Disclosure: Some links on this site are affiliate links. If you purchase through these links, we may earn a commission at no extra cost to you. Thank you for supporting our site.·For informational purposes only—not medical advice.
Best GLP-1 for PCOS: Which Medication Actually Works for Your Symptoms?
The Bottom Line (Read This First)
Best GLP-1 for most women with PCOS: Semaglutide
Semaglutide (Wegovy / Ozempic class) has growing PCOS-specific evidence plus strong obesity outcomes overall, and is widely available as a compounded option starting at $179/month through telehealth programs like MEDVi. PCOS Guideline, 2023
Best for maximum weight loss + severe insulin resistance: Tirzepatide
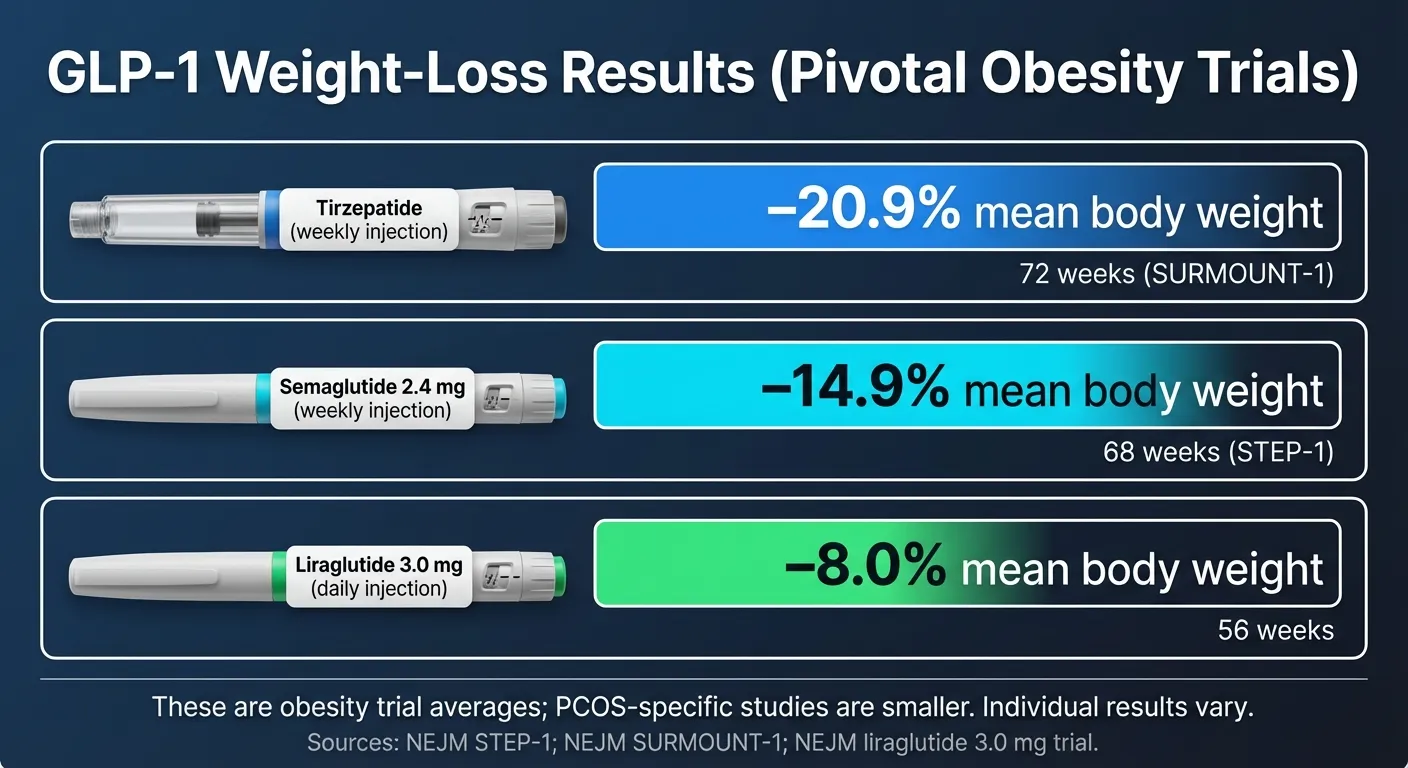
Tirzepatide (Mounjaro / Zepbound class) dual GLP-1 + GIP mechanism produced ~20% mean weight loss at higher doses in obesity trials, and beat semaglutide 2.4 mg head-to-head (−20.2% vs −13.7%). More expensive, but potentially worth it for significant insulin resistance or pre-diabetes. SURMOUNT-1, NEJM 2022; SURMOUNT-5, NEJM 2025
Do not use without medical guidance if:
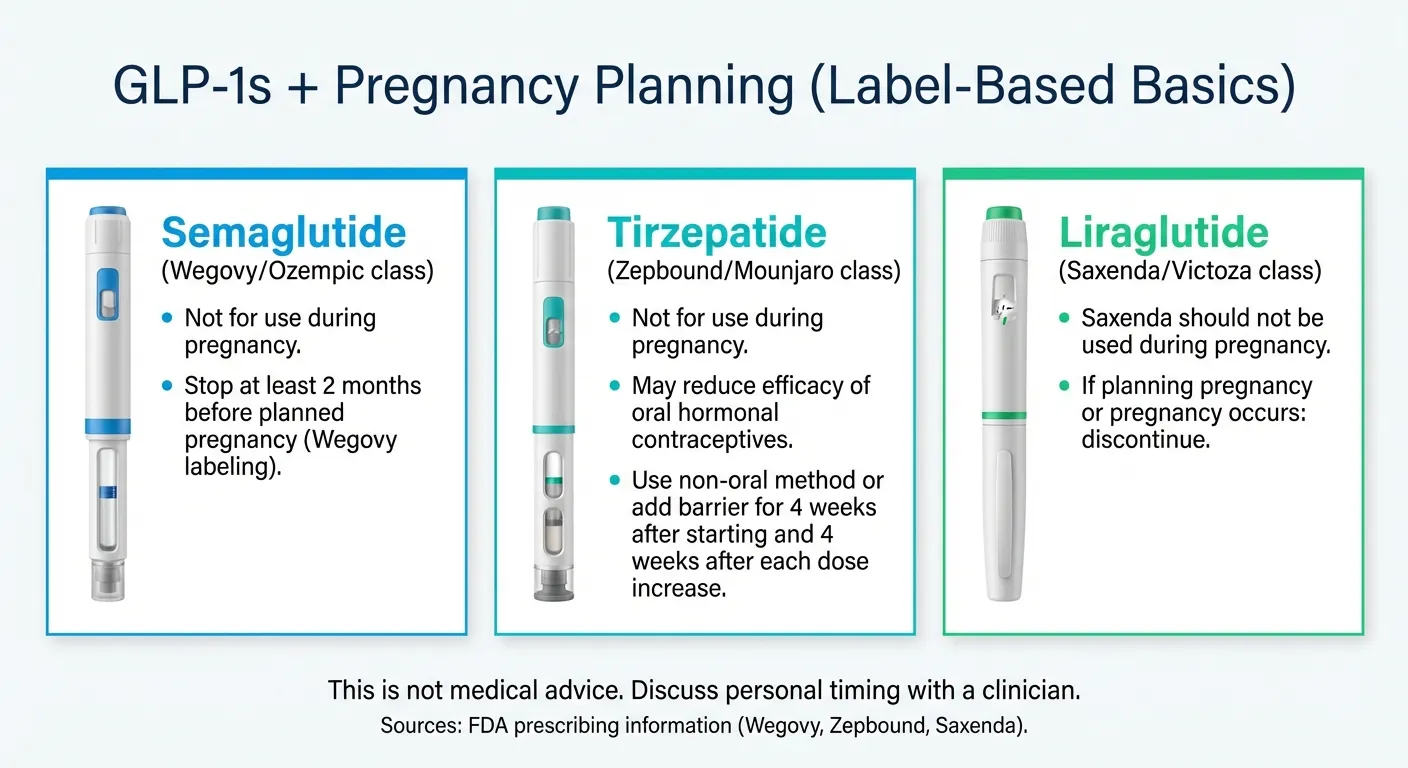
You have a personal/family history of medullary thyroid cancer (MTC) or MEN2 (contraindication), are pregnant, or are planning pregnancy soon — Wegovy labeling advises stopping ≥2 months before a planned pregnancy; Zepbound advises discontinuing when pregnancy is recognized. FDA Prescribing Information
Cost reality:
Brand-name GLP-1s are often $1,000+/month without coverage. Compounded programs start around $179–$199/month (as low as $146/month with a 6-month commitment), but compounded products are not FDA-approved as finished medications — careful provider verification is essential. FDA Warning on Unapproved GLP-1 Drugs
That’s the short version. Below, I’ll break down exactly which GLP-1 fits your specific situation, what the clinical evidence actually shows, how to access it safely, and what to watch out for.
If you have PCOS, I don’t need to explain the frustration. You’ve done everything “right” — the diets, the workouts, the metformin, maybe even the birth control pills — and the scale barely moves. Or it moves, then comes right back. Meanwhile, someone on Instagram lost 40 pounds on Ozempic in three months and you’re wondering: would that actually work for me?
