Best GLP-1 for Prediabetes: 5 Medications Compared (2026)
Disclosure: Some links on this site are affiliate links. If you purchase through these links, we may earn a commission at no extra cost to you. Thank you for supporting our site.·For informational purposes only—not medical advice.
You just got your lab results. A1C somewhere between 5.7% and 6.4%. Your doctor said “prediabetes” — maybe told you to eat better and exercise — and now you’re here looking for the best GLP-1 for prediabetes because you want to do something real about it before it turns into type 2 diabetes. We get it.
Here’s the good news: clinical trials now show that GLP-1 medications can reverse prediabetes in 81–95% of patients. The bad news? There are five different GLP-1s, dozens of telehealth programs, and most websites either bury the answer in medical jargon or just sell you something without showing the evidence.
We did the work so you don’t have to. We compared 5 GLP-1 medications across 8 clinical trials and two meta-analyses, verified pricing on 5 telehealth programs, and built the decision framework below so you can match the right medication to your exact situation in about 60 seconds.
Our Verdict
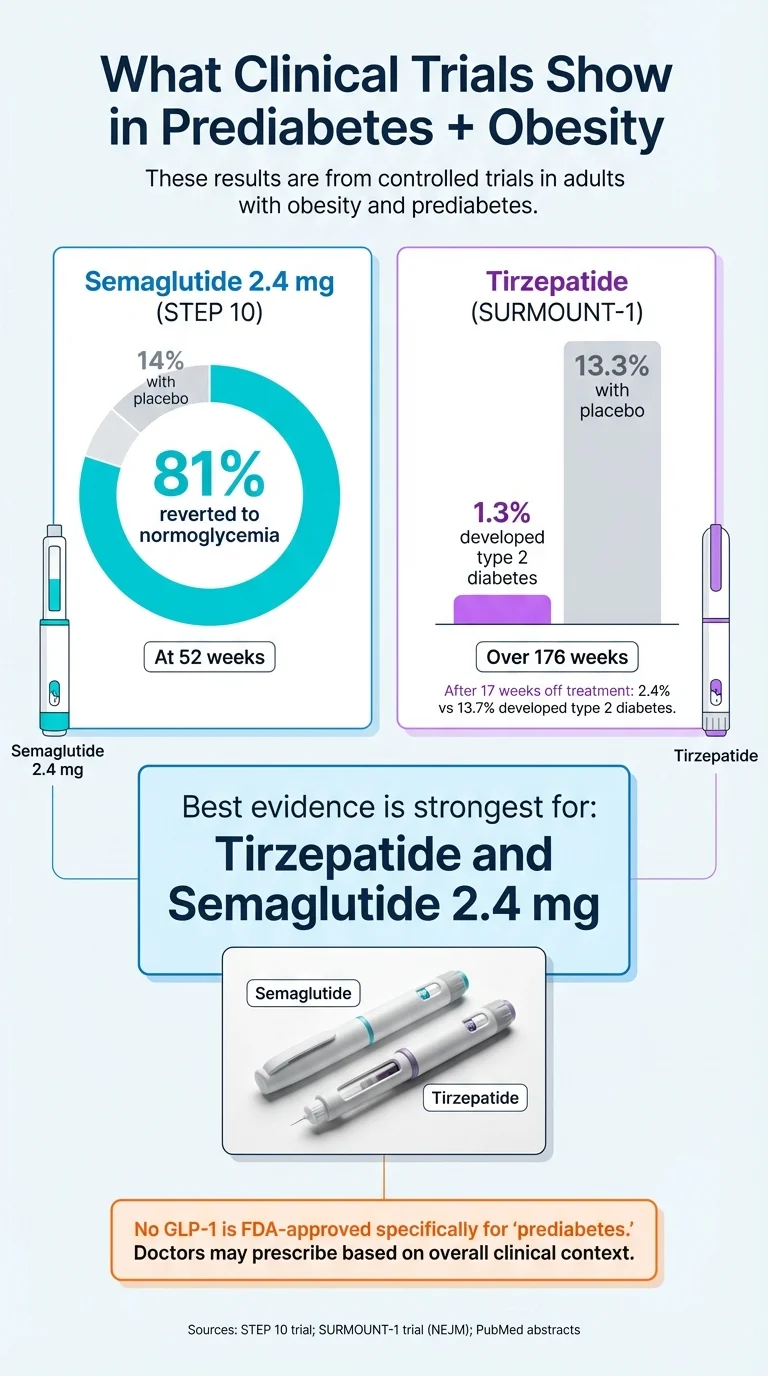
- Strongest evidence for prediabetes: Tirzepatide (Zepbound/Mounjaro) — 95% of prediabetic patients reverted to normal blood sugar at 72 weeks in SURMOUNT-1. Only 1.3% developed type 2 diabetes at 176 weeks vs. 13.3% on placebo.
- Most-studied GLP-1 for prediabetes: Semaglutide 2.4 mg (Wegovy) — 81% achieved normal blood sugar at 52 weeks vs. 14% with lifestyle alone in STEP 10.
- No GLP-1 is FDA-approved specifically for prediabetes. Treatment is off-label — but backed by strong clinical evidence. Wegovy and Zepbound are FDA-approved for chronic weight management in people who meet BMI criteria.
Ready to start? Here’s the simplest path:
MEDVi — Semaglutide program from $179/month. 24/7 physician support. No contract. Weight-loss guarantee (see terms). Over 100,000 patients served.
Check Your EligibilityNot sure which GLP-1 fits your situation? We break it all down below — who each medication is best for, what the clinical trials actually show, what happens when you stop, whether insurance covers it, and the honest truth about compounded vs. brand-name.
If your A1C is 5.7–5.9% and you haven’t tried lifestyle changes yet, medication may not be your first step. See our decision framework.
How Do the 5 Best GLP-1s for Prediabetes Compare?
