stands
| Brand Name | Active Ingredient | Form | FDA-Approved For | Prediabetes Use |
|---|---|---|---|---|
| Wegovy (injection) | Semaglutide 2.4mg | Weekly injection | Obesity/overweight + comorbidity; CV risk reduction; MASH | Off-label; but prediabetes patients often qualify under obesity indication |
| Wegovy pill | Oral semaglutide 25mg | Daily pill | Obesity/overweight + comorbidity; CV risk reduction | Off-label; launched January 2026 |
| Ozempic | Semaglutide 1mg | Weekly injection | Type 2 diabetes; CKD in T2D | Off-label for prediabetes |
| Rybelsus | Oral semaglutide (lower dose) | Daily pill | Type 2 diabetes; CV risk reduction in T2D (added Oct 2025) | Off-label for prediabetes |
| Zepbound | Tirzepatide | Weekly injection | Obesity/overweight + comorbidity; obstructive sleep apnea | Off-label; strongest prediabetes evidence |
| Mounjaro | Tirzepatide | Weekly injection | Type 2 diabetes | Off-label for prediabetes |
| Saxenda | Liraglutide 3mg | Daily injection | Obesity/overweight + comorbidity | Off-label; generic available (Teva, Aug 2025) |
| Victoza | Liraglutide 1.8mg | Daily injection | Type 2 diabetes | Off-label for prediabetes |
| Trulicity | Dulaglutide | Weekly injection | Type 2 diabetes | Off-label; limited prediabetes-specific evidence |
Sources: FDA prescribing information for each medication. Table last verified February 2026.
What “Off-Label” Actually Means
Off-label prescribing is completely legal. It means the FDA hasn’t specifically reviewed and approved the drug for that particular use, but a doctor determines it’s medically appropriate based on available evidence. About 20% of all prescriptions in the U.S. are off-label.
The catch: insurance companies typically follow FDA-approved indications. If your prescription doesn’t match an approved use, coverage gets harder. Not impossible — but harder.
GLP-1 vs. Metformin for Prediabetes: How Do They Compare?
If you have prediabetes, there’s a good chance your doctor mentioned metformin. It’s cheap, well-studied, and has been the go-to pharmacotherapy for diabetes prevention for over two decades.
The Head-to-Head Data
A 2024 Danish nationwide cohort study directly compared GLP-1 receptor agonists versus metformin as first-line therapy in people who had never taken glucose-lowering medication before. The findings were nuanced:
- GLP-1s produced greater A1C reduction in both prediabetes and diabetes groups.
- GLP-1 users were less likely to need additional medications added to their regimen.
- But metformin had significantly better adherence in prediabetes patients — 55.7% of GLP-1 users were non-adherent at one year, compared to 34.8% of metformin users.
That last point matters more than most articles acknowledge. The best medication is the one you actually take consistently.
Source: Sørensen et al., Journal of Diabetes, 2024
The Practical Comparison
| Factor | Metformin | GLP-1 Medications |
|---|---|---|
| FDA-approved for prediabetes? | No (but ADA recommends it for prevention) | No |
| Diabetes risk reduction | 31% (DPP study, 3 years) | 72–93% (multiple trials, 1–3 years) |
| Weight loss | Modest (5–7 lbs typical) | Significant (15–22% of body weight in trials) |
| How you take it | Daily pill (1–2x/day) | Weekly injection or daily pill |
| Monthly cost | $4–$20 (generic) | $149–$1,400+ (depends on brand and access path) |
| Insurance coverage | Generally easy to get covered | Difficult for prediabetes alone; easier under obesity indication |
| Common side effects | GI symptoms (diarrhea, nausea), B12 deficiency long-term | GI symptoms (nausea, vomiting, diarrhea), potential muscle loss |
| 1-year adherence in prediabetes | ~65% | ~44% |
| Best suited for | First-line, budget-focused, mild-moderate risk, or as add-on therapy | Prediabetes + obesity, multiple risk factors, failed metformin, or significant weight loss needed |
Sources: DPP study (Knowler et al., NEJM 2002); Sørensen et al., Journal of Diabetes, 2024; SURMOUNT-1; STEP trials.
Our Take on When Each Makes Sense
Start with metformin if: You have prediabetes with modest weight to lose, no significant comorbidities, and you want an affordable, well-proven starting point. Metformin is not a consolation prize. It has over 20 years of real-world safety data, costs less than a cup of coffee per day, and genuinely reduces diabetes risk.
Consider a GLP-1 if: You have prediabetes and obesity (or overweight with related conditions), lifestyle changes haven’t been enough, you have additional risk factors (PCOS, fatty liver, high cholesterol, cardiovascular disease), or your doctor believes the benefit-risk profile supports it. GLP-1s offer significantly more weight loss and stronger glycemic improvement — but at substantially higher cost and with more side effects to manage.
They’re not mutually exclusive. Many people take both. They work through different mechanisms and can be safely combined.
How GLP-1 Medications Actually Work (in Plain English)
GLP-1 stands for glucagon-like peptide-1. It’s a hormone your gut naturally releases after you eat. GLP-1 medications mimic that hormone at higher, sustained levels.
