History of GLP-1 Drugs: The Complete Timeline From Gut Hormones to a Global Revolution
Disclosure: Some links on this site are affiliate links. If you purchase through these links, we may earn a commission at no extra cost to you. Thank you for supporting our site.·For informational purposes only—not medical advice.
GLP-1 drugs are medicines that mimic or amplify the gut hormone GLP-1 to improve blood sugar control and reduce appetite. The first GLP-1 receptor agonist was FDA-approved in 2005; weight-loss approvals began in 2014 and accelerated after Wegovy's 2021 approval.
Quick answer: GLP-1 drugs evolved from gut-hormone discoveries (1902) to injectable GLP-1 receptor agonists (2005) and modern multi-incretin therapies. The first GLP-1 drug for weight loss was approved in 2014. The timeline below covers every major milestone and FDA approval through 2026.
The history of GLP-1 drugs doesn't start with Ozempic. It starts in 1902, in a London laboratory, with a dog and a piece of intestine.
What followed is one of the most remarkable stories in modern medicine: a 120-year chain of discoveries connecting gut hormones, lizard venom, a peptide chemist fighting for credit, and one of the fastest-growing drug classes in pharmaceutical history. GLP-1–based medicines — including GLP-1 receptor agonists (Ozempic, Wegovy) and dual incretin agonists like tirzepatide (Mounjaro, Zepbound) — were built on decades of science that most people have never heard of.
This page covers every major milestone in that story. Every discovery. Every FDA approval. Every scientist who made it happen. The major drugs in development right now. Whether you're a patient trying to understand what you're putting in your body, a journalist who needs facts with primary sources listed, or a researcher who wants the full picture in one place — we built this to be that resource.
And the punchline up front: these drugs are not a fad. They are backed by more than a century of incretin biology research, over 20 years of clinical use, and safety data from some of the largest cardiovascular outcome trials ever conducted.
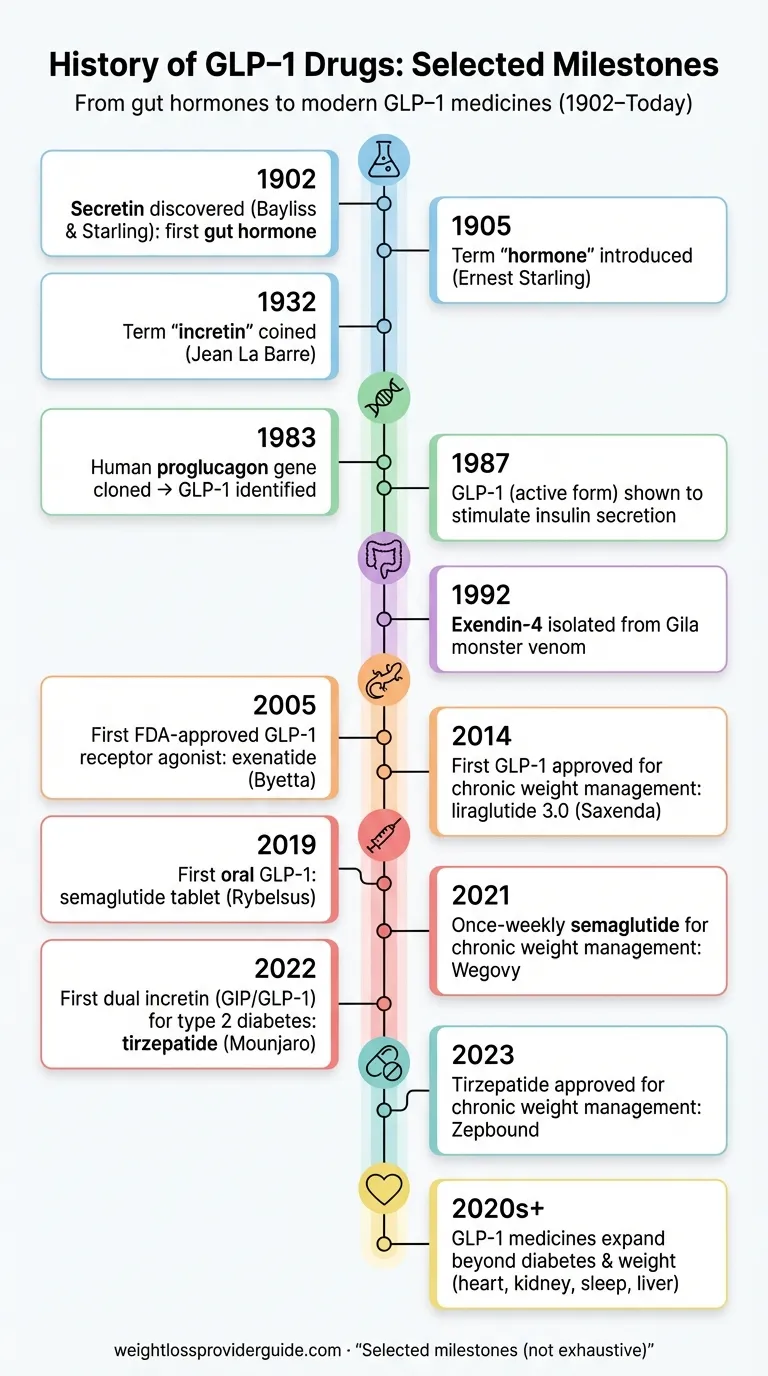
Here's the entire timeline at a glance — then we'll break every era apart.
Illustration for educational purposes only. Actual product appearance may vary.
GLP-1 Drug Timeline at a Glance: Key Milestones From 1902 to 2026
| Year | Milestone |
|---|---|
| 1902 | Bayliss and Starling discover secretin — the first gut hormone — proving the intestine sends chemical signals to other organs |
| 1906 | Liverpool researchers show intestinal extract lowers blood glucose; the “incretine” concept is born |
| 1932 | La Barre coins the term “incretine” for a gut factor that stimulates insulin independently |
| 1960s | Radioimmunoassay technology enables precise measurement of gut hormones for the first time |
| 1970s | GIP (glucose-dependent insulinotropic polypeptide) identified as the first incretin hormone |
| 1983 | Bell et al. clone the human proglucagon gene, revealing the sequences of GLP-1 and GLP-2 |
| 1985–87 | Mojsov identifies the biologically active form of GLP-1; Mojsov, Habener, Drucker, and Holst prove it stimulates insulin secretion |
| 1992 | John Eng discovers exendin-4 in Gila monster venom — a peptide that mimics GLP-1 but lasts hours instead of minutes |
| 1995 | Lotte Knudsen begins engineering a long-acting human GLP-1 analog at Novo Nordisk |
| 2005 | FDA approves exenatide (Byetta) — the first GLP-1 receptor agonist, derived from Gila monster venom |
| 2010 | FDA approves liraglutide (Victoza) — the first once-daily GLP-1 drug |
| 2014 | FDA approves liraglutide for obesity (Saxenda) — the first GLP-1 drug for weight loss |
| 2017 | FDA approves semaglutide (Ozempic) for type 2 diabetes — the molecule that changes everything |
| 2019 | FDA approves oral semaglutide (Rybelsus) — the first GLP-1 you can swallow |
| 2021 | FDA approves semaglutide for weight loss (Wegovy) — GLP-1 drugs go mainstream |
| 2022 | FDA approves tirzepatide (Mounjaro) — first dual GLP-1/GIP agonist for diabetes |
| 2023 | FDA approves tirzepatide for weight loss (Zepbound); GLP-1 prescriptions among commercially insured adults surge over 360% (FAIR Health data, 2019–2024) |
| 2024 | Wegovy approved for cardiovascular risk reduction (SELECT trial); Zepbound approved for sleep apnea; Lasker Award honors GLP-1 pioneers |
| 2025 | Ozempic approved for kidney disease (FLOW trial); Wegovy approved for fatty liver disease (MASH); generic liraglutide arrives; semaglutide shortage resolved |
| 2026 | Oral Wegovy tablets launch (Jan 2026); Ozempic tablets approved (Jan 2026); Foundayo (orforglipron) FDA-approved April 1, 2026 — first non-peptide oral GLP-1 for obesity; Medicare GLP-1 Bridge launches July 1, 2026, covering Wegovy and Zepbound for Part D beneficiaries at $50/month |
Each of these milestones is expanded with full context, citations, and sourcing in the sections that follow.