We ranked five GLP-1 medications based on one thing: how well they work specifically for prediabetes, backed by published clinical trial data. Not marketing. Not hype. Data.
| Medication | Type | How Taken | Prediabetes → Normal Blood Sugar | Diabetes Prevention | Avg Weight Loss | Key Trial | FDA Approved for Prediabetes? | Telehealth Cost | Best For |
|---|---|---|---|---|---|---|---|---|---|
| Tirzepatide (Mounjaro/Zepbound) | Dual GLP-1/GIP | Weekly injection | 95% at 72 wks | 1.3% vs 13.3% T2D at 176 wks | 15–22.5% | SURMOUNT-1 (NEJM, 2024) | No (off-label) | From ~$199/mo | Highest A1C + obesity |
| Semaglutide injection (Ozempic/Wegovy) | GLP-1 | Weekly injection | 81–89% at 52–68 wks | ~86% (STEP data) | 13–15% | STEP 10, STEP 1 (Lancet/NEJM) | No (off-label) | From $179/mo | Most-studied, best balance |
| Oral semaglutide (Rybelsus) | GLP-1 | Daily pill | Comparable A1C reduction | Limited specific data | 5–8% | PIONEER trials | No (off-label) | From ~$199/mo | Needle-phobic |
| Liraglutide (Saxenda/Victoza) | GLP-1 | Daily injection | 79% diabetes risk reduction | 79% over 3 yrs | 5–8% | SCALE (Lancet, 2017) | No (off-label) | Rx only | Longest safety data |
| Dulaglutide (Trulicity) | GLP-1 | Weekly injection | Limited prediabetes data | Limited | 3–5% | REWIND | No (off-label) | Rx only | Heart disease risk |
Important: No GLP-1 medication is FDA-approved specifically for prediabetes. All use in prediabetes is off-label, meaning your doctor prescribes based on clinical evidence and medical judgment. This is legal, common, and well-supported by data — but you should know it upfront.
Which GLP-1 Should You Pick?
Not every GLP-1 is right for every prediabetes situation. Here’s how to match the medication to where you are right now.
If your A1C is 6.0–6.4% and you have obesity (BMI 30+): Tirzepatide. It has the strongest combined evidence for blood sugar normalization AND weight loss. The SURMOUNT-1 data is hard to argue with — 95% normoglycemia, up to 22.5% weight loss. If cost is a concern, compounded tirzepatide is available through providers like TrimRX and Yucca Health.
If your A1C is 5.7–5.9% and lifestyle changes haven’t been enough: Semaglutide injection (Wegovy dose). This is the most studied GLP-1 for prediabetes with multiple large trials confirming results. It’s the “safe bet” — your doctor is most likely to be familiar with it, and it’s widely available through telehealth from $179/month.
If you absolutely won’t do injections: Oral semaglutide (Rybelsus). Same active ingredient as Ozempic, just in a daily pill. You’ll see less weight loss than the injectable, but meaningful blood sugar improvement. Compounded oral options are available through TrimRX and SkinnyRX — and Embody offers a needle-free GLP-1 gum if you want to skip both pills and needles.
If you want the longest safety record: Liraglutide (Saxenda). The 3-year SCALE trial is still the longest prediabetes-specific GLP-1 study ever published. Downside: daily injections and less weight loss than the newer options.
If you have prediabetes plus heart disease risk factors: Dulaglutide (Trulicity). It’s the only GLP-1 with cardiovascular outcome data from the REWIND trial (12% MACE reduction). Less weight loss than semaglutide or tirzepatide, but the heart protection may matter more for your situation.
If budget is everything: Yucca Health ($146/month on a 6-month plan) or MEDVi ($179 first month) for compounded semaglutide.
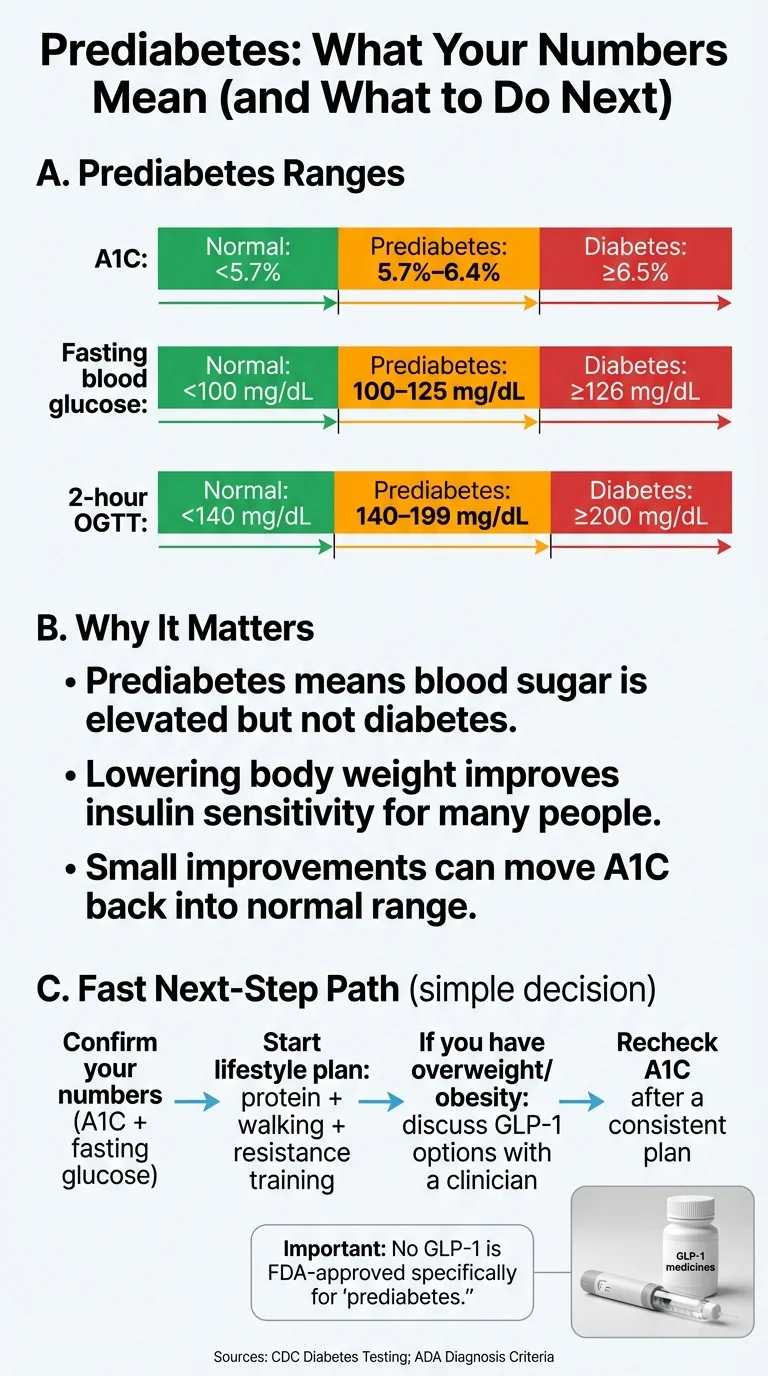
If your A1C is 5.7–5.9% and you haven’t tried diet and exercise yet: Start there first. The Diabetes Prevention Program showed 58% diabetes risk reduction with just 7% weight loss and 150 minutes of walking per week. GLP-1s are powerful, but lifestyle changes are still step one per ADA guidelines — and they’re free. Read our guide on how to start.