Here’s what that does — and why it matters for prediabetes specifically:
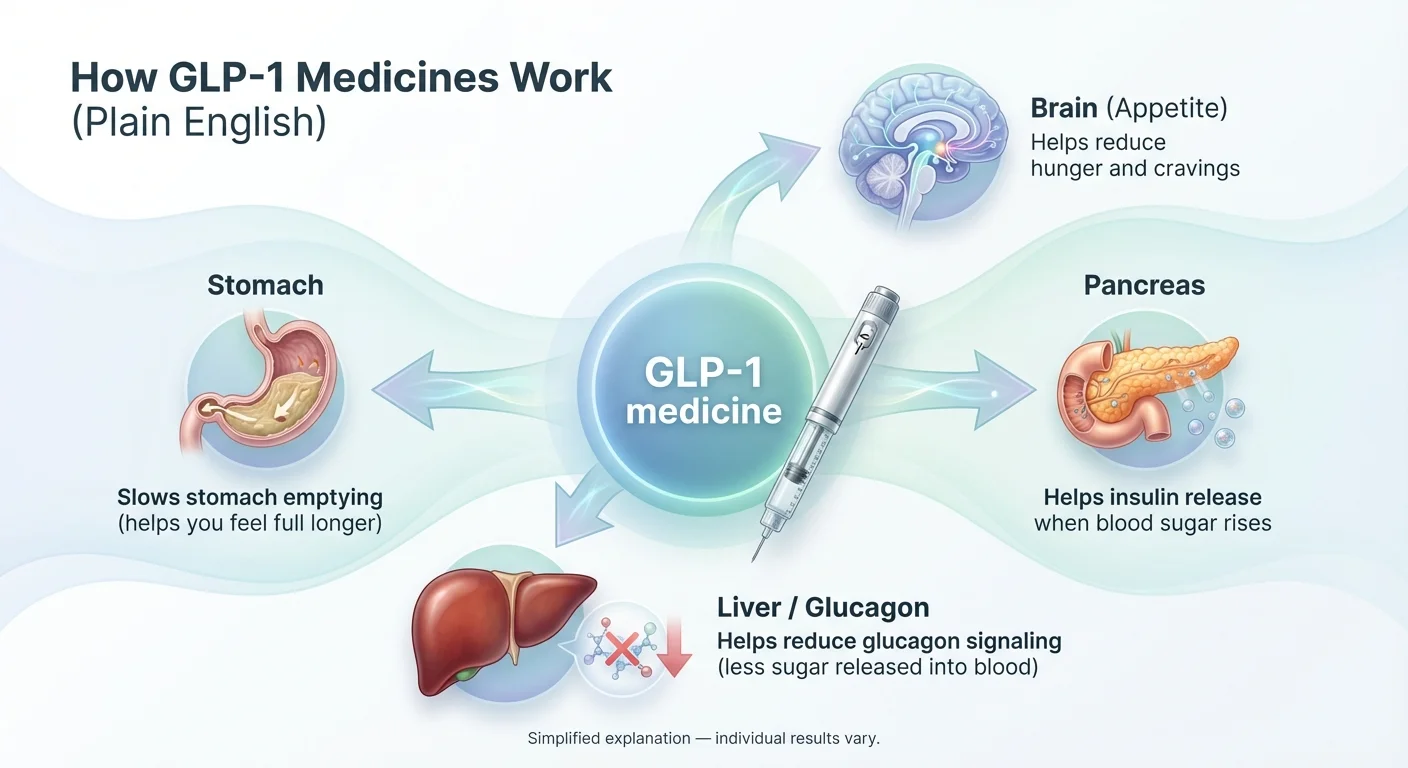
1. Improves your insulin response
GLP-1s signal your pancreas to release more insulin when blood sugar rises. This is “glucose-dependent,” meaning it only kicks in when your blood sugar is actually elevated — so the risk of dangerously low blood sugar is low when used alone.
2. Reduces glucagon
Glucagon is the hormone that tells your liver to dump stored sugar into your bloodstream. GLP-1s dial that down, which helps keep fasting blood sugar in check.
3. Slows stomach emptying
Food moves through your digestive system more slowly, so you don’t get the same blood sugar spikes after meals. This also contributes to feeling full longer.
4. Reduces appetite
GLP-1s act on areas of the brain involved in hunger, cravings, and fullness. This is the primary driver of the weight loss that’s central to both the diabetes prevention benefit and the media attention.
Why This Matters for Prediabetes Specifically
Prediabetes means your insulin system is under strain but still functional. GLP-1s support the system during this critical window — both directly (through improved insulin response and reduced glucagon) and indirectly (through weight loss, which independently improves insulin resistance).
It’s a dual benefit that’s hard to replicate with lifestyle changes alone for many people, especially those with significant weight to lose.
GLP-1 vs. GIP/GLP-1 (Tirzepatide)
Tirzepatide (Mounjaro, Zepbound) isn’t just a GLP-1. It’s a “dual agonist” — it activates both the GLP-1 receptor and the GIP (glucose-dependent insulinotropic polypeptide) receptor. This dual mechanism may explain why tirzepatide showed the strongest results in the prediabetes trials — ~93% risk reduction versus 72–79% for GLP-1-only drugs. Learn more in our semaglutide vs. tirzepatide comparison.
What’s Coming Next
The GLP-1 pipeline is moving fast. Two developments to watch:
- Foundayo (orforglipron) (Eli Lilly) — FDA-approved April 1, 2026. A daily oral pill that’s a non-peptide GLP-1, meaning it’s smaller and easier to manufacture. Available now through Ro, LillyDirect, and other providers starting at $149/month self-pay.