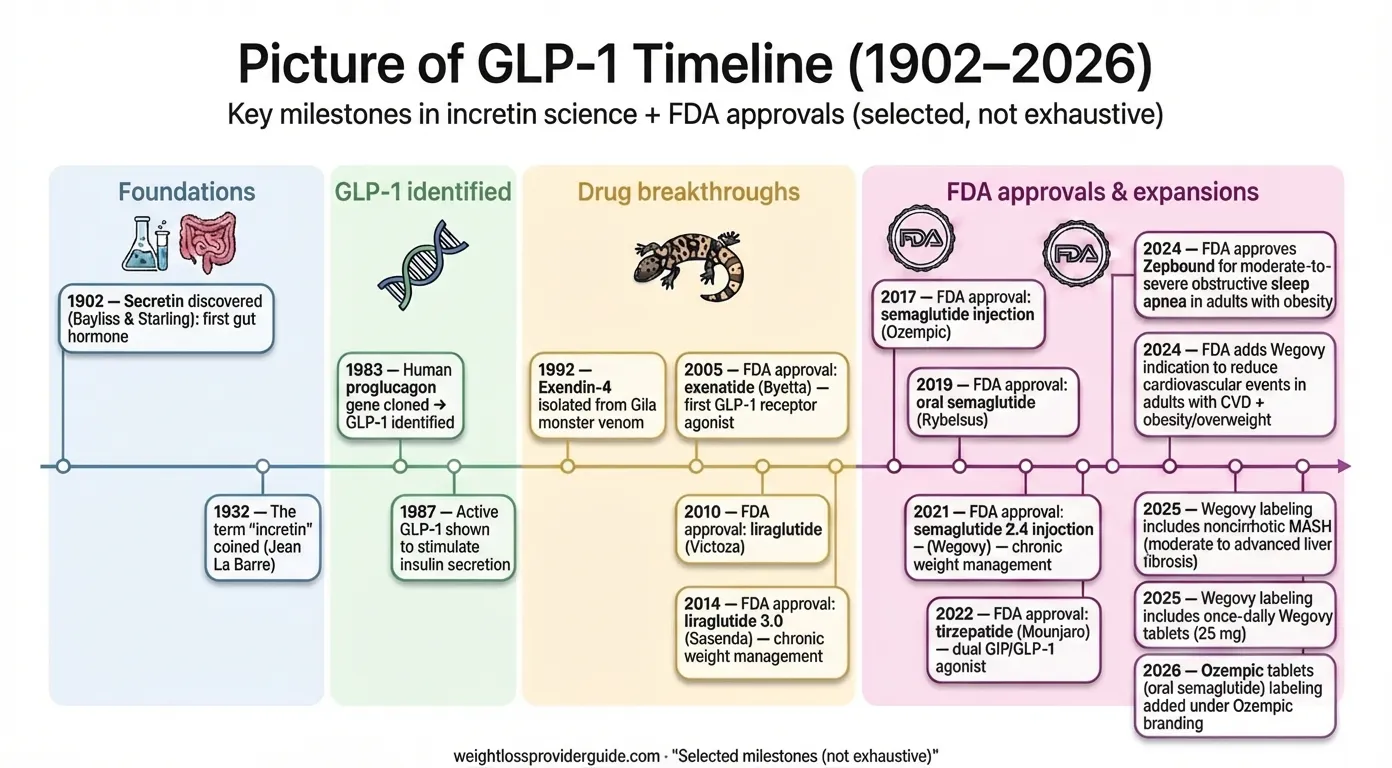
Picture of GLP-1 timeline (1902–2026). Selected milestones; not exhaustive.
Infographic for educational purposes. Data sourced from FDA records and published literature.
Why the History of GLP-1 Drugs Matters Right Now
You might be wondering why a history lesson matters when you're really here because you (or someone you know) just heard about these medications. Here's why the backstory changes everything about how you evaluate them:
These drugs are not new. The underlying science spans over 120 years. The first GLP-1 drug was approved in 2005 — that's two decades of real-world clinical use. The Ozempic molecule (semaglutide) was approved in 2017. The weight-loss formulation (Wegovy) followed in 2021. What's new is the public awareness, not the pharmacology.
The numbers are staggering. Among adults with an overweight or obesity diagnosis, FAIR Health data shows GLP-1 prescribing increased 586.7% between 2019 and 2024. Across all commercially insured adults, GLP-1 prescriptions rose 363.7% over the same period. The global market for these medications is projected to exceed $100 billion by 2030. In a November 2025 KFF survey, approximately 12% of U.S. adults reported currently taking a GLP-1 medication — double the 6% reported in May 2024.
The indications keep expanding. As of early 2026, GLP-1-based drugs carry FDA approvals for type 2 diabetes, chronic weight management, cardiovascular risk reduction, obstructive sleep apnea, diabetic kidney disease, and metabolic dysfunction-associated steatohepatitis (MASH, commonly called fatty liver disease). Clinical trials are underway for Alzheimer's disease, addiction, PCOS, heart failure, and osteoarthritis.
Understanding where these drugs came from — the century of science, the failed attempts, the lizard venom breakthrough, the political battles over credit — gives you something no marketing campaign can: perspective. And perspective is what you need to make an informed decision about whether they're right for you.
Where It All Began: The Incretin Concept (1902–1979)
The First Clue: A Dog, an Intestine, and a New Kind of Hormone (1902)
In January 1902, at University College London, physiologists William Bayliss and Ernest Starling removed a section of a dog's small intestine, separated it from all nerve connections, and introduced acid into it. The blood vessels were still intact. To their surprise, the distant pancreas responded by secreting digestive juices.
This was radical. At the time, scientists believed the nervous system controlled everything. Bayliss and Starling had just proved that the gut could send chemical messages through the blood. They called the messenger “secretin” — and in 1905, Starling introduced the word “hormone” (from the Greek hormōn, meaning “to set in motion”) to describe this new class of chemical signals.
It was the birth of endocrinology. And it planted the first seed of what would become GLP-1 science.
The “Incretine” Idea: Something in the Gut Controls Blood Sugar (1906–1932)
In 1906, a team at the University of Liverpool — Moore, Edie, and Abram — showed that extracts from the gut could lower blood glucose when injected into animals. They hypothesized a gut-derived factor that stimulated the pancreas to manage sugar.
The discovery of insulin in 1921 overshadowed this line of research. Why bother with a mysterious gut factor when you've found the hormone that directly controls blood sugar?
But the gut hormone idea didn't die completely. In 1932, Belgian physiologist Jean La Barre revived it, coining the term “incrétine” (a blend of intestin sécrétion insuline) to describe a substance from the intestine that could stimulate insulin release.
The concept then sat largely dormant for three decades.
The Incretin Effect Gets Proven (1960s–1970s)
The breakthrough came with new technology. In the 1960s, Rosalyn Yalow and Solomon Berson developed the radioimmunoassay — a technique that could measure vanishingly small amounts of hormones in blood. This earned Yalow the Nobel Prize in 1977 and gave researchers the tools they needed to study gut hormones properly.
The key observation came in 1964, when Michael McIntyre and colleagues published a landmark finding in The Lancet: when you give someone glucose by mouth, they produce significantly more insulin than when you inject the same amount of glucose directly into their vein — even though blood sugar levels are identical.
Something in the gut was amplifying the insulin response. This “bonus” insulin secretion was named the incretin effect, and it suggested that 50–70% of the insulin response to a meal is driven not by blood sugar alone, but by hormones released from the gut when food arrives.
In the 1970s, researchers identified the first incretin hormone: GIP (glucose-dependent insulinotropic polypeptide), isolated from porcine intestinal extracts. But GIP only explained part of the incretin effect. And there was a bigger problem: GIP didn't work well in people with type 2 diabetes. Their pancreas seemed to ignore it.
Something else was out there. Another incretin. It would take the molecular biology revolution of the 1980s to find it.
The Discovery of GLP-1: Finding the Missing Incretin (1979–1987)
Cracking the Proglucagon Code
The path to GLP-1 ran through glucagon — the hormone that raises blood sugar, essentially the opposite of insulin. In 1979, researchers sequencing hamster proglucagon (the precursor protein that gets chopped up to make glucagon) noticed something curious: the gene contained extra sequences that looked glucagon-like but weren't glucagon itself.
In 1982, Joel Habener's laboratory at Massachusetts General Hospital found similar glucagon-like sequences in anglerfish. The following year, Graeme Bell and colleagues cloned the full human proglucagon gene and revealed the complete picture: the gene encoded glucagon and two additional peptides — GLP-1 (glucagon-like peptide-1) and GLP-2 (glucagon-like peptide-2).
It was like finding hidden messages inside a known gene. But nobody yet knew what GLP-1 actually did.
Svetlana Mojsov: The Scientist Who Found the Active Fragment
This is where the story gets both remarkable and uncomfortable.
Svetlana Mojsov, a peptide chemist heading a synthesis facility at Massachusetts General Hospital, took on the painstaking work of figuring out which piece of the GLP-1 sequence was biologically active. The gene encoded a 37-amino-acid peptide, but was all of it necessary? Which fragment mattered?
Mojsov synthesized different truncated versions and developed antibodies to track them. Her critical discovery: the active form was a specific fragment — GLP-1(7-36) amide and GLP-1(7-37) — not the full-length peptide. Only this truncated version could stimulate insulin secretion.
In 1986–87, the pieces came together rapidly. Mojsov, working with Habener and endocrinologist Gordon Weir, demonstrated that GLP-1 stimulated insulin release from a perfused whole rat pancreas. Independently and nearly simultaneously, Jens Juul Holst at the University of Copenhagen published similar findings using pig pancreas tissue.
Meanwhile, Daniel Drucker, a postdoctoral fellow in Habener's lab, demonstrated that GLP-1 could directly stimulate insulin gene transcription in pancreatic cell lines — proof that GLP-1 wasn't just triggering insulin release but actively promoting insulin production at the genetic level.
The missing incretin had been found. GLP-1 was real, it was powerful, and it looked like a legitimate drug target.
But Mojsov's role in the story nearly vanished. Her name was initially left off key patents filed by Massachusetts General Hospital. She fought to be included, and MGH eventually amended four patents to add her as a co-inventor. She received her share of drug royalties for one year.
When major scientific prizes were awarded for GLP-1 research — the 2017 Harrington Award, the 2021 Canada Gairdner International Award — Mojsov was not among the honorees. It wasn't until the 2024 Lasker-DeBakey Clinical Medical Research Award (often called “America's Nobel”) that she finally received the recognition many believed she deserved, alongside Habener and Lotte Bjerre Knudsen. As peptide chemist Richard DiMarchi told Science Magazine, “There's a hard line being drawn between these three gentlemen and Svetlana when it sure seems that there is a hell of a lot of overlap.”
The Half-Life Problem: Why GLP-1 Couldn't Become a Drug (Yet)
Discovering GLP-1 was one thing. Turning it into a medicine was another.
Natural GLP-1 has a half-life of approximately two minutes in the human body. The enzyme DPP-4 (dipeptidyl peptidase-4) chews it apart almost instantly. Only 10–15% of secreted GLP-1 reaches the bloodstream intact, and what does arrive is gone in moments.
You can't build a practical drug around a molecule that disappears in 120 seconds.
This “fatal flaw” sent researchers down two parallel paths that would converge decades later:
- Find a natural GLP-1 mimic that resists DPP-4 (the Gila monster path)
- Engineer a modified human GLP-1 that lasts longer (the Novo Nordisk path)
Both worked. Both led to billion-dollar drugs. And both started with a simple question: How do we make this molecule survive long enough to help people?