Is GLP-1 Actually Right for Prediabetes?
Before we go deeper into each medication, let’s address the question behind the question: should you even be considering GLP-1 medication for prediabetes in the first place?
What Counts as Prediabetes?
Prediabetes means your blood sugar is higher than normal but not high enough for a type 2 diabetes diagnosis. According to the CDC, the ranges are:
- A1C: 5.7% to 6.4% (normal is below 5.7%; diabetes is 6.5%+)
- Fasting blood glucose: 100 to 125 mg/dL
- Oral glucose tolerance test: 140 to 199 mg/dL
About 115.2 million American adults — more than 2 in 5 — have prediabetes right now. About 8 in 10 don’t know it. If you’re reading this, you probably just found out.
The Honest Truth About GLP-1s and Prediabetes
Here’s something most sites either skip or bury: there is no FDA-approved “prediabetes prevention pill.” Not metformin. Not any GLP-1. The FDA hasn’t approved any drug specifically for treating prediabetes or preventing type 2 diabetes.
That sounds discouraging. It’s actually not — and here’s why.
GLP-1 medications like semaglutide (Wegovy) and tirzepatide (Zepbound) are FDA-approved for chronic weight management in people with BMI ≥30, or BMI ≥27 with at least one weight-related comorbidity (FDA labeling lists examples like hypertension, type 2 diabetes, and dyslipidemia). Insurance policies vary on whether prediabetes qualifies as a comorbidity for coverage purposes. So while the label doesn’t say “for prediabetes,” many people with prediabetes meet the weight/BMI criteria for a GLP-1 prescription — and the clinical trials show that the weight loss these medications produce is what drives the blood sugar improvement.
In the STEP 10 trial, semaglutide 2.4 mg moved 81% of prediabetic participants back to normal blood sugar at 52 weeks, compared to just 14% with lifestyle changes alone. That’s not a subtle difference. That’s a category change.
The takeaway: GLP-1s work for prediabetes through weight loss. The FDA just hasn’t caught up to the label yet.
How GLP-1s Actually Work for Prediabetes
GLP-1 stands for glucagon-like peptide-1. It’s a hormone your gut naturally produces after eating. It does three things that matter for prediabetes:
- Signals your pancreas to release insulin — but only when blood sugar is elevated, which is why hypoglycemia risk is low
- Slows gastric emptying — food stays in your stomach longer, so blood sugar doesn’t spike as sharply after meals
- Reduces appetite — by acting on your brain’s satiety centers, which drives the significant weight loss seen in clinical trials
GLP-1 medications are synthetic versions of this hormone engineered to last much longer than the natural version. Injectable semaglutide (Wegovy) and tirzepatide (Zepbound) last a full week from a single dose. The weight loss drives improved insulin sensitivity, which drives better blood sugar control, which drives prediabetes reversion. It’s a cascade — and it’s why the trial numbers are so strong.
Tirzepatide goes a step further. It’s a “dual agonist” — targeting both GLP-1 and GIP (glucose-dependent insulinotropic polypeptide) receptors. This dual mechanism appears to drive even stronger weight loss and blood sugar improvements, which is why tirzepatide’s prediabetes data outperforms everything else published to date.