- CagriSema (Novo Nordisk) — combines a GLP-1 with an amylin analog for potentially stronger effects. Also in late-stage trials; approval timelines can change.
More options are coming, and costs should eventually come down as competition increases.
Who Should Consider a GLP-1 for Prediabetes?
Not everyone with prediabetes needs — or qualifies for — a GLP-1. Here’s how to think about whether it’s worth exploring for your situation.
You’re Most Likely to Qualify (and Benefit) If You Have:
- Prediabetes + BMI of 30 or higher (obesity) — this puts you in the FDA-approved weight management indication for several GLP-1s. Use our BMI eligibility calculator to check.
- Prediabetes + BMI of 27+ with at least one related condition — hypertension, high cholesterol, sleep apnea, PCOS, fatty liver disease, or cardiovascular disease
- A history of trying lifestyle changes without sustained weight loss — this strengthens both the medical case and the insurance argument
- Multiple metabolic risk factors — the ADA notes that people with higher baseline risk (higher A1C, higher BMI, history of gestational diabetes, younger age) may benefit most from pharmacotherapy (ADA Standards of Care, Section 3: Prevention, 2025)
It’s a Harder Case If You Have:
- Prediabetes at a normal weight with no comorbidities — most trial evidence is in people with obesity/overweight. Getting a prescription is possible (off-label) but insurance coverage will be very difficult. Metformin and lifestyle changes are the standard recommendation here.
- Mild prediabetes (A1C just above 5.7%) without other risk factors — the risk-benefit calculation may favor starting with lifestyle changes and monitoring.
Who Should NOT Take a GLP-1
Absolute Contraindications (Do Not Use):
- • Personal or family history of medullary thyroid cancer or Multiple Endocrine Neoplasia syndrome type 2 (MEN2)
- • Known serious hypersensitivity to the medication or its components
Use With Caution — Discuss Carefully With Your Doctor:
- • History of pancreatitis (GLP-1 labeling includes a warning; your doctor will weigh the risk)
- • Gallbladder disease or history of gallstones (risk may increase with rapid weight loss)
- • Severe gastrointestinal conditions like gastroparesis
- • Already taking another GLP-1 or tirzepatide product
Pregnancy: GLP-1s should be discontinued before planned pregnancy. For semaglutide, FDA labeling recommends stopping at least 2 months before a planned pregnancy due to its long half-life. Tell your doctor immediately if you become pregnant while on a GLP-1. Learn more about GLP-1 contraindications.
How Much Do GLP-1s Cost for Prediabetes — and Will Insurance Cover It?
This is the question that stops most people in their tracks. Let’s break it down honestly.
The Insurance Reality (No Sugarcoating)
Most insurance plans do not cover GLP-1 medications for prediabetes alone. Insurance companies follow FDA-approved indications. Since no GLP-1 is approved specifically for prediabetes, an insurer sees “prediabetes” as an insufficient justification.
The workaround that works for many people: If you have prediabetes and meet the obesity/overweight criteria, your doctor can prescribe the GLP-1 under the weight management indication — which IS FDA-approved and IS covered by many plans (though often with prior authorization hoops).
Prior Authorization: The Reality in 2026
Prior authorization requirements for GLP-1s have skyrocketed. According to Penn LDI research, prior authorization was required for fewer than 5% of Medicare beneficiaries for GLP-1s until 2024. By 2025, it was required for nearly 100%. For commercial insurance, over 88% of people with coverage for weight-loss GLP-1s still have to meet additional requirements like prior authorization, and the number of people with no commercial coverage at all for Wegovy increased by 42% compared to 2025.
Sources: Penn LDI, January 2026; GoodRx Insurance Tracking, 2026
What GLP-1s Actually Cost in 2026
| Access Path | Est. Monthly Cost | Notes |
|---|---|---|
| Brand-name injection at retail (no insurance) | $900 – $1,400 | Wegovy injection, Zepbound, Ozempic retail list pricing |
| Brand-name via TrumpRx | $199 (Wegovy/Ozempic pen); $299 (Zepbound) | Per TrumpRx.gov as of Feb 2026; higher doses may cost more |
| Wegovy pill at retail | ~$299–$349/month | Launched January 2026; pricing may vary by pharmacy |
| Wegovy pill via TrumpRx | $149 (starting dose) | Per TrumpRx.gov as of Feb 2026 |
| Medicare (when available via demonstration) | $50 copay/month | GLP-1 payment demonstration expected July 2026; Medicare price $245/month |
| Generic liraglutide (Saxenda generic) | Lower than brand, varies | Teva launched generic August 2025; first generic GLP-1 for weight management |
| Metformin (for comparison) | $4 – $20 | Generic, widely available at almost every pharmacy |
Prices are approximate and change frequently. Verify current pricing before purchasing. Last verified: February 2026.
Coverage by Insurance Type
| Insurance Type | Coverage Likelihood | Typical Barriers | What to Do |
|---|---|---|---|
| Employer commercial plan | Moderate — varies widely | Prior auth, step therapy, BMI documentation | Check your plan’s drug formulary; ask HR about weight management benefits |
| ACA Marketplace plan | Low to moderate | Many exclude weight-loss drugs entirely | Check formulary before selecting a plan during open enrollment |
| Medicare Part D | Currently limited — expanding | GLP-1s for weight loss not yet covered under standard Part D | Check if the Medicare GLP-1 demonstration has launched (expected July 2026). Eligible beneficiaries would pay $50/month copay. |
| Medicaid | Very limited | Only ~13 states cover GLP-1s for obesity under fee-for-service | Contact your state Medicaid office. Coverage varies dramatically by state. |
Sources: KFF Medicaid GLP-1 analysis, January 2026; CMS BALANCE model announcement, December 2025; CMS GENEROUS model announcement, November 2025; GoodRx, 2026.