Here’s what I found after reviewing clinical trials, meta-analyses, real-world data from over 300 million patient records, and the 2023 international PCOS guidelines: GLP-1 medications work for PCOS. Not as a miracle cure — but as the most effective medical tool for PCOS weight loss and insulin resistance that’s emerged in nearly 50 years.
The real question isn’t if they work. It’s which one, and how do you get it affordably.
How Do GLP-1 Medications Compare for PCOS? (Side-by-Side)
Before I get into the details, here’s what the data looks like when you put all three GLP-1 options next to each other — specifically for PCOS outcomes, not just general weight loss.
| Semaglutide (Ozempic, Wegovy, Rybelsus) | Tirzepatide (Mounjaro, Zepbound) | Liraglutide (Saxenda, Victoza) | |
|---|---|---|---|
| How it works | Targets GLP-1 receptor | Targets GLP-1 + GIP receptors (dual action) | Targets GLP-1 receptor |
| Average weight loss | 11.5% at 1 year (GLP-1 class, real-world PCOS data) | ~20% at higher doses (general obesity trials; PCOS data emerging) | ~4.6% body weight (PCOS trials) |
| Insulin resistance | Significant HOMA-IR improvement | Superior improvement (dual mechanism) | Moderate improvement |
| Testosterone reduction | Reductions vs placebo in some meta-analyses (results mixed) | Promising (less PCOS-specific data) | Documented in trials |
| Menstrual regularity | Improved in small PCOS studies (~71% of responders, n=27) | Expected (via weight loss/insulin correction; limited PCOS studies) | 76% in 20-week trial |
| Dosing | Once weekly (injection) or daily (oral) | Once weekly (injection only) | Daily injection |
| Oral option? | Yes (Rybelsus — less potent) | No | No |
| FDA-approved for PCOS? | No (off-label) | No (off-label) | No (off-label) |
| Brand-name cost (no insurance) | $1,000–$1,500/mo | $1,000–$1,500/mo | $1,300+/mo |
| Compounded cost | From $179–$199/mo | From $258–$349/mo | Rarely available |
| Most common side effects | Nausea, diarrhea (fade in 4–8 weeks) | Nausea, diarrhea (may be milder) | Nausea, injection site reactions |
| Fertility note | Stop ≥2 months before planned pregnancy | Stop when pregnancy recognized; switch to non-oral contraception for 4 weeks after each dose increase | Stop before conception |
| Best for (PCOS) | Growing PCOS evidence; most affordable compounded access | Maximum weight loss; severe insulin resistance | Longest PCOS trial history; shorter treatment courses |
All GLP-1 medications are off-label for PCOS. No GLP-1 is FDA-approved specifically for PCOS. Pricing verified February 2026. Weight loss data: SURMOUNT-1 (NEJM 2022), Epic Research (2025). Clinical data sourced from peer-reviewed meta-analyses and the 2023 International PCOS Guidelines.
Which GLP-1 Is Right for YOUR Type of PCOS?
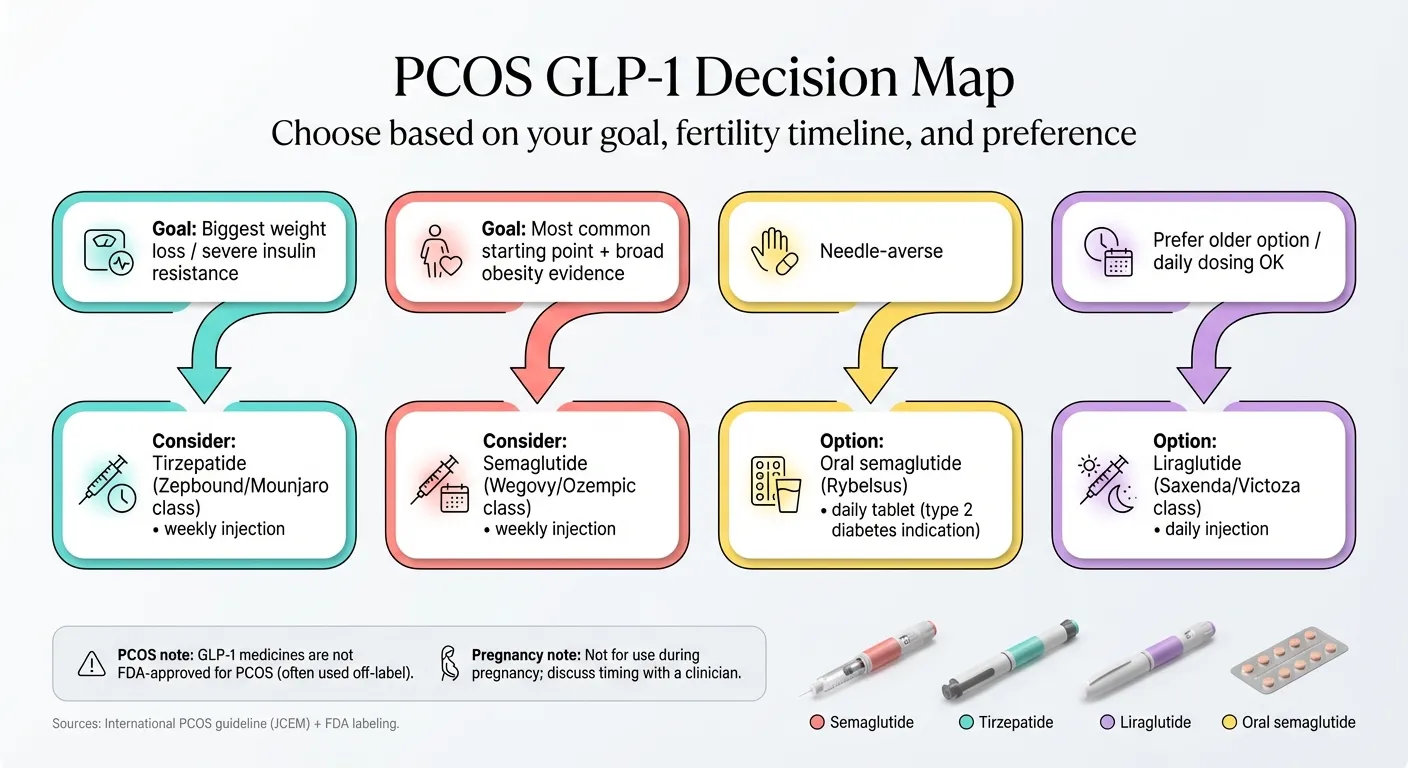
PCOS isn’t one-size-fits-all, and neither is medication choice. Here’s the decision framework I built after analyzing the research:
If your biggest problem is stubborn weight + insulin resistance
Go with tirzepatide (Mounjaro/Zepbound class). The dual GLP-1 + GIP mechanism hits both appetite and metabolic dysfunction harder than anything else available. In the SURMOUNT-1 obesity trial, patients on the highest dose (15 mg) achieved an average weight reduction of about 22.5% of their body weight at 72 weeks (NEJM, 2022). If you’ve tried metformin with limited results, have a BMI over 30, or your labs show worsening HOMA-IR or pre-diabetes, tirzepatide is the most powerful option on the table.
The tradeoff: it’s pricier. Compounded tirzepatide runs around $258–$499/month depending on the provider and dose. Through MEDVi, compounded tirzepatide is listed at $349 for the first month (promos may vary — verify during intake).
If you want the most-studied option with strong PCOS evidence
Go with semaglutide (Ozempic/Wegovy class). Semaglutide has growing PCOS-specific evidence plus strong obesity outcomes overall — and liraglutide actually has the longer PCOS trial history, but semaglutide is more potent and requires only weekly dosing (PubMed meta-analysis, 2024). In real-world data, GLP-1 medications (predominantly semaglutide) produced 11.5% median body weight reduction at one year in women with PCOS, and in a small PCOS study, ~71% of semaglutide responders achieved normal menstrual cycles after 6 months. It also has established cardiovascular benefit data, which matters because PCOS increases heart disease risk.
Semaglutide is also the most accessible. Compounded versions start at $179/month through telehealth programs, making it the most affordable entry point into GLP-1 therapy.
If fertility is your primary goal right now
Use GLP-1 therapy strategically, then stop before trying to conceive. Semaglutide (Wegovy) labeling advises discontinuing at least 2 months before a planned pregnancy. Tirzepatide (Zepbound) advises discontinuation when pregnancy is recognized. Neither is safe during pregnancy. But here’s the strategy that endocrinologists recommend: use a GLP-1 to lose weight and improve insulin sensitivity first, then transition off the GLP-1 and onto metformin (which is safe during TTC and pregnancy) to maintain your gains while you conceive.
Important if you’re on birth control pills while taking tirzepatide: The Zepbound label warns that tirzepatide may reduce oral contraceptive effectiveness due to delayed gastric emptying. Patients should switch to a non-oral contraceptive method or add a barrier method for 4 weeks after starting tirzepatide and for 4 weeks after each dose increase.
Even a 5% weight loss can restore ovulation in PCOS. The “Ozempic babies” phenomenon — unexpected pregnancies in women with PCOS on GLP-1s — is real, and it happens because weight loss + insulin correction can restore ovulation faster than expected. Use effective contraception while on GLP-1s if pregnancy isn’t the plan.