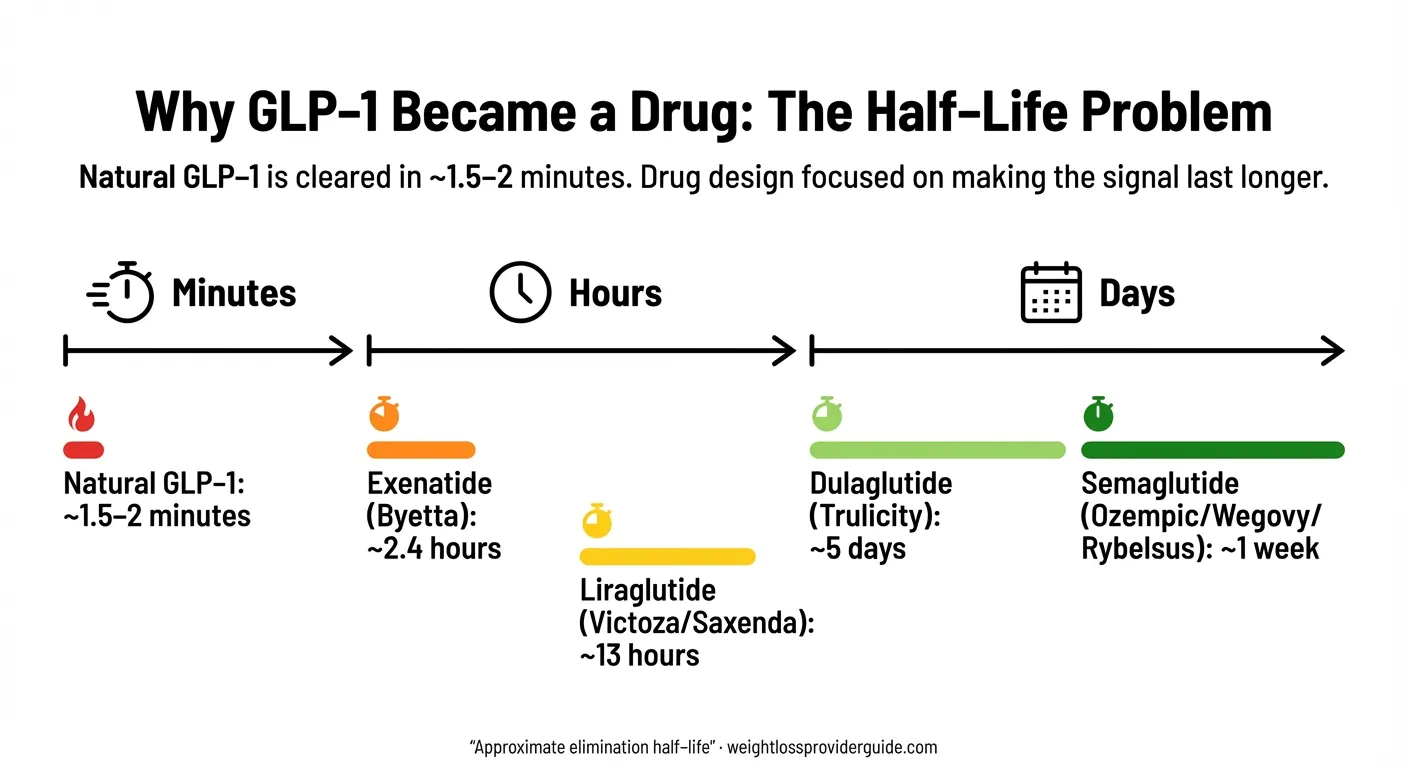
Illustration shows the half-life progression from natural GLP-1 to engineered drug versions.
The Gila Monster Connection: How Lizard Venom Led to the First GLP-1 Drug
This is the part of the story that sounds made up. It isn't.
John Eng and the Venom From the Bronx
In the early 1990s, Dr. John Eng, an endocrinologist at the Veterans Affairs Medical Center in the Bronx, New York, was studying the biochemical components of animal venoms. He had a particular interest in the Gila monster (Heloderma suspectum), a venomous lizard native to the deserts of the American Southwest.
The Gila monster is an unusual creature. It eats only a few times a year — sometimes going months between meals — yet maintains remarkably stable blood sugar levels during these long fasts. Eng wanted to know why.
When he analyzed the lizard's venomous saliva, he found a peptide he named exendin-4. It shared 53% of its amino acid sequence with human GLP-1. And critically, exendin-4 was naturally resistant to DPP-4 degradation. Where human GLP-1 lasted two minutes, exendin-4 lasted hours.
The significance was immediately clear: here was a molecule that activated the same receptor as human GLP-1, with the same beneficial effects on insulin and blood sugar, but without the fatal half-life problem.
Eng licensed the discovery for pharmaceutical development. He couldn't have known it would eventually spawn a drug class worth hundreds of billions of dollars.
Myth vs. Fact: The Gila Monster and GLP-1 Drugs
Myth: “Ozempic is made from lizard venom.”
Fact: Ozempic (semaglutide) is a modified version of human GLP-1. It has no lizard-derived components. The first GLP-1 drug — exenatide (Byetta) — was based on a peptide found in Gila monster saliva. Later drugs like semaglutide and liraglutide were engineered from the human hormone, not from venom.
Myth: “GLP-1 drugs are brand new and untested.”
Fact: The science dates back to 1902. The first GLP-1 drug was approved in 2005. Semaglutide has been in clinical use since 2017. These medications have been tested in large randomized trials — including cardiovascular outcomes programs enrolling over 60,000 participants across the major GLP-1 CVOTs, plus additional large trials like SELECT (17,604 participants).
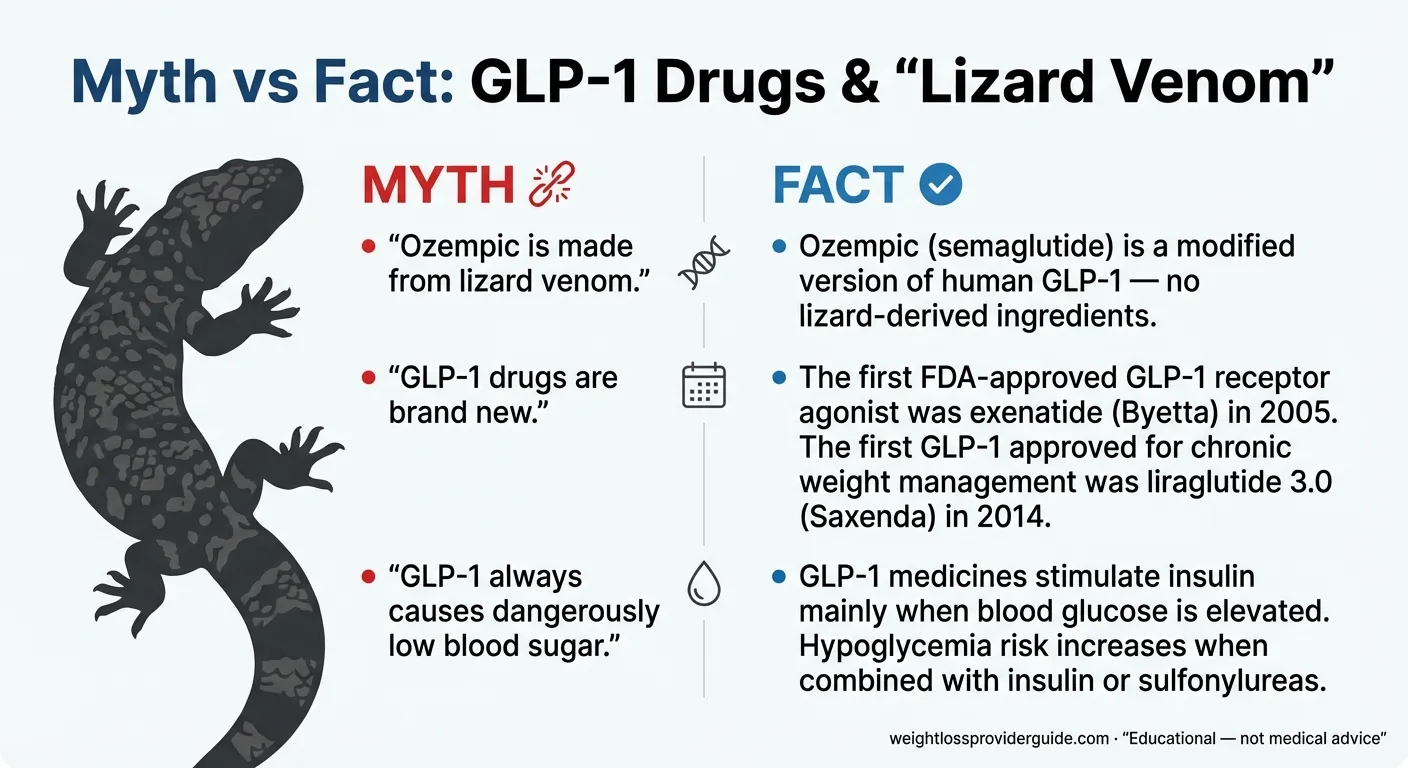
Common GLP-1 myths corrected with evidence-based facts.
From Venom to Pharmacy: Developing Exenatide
Dr. Josephine Egan at the National Institute on Aging and researchers at Amylin Pharmaceuticals began preclinical testing of synthetic exendin-4, designated “exenatide.” Animal studies confirmed it: exenatide potently stimulated insulin secretion, improved glucose control, and — intriguingly — seemed to have beneficial effects on the brain as well.
Meanwhile, Daniel Drucker and colleagues at the University of Toronto cloned the DNA encoding exendin-4 from the Gila monster's salivary gland. They confirmed that exendin-4 was encoded by a separate gene — not a lizard version of GLP-1 but an independent peptide that happened to activate the human GLP-1 receptor.
The drug development path from venom to pharmacy shelf took over a decade. But it would result in the first GLP-1 receptor agonist ever approved.