Who Should (and Shouldn’t) Consider GLP-1 Treatment
Strong Candidates
- Prediabetes (A1C 5.7–6.4%) plus BMI ≥30
- Prediabetes plus BMI 27–29.9 with a weight-related condition (high blood pressure, high cholesterol, sleep apnea, PCOS)
- Already tried lifestyle changes for 3–6+ months without reaching A1C or weight goals
- Family history of type 2 diabetes and trending in the wrong direction
May Not Be Right — Talk to Your Doctor
- Prediabetes with normal BMI — your insulin resistance likely isn’t weight-driven
- A1C 5.7–5.9% with no prior lifestyle intervention
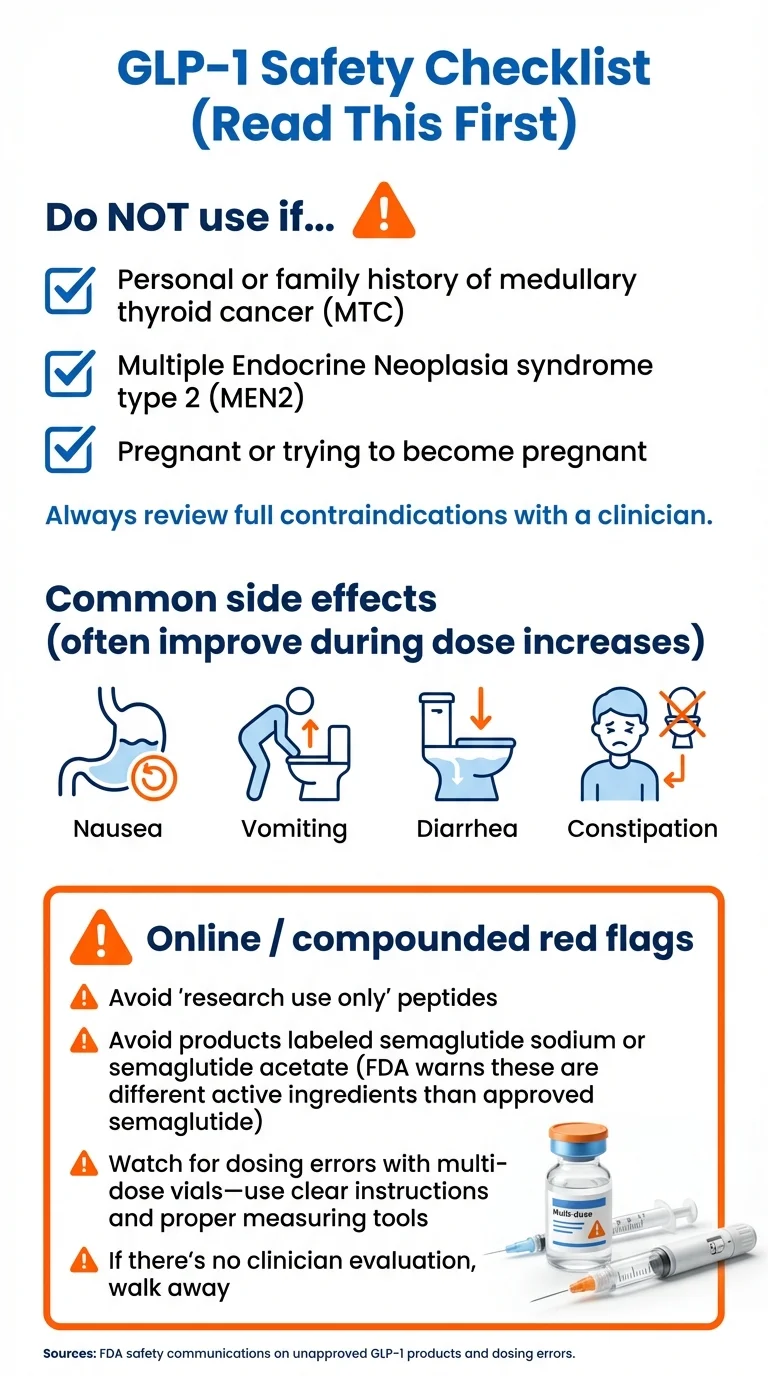
- Personal or family history of medullary thyroid cancer or MEN2 (hard contraindication)
- History of pancreatitis
- Pregnant or planning to become pregnant
Tirzepatide (Mounjaro / Zepbound) — Strongest Prediabetes Evidence
If you’re looking for the single strongest data point for prediabetes reversion, it belongs to tirzepatide.
The Evidence
The SURMOUNT-1 trial, published in the New England Journal of Medicine in 2024, studied tirzepatide in adults with obesity — including a large subgroup with prediabetes. The prediabetes results were striking:
- 95% of prediabetic patients reverted to normal blood sugar at 72 weeks (compared to 62% on placebo)
- By 176 weeks, 1.3% had progressed to type 2 diabetes vs. 13.3% on placebo; after a 17-week off-treatment period, those figures were 2.4% vs. 13.7%
- That translates to a 94% diabetes risk reduction over the study period
- Average weight loss: 15–22.5% of body weight depending on dose
Those numbers are the best in any published GLP-1 trial for prediabetes. Full stop.
How It Works
Tirzepatide is a dual GLP-1/GIP receptor agonist — meaning it targets two gut hormone pathways instead of one. This dual mechanism appears to drive both stronger weight loss and better blood sugar control compared to GLP-1-only medications. It’s a weekly injection.
Who It’s Best For
Tirzepatide is the strongest option if you have prediabetes at the higher end (A1C 6.0–6.4%) combined with obesity (BMI 30+). It’s particularly compelling if you need significant weight loss — 15–22% of body weight is life-changing for most people. If you’ve tried semaglutide and plateaued, tirzepatide targets an additional pathway that may break through.
Who It’s Not For
People with personal or family history of medullary thyroid cancer or MEN2 (hard contraindication on the label). If you only need a modest A1C nudge and you’re closer to the 5.7% end, semaglutide’s extensive data set may be a better fit. Tirzepatide also has less long-term safety data than semaglutide — it’s a newer medication.
The Honest Downside
Tirzepatide is the most expensive brand-name option. Zepbound runs $1,000+ per month without insurance. GI side effects (nausea, diarrhea) tend to be more common at higher doses. And because it’s newer, we have less long-term data than we do for semaglutide or liraglutide.
That said, if the clinical evidence is what matters most to you — and it should be — tirzepatide’s 95% normoglycemia rate and 94% diabetes prevention over 3 years make a compelling case.
How to Access Affordably
Brand-name Zepbound is expensive without insurance, but compounded tirzepatide is available through telehealth providers. TrimRX and Yucca Health offer compounded versions from approximately $199–$327/month. Not cheap — but a fraction of the brand-name cost.
Semaglutide Injection (Ozempic / Wegovy) — Most Studied for Prediabetes
If tirzepatide has the single strongest data point, semaglutide has the deepest body of evidence. More published trials. More patients studied. More long-term follow-up. For most people starting GLP-1 treatment for prediabetes, semaglutide injection is the sweet spot between evidence, accessibility, and price.
The Evidence
Semaglutide 2.4 mg (the Wegovy dose) has been studied across multiple large trials with prediabetic populations:
STEP 10 (2024, Lancet Diabetes & Endocrinology)
The landmark prediabetes-specific trial. 207 adults with obesity and prediabetes received semaglutide 2.4 mg weekly for 52 weeks.