If you’re on a tight budget with no insurance coverage
Start with compounded semaglutide through a telehealth provider. Brand-name Wegovy or Zepbound costs $1,000–$1,500/month without insurance. Insurance coverage for PCOS specifically is uncommon since it’s off-label.
Several reputable telehealth programs now offer compounded semaglutide at a fraction of brand-name cost. MEDVi starts at $179 for the first month ($299 refills) with no contracts and month-to-month flexibility — our top overall pick for the combination of PCOS-aware intake, transparent pricing, and verified reviews. Yucca Health offers the lowest monthly rate at as low as $146/month on a 6-month plan (pricing confirmed after intake), with fast UPS 2-Day Air shipping. And TrimRX charges $199/month for injectable semaglutide with true all-inclusive pricing — no extra fees when your dose increases, follow-up consultations included, and a 3-month results guarantee. All three use U.S.-licensed compounding pharmacies and require physician review before prescribing.
MEDVi
From $179/mo
If you hate needles
Oral semaglutide exists (Rybelsus is the brand name, and compounded oral tablets are available through some telehealth providers). Fair warning: oral dosing is less effective for weight loss than injections because absorption is lower. But if the choice is between an oral GLP-1 you’ll actually take versus an injection you’ll avoid, the oral version still beats doing nothing.
If metformin alone isn’t cutting it
Add a GLP-1 to your metformin — don’t replace it. The combination is well-studied and safe (low hypoglycemia risk). Here’s why this matters: in a 2-year observational PCOS study, women who continued metformin after stopping semaglutide regained about one-third of the semaglutide-associated weight loss — meaning roughly two-thirds of the benefit was maintained. This suggests metformin may help attenuate regain after GLP-1 discontinuation. (PMC, 2024) Metformin protects your progress.
Why GLP-1 Medications Work So Well for PCOS (The Science, Simply)
If you have PCOS, you’re probably living inside a metabolic trap — and most people, including some doctors, don’t fully understand it.
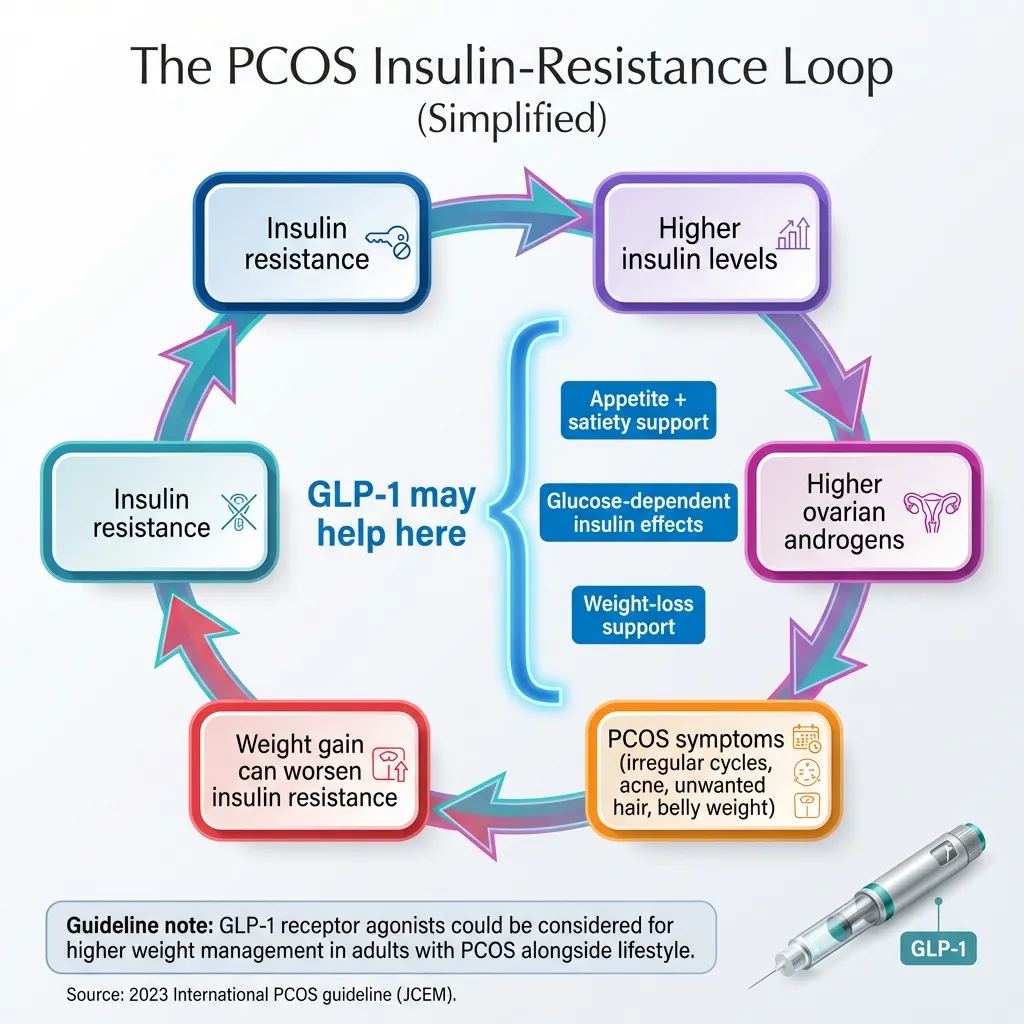
Here’s what’s happening in your body: PCOS causes insulin resistance. Insulin resistance means your cells don’t respond to insulin properly, so your body pumps out more and more insulin to compensate. That excess insulin signals your ovaries to produce more androgens (testosterone). Those elevated androgens cause the symptoms you know too well — weight gain (especially around your middle), irregular periods, acne, hair where you don’t want it, thinning hair where you do.
And here’s the cruel part: the excess weight makes insulin resistance worse, which makes your body produce more insulin, which drives more androgen production, which makes it harder to lose weight. It’s a vicious cycle that has nothing to do with willpower.
This is why “just eat less” doesn’t work for PCOS. Your hunger hormones are dysregulated. A large study found that women with PCOS are significantly more likely to experience binge eating and intense food cravings compared to women without PCOS. You’re not weak. Your biology is fighting you.
GLP-1 medications break this cycle at multiple points:
They improve insulin sensitivity.
GLP-1s trigger insulin release only when blood sugar is elevated (glucose-dependent), which means they help your body use insulin more efficiently without the crash-and-spike pattern that drives PCOS symptoms.
They quiet the “food noise.”
GLP-1s act on appetite centers in the hypothalamus — the part of your brain that controls hunger. Many women with PCOS describe starting a GLP-1 as the first time they’ve felt “normal” around food. The constant cravings, the obsessive thoughts about eating — they quiet down. That’s not cheating. That’s correcting a hormonal dysfunction.
They slow gastric emptying.
Food moves through your stomach more slowly, which means fewer blood sugar spikes after meals and more sustained fullness.
They reduce inflammation.
PCOS is an inflammatory condition. GLP-1 receptor agonists have demonstrated anti-inflammatory effects across multiple organ systems — including the ovaries.
They lower androgen levels indirectly.
As insulin resistance improves and weight decreases, androgen production drops. Some meta-analyses show reductions in total testosterone versus placebo, though results are mixed and may not consistently differ from metformin in all analyses (PubMed, 2024). That translates to potential improvement in acne, hirsutism, and hair loss over 3–6 months — but the degree varies by individual.
Tirzepatide adds a second mechanism — it also activates GIP receptors, which enhances insulin release and improves fat metabolism even further. That’s why it tends to produce greater weight loss than semaglutide alone, and why it may be particularly effective for severe insulin resistance.
Sources: PMC meta-analysis (2023), Nature Communications (2024), FDA prescribing information
Semaglutide for PCOS: What the Research Actually Shows
Semaglutide is the GLP-1 with the most momentum in PCOS research right now — though it’s worth noting that liraglutide actually has a longer PCOS-specific trial history.
The headline numbers:
A 2025 analysis of over 300 million patient records by Epic Research found that women with PCOS on GLP-1 medications (as a class — predominantly semaglutide) lost a median 11.5% of their body weight at one year, compared to just 1.9% for women on metformin. More than half — 55.7% — lost over 10% of their body weight. Only 13.7% of metformin users hit that threshold. (Epic Research, 2025)
A meta-analysis of 8 randomized controlled trials involving 462 women with PCOS found that GLP-1 receptor agonists were superior to metformin for improving insulin sensitivity and reducing BMI and abdominal circumference.
In a small but promising study of 27 women with obesity and PCOS who hadn’t responded to lifestyle changes alone, low-dose semaglutide (0.5mg weekly) for six months showed that approximately 71% of responders achieved normal menstrual cycles — with minimal side effects. This is encouraging but needs confirmation in larger trials. (PMC, 2023)
Who it’s best for:
Semaglutide is the safest bet if you want strong PCOS-specific data backing your decision, you want the most affordable compounded access, and you value the flexibility of an oral option (Rybelsus or compounded tablets) if injections aren’t for you.
Honest downside (and why it’s okay):
Like all GLP-1s, semaglutide works while you take it. In the STEP 1 extension, participants who stopped semaglutide regained roughly two-thirds of their prior weight loss during 1 year off treatment (PubMed, 2022). This is why planning for maintenance — whether through continued low-dose medication or metformin transition — matters from day one. For a deeper dive, see our guide on what happens when you stop taking GLP-1.