The Parallel Path: Novo Nordisk Engineers a Better GLP-1
While the Gila monster path led to exenatide, Novo Nordisk was pursuing a completely different engineering approach.
Since its founding, Novo Nordisk had focused on insulin. But in the early 1990s, the Danish company formed an innovation team to explore new therapeutic frontiers. By 1995, pharmaceutical scientist Lotte Bjerre Knudsen was leading the effort to make a long-acting version of human GLP-1 itself.
Her strategy was elegant: attach a fatty acid chain to the GLP-1 molecule at a specific position so it would bind to albumin (a large, abundant protein in the blood). Albumin acts like a slow-release vehicle — it protects the GLP-1 from enzymatic degradation and shields it from kidney clearance, dramatically extending its half-life.
Knudsen's team used mutagenesis to map which amino acid positions were critical for receptor binding and which could tolerate modification. They tested different fatty acid lengths, linker chemistry, and attachment sites. In 2000, they published the properties of their lead compound: liraglutide — a modified human GLP-1(7-37) with a 16-carbon fatty acid (palmitic acid) coupled via a glutamic acid spacer to lysine at position 26.
The result: a half-life of approximately 13 hours, compared to GLP-1's native 2 minutes. One injection per day instead of continuous infusion.
From the start, Knudsen believed this technology could treat obesity, not just diabetes. Earlier research from Ole Madsen at the University of Copenhagen had shown that transplanting glucagon-producing tumors into animals caused profound appetite loss, and studies by Bloom and colleagues had demonstrated that GLP-1 injected into the brains of rats dramatically reduced food intake.
She was right. But it would take another two decades for the world to catch up.
The FDA Approval Era: Every GLP-1 Drug, Every Milestone (2005–2019)
Every FDA-Approved GLP-1 Drug: The Complete Reference Table
Last Verified: February 2026
| Year | Brand Name | Generic Name | Manufacturer | Type | Approved For | Dosing | Key Notes |
|---|---|---|---|---|---|---|---|
| Apr 2005 | Byetta | Exenatide | Amylin/Lilly | Injection | Type 2 diabetes | Twice daily | First GLP-1 RA; derived from Gila monster exendin-4 |
| Jan 2010 | Victoza | Liraglutide | Novo Nordisk | Injection | Type 2 diabetes | Once daily | First once-daily GLP-1; modified human GLP-1 |
| Jan 2012 | Bydureon | Exenatide ER | AstraZeneca | Injection | Type 2 diabetes | Once weekly | First once-weekly GLP-1; microsphere formulation |
| Sep 2014 | Trulicity | Dulaglutide | Eli Lilly | Injection | Type 2 diabetes | Once weekly | GLP-1 fused to IgG4 antibody fragment |
| Dec 2014 | Saxenda | Liraglutide 3.0 mg | Novo Nordisk | Injection | Chronic weight management | Once daily | First GLP-1 approved for obesity |
| Jul 2016 | Adlyxin | Lixisenatide | Sanofi | Injection | Type 2 diabetes | Once daily | Short-acting; exendin-4 based |
| Dec 2017 | Ozempic | Semaglutide | Novo Nordisk | Injection | Type 2 diabetes | Once weekly | 7-day half-life; acylated human GLP-1 |
| Sep 2019 | Rybelsus | Oral semaglutide | Novo Nordisk | Oral tablet | Type 2 diabetes | Once daily | First oral GLP-1; uses SNAC absorption enhancer |
| Jun 2021 | Wegovy | Semaglutide 2.4 mg | Novo Nordisk | Injection | Chronic weight management | Once weekly | ~15% average weight loss (STEP trials) |
| May 2022 | Mounjaro | Tirzepatide | Eli Lilly | Injection | Type 2 diabetes | Once weekly | First dual GLP-1/GIP agonist |
| Nov 2023 | Zepbound | Tirzepatide | Eli Lilly | Injection | Chronic weight management | Once weekly | Up to 22.5% weight loss (SURMOUNT trials) |
Additional approved formulations: Soliqua (lixisenatide + insulin glargine, 2016), Xultophy (liraglutide + insulin degludec, 2016). Albiglutide (Tanzeum, GSK) was approved in 2014 but withdrawn from market in 2018 due to low commercial uptake.
Generics available: Exenatide (Byetta) generic launched Nov 2024. Liraglutide (Victoza) generics available since Dec 2024. Liraglutide (Saxenda) generic approved Aug 2025.
Data verified against FDA approval letters and drug labels as of February 2026.
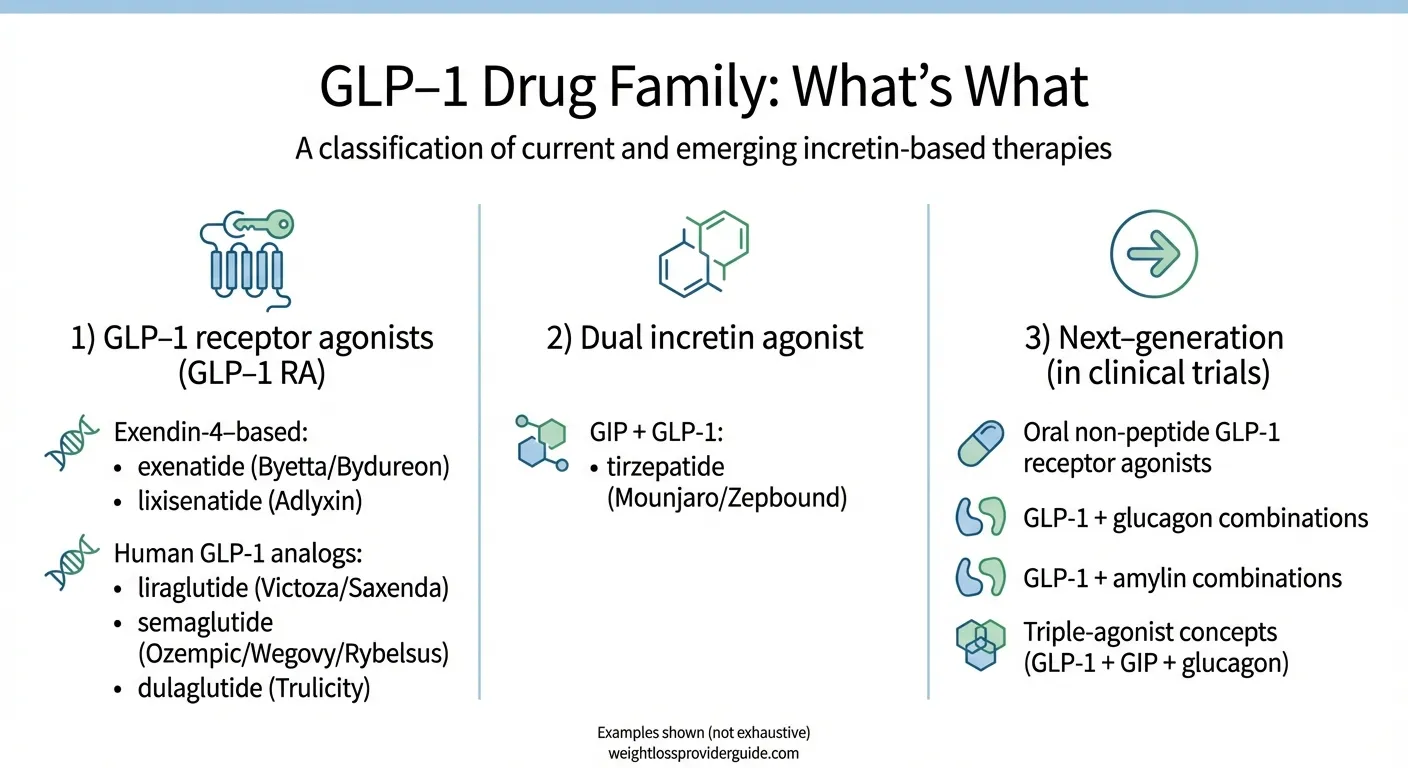
Classification of the GLP-1 drug family from first-generation to next-generation therapies.
2005: Exenatide (Byetta) — The Gila Monster Drug Reaches Patients
On April 28, 2005, the FDA approved exenatide (Byetta) for the treatment of type 2 diabetes. It was the first GLP-1 receptor agonist to reach patients.
It had taken almost 20 years from the identification of GLP-1 as a biologically active hormone to the first drug approval. Exenatide required twice-daily injections — inconvenient, but groundbreaking. For the first time, doctors had a diabetes drug that lowered blood sugar and didn't cause weight gain. Most diabetes medications at the time either caused weight gain (insulin, sulfonylureas) or were weight-neutral at best.
The drug was manufactured by Amylin Pharmaceuticals (later acquired through a chain of mergers by AstraZeneca). It proved the GLP-1 receptor agonist concept worked in humans. But twice-daily injections were a hard sell, and nausea was a common side effect — about 44% of patients experienced it initially.
The stage was set for longer-acting versions.
2010: Liraglutide (Victoza) — The First Once-Daily GLP-1
In January 2010, the FDA approved liraglutide (Victoza) for type 2 diabetes — the product of Lotte Knudsen's fatty acid engineering at Novo Nordisk. One injection per day, taken at any time, regardless of meals.
Victoza represented a different lineage than Byetta. Where exenatide descended from lizard venom, liraglutide was a modified version of the human GLP-1 molecule itself. This distinction matters because the human-based design meant fewer antibody reactions and a more predictable pharmacology.
Liraglutide would later prove its worth in the landmark LEADER trial (published in the New England Journal of Medicine in 2016), which demonstrated a 13% reduction in major cardiovascular events — the first time a GLP-1 drug proved it could protect the heart, not just lower blood sugar.
2012–2016: Weekly Dosing Arrives and the Weight Loss Door Opens
The next wave brought convenience and expanded indications:
2012: Bydureon (exenatide extended-release) became the first once-weekly GLP-1, using a microsphere slow-release technology. One injection per week instead of 14.
2014: Two pivotal approvals in one year. Dulaglutide (Trulicity) offered another once-weekly option, fusing GLP-1 to an antibody fragment to extend its half-life. It would become the top-selling GLP-1 by 2020.