- • 81% achieved normal blood sugar vs. 14% on lifestyle changes alone
- • 13.9% average weight loss vs. 2.7% with placebo
- • At 80 weeks (after stopping for 28 weeks): 44% still maintained normoglycemia vs. 18% in the placebo group
STEP 1 (2021, NEJM)
1,961 participants. In the prediabetic subgroup: 84.1% reverted to normoglycemia at 68 weeks vs. 47.8% on placebo.
STEP 3 (2021, JAMA)
Combined with intensive behavioral therapy: 89.5% normoglycemia vs. 55% placebo.
SELECT (2024, Diabetes Care)
Cardiovascular outcome trial: 20% reduction in major cardiovascular events in people with obesity.
Meta-analysis (2024, Diabetology & Metabolic Syndrome)
12 randomized controlled trials, 4,316 prediabetic patients: GLP-1 RAs significantly increased prediabetes → normoglycemia reversion (relative risk 1.76). Prevented new-onset diabetes (relative risk 0.28).
Let’s Be Honest About One Thing
Here’s the part we think you need to hear, even though it’s not what you want to hear.
When people stop semaglutide, some of the weight comes back. And some of the blood sugar benefit fades. The STEP 10 trial showed normoglycemia dropped from 81% while on treatment to 44% after 28 weeks off. That’s real. This is not a 12-week fix. If you start GLP-1 therapy, the evidence suggests you may need to stay on it long-term to keep the results — or pair it with serious lifestyle changes during treatment so you have a stronger foundation when you come off.
But here’s what often gets lost in that conversation: even after stopping, the semaglutide group still had 2.4 times the normoglycemia rate of the lifestyle-only group. That’s not “it didn’t work.” That’s “it worked, and it still had lasting impact even when discontinued.” And with compounded semaglutide now available from $179/month, staying on treatment long-term is more financially realistic than it’s ever been.
This isn’t a cure. It’s a tool — possibly the most effective tool available for prediabetes right now. And tools work best when you keep using them.
Who It’s Best For
Semaglutide injection is the right choice for most people with prediabetes and overweight/obesity who want the deepest clinical evidence behind their decision. It’s also your best option if cardiovascular protection matters (the SELECT trial showed a 20% MACE reduction). Most doctors are already familiar with it, which makes conversations easier.
Who It’s Not For
History of pancreatitis is a caution. If you’re genuinely needle-phobic and can’t get past it, oral semaglutide exists (next section). If your budget is extremely tight, Yucca Health offers compounded semaglutide from $146/month on a 6-month commitment.
How to Access Affordably
Brand-name Wegovy costs $1,300+/month without insurance. Ozempic (the diabetes dose) runs about $900+/month. Most insurance plans won’t cover either specifically for prediabetes.
That’s where telehealth platforms come in. Several offer compounded semaglutide at a fraction of the brand-name cost. Important context: compounded drugs are not FDA-approved as finished products, and the clinical trial outcomes we cited above come from FDA-approved semaglutide (Wegovy) — not compounded versions. FDA has also warned that some compounded products use semaglutide salt forms (e.g., semaglutide sodium), which FDA considers different active ingredients than the approved drug. If you’re considering a compounded option, ask your prescriber which form is used and whether the pharmacy is a state-licensed 503A or FDA-registered 503B facility.
Telehealth pricing for compounded semaglutide programs:
- • MEDVi: $179 first month, $299/month ongoing. 24/7 provider support. No contract. 100,000+ patients served. Weight-loss guarantee.
- • Embody: $99 first month for the semaglutide injection, then $299/month ongoing. Needle-free GLP-1 gum option; cash-pay with 24/7 support.
- • SkinnyRX: $199/month. Three format options (injectable, sublingual, tablet). No dosage price increases.
“I’m glad I chose Medvi… Pricing is competitive and support is included!” — MEDVi Trustpilot reviewer
MEDVi
From $179/mo
Oral Semaglutide (Rybelsus) — The Pill Option
Not everyone can do injections. If needles are a hard no for you, oral semaglutide is worth knowing about.
What It Is
Rybelsus is the brand-name oral semaglutide pill, FDA-approved for type 2 diabetes. It uses the same active ingredient as Ozempic — semaglutide — but in a daily tablet. A newer oral version for obesity (oral Wegovy) has been approved but availability remains limited as of early 2026.
The Evidence
The PIONEER trial program showed meaningful A1C reductions and weight loss in people with type 2 diabetes. Prediabetes-specific trial data is limited for the oral version, but the mechanism is identical to injectable semaglutide — it just has lower bioavailability, which means you absorb less of the active ingredient.
In practical terms: expect similar blood sugar benefits but roughly half the weight loss compared to injectable semaglutide.
The Tradeoff
Oral semaglutide has strict dosing requirements — take it on an empty stomach with no more than 4 ounces of water, then wait 30 minutes before eating or drinking anything else. Miss those rules and absorption drops significantly. It’s less convenient than a once-weekly injection for many people.
But if the choice is between a daily pill and not treating your prediabetes at all? The pill wins.
How to Access
Brand-name Rybelsus is available through insurance for type 2 diabetes. Compounded oral semaglutide (sublingual or tablet form) is offered by TrimRX and SkinnyRX in the $199–$249/month range. If you’d rather avoid both pills and needles, Embody offers a needle-free GLP-1 gum.
Wegovy vs. Ozempic: What’s the Difference?
This is one of the most common points of confusion. Both are semaglutide. Both are made by Novo Nordisk. Both are weekly injections. But they’re not the same product.
| Ozempic | Wegovy | |
|---|---|---|
| Active ingredient | Semaglutide | Semaglutide |
| FDA-approved for | Type 2 diabetes | Chronic weight management (BMI ≥30 or ≥27 with comorbidity); also CV risk reduction |
| Maximum dose | 2.0 mg/week | 2.4 mg/week |
| Titration schedule | 0.25 → 0.5 → 1.0 → 2.0 mg | 0.25 → 0.5 → 1.0 → 1.7 → 2.4 mg |
| Prediabetes trials | Not the studied dose for prediabetes | STEP trials used the 2.4 mg dose |
| Typical cost | ~$900/month | ~$1,300/month |
For prediabetes specifically: The clinical trial data (STEP 10, STEP 1, etc.) used the 2.4 mg dose — which is the Wegovy dose, not Ozempic. Some doctors prescribe Ozempic off-label at its maximum 2.0 mg dose for weight management, which is close but not identical to the studied protocol.