But let’s reframe this: PCOS is a chronic metabolic condition. You wouldn’t stop blood pressure medication because your blood pressure normalized and then blame the pill when it went back up. GLP-1 therapy for PCOS is similar — it may be a long-term tool, not a short course. Many women maintain results on lower maintenance doses, and combining with metformin significantly protects weight loss. The goal isn’t to take GLP-1s forever — it’s to use them to break the metabolic cycle, build healthy habits during the window of reduced appetite, and then find your sustainable maintenance plan with your provider.
Sources: Epic Research (Nov 2025), GLP-1 RAs vs Metformin meta-analysis (RBM Online, 8 RCTs), ScienceDirect meta-analysis (Aug 2024)
Tirzepatide for PCOS: The Dual-Action Powerhouse
If semaglutide is the best-studied GLP-1 for PCOS, tirzepatide is the most powerful.
Tirzepatide (brand names Mounjaro for T2D, Zepbound for obesity) works on two hormone pathways instead of one — GLP-1 and GIP. This dual mechanism produces greater weight loss and more aggressive insulin resistance improvement in head-to-head trials. For a full comparison, see our semaglutide vs tirzepatide guide.
The headline numbers:
In the SURMOUNT-1 clinical trial, tirzepatide at its highest dose (15 mg) produced an average ~22.5% body weight reduction at 72 weeks, with 10 mg achieving ~21.4% (NEJM, 2022). In a head-to-head trial (SURMOUNT-5), tirzepatide outperformed semaglutide 2.4 mg directly: −20.2% vs −13.7% (NEJM, 2025).
A PMC review concluded that “tirzepatide has shown better results in reduction of weight and glycated hemoglobin compared to semaglutide.” It also noted that tirzepatide’s dual receptor action may actually reduce the intensity of GI side effects compared to pure GLP-1 agents — a real benefit for women who are worried about nausea.
Who it’s best for:
Tirzepatide is the pick if you’re dealing with severe insulin resistance or pre-diabetes alongside PCOS, you have a higher BMI and need maximum weight loss to improve symptoms, or semaglutide alone hasn’t produced adequate results. Some women who plateau on semaglutide see renewed progress after switching to tirzepatide.
Cost reality:
Tirzepatide is more expensive than semaglutide. Compounded versions start around $258–$349/month depending on the provider and dose. Brand-name Zepbound or Mounjaro without insurance runs $1,000–$1,500/month. MEDVi lists compounded tirzepatide at $349 for the first month (promos may vary). Yucca Health offers it as low as $258/month on a 6-month plan. TrimRX starts at $349/month but includes all follow-up visits and dose adjustments. If budget is tight, starting with semaglutide from any of these providers and switching to tirzepatide later is a smart strategy.
Sources: SURMOUNT-1 (NEJM, 2022), SURMOUNT-5 (NEJM, 2025), PMC review (2023), FDA prescribing information (Zepbound)
Liraglutide for PCOS: The Original GLP-1
Liraglutide (Saxenda for obesity, Victoza for T2D) is the first GLP-1 that was seriously studied in PCOS populations. It has more direct PCOS trial history than many realize.
In a 20-week placebo-controlled trial, 76% of women with PCOS on liraglutide lost more than 5% of their body weight. It also showed reductions in hyperandrogenism and improvements in cardiovascular risk markers.
The catch: Liraglutide requires daily injections (versus weekly for semaglutide and tirzepatide), and its weight loss potency is lower — roughly 4.6% average body weight in PCOS studies versus 11.5% for semaglutide.
When liraglutide makes sense: If you can’t tolerate semaglutide or tirzepatide, if your doctor recommends a shorter or lower-dose treatment course, or if you have insurance that covers Saxenda but not Wegovy or Zepbound. For most women starting fresh, though, semaglutide or tirzepatide will deliver better results.
Sources: PMC liraglutide PCOS review (2023), 2023 PCOS International Guidelines
GLP-1 vs. Metformin for PCOS: Do You Need Both?
This is the comparison nearly every woman with PCOS asks about. Here’s how they actually stack up:
| GLP-1 (Semaglutide) | Metformin | |
|---|---|---|
| Median weight loss at 1 year | 11.5% body weight | 1.9% body weight |
| % losing >10% body weight | 55.7% | 13.7% |
| HbA1c reduction | 0.5 points median | 0.1 points median |
| Insulin sensitivity | Superior | Good (first-line) |
| Cost | $179–$299/mo (compounded) | $4–$30/mo (generic) |
| Long-term safety data | Growing (years) | Extensive (decades) |
| Safe during TTC/pregnancy | No — stop ≥2 months before | Generally yes |
| Best for | Significant weight loss needed; IR not controlled by metformin | Mild-moderate IR; cost-sensitive; actively trying to conceive |
Source: Epic Research (2025), 300M+ patient records. Note: “GLP-1” here refers to the medication class, predominantly semaglutide.
My take: It’s not either-or. The combination often works better than either alone. Metformin is cheap, safe, well-understood, and remains a solid foundation for PCOS management. GLP-1s are the accelerant. If metformin alone isn’t moving the needle on your weight or insulin markers, adding a GLP-1 is the logical next step — not replacing metformin.
And here’s the key data point: in a 2-year observational study, women who continued metformin after stopping their GLP-1 maintained significantly more of their weight loss than might otherwise be expected (PMC, 2024). Think of metformin as the safety net.
What the 2023 PCOS Guidelines Actually Say About GLP-1s
I want to be transparent about where the official guidance stands, because this matters for credibility — yours and mine.
The 2023 International Evidence-Based PCOS Guideline (developed by Monash University and endorsed globally) states that GLP-1 receptor agonists “could be considered” for the management of higher weight in adults with PCOS, alongside lifestyle changes. Semaglutide and liraglutide are specifically named in the guideline. (JCEM, 2023)
The practice points are important:
- The guideline recommends effective contraception when using GLP-1s because pregnancy safety data is lacking.
- It advises gradual dose escalation to minimize GI side effects.
- It acknowledges that long-term use may be necessary since weight regain risk after stopping is high.
- It notes that long-term safety data is still limited.
- For reproductive outcomes specifically (fertility, pregnancy), the guideline recommends GLP-1s only in research settings.
What this means in plain language: GLP-1s are recognized by the global PCOS medical community as a legitimate weight management tool for women with PCOS. They’re not fringe or experimental. But they’re also not a cure-all, and the fertility angle requires careful planning with your doctor.
Source: 2023 International Evidence-Based Guideline for the Assessment and Management of PCOS (Monash University)
Are GLP-1s FDA-Approved for PCOS?
No. Not a single GLP-1 medication has FDA approval specifically for PCOS. Ozempic and Mounjaro are approved for type 2 diabetes. Wegovy and Zepbound are approved for chronic weight management in adults with obesity (BMI ≥30) or overweight (BMI ≥27) with at least one weight-related condition.
When doctors prescribe GLP-1s for PCOS, they’re prescribing “off-label.” This is standard medical practice — roughly 20% of all prescriptions in the U.S. are off-label. Your doctor isn’t doing anything unusual or risky by prescribing a GLP-1 for PCOS.
That said, insurance coverage for PCOS-specific use is tricky. Most insurers will cover GLP-1s only if you meet the FDA-approved criteria (obesity or T2D). If your BMI qualifies or you have a co-diagnosis like pre-diabetes, you may get coverage. If not, cash-pay telehealth is the most realistic route.
In Truveta’s EHR dataset, the share of women with PCOS prescribed semaglutide or tirzepatide rose from 2.4% (2021) to 17.6% (2024) — a 637% relative increase. Across 2021–2024, approximately 20.3% had at least one GLP-1 prescription. (Truveta, 2024) The medical community is rapidly adopting these medications for PCOS — the formal approval just hasn’t caught up yet.
Sources: FDA prescribing information, Truveta/Reuters (Dec 2025)
How to Get a GLP-1 Prescription for PCOS (3 Paths)
Path 1: Through your doctor (brand-name, insurance)
Ask your OB-GYN, endocrinologist, or primary care doctor about off-label GLP-1 therapy for PCOS. If your BMI is 30+ (or 27+ with a weight-related condition), you likely qualify for an FDA-approved weight management indication. Insurance may cover it with prior authorization. Bring the data — mention the PCOS guideline, the Epic Research study, the ASRM recommendation. A letter of medical necessity from your doctor can help if the first claim is denied.
Pros: FDA-approved medications, insurance may cover it, in-person relationship with your provider. Cons: Lengthy approval process, high cost if insurance denies ($1,000+/month), limited to what your formulary covers.
Path 2: Telehealth with compounded GLP-1 (most accessible)
This is how most women without insurance coverage are accessing GLP-1 therapy. Telehealth providers connect you with licensed clinicians who evaluate your history and prescribe compounded semaglutide or tirzepatide, shipped directly to your door. For more options, see our best GLP-1 online programs guide.