What’s Changing: BALANCE Model, Medicare GLP-1 Demonstration, and TrumpRx
GENEROUS Model (November 2025): A Medicaid drug pricing initiative allowing CMS to negotiate lower drug prices for state Medicaid programs using most-favored-nation pricing. States can opt in to purchase GLP-1s (and other drugs) at internationally competitive prices.
BALANCE Model (December 2025): A voluntary CMS Innovation Center model designed to enable both state Medicaid agencies and Medicare Part D plans to cover GLP-1 medications for weight management and metabolic health, while controlling costs. Medicaid coverage launches as early as May 2026; Medicare Part D coverage launch has been delayed — check cms.gov for the current date.
Medicare GLP-1 Payment Demonstration (July 2026): A short-term bridge program so Medicare beneficiaries can access GLP-1s before BALANCE fully launches in Part D. Eligible Medicare beneficiaries will pay $50 per month. This operates outside the normal Part D benefit structure.
TrumpRx: A direct-to-consumer portal connecting eligible self-pay patients with discounted GLP-1 prices negotiated with Novo Nordisk and Eli Lilly. Launched early February 2026.
None of this is guaranteed long-term. Policy can change. Manufacturer participation is voluntary. We’ll update this section as developments become concrete.
Your Best Access Path Based on Your Situation
If you have commercial insurance + BMI ≥30 (or ≥27 with comorbidity): Your strongest path is through the weight management indication. Ask your doctor to submit prior authorization with full documentation — BMI, comorbidities, history of lifestyle change attempts, and lab results. Expect the first request to be denied and be prepared to appeal. Persistence pays.
If you have Medicare: Check whether the Medicare GLP-1 payment demonstration has launched (expected July 2026, with $50/month copay for eligible beneficiaries). If not yet available, TrumpRx may offer a lower self-pay path. Learn more about GLP-1 options for Medicare-age adults.
If you’re self-pay / no insurance coverage: The Wegovy pill at $149/month (starting dose via TrumpRx) or the Wegovy/Ozempic pen at $199/month via TrumpRx are the most accessible brand-name paths. Zepbound is available at $299/month. Telehealth weight management programs like MEDVi also offer access. Read our guide to getting GLP-1 without insurance.
If cost is the main barrier: Metformin at $4–20/month is a genuine, evidence-backed intervention for prediabetes prevention — not a consolation prize. Start there, combine it with a structured lifestyle program, and revisit GLP-1s when access or pricing improves.
How to Check Your Specific Coverage (Step by Step)
- Find your plan’s drug formulary — search “[your insurer name] drug formulary 2026” or call the number on your insurance card.
- Search for the specific medication — semaglutide, tirzepatide, or liraglutide.
- Check the tier and requirements — look for “prior authorization required,” “step therapy,” or “not covered.”
- Call your insurer directly and ask: “Is [specific GLP-1] covered for chronic weight management under my plan? What documentation do I need for prior authorization?”
- Ask your doctor’s office for help — most offices have staff experienced with prior authorization submissions.
Which GLP-1 Is Best If You Have Prediabetes?
There’s no single “best” GLP-1 for everyone with prediabetes. The right choice depends on your evidence priorities, budget, insurance situation, and personal preferences.
Best Overall Evidence for Prediabetes: Tirzepatide (Zepbound / Mounjaro)
The SURMOUNT-1 extension data is the strongest evidence we have — about 93% reduced diabetes progression (1.3% vs 13.3%), with the most weight loss (~12–20% of body weight).
Best for: Significant weight loss needed, prediabetes + obesity, can access/afford it. Limitation: Most expensive tier, requires weekly injection.
Best for Cardiovascular Risk: Semaglutide Injection (Wegovy)
Wegovy is the only GLP-1 FDA-approved to reduce the risk of heart attack, stroke, and cardiovascular death in adults with obesity/overweight and established heart disease (SELECT trial). If you have prediabetes plus cardiovascular risk factors, this indication may also help your insurance case.
Best for: Prediabetes + heart disease risk, want cardiovascular protection.
Best for People Who Won’t Do Injections: Wegovy Pill (Oral Semaglutide 25mg)
Launched January 2026, this is the first oral GLP-1 for weight management. The OASIS 4 data showed comparable weight loss to the injectable version, and 71% of prediabetes participants achieved normal blood sugar. Read more about the Wegovy pill cost and availability.
Best for: Needle-averse, want convenience of a daily pill, prediabetes + obesity. Limitation: Must be taken on an empty stomach with limited water; specific dosing instructions matter.
Best Budget Option: Generic Liraglutide (Saxenda Generic)
Teva launched the first generic version of Saxenda in August 2025. While liraglutide requires daily injection and produces less weight loss than semaglutide or tirzepatide, it has solid 3-year prediabetes data (79% reduced diabetes progression).
Best for: Budget-conscious, comfortable with daily injections, want proven prediabetes evidence at lower cost.