And then the real game-changer: Saxenda (liraglutide 3.0 mg) was approved in December 2014 specifically for chronic weight management — the first GLP-1 drug with an obesity indication. This was the moment GLP-1 drugs crossed from the endocrinology clinic into the broader weight loss conversation.
2016: The LEADER cardiovascular outcomes trial transformed treatment guidelines. For the first time, a diabetes drug had proven it didn't just manage sugar — it reduced heart attacks and strokes. The American Diabetes Association rewrote its guidelines to recommend GLP-1 drugs for patients with cardiovascular risk.
2017: Semaglutide (Ozempic) — The Molecule That Changed Everything
In December 2017, the FDA approved semaglutide (Ozempic) for type 2 diabetes. On the surface, it was just another weekly GLP-1 injection. Under the surface, it was a quantum leap in pharmaceutical engineering.
Novo Nordisk's team had built on Knudsen's liraglutide platform with two key upgrades:
- An amino acid substitution (alpha-aminoisobutyric acid replacing alanine at position 8) that made the molecule nearly impervious to DPP-4 degradation
- An 18-carbon fatty diacid attached via a longer, more hydrophilic linker that bound even more tightly to albumin
The result: a half-life of approximately seven days — 5,000 times longer than natural GLP-1. One injection per week. One molecule that would reshape the pharmaceutical industry.
The SUSTAIN clinical trial program demonstrated superior glucose control compared to virtually every comparator, along with meaningful weight loss. But the real explosion was still four years away.
2019: Oral Semaglutide (Rybelsus) — The First GLP-1 Pill
Delivering a peptide drug orally was supposed to be impossible. Stomach acid destroys proteins. The gastrointestinal tract is designed to break apart exactly the kind of molecules that GLP-1 drugs are.
Novo Nordisk solved it. They combined semaglutide with an absorption enhancer called SNAC (sodium N-[8-(2-hydroxybenzoyl)amino] caprylate). SNAC raises the local pH in the stomach and temporarily increases cell membrane permeability, creating a brief window for semaglutide to cross the stomach lining intact.
In September 2019, oral semaglutide was approved as Rybelsus for type 2 diabetes — the first oral GLP-1 receptor agonist. The PIONEER trial program demonstrated effective glucose control, though with somewhat lower bioavailability than the injectable form (patients had to take it on an empty stomach with minimal water and wait 30 minutes before eating).
It was proof of concept. The idea that GLP-1 drugs could only be injections was officially dead.
The GLP-1 Explosion: How These Drugs Became the Most Talked-About Medications on Earth (2021–2026)
2021: Wegovy Launches and the World Pays Attention
On June 4, 2021, the FDA approved semaglutide 2.4 mg (Wegovy) for chronic weight management in adults with obesity or overweight with at least one weight-related condition.
The clinical data was staggering. In the STEP 1 trial (published in The New England Journal of Medicine), participants lost an average of approximately 15% of their body weight over 68 weeks — roughly three times what previous weight loss medications had achieved.
For context: a 250-pound person losing 15% of their weight drops nearly 38 pounds. Not from a crash diet. Not from surgery. From a weekly injection.
Demand overwhelmed supply almost immediately. Shortages began within months of launch and persisted for years. The FDA formally listed semaglutide products in shortage, which had significant legal and market consequences (more on that below).
Simultaneously, Ozempic — the diabetes formulation of the same molecule — became a cultural phenomenon. Celebrities, influencers, and social media users drove awareness (and controversy) to unprecedented levels. “Ozempic face,” “Ozempic babies,” and heated debates about who “deserved” access to these drugs dominated platforms from TikTok to the New York Times.
Between 2018 and 2023, prescriptions for GLP-1 drugs increased by more than 300%.
2022–2023: Tirzepatide and the Dual Agonist Revolution
While semaglutide dominated the conversation, Eli Lilly was building something different.
Tirzepatide doesn't just activate the GLP-1 receptor — it activates both the GLP-1 and GIP receptors simultaneously. It's built on a modified GIP backbone that also engages the GLP-1 receptor, creating a dual-action effect.
In May 2022, the FDA approved tirzepatide as Mounjaro for type 2 diabetes. In November 2023, it was approved for weight loss as Zepbound. The SURMOUNT-1 trial (published in NEJM) showed weight loss of up to 22.5% at the highest dose — the most ever achieved by a medication.
By 2024, Eli Lilly became the world's most valuable pharmaceutical company by market capitalization, driven largely by tirzepatide.
2024–2025: Beyond Diabetes and Weight Loss — A Cascade of New Approvals
What happened over the next two years fundamentally expanded what GLP-1 drugs are:
March 2024 — Cardiovascular risk reduction: The FDA approved Wegovy to reduce the risk of major adverse cardiovascular events (heart attack, stroke, cardiovascular death) in adults with obesity or overweight who also have established cardiovascular disease. This was based on the SELECT trial, which showed a 20% reduction in cardiovascular events — and was the first time a weight loss drug had ever proven cardiovascular protection. Participants in the trial did not need to have diabetes.
December 2024 — Obstructive sleep apnea: Zepbound (tirzepatide) became the first medication ever approved for obstructive sleep apnea, based on the SURMOUNT-OSA trial.
January 2025 — Kidney disease: Ozempic received approval to reduce the risk of kidney disease progression and kidney failure in adults with type 2 diabetes and chronic kidney disease, based on the FLOW trial.
August 2025 — Fatty liver disease (MASH): Wegovy received accelerated approval for noncirrhotic metabolic dysfunction-associated steatohepatitis (MASH) with moderate to advanced liver fibrosis (stages F2–F3), based on the ESSENCE trial. It became the only GLP-1 approved for a liver disease indication.
October 2025 — Oral semaglutide for cardiovascular risk: Rybelsus (oral semaglutide 14 mg) gained a cardiovascular risk reduction indication based on the SOUL trial, showing a 14% reduction in major cardiovascular events over approximately 5 years.
Late 2025 — Oral Wegovy tablet: Novo Nordisk received FDA approval for a 25 mg oral semaglutide formulation (Wegovy tablet) for chronic weight management and cardiovascular risk reduction.
January 2026 — Ozempic tablets: The FDA approved the rebrand/reformulation of oral semaglutide under the Ozempic brand name for diabetes, completing the oral lineup.
The pattern is unmistakable: GLP-1 drugs are no longer “diabetes drugs” or even “weight loss drugs.” They are becoming a new category of cardiometabolic medicine with applications across organ systems.
The Shortage Crisis and Compounding Controversy
The demand surge created a crisis. Starting in 2022, semaglutide (both Ozempic and Wegovy) was in persistent shortage. Patients with diabetes who depended on these medications couldn't get them filled. Wait lists stretched for months.
Under federal law, when a drug is in shortage, compounding pharmacies can produce copies. This legal opening created a parallel market for compounded semaglutide — often sold through telehealth platforms at lower prices. However, compounded versions are not FDA-approved, may use different salt forms (like semaglutide sodium vs. the branded semaglutide base), and lack the regulatory oversight of manufactured drugs.
On February 21, 2025, the FDA determined the shortage of semaglutide injection products was resolved. The agency provided a transition period before enforcement: 503A state-licensed pharmacies had until April 22, 2025, and 503B outsourcing facilities had until May 22, 2025, to cease compounding semaglutide products that are “essentially a copy” of the FDA-approved drug. This triggered lawsuits from compounding pharmacy trade associations and intense debate about access, affordability, and patient safety.
The FDA has issued explicit warnings about unapproved GLP-1 products, noting risks including incorrect dosing, contamination, and lack of sterility assurance. If you're evaluating any GLP-1 medication, checking whether it's an FDA-approved product from a licensed pharmacy is essential.
2024 Lasker Award: The Science Finally Gets Its Due
The 2024 Lasker-DeBakey Clinical Medical Research Award was given to three scientists for the work that made GLP-1 drugs possible:
- Joel Habener, MD — for his laboratory's role in identifying the GLP-1 peptide sequence
- Svetlana Mojsov, PhD — for isolating the biologically active form of GLP-1
- Lotte Bjerre Knudsen, PhD — for engineering sustained-acting GLP-1 drugs into clinical reality
The award was notable for finally including Mojsov, whose contributions had been overlooked in previous prizes. The Lasker Foundation's citation recognized the distinct and complementary skills each scientist brought: molecular biology, peptide chemistry, and pharmaceutical engineering.
How GLP-1 Drugs Actually Work: The Mechanism Explained
The 60-Second Version
GLP-1 is a hormone your gut naturally produces after you eat. It does four things simultaneously:
- Tells your pancreas to release insulin (but only when blood sugar is actually elevated — this built-in safety switch is why GLP-1 drugs rarely cause dangerously low blood sugar when used without insulin or sulfonylureas)
- Suppresses glucagon (the hormone that tells your liver to dump more sugar into your blood)
- Slows gastric emptying (food stays in your stomach longer, so you feel full longer)
- Acts on your brain (specifically the hypothalamus and brainstem) to reduce appetite and increase feelings of satiety
Natural GLP-1 does all of this. The problem is it disappears in about 2 minutes, destroyed by the DPP-4 enzyme.
GLP-1 drugs are engineered versions that resist degradation and last hours to days, amplifying these natural effects to a therapeutic level.