What “compounded” means: Compounded GLP-1 products are not FDA-approved as finished medications. They are prepared by U.S.-licensed compounding pharmacies using the same active ingredient as brand-name drugs. However, the FDA has warned that some products marketed as “semaglutide” may use salt forms (e.g., semaglutide sodium or acetate) that are not the same as the approved active ingredient. If you pursue compounded medication, ask the provider/pharmacy exactly what form is used and what quality/testing standards apply. For more on safety, see our guide on is compounded semaglutide safe.
Provider Comparison: MEDVi vs. Yucca Health vs. TrimRX
| MEDVi | Yucca Health | TrimRX | |
|---|---|---|---|
| Semaglutide (injectable) | $179/mo first month; $299/mo refills | As low as $146/mo (6-month plan; pricing confirmed after intake) | $199/mo (all-inclusive) |
| Tirzepatide | From $349/mo first month (promos may vary) | As low as $258/mo (6-month plan) | $349/mo (all-inclusive) |
| Oral semaglutide option? | Yes | No | Yes ($179/mo) |
| Contracts required? | No — month-to-month | 6-month plan gets best pricing | No — month-to-month |
| Price increases at higher doses? | Possible on refill | Included in plan pricing | No — flat rate at any dose |
| Follow-up visits included? | Messaging access 24/7 | Scheduled follow-up calls | Unlimited consults included |
| Shipping | Free, standard | UPS 2-Day Air | Free, within 3 days of approval |
| States available | 49 (not North Dakota) | All 50 states | Most U.S. states |
| PCOS-specific intake? | Yes (PCOS checkbox on form) | General weight loss intake | General weight loss intake |
| Trustpilot rating | 4.4★ (9,800+ reviews) | 4.0★ (725+ reviews) | 4.3★ (650+ reviews) |
| Money-back guarantee? | Yes — weight loss guarantee (terms apply) | 90-day guarantee (terms apply) | 3-month results guarantee |
| Pharmacy partner | Belmar Pharma Solutions (named) | U.S.-licensed (not publicly named) | FDA-registered, LegitScript certified |
| Best for | Overall best: PCOS-aware, flexible, most reviewed | Lowest monthly cost if you commit 6 months | All-inclusive pricing with no surprise fees |
Pricing verified February 2026. All providers offer compounded medications only (not FDA-approved as finished products) unless brand-name is specifically selected at premium pricing.
Our top pick: MEDVi
MEDVi is our primary recommendation for women with PCOS seeking compounded GLP-1 therapy. Their intake form specifically includes a PCOS checkbox, meaning their providers are already set up to evaluate and prescribe for women with PCOS — not just general weight loss. They partner with Belmar Pharma Solutions, a named and established U.S. compounding pharmacy. Month-to-month billing with no contracts means you’re not locked in. And with 9,800+ Trustpilot reviews at a 4.4-star rating and LegitScript certification, they’re the most heavily reviewed and independently verified option. HSA/FSA eligible. 24/7 messaging access to your care team. Read our full MEDVi pills review.
The honest tradeoff: MEDVi’s refill pricing ($299/month for semaglutide) is higher than the first month ($179) and higher than Yucca’s long-term rate. There’s no structured nutrition coaching — support is via messaging, not scheduled calls. And some reviewers on Trustpilot report occasional billing hiccups or shipping delays. None of these are dealbreakers, but you should know.
MEDVi
From $179/mo
Strong alternative: Yucca Health
Yucca Health is the best option if you’re confident about committing to treatment and want the lowest possible monthly cost. Their 6-month semaglutide plan advertises pricing as low as $146/month — the lowest verified advertised rate from a reputable provider. Available in all 50 states. Fast UPS 2-Day Air shipping. Flexible payment options through Affirm, Klarna, and Afterpay. See our full MEDVi vs Yucca Health comparison.
The honest tradeoff: The best pricing requires a 6-month commitment upfront. Yucca’s Trustpilot reviews (4.0 stars, 725+ reviews) are solid but thinner than MEDVi’s. Some reviewers report billing confusion around auto-renewals, and their Terms of Service include binding arbitration and a class-action waiver. They also don’t have a PCOS-specific intake pathway.
Strong alternative: TrimRX
TrimRX is the best option if you want true all-inclusive pricing with no surprise costs. Their $199/month semaglutide price includes everything: medication, all injection supplies, shipping, unlimited provider follow-ups, and free dose adjustments. They also offer a 3-month results guarantee. Read our full TrimRX review.
The honest tradeoff: TrimRX’s monthly rate ($199) is higher than both MEDVi’s first month ($179) and Yucca’s 6-month rate ($146). Their tirzepatide pricing ($349/month) is notably higher than alternatives. Trustpilot reviews (4.3 stars, 650+ reviews) include some complaints about billing confusion on annual plans and slow customer service response.
Path 3: Insurance navigation through telehealth
Some telehealth platforms (like Ro or Hims) offer insurance navigation services to help you get brand-name Wegovy or Zepbound covered. This can work if your plan covers weight management medications, but expect higher costs if paying out-of-pocket for brand-name — sometimes over $1,000/month.
The Safety Checklist for Buying GLP-1 Medication Online
The FDA has issued specific warnings about unapproved GLP-1 drugs sold online for weight loss. Before you buy from any telehealth provider, run through this checklist. For a more detailed guide, see how to take GLP-1 safely.
- Is the prescribing done by a licensed clinician? (Not just an automated quiz)
- Can they name their compounding pharmacy? (If they won’t tell you, walk away)
- Is the pharmacy U.S.-licensed and USP-compliant?
- Do they require a medical intake with contraindication screening? (History of pancreatitis, thyroid cancer, pregnancy status)
- Is the dosing clearly stated in mg/mL and mg/week?
- Does the medication arrive properly refrigerated?
- Is pricing transparent — including what refills cost, not just month 1?
- Can you cancel without jumping through hoops?
- Do they offer adverse event support? (What happens if you have a bad reaction at 2 AM?)
- Do they have verifiable third-party reviews? (Trustpilot, ConsumerAffairs — not just their own website)
MEDVi checks all of these boxes. Their prescribing is done through OpenLoop Health’s network of licensed clinicians. They partner with Belmar Pharma Solutions (a named, established U.S. compounding pharmacy). Month-to-month billing with no contracts. Yucca Health and TrimRX also meet these criteria — both use licensed U.S. pharmacies and require physician review — though Yucca’s 6-month commitment and TrimRX’s annual plan options are worth understanding before you sign up.
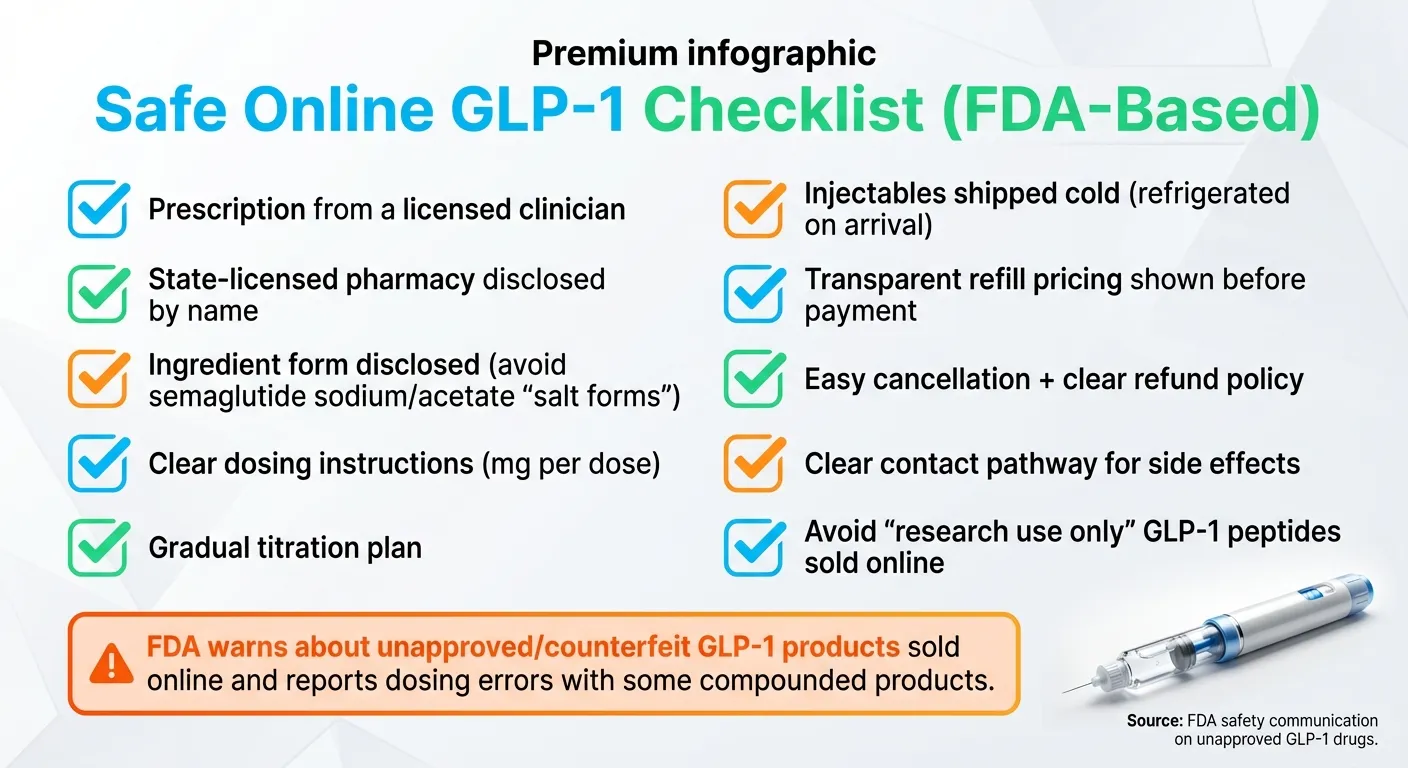
Source: FDA safety communication on unapproved GLP-1 drugs (fda.gov)
Real Experiences: What Women with PCOS Say About GLP-1s
“It wasn’t a shortcut — I was sick”
One woman’s account, published through Harvard Medical School, describes losing nearly 70 pounds (38.8% of her body weight) over 24 months on GLP-1 medication after being diagnosed with PCOS and celiac disease. She had been running marathons, eating well, and still gaining weight. Her endocrinologist helped her understand that with insulin resistance from PCOS, medication was a medical tool — not a crutch.