Best First Step for Most People: Metformin
We keep coming back to this because it deserves repeating. Metformin isn’t a GLP-1, but it’s cheap, proven, oral, and specifically recommended by the ADA for diabetes prevention. You can always add a GLP-1 later.
Side Effects and Risks: What You Need to Know
We’re not going to downplay this section. GLP-1s are effective medications with real side effects, and you deserve to know what to expect. For a deeper look, see our complete GLP-1 side effects guide.
Common Side Effects (Most People Experience at Least One)
The most frequent side effects are gastrointestinal — and they’re most intense during the first few weeks as your body adjusts, especially during dose escalation:
- • Nausea — the most commonly reported side effect across all GLP-1 trials
- • Vomiting — less common than nausea but can be significant
- • Diarrhea
- • Constipation
- • Abdominal pain
- • Decreased appetite (this is part of how the drug works, but it can be more intense than expected)
The good news: For most people, these symptoms improve substantially after the first 1–2 months. Proper dose titration (starting at a low dose and increasing slowly) is the single most effective way to manage GI side effects. Don’t let anyone rush your dose escalation.
Serious but Rare Risks
- Pancreatitis — rare but serious. If you develop severe, persistent abdominal pain (especially radiating to the back), seek immediate medical care.
- Gallbladder disease / gallstones — risk increases with rapid weight loss. Report any right upper abdominal pain.
- Thyroid concerns — animal studies showed thyroid C-cell tumors in rodents. This hasn’t been confirmed in humans, but all GLP-1s carry a boxed warning. GLP-1s are contraindicated if you have a personal or family history of medullary thyroid cancer or MEN2 syndrome.
- Diabetic retinopathy — some evidence of worsening in patients with pre-existing eye conditions, primarily in people with type 2 diabetes. Less relevant for prediabetes, but worth noting.
Sources: FDA prescribing information for semaglutide, tirzepatide, and liraglutide.
The Muscle Loss Concern (Important and Underreported)
Research suggests that roughly 25–39% of the weight lost on GLP-1 medications comes from lean body mass (muscle and other non-fat tissue), not just fat. Muscle loss can affect your metabolism, strength, mobility, and long-term metabolic health — which is particularly counterproductive if the whole point is improving your metabolic outlook.
How to mitigate this:
- Prioritize protein: Adequate protein intake is essential to preserve muscle during weight loss. Ask your doctor or a registered dietitian for a protein target that’s safe for your situation.
- Resistance training: Strength training 2–3 times per week is the single most effective intervention for preserving muscle mass during weight loss.
- Don’t under-eat dramatically. GLP-1s reduce appetite, but severely restricting calories on top of the drug’s appetite suppression can accelerate muscle loss.
When to Contact Your Doctor Immediately
- • Severe, persistent abdominal pain (especially with vomiting)
- • Signs of allergic reaction (swelling, difficulty breathing, severe rash)
- • Changes in vision
- • Symptoms of low blood sugar (shakiness, confusion, sweating — more likely if taking insulin or sulfonylureas simultaneously)
- • Signs of kidney problems (changes in urination, swelling)
- • A lump or swelling in your neck, hoarseness, or difficulty swallowing
Special Situations: PCOS, High Cholesterol, Fatty Liver, Sleep Apnea
Prediabetes + PCOS
Polycystic ovary syndrome (PCOS) is closely linked to insulin resistance — which is the same underlying issue in prediabetes. GLP-1s address both the insulin resistance and the weight component of PCOS. While no GLP-1 is FDA-approved specifically for PCOS, many endocrinologists prescribe them when a patient has PCOS with obesity and/or prediabetes. The combination of weight loss + improved insulin sensitivity can improve menstrual regularity, fertility markers, and metabolic parameters. Read our full guide on GLP-1 and PCOS.
Insurance angle: If you have PCOS + prediabetes + BMI qualifying you for the obesity indication, you have a reasonable case for coverage.
Prediabetes + High Cholesterol
GLP-1s generally improve lipid profiles as part of their metabolic benefits — the 2024 meta-analysis showed significant reductions in triglycerides and LDL cholesterol. If you have prediabetes and high cholesterol, a GLP-1 may address multiple risk factors simultaneously.
High cholesterol also counts as a weight-related comorbidity for GLP-1 eligibility under the obesity indication if your BMI is ≥27.
Prediabetes + Fatty Liver (NAFLD/MASH)
This is where the clinical guidelines are moving fastest. The 2025 ADA Standards of Care now specifically recommend considering GLP-1 receptor agonists or dual GIP/GLP-1 agonists for adults with type 2 diabetes or prediabetes and NAFLD.
Wegovy received FDA approval for MASH (metabolic dysfunction-associated steatohepatitis, the more advanced form of fatty liver) in 2025 — the first GLP-1 approved for liver disease. If you have prediabetes + diagnosed fatty liver, this may strengthen your case for both a prescription and insurance coverage.
Prediabetes + Sleep Apnea
Zepbound (tirzepatide) was approved by the FDA in December 2024 for moderate-to-severe obstructive sleep apnea in adults with obesity. If you have prediabetes + sleep apnea + obesity, tirzepatide could address all three — and the OSA indication may provide an additional coverage pathway.