A note on compounded semaglutide: The STEP trials used FDA-approved semaglutide products. Compounded products are not FDA-approved as finished products, and you should not assume compounded dosing produces identical outcomes to the clinical trials. FDA has warned that some compounded products use semaglutide salt forms, which are considered different active ingredients than the approved drug. That said, many patients use compounded semaglutide through telehealth platforms as a more affordable access point — just go in with eyes open about what you’re getting. Read our compounded semaglutide safety guide.
Liraglutide (Saxenda / Victoza) — Longest Prediabetes Data
Liraglutide doesn’t get the headlines anymore. Semaglutide and tirzepatide have grabbed the spotlight. But liraglutide has something neither of them can claim: a full 3-year prediabetes trial.
The Evidence
The SCALE Obesity and Prediabetes trial (2017, The Lancet) followed patients with obesity and prediabetes for 3 years on liraglutide 3.0 mg daily.
- • 79% reduction in new diabetes diagnoses vs. placebo at 3 years
- • Sustained weight loss of 5–8% of body weight
- • Clear evidence that longer treatment = longer protection
This remains the longest prediabetes prevention study for any GLP-1 medication.
Who It’s Best For
If you prioritize long-term safety data above all else — if knowing that a medication has been studied for 3+ years in people exactly like you matters more than having the highest weight loss number — liraglutide is your pick.
The Honest Downside
It’s a daily injection (not weekly like semaglutide or tirzepatide). The weight loss is more modest — 5–8% vs. 14–22% with newer options. And it’s gradually being phased out by many telehealth platforms in favor of newer medications. Fewer compounded options are available.
Dulaglutide (Trulicity) — Best for Heart Disease Risk
If your prediabetes comes packaged with high blood pressure, high cholesterol, or a family history of heart disease, dulaglutide has relevant cardiovascular data worth considering.
The Evidence
The REWIND trial showed dulaglutide reduced major cardiovascular events (heart attack, stroke, cardiovascular death) by 12% in people with type 2 diabetes. It’s not the only GLP-1 with cardiovascular outcome data — liraglutide (LEADER trial) and semaglutide (SUSTAIN-6, SELECT) also demonstrated cardiovascular benefits. But dulaglutide’s REWIND trial included a broader population (not just high-risk CV patients), which some clinicians find more applicable to real-world patients. Prediabetes-specific data is more limited, but A1C and weight improvements are consistent across its trial program.
Who It’s Best For
People with prediabetes plus significant cardiovascular risk factors. If you’re already on blood pressure and cholesterol medications, a GLP-1 with proven heart protection has compounding value.
The Honest Downside
Less weight loss than semaglutide or tirzepatide (~3–5% body weight). Less prediabetes-specific evidence. Being overshadowed by newer medications in both research and telehealth availability. Insurance typically requires a type 2 diabetes diagnosis for coverage.
How to Start GLP-1 Treatment for Prediabetes (Without Paying $1,300/Month)
Let’s talk about the elephant in the room: cost.
Brand-name GLP-1s run $900–$1,500 per month without insurance. Most insurance plans don’t cover GLP-1s for prediabetes specifically — they require either a type 2 diabetes diagnosis or an obesity indication with specific BMI criteria. Medicare generally can’t cover drugs prescribed solely for weight loss. However, Part D coverage may apply when a drug is prescribed for another medically accepted indication — for example, Wegovy is now FDA-approved to reduce cardiovascular events in certain patients with established heart disease, and Part D plans can cover it for that use. Coverage is plan- and diagnosis-dependent, so check with your specific plan.
This is why telehealth platforms offering compounded semaglutide and tirzepatide have changed the game. They provide physician oversight, prescriptions, and medication delivered to your door — for $146–$299/month.
Here’s how the top 5 providers compare:
| Provider | Starting Price | Ongoing Price | Medications | Formats | Provider Support | Contract | Guarantee | Best For |
|---|---|---|---|---|---|---|---|---|
| MEDVi | $179/mo | $299/mo | Semaglutide + Tirzepatide | Injectable + Oral | 24/7 support | No contract | Weight-loss guarantee | Best overall — balance of price, support, flexibility |
| TrimRX | $199/mo | Same | Semaglutide + Tirzepatide | Injectable + Oral | Unlimited check-ins | Month-to-month | Results guarantee (terms apply) | Comprehensive program + supplements |
| Embody | $99 first mo | $299/mo | Semaglutide + Tirzepatide | Injectable + needle-free gum | 24/7 support | Cash-pay; no insurance | — | Low first-month price; needle-free gum option |
| Yucca Health | $146/mo | Same (6-mo plan) | Semaglutide + Tirzepatide | Injectable | Provider oversight | 6-month commitment | All sales final (compounded meds) | Lowest cost if you can commit |
| SkinnyRX | $199/mo | Same | Semaglutide + Tirzepatide | Injectable + Sublingual + Tablet | Provider access | Month-to-month | — | Most medication format options |
Pricing last verified: February 2026. Visit each provider’s website to confirm current pricing.
Why We Recommend MEDVi for Most People
We’ve looked at a lot of telehealth GLP-1 platforms. For most people just starting out, MEDVi hits the best balance of what matters: transparent pricing ($179 first month, $299 ongoing — no hidden fees), 24/7 provider support, both semaglutide and tirzepatide available, no long-term contract, and a weight-loss guarantee.
They’ve served over 100,000 patients, and the process is straightforward. They accept HSA/FSA cards, and you can cancel anytime.
The first month is lower because they want you to try it without a massive upfront commitment. Month two does go up to $299 — that’s the honest part. But compared to $1,300 for brand-name Wegovy, it’s a meaningful difference. And unlike some platforms, what you see is what you pay. No surprise charges on your credit card.