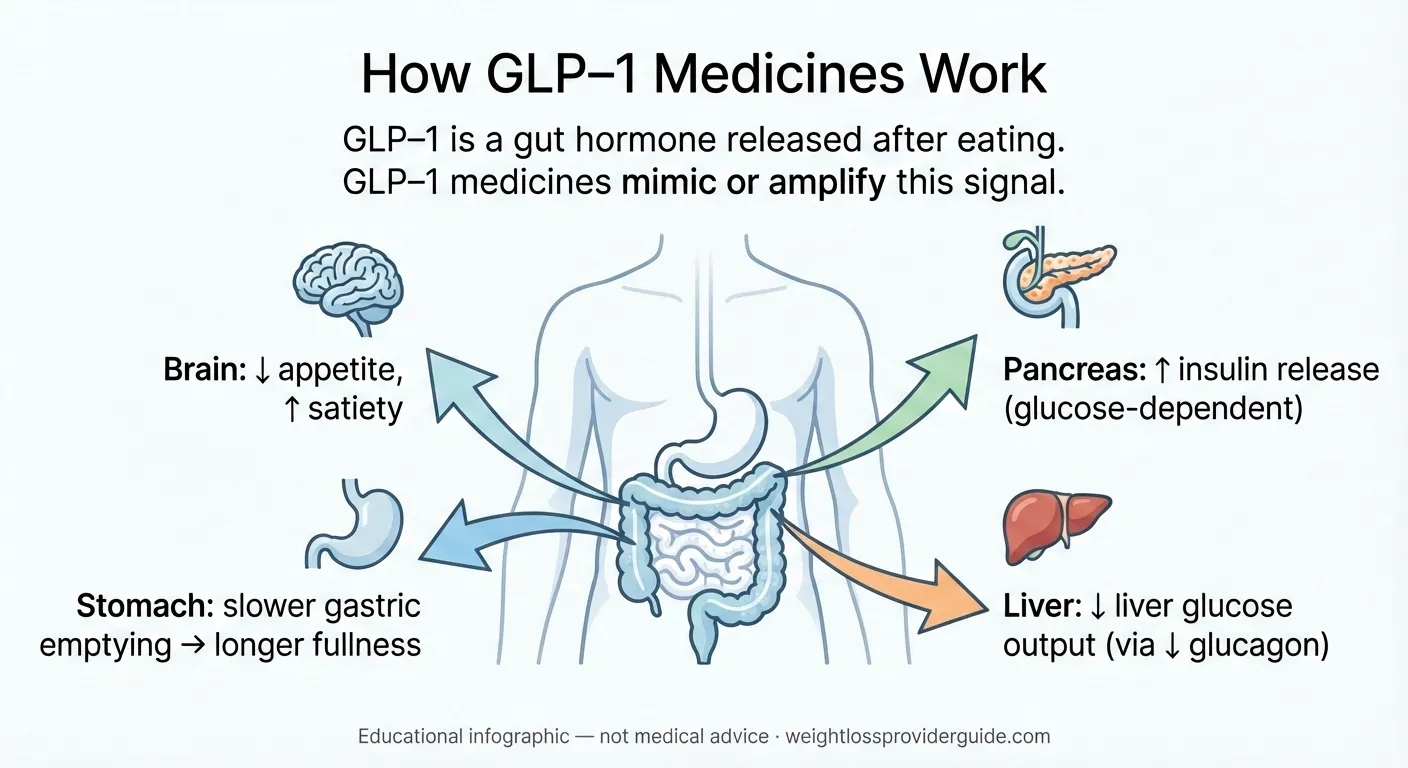
Simplified diagram of GLP-1 drug mechanisms. For educational purposes only.
Why There Are Different Types
Not all GLP-1 drugs are built the same way:
Exendin-4 based (from Gila monster venom): Exenatide (Byetta, Bydureon) and lixisenatide (Adlyxin) are synthetic copies of the Gila monster peptide. They activate the GLP-1 receptor but are structurally different from human GLP-1.
Modified human GLP-1: Liraglutide (Victoza, Saxenda), semaglutide (Ozempic, Wegovy, Rybelsus), and dulaglutide (Trulicity) are modified versions of the human GLP-1 sequence. Different engineering strategies — fatty acid acylation, IgG fusion, amino acid substitution — extend their half-lives from minutes to days.
Dual and triple agonists: Tirzepatide (Mounjaro, Zepbound) activates both the GLP-1 and GIP receptors. Next-generation drugs in development target GLP-1 + glucagon (survodutide) or GLP-1 + GIP + glucagon (retatrutide). These combinations may produce greater effects by engaging multiple metabolic pathways simultaneously.
Small molecule agonists: Orforglipron (in development by Eli Lilly) is not a peptide at all — it's a small molecule that activates the GLP-1 receptor. This means it can be taken as a simple daily pill without the special absorption enhancers that oral semaglutide requires.
The “Incretin Effect” — Why Oral Glucose Triggers More Insulin Than IV Glucose
This is the foundational concept behind the entire drug class.
When you eat a meal, your gut releases GLP-1 and GIP into the bloodstream. These hormones travel to the pancreas and amplify the insulin response — producing 50–70% more insulin than blood sugar alone would trigger. This amplification is called the incretin effect.
In type 2 diabetes, the incretin effect is impaired. The pancreas becomes less responsive to these gut signals. GLP-1 drugs restore this response by flooding the system with a potent, long-lasting version of the signal.
In people without diabetes who use GLP-1 drugs for weight loss, the primary mechanism shifts toward appetite suppression and slowed gastric emptying. The drugs reduce hunger signals in the brain, food stays in the stomach longer, and people naturally eat less — not through willpower but through altered physiology.
What's Coming Next: The GLP-1 Pipeline (2026 and Beyond)
The current generation of GLP-1 drugs is already transformative. What's in development may make them look like version 1.0.
Oral GLP-1s: The End of Injections
Oral Wegovy (semaglutide 25 mg tablet) launched in January 2026, becoming the first oral GLP-1 approved for weight loss. It still requires the same empty-stomach dosing as Rybelsus, but it eliminates the injection barrier entirely.
Orforglipron (Eli Lilly) is the most watched pipeline drug. It's a non-peptide small molecule GLP-1 receptor agonist — meaning it can be taken as a simple daily pill without the absorption enhancer technology that oral semaglutide needs. No fasting requirements. No special timing. Phase 3 trials showed approximately 11% body weight loss at 72 weeks. An FDA decision is expected in the first half of 2026. Analysts project $16 billion in annual sales by 2031.
Dual and Triple Agonists: Pushing Beyond GLP-1 Alone
CagriSema (Novo Nordisk): A combination of semaglutide (GLP-1 agonist) with cagrilintide (an amylin analog). Amylin is a hormone co-secreted with insulin that promotes fullness. Phase 3 REDEFINE trials showed approximately 22.7% mean weight loss at 68 weeks. Filing and FDA review expected in 2026.
Survodutide (Boehringer Ingelheim / Zealand Pharma): A dual GLP-1 and glucagon receptor agonist. Glucagon agonism promotes fat burning and energy expenditure. Phase 3 trials showed 14.9% weight loss at 49 weeks, with additional promise for MASH (fatty liver disease). FDA decision possible in 2027.
Retatrutide (Eli Lilly): The first triple agonist — activating GLP-1, GIP, and glucagon receptors simultaneously. Phase 2 data showed up to 24% body weight loss. Phase 3 readouts expected in 2026–2027. Analysts project $30 billion in revenue by 2031. This may represent the ceiling of what hormonal weight loss therapy can achieve.
MariTide (maridebart cafraglutide/AMG 133, Amgen): A long-acting injectable that combines GLP-1 receptor agonism with GIP receptor antagonism — a fundamentally different approach than tirzepatide's dual agonism. Its antibody-peptide conjugate structure provides a ~21-day half-life, designed for monthly or less frequent dosing. Phase 2 data showed up to 20% weight loss at 52 weeks. Phase 3 MARITIME program underway. FDA approval possible 2028 or later.
Amycretin (Novo Nordisk): A novel single-molecule GLP-1 and amylin receptor agonist, available in both injectable and oral formulations. Moving to Phase 3 in early 2026.
VK2735 (Viking Therapeutics): An oral dual GLP-1/GIP receptor agonist. In the Phase 2 VENTURE-Oral trial, Viking reported up to 12.2% mean weight loss from baseline at 13 weeks, and up to 10.9 percentage points greater weight loss than placebo, with weight loss still progressing at week 13 (no plateau observed). Phase 3 VANQUISH program initiated.
New Conditions Being Investigated
GLP-1 receptors are expressed throughout the body — in the brain, heart, kidneys, liver, and immune system. Researchers are now testing whether GLP-1 drugs can treat conditions far beyond diabetes and obesity:
- Alzheimer's disease: The EVOKE trial is testing semaglutide for early Alzheimer's. GLP-1 receptor activation appears to reduce neuroinflammation and may slow cognitive decline.
- Addiction: Preclinical evidence suggests GLP-1 drugs reduce alcohol, nicotine, and opioid cravings by modulating the brain's reward circuits. Human trials are underway.
- Polycystic ovary syndrome (PCOS): GLP-1 drugs improve insulin sensitivity and may address the metabolic dysfunction underlying PCOS.
- Heart failure: Semaglutide for heart failure with preserved ejection fraction (HFpEF) in patients with obesity is under FDA review.
- Osteoarthritis: Trials evaluating whether GLP-1-mediated weight loss reduces joint pain and disability.
Not all of these will pan out. But the breadth of investigation reflects how fundamentally GLP-1 biology intersects with human health.
The Access Question: Cost, Insurance, and the Path Forward
The biggest barrier to GLP-1 drugs isn't the science. It's the price tag.
Brand-name injectable GLP-1 medications cost approximately $900–1,300 per month without insurance. Many insurance plans still don't cover them for weight loss, or require extensive prior authorization. This has created significant health equity concerns — the people who could benefit most are often the least able to afford them.
Several developments are changing the landscape:
- Generic liraglutide became available in late 2024 (Victoza generics) and 2025 (Saxenda generic), bringing costs down substantially for liraglutide-based treatments.
- Cash-pay options and manufacturer discounts: In late 2025 and early 2026, Novo Nordisk and Eli Lilly expanded savings programs and entered pricing agreements to reduce costs for eligible patients. Actual out-of-pocket prices vary by insurance coverage, pharmacy, and program. Always verify current pricing directly with the pharmacy or provider.
- Competition: With 1–2 new GLP-1 drug launches expected annually through 2030, increased competition should apply downward pressure on pricing.