Prediabetes + Cardiovascular Disease
Wegovy is approved to reduce the risk of major adverse cardiovascular events (death, heart attack, stroke) in adults with obesity/overweight and established cardiovascular disease. If you have prediabetes and heart disease, this is the strongest approved indication — and insurance coverage is most likely through this path.
What to Expect If You Start a GLP-1
Setting realistic expectations is one of the most important things we can do. Here’s what the timeline typically looks like. For full details, see our complete guide to starting GLP-1.
Weeks 1–4: Adjustment Period
- • Appetite changes begin (often noticeable within the first week)
- • Nausea is most common during this phase — eat smaller meals, stay hydrated, avoid greasy or heavy foods
- • You’re typically on the lowest dose
- • Weight loss may start, but don’t expect dramatic changes yet
Weeks 4–12: Dose Escalation
- • Your dose increases on a schedule (every 4 weeks for most GLP-1s)
- • Each increase can temporarily bring back some GI side effects
- • Weight loss typically accelerates
- • You may notice “food noise” quieting — the constant background thinking about food that many people with obesity experience
Months 3–6: Hitting Stride
- • Most people reach their target dose
- • Side effects have usually stabilized
- • Weight loss continues; A1C and fasting glucose typically improving
- • Your doctor should be checking labs periodically
Months 6–12+: Ongoing Management
- • Weight loss trajectory varies — some plateau, some continue losing
- • Metabolic improvements tend to be well-established
- • The conversation shifts to: maintenance dose? Long-term plan? Muscle preservation?
Why Some People Don’t See Expected Results
- • Dose titration too fast or too slow — work with your prescriber to find the right pace
- • Not addressing lifestyle factors — GLP-1s work best alongside dietary changes and physical activity, not as a replacement. See our GLP-1 plateau guide for a complete troubleshooting framework.
- • Sleep and stress — both significantly impact insulin resistance and weight loss
- • Medication interactions — some medications can blunt the effects
- • Individual biology — not everyone responds the same way. If one GLP-1 isn’t working, switching to a different one sometimes helps
Lifestyle Changes That Make GLP-1s Work Better
GLP-1s aren’t magic pills (or injections). They’re most effective when combined with lifestyle changes — and the good news is that GLP-1s actually make those changes easier to sustain because they reduce the constant hunger and cravings that derail so many attempts.
Nutrition
Focus on protein at every meal (aim for 25–30g per meal minimum), fiber-rich vegetables, and whole foods. Use the reduced appetite as a window to rebuild better eating habits.
Movement
Resistance training 2–3 times per week is non-negotiable for preserving muscle mass. Add 150 minutes of moderate activity per week for insulin sensitivity.
Sleep
Poor sleep independently worsens insulin resistance. If you’re not consistently getting 7+ hours, addressing that may improve your prediabetes as much as any medication.
Stress Management
Chronic stress elevates cortisol, which directly raises blood sugar and promotes abdominal fat storage. This isn’t fluffy self-care advice — it’s metabolic reality.
The people who get the best long-term results from GLP-1s aren’t the ones who rely solely on the medication. They’re the ones who use the appetite-reduction window to rebuild habits that sustain them whether or not they stay on the drug long-term.
What Happens When You Stop a GLP-1?
We’re not going to sugarcoat this. The honest answer is that many people regain a significant portion of the weight they lost after stopping GLP-1 therapy — and blood sugar improvements can fade with it.
The STEP 1 extension study showed that one year after stopping semaglutide, participants regained about two-thirds of their lost weight (Wilding et al., Diabetes Obes Metab, 2022). The liraglutide SCALE trial showed similar patterns. For a deeper look, see our guide on what happens when you stop taking GLP-1.
This isn’t a failure of willpower. It’s biology. Obesity and the metabolic dysfunction behind prediabetes involve changes in appetite hormones, brain signaling, and metabolic set points that don’t simply reset after a period of treatment.
What This Means Practically
- For many people, GLP-1 therapy may need to be long-term — similar to how blood pressure medication is ongoing, not a “cure and stop” treatment.
- If you’re considering stopping, work with your doctor on a gradual plan. Abrupt discontinuation tends to produce faster rebound.
- Lifestyle habits built during treatment matter enormously. The people who maintain the most benefit after stopping are those who used the treatment window to establish sustainable eating patterns, regular exercise, and better sleep.
- Maintenance doses (lower than the maximum treatment dose) are an area of active research and clinical discussion.
- Switching to metformin as a maintenance strategy may help — it’s affordable for long-term use and provides modest ongoing metabolic support.
The key insight most people miss: the goal isn’t necessarily to be on a GLP-1 forever. For some people with prediabetes, the goal is to use GLP-1 therapy as a metabolic reset — lose the weight, restore insulin sensitivity, build sustainable habits — and then transition to a lower-cost maintenance strategy. Whether that’s a lower GLP-1 dose, metformin, lifestyle changes alone, or some combination depends on your individual response and your doctor’s assessment.
This is a conversation to have with your doctor early in treatment — not after you’ve already decided to stop.
How to Get a GLP-1 Safely (and Avoid Scams)
The demand for GLP-1s has created an ecosystem that includes excellent providers — and dangerous ones. Here’s how to protect yourself. For a more thorough guide, see our GLP-1 safety guide.
The FDA’s Warning (Take This Seriously)
The FDA has issued specific warnings about unapproved GLP-1 drugs being sold for weight loss, including products illegally marketed “for research purposes” and direct-to-consumer supplies with unknown quality. These products may contain incorrect doses, contaminants, or entirely different substances than what’s on the label (FDA.gov).