MEDVi
From $179/mo
How Getting Started Actually Works (Step by Step)
The process is simpler than most people expect. Here’s what it looks like with most telehealth GLP-1 platforms:
Online health questionnaire (5–10 minutes)
You’ll answer questions about your medical history, current medications, A1C or recent lab work, height, weight, and health goals. This is how the platform determines if you’re a candidate.
Physician review (24–72 hours)
A licensed provider reviews your information. Some platforms do a video consultation; others use asynchronous review. Either way, a real doctor is making the prescribing decision. If you’re not a good candidate, they’ll tell you — you won’t be charged.
Prescription and pharmacy fulfillment (3–7 days)
If approved, your prescription goes to a licensed pharmacy. Your medication is compounded and shipped directly to your home in an insulated package. Most platforms include syringes, alcohol pads, and injection instructions.
Start low, titrate up
You’ll begin at the lowest dose and gradually increase over several weeks. This slow ramp-up is critical for minimizing side effects. Your provider should be guiding you through this — don’t try to skip ahead on dosing.
Ongoing support and refills
Monthly refills ship automatically. Good platforms offer check-ins with your provider to monitor progress, adjust dosing, and address side effects. MEDVi’s 24/7 support means you can reach a clinician at 11 PM on a Tuesday if something feels off.
If Budget Is Your Top Priority
Yucca Health offers the lowest per-month cost at $146/month — but you’re committing to 6 months. If you’re confident about starting and can commit to that timeline, it’s hard to beat on price. Note: Yucca’s refund policy states compounded medications cannot be returned or refunded, so make sure you’re committed before signing up.
A Note on Compounded Medications
All providers listed above offer compounded GLP-1 medications. This means:
- • Not FDA-approved as finished products
- • Quality and formulation can vary between compounding pharmacies
- • FDA has warned that some compounded products use semaglutide salt forms (e.g., semaglutide sodium), which FDA considers different active ingredients than the approved drug
- • The clinical trial outcomes cited on this page come from FDA-approved products — not compounded versions
- • Prepared by pharmacies (503A or 503B facilities) that operate under FDA and state oversight
The FDA resolved the semaglutide shortage on February 21, 2025, which affects the legal basis for compounding. The regulatory landscape continues to evolve. Reputable platforms like MEDVi, Embody, and TrimRX require physician evaluation before prescribing. We recommend discussing compounded vs. brand-name options with your prescribing provider.
What Does the Research Actually Say? (The Clinical Evidence)
If you’re the type who wants to see the data before making a decision — good. You should be. Here’s what the published clinical trials show, translated from medical-journal language into plain English.
The Baseline: Lifestyle Changes Alone
Before GLP-1s entered the picture, the gold standard was the Diabetes Prevention Program (DPP), published in the NEJM in 2002. It found:
- • Lifestyle intervention (7% weight loss + 150 minutes of exercise/week) reduced diabetes risk by 58%
- • Metformin reduced risk by 31%
These are the benchmarks. Lifestyle changes work. But here’s the reality: most people struggle to sustain 7% weight loss through diet and exercise alone long-term. That’s not a character flaw — it’s biology. And that’s where GLP-1s come in.
STEP 10: The Prediabetes-Specific Semaglutide Trial
Published in The Lancet Diabetes & Endocrinology (2024). 207 adults with obesity and prediabetes. Semaglutide 2.4 mg weekly for 52 weeks.
- • 81% prediabetes remission vs. 14% with lifestyle alone
- • 13.9% weight loss vs. 2.7%
- • After stopping (80 weeks): 44% still maintained normoglycemia vs. 18%
STEP 1: The Landmark Weight Loss Trial
Published in the NEJM (2021). 1,961 participants. The prediabetic subgroup analysis showed: 84.1% achieved normoglycemia at 68 weeks vs. 47.8% on placebo.
SURMOUNT-1: Tirzepatide’s Breakthrough
Published in the NEJM (2024). This is where tirzepatide’s numbers come from:
- • 95% normoglycemia at 72 weeks in the prediabetic subgroup
- • By 176 weeks, 1.3% on tirzepatide vs. 13.3% on placebo developed type 2 diabetes; after 17 weeks off treatment, 2.4% vs. 13.7%
- • 94% diabetes risk reduction over the study period
- • Weight loss of 15–22.5% depending on dose
SCALE: Liraglutide’s 3-Year Run
Published in The Lancet (2017). 3-year study of liraglutide 3.0 mg in adults with obesity and prediabetes: 79% reduction in new diabetes diagnoses over 3 years. The longest GLP-1 prediabetes prevention study published to date.
What the Meta-Analyses Show
A 2024 meta-analysis in Diabetology & Metabolic Syndrome pooled 12 randomized controlled trials with 4,316 prediabetic patients: GLP-1 RAs significantly increased prediabetes → normoglycemia reversion (RR 1.76, p < 0.00001) and prevented new-onset diabetes (RR 0.28, p < 0.00001).
A 2026 updated meta-analysis in Diabetes Metabolism Research and Reviews analyzed 8 RCTs with 14,564 participants: GLP-1 RAs restored normoglycemia with odds ratio 4.62 vs. placebo (p < 0.00001). Both semaglutide and liraglutide were effective. Exenatide was not.
The Bottom Line on the Evidence
The clinical data is now strong: GLP-1 medications — particularly semaglutide and tirzepatide — can reverse prediabetes in the majority of patients when combined with lifestyle changes. These results significantly outperform lifestyle modifications alone. But this isn’t a blank check. GLP-1s aren’t FDA-approved for prediabetes. Benefits decrease when you stop taking them. And long-term studies beyond 3 years are still limited. The evidence says they work. It doesn’t say they work forever without effort on your part.
What Results Can You Realistically Expect?
Let’s set honest expectations — because “95% normoglycemia” in a clinical trial and “what happens to me in real life” are two different conversations.