- Oral formulations: Pills are generally cheaper to manufacture and distribute than injectable biologics. The oral GLP-1 wave (Wegovy pill, orforglipron, VK2735) could fundamentally reshape the cost structure.
When Did GLP-1 Drugs Become Popular — and Why That Timing Matters
This is one of the most-searched questions about GLP-1 drugs, and the answer reveals something important about the gap between scientific reality and public perception.
The scientific timeline: GLP-1 drugs have been available since 2005. Liraglutide was approved for weight loss in 2014. Ozempic launched in 2017. By the time the general public “discovered” these medications, they had already been prescribed to millions of patients for years.
The cultural tipping point: Everything changed in 2021–2022. Three forces collided simultaneously:
1. Unprecedented clinical results. The STEP 1 trial showed semaglutide producing ~15% body weight loss — roughly three times what any previous medication had achieved. The SURMOUNT trials then showed tirzepatide achieving over 20%. These weren't marginal improvements. They were paradigm shifts that forced the medical community to reclassify obesity treatment.
2. Celebrity and social media amplification. Reports of Hollywood celebrities and public figures using Ozempic for weight loss went viral. The hashtag #Ozempic accumulated billions of views across TikTok and Instagram. “Ozempic face” (the gaunt appearance some users developed from rapid weight loss) became tabloid fodder. The conversation became impossible to avoid, even for people with no personal interest in the drugs.
3. Supply shortages creating scarcity psychology. When Wegovy launched in 2021 and demand immediately overwhelmed supply, the shortage became a news story in itself. Scarcity amplified interest. People who couldn't get the drug talked about it constantly. People who hadn't heard of it learned about it through the shortage coverage. Telehealth startups raced to fill the gap, creating a direct-to-consumer GLP-1 market that barely existed two years earlier.
Why this matters for you: When someone says “GLP-1 drugs are new,” what they usually mean is “I just heard about them.” The science is decades old. The clinical use is two decades old. The weight loss applications are over a decade old. What's genuinely new is the scale of public awareness and the expanding range of indications (cardiovascular protection, kidney disease, liver disease, sleep apnea) approved since 2024.
This distinction matters because it directly addresses one of the most common fears: “Am I a guinea pig?” You're not. These drugs have been through some of the largest and longest clinical trials in pharmaceutical history, with the major cardiovascular outcomes trials alone enrolling over 60,000 participants. The people taking them in 2026 are benefiting from safety data spanning over 20 years of clinical use across millions of prescriptions.
Are GLP-1 Drugs Safe? What Two Decades of Data Actually Show
If you're considering a GLP-1 medication, or if you're reporting on them, this section is about what we know, what we don't know, and where the honest uncertainties remain.
What Side Effects Are Common
Gastrointestinal effects are the most frequently reported side effects, and they're directly related to how these drugs work. Slowed gastric emptying can cause:
- Nausea (most common — reported in up to 44% of patients initially with some formulations, but typically decreases significantly over the first few weeks)
- Vomiting, diarrhea, and constipation (also generally improve with time)
- Injection site reactions (less common with newer long-acting formulations)
These side effects are why GLP-1 drugs are started at low doses and titrated up gradually — a process called “dose escalation.” Most patients who stick through the initial adjustment period find these effects manageable or absent at steady state.
The Thyroid Cancer Question
Every GLP-1 drug label carries a boxed warning about thyroid C-cell tumors, including medullary thyroid cancer (MTC). This is based on animal studies — in rodents, long-term GLP-1 exposure stimulated calcitonin secretion and led to C-cell tumors.
However: this effect has not been observed in humans. No increased calcitonin secretion has been seen in human studies. Large retrospective analyses — including studies with over 10 years of follow-up — have not found an increased risk of thyroid cancer in people taking GLP-1 drugs. One French cohort study reported a signal at 1–3 years of use, but other large studies have not replicated this finding.
GLP-1 drugs remain contraindicated in people with a personal or family history of medullary thyroid cancer or multiple endocrine neoplasia type 2 (MEN2). This is a precautionary measure based on the animal data.
Pancreatitis
Early case reports raised concerns about a possible link between GLP-1 drugs and pancreatitis. Multiple large meta-analyses of clinical trial data have not found a reliable association with pancreatitis or pancreatic cancer. The American Association of Clinical Endocrinologists recommends caution in people with a history of pancreatitis, and discontinuation if acute pancreatitis occurs.
What We Don't Know Yet
Honesty demands acknowledging the open questions:
- Long-term muscle and bone effects: Rapid weight loss from any cause can reduce lean muscle mass and bone density. The degree to which this is a concern with GLP-1 drugs at current doses — and whether resistance exercise fully offsets it — is still being studied.
- Weight regain after stopping: Clinical trial data consistently shows that weight tends to return when GLP-1 drugs are discontinued. Whether this makes them “lifetime medications” is an active area of research and debate.
- Effects on fertility and pregnancy: GLP-1 drugs are not approved for use during pregnancy. Semaglutide labeling recommends discontinuing at least 2 months before a planned pregnancy due to its long washout period. For liraglutide (Saxenda), labeling advises discontinuing once pregnancy is recognized; clinicians may recommend stopping 10–14 days before planned conception given its shorter half-life. The “Ozempic babies” phenomenon (anecdotal reports of unexpected pregnancies while on GLP-1 drugs) is being investigated but not yet well understood.
- Eye health: A potential signal for non-arteritic anterior ischemic optic neuropathy (NAION) has been reported in some observational studies. This requires further research to determine if a causal relationship exists.
- Very long-term outcomes: Semaglutide has been available since 2017, tirzepatide since 2022. We don't yet have 20+ years of data on these specific molecules, though the GLP-1 drug class as a whole has been in use since 2005.
This is the reality: these are powerful medications with robust clinical evidence and an established safety profile, and there are legitimate open questions that ongoing research is addressing.
The Scientists Who Made It Happen
Behind every drug on the timeline table above is a human being who spent years — sometimes decades — pursuing an idea that most of their peers thought was a long shot. Here are the key figures:
Joel Habener, MD — Endocrinologist and molecular biologist at Massachusetts General Hospital. His laboratory's cloning of proglucagon sequences in the early 1980s revealed the existence of GLP-1 and GLP-2. Habener's lab became the intellectual home base for much of the early GLP-1 research. 2024 Lasker Award recipient.
Svetlana Mojsov, PhD — Peptide chemist, currently at Rockefeller University. Mojsov identified the biologically active fragment of GLP-1 (positions 7-36/37), synthesized it, created the antibodies to track it, and was a co-author on the key papers proving it stimulated insulin. She fought for recognition and patent inclusion for years before the 2024 Lasker Award acknowledged her contributions. Her story is a case study in how scientific credit can be shaped by institutional politics and gender.
Daniel J. Drucker, MD — Professor at the University of Toronto. Drucker demonstrated GLP-1's ability to stimulate insulin gene transcription, proved its effects on food intake and body weight in animals, led foundational work on GLP-1 receptor biology and GLP-2, and has been one of the most prolific translational researchers in diabetes history. 2017 Harrington Award. 2021 Gairdner Award.
Jens Juul Holst, MD, DMSc — Professor at the University of Copenhagen. Holst independently demonstrated GLP-1's insulinotropic activity around the same time as the MGH team. His decades of work on incretin physiology provided much of the biological foundation for the entire drug class. 2021 Gairdner Award.
John Eng, MD — Endocrinologist at the Veterans Affairs Medical Center in the Bronx, New York. Eng discovered exendin-4 in Gila monster venom in the early 1990s and licensed the discovery that led directly to exenatide (Byetta), the first approved GLP-1 drug.
Lotte Bjerre Knudsen, PhD — Pharmaceutical scientist at Novo Nordisk. Knudsen led the team that developed the fatty acid acylation platform underlying liraglutide and semaglutide. She championed the idea that GLP-1 drugs could treat obesity when most of the field was focused solely on diabetes. 2024 Lasker Award recipient.
Josephine Egan, MD — Researcher at the National Institute on Aging. Egan led preclinical testing of exendin-4 for diabetes and later discovered neuroprotective effects of GLP-1 receptor activation, helping launch the neurodegenerative disease research pipeline.
The Clinical Trials That Changed Practice
For journalists, researchers, and anyone who wants to understand why these drugs gained their current indications, here are the pivotal trials:
| Trial Name | Year | Drug | Key Finding | Significance |
|---|---|---|---|---|
| LEADER | 2016 | Liraglutide | 13% reduction in major cardiovascular events | First GLP-1 to prove cardiovascular benefit |
| SUSTAIN-6 | 2016 | Semaglutide (inj.) | 26% reduction in cardiovascular events | Confirmed semaglutide's CV profile |
| PIONEER 6 | 2019 | Oral semaglutide | Non-inferiority for CV safety | Validated oral GLP-1 approach |
| STEP 1 | 2021 | Semaglutide 2.4 mg | ~15% mean weight loss at 68 weeks | Established GLP-1s as first-line obesity treatment |
| SURMOUNT-1 | 2022 | Tirzepatide | Up to 22.5% weight loss at 72 weeks | Highest medication-induced weight loss ever recorded |
| SELECT | 2023 | Semaglutide 2.4 mg | 20% reduction in CV events (obesity, no diabetes) | First weight loss drug to prove cardiovascular protection |
| SURMOUNT-OSA | 2024 | Tirzepatide | Significant reduction in sleep apnea severity | First medication approved for OSA |
| FLOW | 2024 | Semaglutide | Reduced kidney disease progression | First GLP-1 approved for CKD |
| ESSENCE | 2025 | Semaglutide 2.4 mg | Improvement in liver fibrosis (MASH) | First GLP-1 approved for liver disease |
| SOUL | 2025 | Oral semaglutide | 14% reduction in MACE over ~5 years | Validated oral semaglutide for CV protection |
All trials listed above were multi-center, randomized, placebo-controlled studies published in peer-reviewed journals.