The Safest Path Hierarchy
- Your primary care doctor, endocrinologist, or obesity medicine specialist — this is the gold standard. They know your full medical history, can order appropriate labs, and manage your care comprehensively.
- Reputable telehealth platforms with real medical oversight — legitimate telehealth providers connect you with licensed physicians who review your medical history, order labs when appropriate, and provide ongoing follow-up. See our comparison of top GLP-1 telehealth providers.
- Avoid at all costs: Products labeled “for research purposes only,” medications from unregulated websites, supplies without a valid prescription, and anything that doesn’t come from a licensed pharmacy.
Telehealth Vetting Checklist
- Licensed prescribers (MD, DO, NP, PA) in your state
- Medical screening includes health history review and labs when appropriate
- Regular follow-up scheduled (not just a one-time prescription)
- Transparent pricing — no hidden fees, clear cancellation terms
- Medications sourced from licensed, regulated pharmacies
- Clear disclosure of whether medications are brand-name or compounded
- Real customer support you can actually reach
Looking for a vetted GLP-1 provider?
Pricing, medical oversight & medication sourcing verified
A Note on Compounded GLP-1s
During the drug shortage, the FDA allowed compounding pharmacies to produce semaglutide and tirzepatide. In 2025, the FDA declared the shortages resolved and moved to end this compounding. Some compounding continues under legal challenges, but the regulatory status is unstable.
Compounded medications are NOT FDA-approved. They are not tested for safety, efficacy, or quality the way brand-name drugs are. If you choose a compounded product, understand the risks and verify the pharmacy’s credentials (look for PCAB accreditation or 503A/503B designation). Read our compounded semaglutide safety guide.
Your Next Step: A 10-Minute Action Plan
You’ve read the evidence. Now here’s exactly what to do with it.
If You Were Recently Diagnosed With Prediabetes
- Confirm your numbers. Make sure you have recent lab results: A1C, fasting glucose, lipid panel, and (ideally) liver function tests for NAFLD screening.
- Know your BMI and waist circumference. This determines your eligibility pathway for GLP-1s. Check with our BMI eligibility calculator.
- List your comorbidities. PCOS, high cholesterol, hypertension, sleep apnea, fatty liver, cardiovascular disease — each one strengthens your case for treatment and coverage.
- Start a structured lifestyle program. The CDC’s National Diabetes Prevention Program (DPP) is free or low-cost and proven to reduce diabetes risk. Find one at cdc.gov/diabetes-prevention. This is valuable on its own AND demonstrates “prior lifestyle attempt” for insurance purposes.
If You Think You Qualify for a GLP-1
Bring this to your next doctor’s appointment:
Questions to Ask Your Doctor:
- • “My A1C is [X] and my BMI is [Y]. Based on the SURMOUNT-1 and STEP trial data, am I a candidate for GLP-1 therapy?”
- • “Can we prescribe this under the weight management indication so it’s more likely to be covered?”
- • “Would you be willing to help with prior authorization documentation?”
- • “What labs and monitoring do you recommend if I start?”
- • “Should I start with metformin first, or go directly to a GLP-1?”
If You Don’t Qualify — or Can’t Afford It Right Now
This isn’t the end of your options:
- Metformin ($4–20/month) is proven to reduce diabetes risk by 31% — your doctor can prescribe it today.
- The CDC’s Diabetes Prevention Program reduces risk by 58% through structured lifestyle changes.
- GLP-1 access is improving. Generic options are expanding, oral formulations are launching, and government programs are lowering prices. What’s unaffordable today may become accessible within a year.
Ready to explore GLP-1 options?
Compare pricing, medical oversight & medication sourcing
Frequently Asked Questions
Is Ozempic approved for prediabetes?
No. Ozempic (semaglutide) is FDA-approved for type 2 diabetes and chronic kidney disease in T2D patients. It is not approved for prediabetes. However, if you have prediabetes and also qualify for a GLP-1 under a different indication (like obesity), your doctor may prescribe one that way.
Is Wegovy approved for prediabetes?
No. Wegovy is approved for chronic weight management in adults with obesity or overweight plus a comorbidity, and for cardiovascular risk reduction. It is not specifically approved for prediabetes — but many people with prediabetes meet the weight management criteria.
Can GLP-1s actually reverse prediabetes?
Clinical trials show they can return blood sugar levels to normal in a significant number of people. In STEP 10, 81% of participants with prediabetes achieved normal blood sugar on semaglutide versus 14% on placebo. However, these improvements were measured while on medication, and some benefit may be lost after stopping.
Will insurance cover a GLP-1 for prediabetes?
Typically not for prediabetes alone. Coverage is more likely if you qualify under the obesity/overweight indication (BMI ≥30, or ≥27 with a comorbidity). Medicare coverage is expanding through pilot programs. Check your specific plan's formulary.
Will Medicare cover GLP-1s for prediabetes?
Not yet under standard Part D — Medicare is currently prohibited by law from covering weight-loss drugs. However, CMS plans a GLP-1 payment demonstration starting July 2026 (eligible beneficiaries would pay $50/month), and the BALANCE Model will bring Part D coverage and has been delayed — check cms.gov for the current launch date. Details are still being finalized.
What does "off-label" mean?