The weight loss was significant, but she describes the improvements beyond the scale as even more profound: chronic joint pain diminished, brain fog cleared, and fatigue that had made daily tasks a struggle lifted. She wrote that she felt “more present in my life, more engaged with my family.”
Source: Harvard Medical School Primary Care Perspectives
“I finally got a positive test”
Multiple women with PCOS have shared fertility success stories after metabolic improvement on GLP-1s. One woman posted: “I’ve struggled with infertility issues because of PCOS/insulin resistance/obesity and while I’m still overweight, I finally got a positive test.” Her doctor explained that even 5-to-10 pounds of weight loss can restore ovulation and enable pregnancy.
Source: Motherly.com, reporting on Reddit PCOS communities
“My confidence is restored”
One MEDVi user shared on ConsumerAffairs: “My confidence is restored and I will continue with Medvi and compounded semaglutide as long as is necessary to reach my goal weight. I’m excited to see my next round of lab results and if my A1C, cholesterol and glucose numbers are improving. If you are on the fence — I recommend Medvi.”
Another Trustpilot reviewer noted: “The doctors are accessible! So important. This doesn’t feel dangerous. Online medication management can feel scary, but they are careful — order labs and schedule face-time appointments.”
Sources: ConsumerAffairs verified reviews, Trustpilot (medvi.org)
Reviews are individual experiences. Results vary.
Honest Tradeoffs: What You Need to Know Before Starting
I’m not going to pretend GLP-1s are perfect. You deserve the full picture. But I’m also going to give you context — because raw negatives without context create unnecessary fear.
Weight comes back if you stop (for most people)
This is the most commonly cited downside. In the STEP 1 extension, roughly two-thirds of lost weight returned within 1 year of stopping semaglutide. That sounds discouraging until you think about it differently: PCOS is a chronic condition with no cure. Managing it with medication isn’t a failure — it’s treatment. Many women find a lower maintenance dose sufficient long-term. Others use GLP-1s as a catalyst, build strong nutrition and exercise habits during the window of reduced appetite, then transition to metformin alone for maintenance.
GI side effects are real (but temporary)
About 44% of users experience nausea, especially in the first few weeks. Roughly 24% experience some vomiting. These effects are dose-dependent and almost always fade within 4–8 weeks as your body adjusts. The key is gradual dose titration — starting low and increasing slowly. Tirzepatide may cause milder GI effects than semaglutide due to its dual mechanism.
It’s not FDA-approved for PCOS
True — but off-label prescribing is how medicine advances. Metformin for PCOS is also technically off-label (it’s approved for T2D). Over 17% of PCOS patients are now prescribed these medications. The global PCOS guideline endorses their use for weight management alongside lifestyle changes.
Compounded medications aren’t FDA-approved as finished products
This is the honest tradeoff that makes affordable access possible. The FDA regulates compounding pharmacies but doesn’t approve the finished compounds individually. The FDA has also warned that some products marketed as “semaglutide” may contain salt forms that differ from the approved active ingredient. The mitigation: choose a provider that uses a named, reputable pharmacy and ask specifically about the form of semaglutide used. MEDVi partners with Belmar Pharma Solutions. TrimRX uses FDA-registered, LegitScript-certified pharmacies. Yucca Health works with U.S.-licensed partner pharmacies.
12–15% of people don’t respond strongly
Not everyone loses dramatic weight on GLP-1s. Clinical trials found that 12–15% of semaglutide users lost less than 5% of body weight. But even modest weight loss improves PCOS symptoms — international guidelines recommend aiming for 5–15% weight loss to see meaningful improvement in menstrual regularity, insulin sensitivity, and androgen levels.
Who should NOT use GLP-1 medications
These are hard stops, not soft cautions. For a comprehensive list, see our GLP-1 contraindications guide.
- Currently pregnant or breastfeeding
- Personal or family history of medullary thyroid carcinoma (MTC) or Multiple Endocrine Neoplasia syndrome type 2 (MEN 2)
- History of pancreatitis
- Active severe gastrointestinal disease
- Active eating disorder (discuss with your mental health provider first)
Sources: FDA prescribing information, 2023 PCOS Guidelines, clinical trial data
PCOS, Fertility, and GLP-1s: What Nobody Tells You
This is one of the most searched — and most misunderstood — intersections. So let me be direct.
GLP-1 medications are not fertility drugs. The 2023 PCOS guidelines recommend GLP-1s for reproductive outcomes only in research settings. No GLP-1 is approved, recommended, or prescribed as a fertility treatment.
But GLP-1s can improve fertility indirectly — sometimes dramatically. When you lose weight and correct insulin resistance, your ovaries start functioning more normally. Androgens drop. Ovulation can resume. This is why there’s a real phenomenon of “Ozempic babies” — women with PCOS who had struggled with infertility for years getting surprise positive pregnancy tests after a few months on GLP-1 therapy.
The critical safety rule: You must stop semaglutide at least 2 months before a planned pregnancy. For tirzepatide (Zepbound), the prescribing label advises discontinuation when pregnancy is recognized and includes guidance about oral contraceptive absorption during dose escalation — meaning your birth control pill might be less effective when you increase your tirzepatide dose. This is not a minor detail. Discuss it with your provider.
The strategic approach most endocrinologists recommend:
- Phase 1 (3–12 months): Use GLP-1 therapy to lose weight, improve insulin sensitivity, and restore metabolic health. Use effective contraception during this phase.
- Phase 2 (transition): Stop GLP-1, continue metformin (which is considered safe during TTC and pregnancy), maintain lifestyle habits.
- Phase 3 (TTC): Your metabolic foundation is now significantly better than before. Ovulation is more likely. If additional fertility support is needed, your reproductive endocrinologist has a much better starting point to work with.
GLP-1s aren’t a fertility shortcut. They’re a metabolic reset that can create the conditions for fertility to happen naturally.
Sources: 2023 PCOS Guidelines (Monash University), FDA prescribing labels, Motherly.com, CNBC (July 2025)
Side Effects and Safety: What Matters Most for Women with PCOS
The first 2–4 weeks are the hardest. Nausea affects roughly 44% of GLP-1 users. About 24% experience vomiting. 15% report dizziness. These numbers sound high, but context matters: most side effects are mild to moderate, dose-dependent, and temporary. They’re most intense during the initial weeks and during dose increases, then fade as your body adjusts.
The 2023 PCOS guidelines specifically recommend gradual dose escalation to minimize these effects. A good provider will start you on the lowest dose and increase slowly over weeks — not rush you to the target dose.
PCOS-specific concerns to watch for:
Disordered eating risk.
PCOS already has a higher association with binge eating and food-related anxiety. GLP-1 medications dramatically reduce appetite, which is the point — but for some women, the sudden shift from constant food thoughts to almost no appetite can trigger a different kind of disordered pattern (under-eating, food avoidance). If you have a history of eating disorders, have an honest conversation with your provider and consider involving a therapist who specializes in eating behaviors.
Nutrient deficiency.
When you eat significantly less food, you get fewer vitamins and minerals. PCOS women are already commonly deficient in vitamin D, B12, and iron (especially if on metformin, which depletes B12). A quality multivitamin and intentional protein intake become non-negotiable, not optional.
Muscle loss.
Rapid weight loss without adequate protein and resistance training means you lose muscle along with fat. Muscle loss slows your metabolism, which is the opposite of what you want long-term. This is preventable — see our guide on preventing muscle loss on GLP-1.
Hair shedding.
Some women report increased hair shedding in the first few months of rapid weight loss. This is telogen effluvium — a temporary stress response to metabolic change — not permanent hair loss. It typically resolves within 3–6 months. Adequate protein and a biotin supplement may help.
Gallbladder issues.
Rapid weight loss increases the risk of gallstones. If you experience sharp pain in your upper right abdomen, especially after eating, contact your provider immediately.
What’s reassuring: GLP-1 receptor agonists have a good safety profile overall. They do not increase the risk of hypoglycemia (low blood sugar) when used without insulin. The 2023 PCOS guidelines note they are “generally well tolerated” in PCOS management. Most adverse effects are gastrointestinal and resolve with time and proper dose titration.