Frequently Asked Questions About the History of GLP-1 Drugs
Glossary: Key Terms Explained
If you've encountered unfamiliar terms in this article (or in your research), here's a quick reference:
GLP-1 (Glucagon-Like Peptide-1): A hormone produced by L-cells in the gut after eating. It stimulates insulin release, suppresses glucagon, slows gastric emptying, and reduces appetite.
GLP-1 Receptor Agonist (GLP-1 RA): A drug that activates the GLP-1 receptor, mimicking or enhancing the effects of natural GLP-1. Examples: semaglutide, liraglutide, exenatide, dulaglutide.
Incretin: A gut hormone that amplifies insulin secretion in response to food. The two main incretins are GLP-1 and GIP.
GIP (Glucose-Dependent Insulinotropic Polypeptide): The other major incretin hormone, first identified in the 1970s. GIP works alongside GLP-1. Tirzepatide targets both GLP-1 and GIP receptors.
DPP-4 (Dipeptidyl Peptidase-4): The enzyme that rapidly breaks down natural GLP-1 (and GIP) in the body. GLP-1 drugs are engineered to resist DPP-4 degradation.
Exendin-4: A peptide found in Gila monster venom that mimics GLP-1 but is naturally resistant to DPP-4. The basis for exenatide (Byetta, Bydureon).
MACE (Major Adverse Cardiovascular Events): A composite endpoint in clinical trials typically including cardiovascular death, non-fatal heart attack, and non-fatal stroke.
MASH (Metabolic Dysfunction-Associated Steatohepatitis): A form of fatty liver disease involving inflammation and liver cell damage, previously called NASH. Can progress to cirrhosis.
OSA (Obstructive Sleep Apnea): A condition where the airway repeatedly collapses during sleep, causing breathing interruptions. Zepbound is the first FDA-approved medication for OSA.
Accelerated Approval: An FDA pathway that allows earlier approval of drugs for serious conditions based on a surrogate or intermediate endpoint, with the requirement for confirmatory trials.
CVOT (Cardiovascular Outcomes Trial): Large, long-term clinical trials required by the FDA since 2008 to ensure diabetes drugs don't increase cardiovascular risk. Several GLP-1 CVOTs showed not just safety but benefit.
How to Verify a GLP-1 Medication Is Legitimate
With the explosion of telehealth platforms, compounding pharmacies, and direct-to-consumer marketing, knowing whether you're getting an FDA-approved product has become genuinely important. The FDA has issued specific guidance on unapproved GLP-1 products, and here's what you should know:
FDA-approved GLP-1 drugs come from licensed manufacturers (Novo Nordisk, Eli Lilly, AstraZeneca, Sanofi), are dispensed by licensed pharmacies, include FDA-approved labeling, and have a National Drug Code (NDC) number you can verify.
Compounded GLP-1 products are mixed by compounding pharmacies, often using different salt forms (like semaglutide sodium instead of semaglutide base). They are not FDA-approved, have not undergone the same manufacturing quality controls, and may carry risks including incorrect dosing, contamination, or sterility issues. The legal status of compounded semaglutide changed after the FDA declared the shortage resolved in February 2025.
Red flags to watch for:
- Products marketed as “generic Ozempic” or “generic Wegovy” (no generics exist for semaglutide as of early 2026)
- Prices that seem dramatically lower than any legitimate source
- Products shipped without proper cold chain storage (semaglutide requires refrigeration before first use)
- Providers who prescribe without any medical evaluation or history
- Products from overseas pharmacies not licensed in the United States
This isn't about being paranoid — it's about safety. The FDA's concerns about unapproved GLP-1 products are well documented and worth reading if you're evaluating any non-standard source.
What to Do Next
Now you have the full picture — 120 years of science, every approval, every scientist, every drug in the pipeline. Here's where to go from here based on what brought you to this page:
If you're researching GLP-1 drugs for yourself or a family member: Understanding the history is important, but your next step is talking to a healthcare provider about whether these medications make sense for your specific situation. If you're comparing online providers and pricing, we've done extensive research on that:
- Best Online GLP-1 Providers Compared (2026) — verified pricing across telehealth platforms, honest reviews, and provider-specific details
- Cheapest GLP-1 Options Without Insurance — a cost-focused breakdown for self-pay patients
- Cheapest Tirzepatide Online Without Insurance — real prices, ranked
- Best GLP-1 Telehealth Providers (2026) — ranked and reviewed
- How to Get GLP-1 Without Insurance — step-by-step guide
- Semaglutide vs. Tirzepatide — head-to-head comparison
If you're a journalist or content creator: We list primary sources for all major claims in this article — FDA approval letters, peer-reviewed trials, and official award citations. Our complete reference list is below. You're welcome to cite this timeline with attribution. Contact us for additional information, corrections, or press inquiries.
If you want to stay updated: This page is maintained and updated as new approvals, clinical trial results, and regulatory changes occur. Bookmark it. We'll keep it current.
More resources: Do I Qualify for Wegovy? · GLP-1 Eligibility · Microdosing Tirzepatide · Oral Tirzepatide FDA Status · Best Oral Tirzepatide · MEDVi Reviews · GLP-1 Pricing Index · Semaglutide Providers in Texas · Compare Providers
Sources, Methodology, and Update Policy
How We Built This Timeline
This article was compiled from primary scientific literature, FDA regulatory documents, and authoritative medical databases. Our source categories include:
Regulatory sources: FDA approval letters, drug labels (via FDA AccessData), FDA press announcements, FDA safety communications
Scientific literature: Original research papers published in Nature, The New England Journal of Medicine, The Lancet, PNAS, Journal of Clinical Investigation, Diabetes, and Diabetologia; accessed via PubMed and PubMed Central
Award citations: Lasker Foundation, Gairdner Foundation
Clinical trial data: ClinicalTrials.gov registrations; published trial results in peer-reviewed journals
Pipeline and market data: Company press releases, FDA filings, Prime Therapeutics pipeline reports, Clarivate Drugs to Watch 2026
Prescription and market statistics: Fair Health data, CMS databases, FDA shortage database
What We Don't Do
- We do not provide medical advice. This is an informational resource. Consult your healthcare provider for treatment decisions.
- We do not make unsourced health claims. Factual assertions in this article are supported by the primary sources listed in our references section, derived from FDA-approved labeling, or clearly marked as our analysis.
- We are not medical professionals. We are a research team that specializes in GLP-1 provider comparison and patient education.
Update and Verification Policy
This page is reviewed and updated when:
- A new GLP-1 drug receives FDA approval
- An existing drug receives a new indication or label change
- Significant clinical trial results are published
- FDA safety communications are issued
- Pricing, availability, or access conditions materially change
“Last Updated” reflects the most recent editorial review. “Last Verified” reflects the most recent verification of all drug data, approval dates, and pricing information against primary sources.
Affiliate Disclosure
Weight Loss Provider Guide earns commissions from some links on this site. Our comparison methodology is published separately and applies equally to all providers regardless of affiliate status.
Key References
- Bayliss WM, Starling EH. “The mechanism of pancreatic secretion.” J Physiol. 1902.
- McIntyre N, Holdsworth CD, Turner DS. “New interpretation of oral glucose tolerance.” The Lancet. 1964.
- Bell GI, Sanchez-Pescador R, et al. “Exon duplication and divergence in the human preproglucagon gene.” Nature. 1983.
- Mojsov S, Weir GC, Habener JF. “Insulinotropin: glucagon-like peptide I (7-37) co-encoded in the glucagon gene is a potent stimulator of insulin release in the perfused rat pancreas.” J Clin Invest. 1987.
- Drucker DJ, Philippe J, Mojsov S, et al. “Glucagon-like peptide I stimulates insulin gene expression and increases cyclic AMP levels in a rat islet cell line.” PNAS. 1987.
- Eng J, Kleinman WA, Singh L, et al. “Isolation and characterization of exendin-4, an exendin-3 analogue, from Heloderma suspectum venom.” J Biol Chem. 1992.
- Knudsen LB, Nielsen PF, Huusfeldt PO, et al. “Potent derivatives of glucagon-like peptide-1 with pharmacokinetic properties suitable for once daily administration.” J Med Chem. 2000.
- Marso SP, Daniels GH, et al. “Liraglutide and cardiovascular outcomes in type 2 diabetes.” NEJM. 2016. (LEADER trial)
- Wilding JPH, Batterham RL, et al. “Once-weekly semaglutide in adults with overweight or obesity.” NEJM. 2021. (STEP 1 trial)
- Jastreboff AM, Aronne LJ, et al. “Tirzepatide once weekly for the treatment of obesity.” NEJM. 2022. (SURMOUNT-1 trial)
- Lincoff AM, Brown-Frandsen K, et al. “Semaglutide and cardiovascular outcomes in obesity without diabetes.” NEJM. 2023. (SELECT trial)
- Friedman JM. “The discovery and development of GLP-1 based drugs that have revolutionized the treatment of obesity.” PNAS. 2024. (Lasker Award article)
- Drucker DJ. “The GLP-1 journey: from discovery science to therapeutic impact.” J Clin Invest. 2024.
- Lasker Foundation. “GLP-1-based therapy for obesity.” 2024 Award Citation.
- FDA approval letters and drug labels: Byetta (2005), Victoza (2010), Saxenda (2014), Ozempic (2017), Rybelsus (2019), Wegovy (2021), Mounjaro (2022), Zepbound (2023). Accessed via FDA AccessData.
- FDA press announcements: Wegovy CV indication (2024), Zepbound OSA (2024), Ozempic CKD (2025), Wegovy MASH (2025), Ozempic tablets (2026).
- FDA. “FDA's Concerns with Unapproved GLP-1 Drugs Used for Weight Loss.” Safety Communication.
- Prime Therapeutics. “GLP-1 Pipeline Update.” November 2025.
- Clarivate. “Drugs to Watch 2026.” January 2026.
- Fair Health. GLP-1 prescription trend data, 2019–2024.
This page is maintained by the WPG Research Team at Weight Loss Provider Guide. For corrections, updates, or press inquiries, contact us. For provider comparisons and current pricing, visit our GLP-1 Provider Comparison Hub. Read our medical disclaimer.