Off-label means a doctor prescribes a medication for a use not specifically approved by the FDA. It's legal, common (about 20% of all U.S. prescriptions), and based on the doctor's clinical judgment and available evidence.
Which is better for prediabetes: semaglutide or tirzepatide?
Tirzepatide has the strongest single-trial evidence (~93% reduced diabetes progression in SURMOUNT-1). Semaglutide has broader evidence across multiple trials and now offers an oral option (Wegovy pill). Your doctor can help determine which is best for your specific situation.
Can I get a GLP-1 if I'm not obese?
It's harder. Most approved indications require BMI ≥30 or BMI ≥27 with a comorbidity. If you have prediabetes at a normal weight, a GLP-1 would be off-label, and insurance coverage is unlikely. Metformin and lifestyle changes are the standard recommendation in this scenario.
What are the most common side effects of GLP-1 for prediabetes?
Nausea, vomiting, diarrhea, constipation, and abdominal pain — primarily during the first 1–2 months and during dose increases. These typically improve with time and proper dose titration.
Is compounded semaglutide safe?
Compounded medications are not FDA-approved and are not tested for safety, efficacy, or quality the same way brand-name drugs are. The FDA has warned about unapproved GLP-1 products and urges consumers to get medications only through legitimate pharmacies with valid prescriptions.
How fast will I see results with GLP-1 for prediabetes?
Appetite changes often begin within the first week. Noticeable weight loss typically starts within 4–8 weeks. Lab improvements (A1C, fasting glucose) are usually measurable by 3 months. Maximum effects develop over 6–12 months at target dosing.
What happens if I stop taking a GLP-1?
Many people regain a significant portion of lost weight after stopping, and blood sugar improvements can fade. This isn't a willpower issue — it's biology. Discuss a long-term plan with your doctor before starting, not after.
Can I take metformin and a GLP-1 together?
Yes. They work through different mechanisms and are commonly used together. The combination may provide additive benefits for blood sugar control and weight management.
Does prediabetes count as a "comorbidity" for GLP-1 eligibility?
It depends on the plan. Some insurers list prediabetes as a qualifying comorbidity for weight management drugs; others do not. Check with your specific insurer. Other qualifying conditions include hypertension, dyslipidemia, cardiovascular disease, sleep apnea, and PCOS.
How We Researched This Guide
We built this guide by reviewing published clinical trial data, systematic reviews, and current treatment guidelines — not industry press releases or social media claims.
Primary Sources Used
- • Clinical trials: SURMOUNT-1 extension (Jastreboff et al., NEJM 2025), STEP 10 (McGowan et al., Lancet Diabetes Endocrinol 2024), STEP pooled analysis (Perreault et al., Lancet Diabetes Endocrinol 2023), SCALE (le Roux et al., The Lancet 2017), OASIS 4 (Novo Nordisk 2025)
- • Meta-analyses: Salamah et al., Diabetol Metab Syndr, 2024 (12 trials, 4,316 patients)
- • Guidelines: ADA Standards of Care 2025 (Section 3: Prevention), USPSTF Prediabetes Screening Recommendation
- • Regulatory sources: FDA prescribing information for Wegovy, Ozempic, Rybelsus, Zepbound, Mounjaro, Saxenda; FDA safety warning on unapproved GLP-1 products
- • Insurance/coverage data: GoodRx Insurance Tracking 2026, KFF Medicaid GLP-1 Analysis (January 2026), Penn LDI Prior Authorization Research (January 2026), CMS BALANCE model announcement (December 2025), CMS GENEROUS model announcement (November 2025), CMS Medicare GLP-1 payment demonstration
- • Head-to-head comparison: Sørensen et al., Journal of Diabetes, 2024 (GLP-1 vs. metformin nationwide cohort study)
- • Diabetes Prevention Program: Knowler et al., NEJM 2002
What We Verify and When
- • Pricing data: Verified quarterly against manufacturer websites, TrumpRx.gov, and major pharmacy platforms
- • Insurance coverage: Reviewed quarterly; updated when major policy changes are announced
- • Clinical evidence: Reviewed when new trials are published or guidelines are updated
- • FDA approval status: Checked monthly for new approvals or label changes
- • “Last Verified” dates throughout this page are updated only when we actually re-verify the information, not automatically
What This Page Is NOT
This page is not medical advice. It’s not a substitute for a conversation with a healthcare provider who knows your full medical history. We don’t prescribe. We don’t diagnose. We synthesize the best available evidence into plain language so you can have a more informed conversation with the person who does.
Have questions we didn’t cover? Contact us — we update this guide regularly based on reader questions and new evidence.
Looking for a GLP-1 provider? → Compare the top online GLP-1 providers — pricing, medical oversight, and medication sourcing verified.
Related Articles
Oral Semaglutide vs Injectable
Comparing oral and injectable semaglutide forms by effectiveness, convenience, and price.
What Happens When You Stop Taking GLP-1
What to expect when discontinuing GLP-1 medications including weight regain and withdrawal effects.
What Is GLP-1?
A complete beginner's guide to GLP-1 medications, how they work, and what to expect.
GLP-1s for Weight Loss
How GLP-1 receptor agonists promote weight loss through appetite reduction and metabolic changes.
Learn About GLP-1
Educational hub covering GLP-1 science, medications, eligibility, and treatment options.
History of GLP-1 Drugs
The complete timeline of GLP-1 drug development from discovery to modern weight loss treatments.