Sources: FDA prescribing information, 2023 PCOS Guidelines, PMC safety review (Nov 2025)
What to Eat and How to Train on GLP-1s with PCOS
GLP-1 medications reduce your appetite. That’s the point. But reduced appetite without a plan can lead to under-eating, muscle loss, nutrient deficiencies, and the hair shedding that scares a lot of women. This section is short but critical — it’s the difference between losing weight well and losing weight in a way you’ll regret.
Prioritize protein at every meal.
Aim for 25–30 grams per meal, minimum. Protein preserves muscle mass during weight loss — critical because PCOS + rapid weight loss + inadequate protein is a recipe for losing the wrong kind of weight. Good sources: Greek yogurt, eggs, chicken, fish, legumes, cottage cheese. If you can’t eat enough, a protein shake counts.
Don’t skip resistance training.
Strength training 2–3 times per week helps preserve (and build) muscle while you’re losing fat. This matters for metabolism long-term and for maintaining your results after you eventually reduce your dose. You don’t need to become a powerlifter — bodyweight exercises, dumbbells, or machines all work. Consistency beats intensity.
Manage the GI side effects proactively.
Eat slowly. Smaller, more frequent meals instead of large ones. Stay hydrated — dehydration makes nausea worse and can affect kidney function. Ginger tea helps some women with nausea. Increase fiber gradually (not all at once) to manage constipation. If nausea is severe enough to prevent eating, talk to your provider about slowing dose escalation or adjusting timing.
Watch your nutrient intake.
When you’re eating less food overall, every bite matters more. Focus on nutrient-dense foods over empty calories. Consider a multivitamin with iron and vitamin D — both commonly deficient in PCOS, and metformin further depletes B12. A registered dietitian who understands PCOS can be invaluable here, especially in the first 3 months of GLP-1 therapy when your eating patterns are shifting the most.
The PCOS-specific nutrition trap: Many women with PCOS have spent years restricting, cycling through diets, and developing complicated relationships with food. GLP-1s can feel like a relief — finally, the food noise is quiet. But don’t swing from over-eating to under-eating. Aim for adequate nutrition, not minimum nutrition. Your body still needs fuel to function, build muscle, and maintain your hair, skin, and energy.
What Happens When You Stop GLP-1 Medication? (The Honest Answer + Your Plan)
This is the question that stops a lot of women from starting. So I’ll give it to you straight, and then I’ll tell you why it shouldn’t stop you. For a full deep-dive, see our guide on what happens when you stop taking GLP-1.
The data: In the STEP 1 extension trial, participants who stopped semaglutide regained roughly two-thirds of their prior weight loss during 1 year off treatment (PubMed, 2022). Hunger signals returned. Cravings came back.
The reframe (and this is important): PCOS is a chronic metabolic condition. There is no cure. The question isn’t “can I stop and keep the results forever?” — it’s “what’s my long-term management plan?”
Here are the strategies that work:
Stay on metformin.
Women who continued metformin after stopping GLP-1s maintained significantly more weight loss than those who stopped all medication. Metformin is your safety net. It’s cheap ($4–$30/month), well-studied for decades, and safe for long-term use.
Use the GLP-1 window to build habits.
The 6–12 months when your appetite is suppressed is a gift. Use it to establish new eating patterns, start a strength training routine, build the infrastructure of a healthy lifestyle. These habits protect your results even if you eventually reduce or stop the medication.
Consider a maintenance dose.
Not everyone needs to stop completely. Many providers offer lower maintenance doses for women who’ve reached their goal weight but want to prevent regain. This is emerging as the standard approach for chronic weight management.
Don’t let perfect be the enemy of progress.
Even if you eventually regain some weight after stopping, the metabolic benefits you gained during treatment — improved insulin sensitivity, reduced inflammation, better cardiovascular markers, normalized menstrual cycles — have lasting value. You’re not back to square one. You’re at a new, better baseline.
What “Success” Actually Looks Like with GLP-1s and PCOS
Don’t measure success only by the scale. Here’s what to track:
Weeks 1–4:
Appetite reduction, reduced food noise, fewer cravings. Weight loss may begin (1–2 lbs/week is healthy and sustainable). Some GI adjustment.
Months 1–3:
Measurable weight loss (5–7% is a strong start). Energy levels improving. Blood sugar stabilizing. You may notice your clothes fitting differently before the scale moves dramatically.
Months 3–6:
Menstrual cycles may become more regular. Labs may show improved fasting insulin, HbA1c, and lipids. Skin may start clearing. Excess hair growth may slow (this takes time — the hormonal shift is gradual).
Months 6–12:
Full metabolic rebalancing. At 12 months, median weight loss on GLP-1 medications is 11.5% for women with PCOS (Epic Research, 2025). Some meta-analyses show reductions in testosterone versus placebo, though results are mixed. Cardiovascular risk markers improving.
What success is NOT: Overnight transformation. Losing 30 pounds in a month. “Curing” PCOS. Dropping to a specific number on the scale. Your body has its own metabolic equilibrium, and GLP-1s help you find a healthier one — not an Instagram-perfect one.
PCOS + GLP-1 Edge Cases
Will insurance cover GLP-1 for PCOS?
Usually not for PCOS alone, since it’s off-label. But if you also qualify for an obesity or T2D indication (BMI ≥30, or ≥27 with a comorbidity like pre-diabetes or hypertension), your insurer may cover Wegovy or Zepbound with prior authorization. Ask your doctor to submit a letter of medical necessity. If denied, appeal once — it works more often than you’d think. If that fails, compounded semaglutide through a cash-pay program is the backup: MEDVi from $179/mo, Yucca Health as low as $146/mo (6-month plan), or TrimRX from $199/mo all-inclusive — none require insurance.
Can I take a GLP-1 while trying to conceive?
No. Stop semaglutide at least 2 months before attempting pregnancy. For tirzepatide, the label advises discontinuation when pregnancy is recognized. The smart strategy: use GLP-1s to optimize your metabolic health, then transition to metformin for the TTC period. Discuss exact timing with your reproductive endocrinologist — the washout period matters.
Are GLP-1s available in all 50 states?
MEDVi is available in 49 states (all except North Dakota). Yucca Health and TrimRX both claim availability in all 50 states. Some states require a live video telehealth appointment before prescribing: Kansas, Indiana, Mississippi, New Mexico, Oklahoma, and West Virginia. Alabama and California may be limited to injectable formulations only (no oral tablets due to state law). Check your specific provider’s state page before starting the intake process.
Can I take a GLP-1 with metformin?
Yes. The combination is well-studied, safe, and many PCOS specialists recommend it. Hypoglycemia risk is low since GLP-1s work in a glucose-dependent manner. The meta-analysis of 8 RCTs studying GLP-1 vs. metformin in PCOS included combination data with positive results.
How long until I see results?
Weight loss typically begins within 4–8 weeks. Menstrual regularity may improve within 2–3 months. Full hormonal rebalancing (visible improvements in acne, hirsutism, hair health) can take 6–12 months. Insulin resistance improvement often begins before significant weight loss is visible on the scale.
Compounded vs. brand-name — what’s the real difference?
Brand-name (Wegovy, Zepbound) is manufactured by the drug company (Novo Nordisk, Eli Lilly) and carries FDA approval for specific indications. Compounded versions are prepared by U.S.-licensed compounding pharmacies but are not FDA-approved as finished products. The FDA has warned that some compounded products may use salt forms of semaglutide that differ from the approved ingredient — always confirm with your provider what form their pharmacy compounds. The practical difference for most people: price. Brand-name = $1,000+/month. Compounded = $146–$299/month.
Is tirzepatide or semaglutide better for severe insulin resistance?
Tirzepatide’s dual GLP-1 + GIP mechanism targets insulin resistance more aggressively. If your HOMA-IR is significantly elevated, you have pre-diabetes (HbA1c 5.7–6.4%), or metformin alone hasn’t improved your metabolic markers, tirzepatide may be the better clinical choice. Semaglutide is still effective for insulin resistance — just not quite as powerful on that specific axis.
Will GLP-1s help with PCOS acne, hair loss, and excess hair growth?
Indirectly, yes — and this is one of the most motivating outcomes for many women. These symptoms are driven by excess androgens, which are driven by insulin resistance. By correcting insulin → lowering androgens → symptoms improve. Some meta-analyses show reductions in total testosterone versus placebo with GLP-1 use, though results are mixed across studies (PubMed, 2024). Visible improvement in hormonal symptoms typically takes 3–6 months after metabolic correction begins.
What about “lean PCOS”? Should I use GLP-1s if my BMI is normal?
Evidence is limited. GLP-1s are primarily studied and recommended for women with PCOS and higher weight. If you have lean PCOS (normal BMI), GLP-1 therapy is not usually first-line. Your insulin resistance may respond better to metformin, inositol, or lifestyle modifications. Talk to an endocrinologist who specializes in PCOS — the nuance matters here.
Questions to Ask Your Doctor About GLP-1s for PCOS (Copy This List)
If you’re bringing up GLP-1 therapy with your doctor — especially one who hasn’t proactively suggested it — having specific, informed questions makes the conversation more productive. Print this or screenshot it:
- “Based on my current labs (HOMA-IR, HbA1c, testosterone, lipids), would I benefit from adding a GLP-1 to my PCOS treatment plan?”
- “Would semaglutide or tirzepatide be more appropriate given my level of insulin resistance?”
- “Can you prescribe this off-label for PCOS weight management, or should I see an endocrinologist?”
- “If my insurance denies coverage, would you support a letter of medical necessity or prior authorization appeal?”
- “I’m considering a telehealth program for compounded GLP-1 medication — what should I look for in a provider?”
- “How should I adjust my metformin if I start a GLP-1?”
- “I’m planning to try to conceive in [timeframe] — what’s the right medication and timing strategy?”
- “What labs should I monitor while on GLP-1 therapy, and how often?”
- “What’s your recommended dose titration schedule to minimize side effects?”
- “Is there anything in my medical history that would make GLP-1s unsafe for me?”
Doctors respond well to informed patients. Coming in with specific questions signals that you’ve done your homework and are serious about a treatment plan — not just chasing a trend.
Frequently Asked Questions
Is Ozempic FDA-approved for PCOS?
No. Ozempic (semaglutide) is FDA-approved for type 2 diabetes only. It is prescribed off-label for PCOS by clinicians when medically appropriate. Off-label prescribing is legal, common, and backed by clinical evidence.
Which is better for PCOS — Ozempic or Mounjaro?
Both help. Mounjaro (tirzepatide) produces greater weight loss in clinical studies. Ozempic (semaglutide) has more PCOS-specific research and is more affordable in compounded form. Your choice depends on severity of insulin resistance, budget, and your provider's recommendation.
How much weight can I lose on a GLP-1 with PCOS?
Real-world data shows 11.5% median body weight loss at one year with semaglutide. Tirzepatide may achieve 17–25%. Results vary based on starting weight, insulin resistance severity, diet, exercise, and medication adherence.
Can GLP-1 medications help me get pregnant with PCOS?
They can improve fertility indirectly by restoring ovulation through weight loss and insulin correction. But GLP-1s are not fertility medications, and you must stop them at least 2 months before trying to conceive. Use them strategically — optimize your metabolic health first, then transition off before TTC.
How much does GLP-1 treatment cost for PCOS without insurance?
Brand-name: $1,000–$1,500/month. Compounded semaglutide through telehealth: as low as $146/month (Yucca Health 6-month plan), $179/month first month (MEDVi), or $199/month all-inclusive (TrimRX). Compounded tirzepatide: from $258–$349/month depending on provider. HSA/FSA eligible at most providers.
Are compounded GLP-1 medications safe?
Compounded GLP-1 products are not FDA-approved as finished medications. They are prepared by U.S.-licensed pharmacies in FDA-regulated facilities, but the FDA has warned that some compounded "semaglutide" products may contain salt forms that differ from the approved active ingredient. Choose a provider that names their pharmacy partner, uses USP-compliant processes, and can confirm the specific form of semaglutide or tirzepatide being compounded.
Can I take GLP-1 and metformin together for PCOS?
Yes. This combination is well-studied and recommended by many PCOS specialists. Low risk of hypoglycemia. Metformin may also help preserve your weight loss if you eventually stop the GLP-1.
What are the side effects of GLP-1 medications?
Most common: nausea (44%), diarrhea, constipation. These typically fade within 4–8 weeks. Gradual dose titration — starting low, increasing slowly — significantly reduces severity. Rare but serious: pancreatitis, gallbladder issues. Report severe abdominal pain to your doctor immediately.
What happens if I stop taking GLP-1 medication?
Most people regain some weight. Maintaining lifestyle changes and continuing metformin helps preserve results. Some women use lower maintenance doses long-term. This isn't a failure of the medication — it reflects PCOS as a chronic condition that benefits from ongoing management.
Is MEDVi legitimate?
MEDVi holds a 4.4-star rating on Trustpilot across 9,800+ reviews and is LegitScript certified. They're a Delaware-registered LLC partnering with licensed clinicians through OpenLoop Health and compounding through Belmar Pharma Solutions. They operate in 49 states with no contracts and transparent pricing.
Is Yucca Health legitimate?
Yucca Health holds a 4.0-star rating on Trustpilot across 725+ reviews and claims 20,000+ patients. Based in Beverly Hills, CA, they connect patients with board-certified physicians and ship via UPS 2-Day Air. They offer flexible payment through Affirm, Klarna, and Afterpay.
Is TrimRX legitimate?
TrimRX holds a 4.3-star rating on Trustpilot across 650+ reviews. Based in San Diego, CA, they partner with FDA-registered, LegitScript-certified compounding pharmacies and offer a 3-month results guarantee. Their all-inclusive pricing model is genuinely transparent — no dose-increase fees.
How We Built This Guide
Clinical sources reviewed: 8+ randomized controlled trials, 3 meta-analyses, the 2023 International Evidence-Based PCOS Guideline (Monash University), FDA prescribing information for Ozempic, Wegovy, Mounjaro, Zepbound, and Saxenda, peer-reviewed studies from PMC, Nature Communications, ScienceDirect, and Epic Research.
Real-world data: Analysis by Epic Research (November 2025) covering 300+ million patient records across 1,800 hospitals and 41,000 clinics in all 50 states. Truveta/Reuters data on PCOS prescribing trends (December 2025).
Provider verification: MEDVi, Yucca Health, and TrimRX pricing, state availability, pharmacy partnerships, and review profiles verified directly on their official websites, Trustpilot, ConsumerAffairs, and LegitScript — as of February 2026.
Evidence grading approach: We distinguish between PCOS-specific RCT data, general obesity trial data applied to PCOS, and provider-stated claims. Where evidence is limited or preliminary, we say so explicitly.
Update schedule: This page is reviewed monthly. Pricing, state availability, and clinical developments are re-verified. “Last Verified” dates on all provider claims reflect actual verification, not automatic timestamps.
Affiliate relationship: We have affiliate relationships with MEDVi, Yucca Health, and TrimRX and may earn a commission if you sign up through our links. This does not affect our clinical analysis or the methodology behind our recommendations. Providers are featured based on verified pricing, access, clinical quality, and user reviews.
Your Next Step
You’ve read the evidence. You understand the options. Here’s what to do now:
- Decide your primary goal — weight loss, insulin resistance improvement, fertility optimization, or a combination.
- Choose the medication that fits. For most women with PCOS, semaglutide is the smartest starting point: strong evidence, accessible price, flexible dosing options. If you need maximum metabolic impact, consider tirzepatide.
- Choose your access path. If you have insurance that covers GLP-1s, start with your doctor. If you’re paying out of pocket, a telehealth program with compounded options is the practical route.
- If you’re on metformin, keep taking it. If you’re not, ask your provider about combining.
- Set your expectations. Give it 12 weeks to see meaningful change. Track your weight, waist measurement, energy levels, and cycle regularity — not just the scale.
If you have PCOS, you’ve been fighting your body’s biology with tools that were never designed for this fight. Metformin helps. Lifestyle changes help. But for millions of women, they’re not enough — and that’s not your fault. GLP-1 medications give your body the metabolic support it needs so that your effort actually produces results.
This isn’t cheating. It’s treating a medical condition. And you deserve to know it exists, how it works, and how to access it safely.
MEDVi
From $179/mo
Medical Disclaimer: This content is for informational purposes only and does not constitute medical advice. Always consult a licensed healthcare provider before starting any medication. GLP-1 medications are prescription drugs with potential side effects and contraindications. Individual results vary.
Sources & References
- 2023 International Evidence-Based Guideline for the Assessment and Management of PCOS — Monash University
- FDA Prescribing Information — Ozempic (semaglutide), Wegovy (semaglutide), Mounjaro (tirzepatide), Zepbound (tirzepatide), Saxenda (liraglutide)
- Epic Research — “GLP-1s Lead to Greater Weight Loss and A1C Improvement Than Metformin in Patients with PCOS” (November 2025)
- Truveta/Reuters — “Rising Use of GLP-1 Medications Among Women with PCOS” (December 2025)
- PMC — “Do GLP-1 Analogs Have a Place in the Treatment of PCOS?” (2023)
- PMC — “The Potential Utility of Tirzepatide for the Management of Polycystic Ovary Syndrome” (2023)
- ScienceDirect — Meta-analysis: Efficacy and Safety of GLP-1 Agonists in PCOS Women (August 2024)
- Nature Communications — “Superior Metabolic Improvement of PCOS Traits After GLP1-Based Multi-Agonist Therapy” (October 2024)
- Reproductive BioMedicine Online — “GLP-1 Receptor Agonists vs Metformin in PCOS” (8 RCTs, 462 women)
- CNBC — “Weight Loss Drugs Could Be a Gamechanger for Women with PCOS” (July 2025)
- Harvard Medical School — First-person GLP-1 + PCOS Journey Account
- FDA — “Concerns About Unapproved GLP-1 Drugs Used for Weight Loss”
- American Society for Reproductive Medicine (ASRM) — GLP-1 included for obesity management in PCOS
- MEDVi (medvi.org) — Provider pricing, availability, and pharmacy partnerships verified February 2026
- Yucca Health (tryyucca.com) — Provider pricing, 6-month plan terms, and Trustpilot reviews verified February 2026
- TrimRX (trimrx.com) — All-inclusive pricing, results guarantee, and Trustpilot reviews verified February 2026