The First Month (Weeks 1–4)
You’ll likely start at the lowest dose. Weight loss at this stage is modest — maybe 2–4 pounds. The appetite suppression is the first thing most people notice. Food just... becomes less interesting. You’re eating less without white-knuckling it. Some nausea is normal during this period. It usually peaks in the first two weeks and fades. Your A1C won’t change meaningfully in month one. Don’t recheck yet.
Months 2–3 (Weeks 5–12)
As your dose increases, weight loss accelerates. Most patients lose 5–10% of their body weight in this window. The blood sugar improvements follow the weight loss — you may start to see fasting glucose numbers dropping into the normal range. Energy levels often improve as insulin sensitivity gets better. The GI side effects usually settle by now for most people.
Months 4–6 (Weeks 13–26)
This is where the clinical trial results start becoming your reality. Weight loss continues. A1C changes become measurable — typically 0.3–0.5 percentage point reductions from baseline. Many patients cross from prediabetic back to normal range during this period.
Months 6–12 (Weeks 26–52)
In the STEP 10 trial, peak results came at 52 weeks: 81% normoglycemia, 13.9% weight loss. The trajectory slows as you approach your new set point, but the gains accumulate. By this stage, you should be building the lifestyle habits — exercise, nutrition, sleep, stress management — that will support long-term results regardless of whether you continue medication.
After 12+ Months
Long-term data from SURMOUNT-1 (tirzepatide, 176 weeks) shows sustained diabetes prevention at 94% risk reduction. The evidence supports continued use for continued benefit. The question isn’t whether it works long-term — it’s whether you want to (and can afford to) stay on it.
Brand-Name vs. Compounded GLP-1: What You Need to Know
This topic makes some sites uncomfortable. We’re going to be direct about it.
What’s the Difference?
Brand-name (Ozempic, Wegovy, Mounjaro, Zepbound): Made by the original manufacturer (Novo Nordisk or Eli Lilly), FDA-approved as finished products, and the clinical trial evidence cited throughout this page applies directly to these products. Costs $900–$1,500/month.
Compounded: Not FDA-approved as finished products. Quality and formulation can vary by pharmacy. FDA has warned about unapproved GLP-1 products marketed online and has stated that some compounded products use semaglutide salt forms (e.g., semaglutide sodium or acetate), which FDA considers different active ingredients than the approved drug. Costs $146–$299/month through telehealth platforms.
Why Compounded Exists
When brand-name GLP-1s were in shortage (which was the case for much of 2023–2024), federal law allowed compounding pharmacies to prepare alternatives. The FDA declared the semaglutide shortage resolved in February 2025. The legal landscape for compounded semaglutide is evolving, and some platforms may be affected.
What the FDA and ADA Say
The FDA has explicitly warned consumers about unapproved GLP-1 products sold online — particularly those marketed with misleading claims or sold without proper physician oversight. The American Diabetes Association recommends against non-FDA-approved compounded GLP-1 medications due to uncertainty around safety, quality, and effectiveness of compounded formulations.
How to Protect Yourself
If you’re considering compounded GLP-1 medication, here’s what to verify:
- Physician involvement is required. If a platform lets you buy medication without a medical evaluation, walk away.
- Ask about the pharmacy. Reputable platforms will disclose whether they use 503A or 503B compounding pharmacies.
- Look for FDA-regulated facilities. “Compounded” doesn’t mean unregulated — it should mean prepared under FDA oversight.
- Avoid “research use only” peptides. These are not medications. They are not prescribed. They are not safe for human use.
- No platform should claim GLP-1s are “FDA approved for prediabetes.” That’s false — and it’s a red flag about their credibility.
The providers we feature — MEDVi, TrimRX, Embody, Yucca Health, SkinnyRX — all require physician evaluation and use licensed pharmacies. That doesn’t make them identical to brand-name products. It does mean they’re operating within a medical framework, not selling unregulated peptides out of a garage.
What Are the Risks and Side Effects?
No honest page about GLP-1s would skip this section. Side effects are real, and you should know what to expect. Learn more in our guide to GLP-1 side effects and downsides.
Common Side Effects (and What to Do)
The most common side effects across all GLP-1 medications, especially during the first 4–8 weeks as your body adjusts:
- • Nausea (20–44% of patients in trials) — the most frequent complaint. Usually mild. Subsides as your body adjusts. Eating smaller meals and staying hydrated helps.
- • Diarrhea (15–30%) — usually temporary
- • Constipation (10–20%) — fiber and hydration help
- • Vomiting (5–15%) — more common during dose increases
- • Fatigue and headache — typically mild and short-lived
The strategy most providers use: slow titration. You start at a low dose and gradually increase over weeks. This gives your body time to adjust and significantly reduces the severity of side effects. For help managing side effects, visit our GLP-1 SOS side effect relief tool.
Serious but Rare Risks
- • Pancreatitis — rare, but report severe abdominal pain to your provider immediately
- • Gallbladder issues — risk increases with rapid weight loss
- • Thyroid C-cell tumors — Boxed warning on all GLP-1 labels. In animal studies, GLP-1s caused thyroid tumors in rodents. This has not been confirmed in humans, but GLP-1s are contraindicated in people with personal or family history of medullary thyroid carcinoma (MTC) or Multiple Endocrine Neoplasia syndrome type 2 (MEN2).
The Muscle Loss Question
Rapid weight loss from any source — GLP-1s, surgery, crash diets — can include lean muscle mass. This is a legitimate concern. The solution: resistance training (even bodyweight exercises) and adequate protein intake (0.7–1g per pound of body weight per day) while on GLP-1 therapy. Your provider should be discussing this with you. Use our GLP-1 protein calculator to find your target.
Hypoglycemia Risk
For people with prediabetes (not taking insulin or sulfonylureas), the risk of hypoglycemia on GLP-1 therapy is low. GLP-1s are “glucose-dependent” — they primarily work when blood sugar is elevated. This is one of their safety advantages over older diabetes medications.
Will Insurance Cover GLP-1 for Prediabetes?
Short answer: probably not specifically for prediabetes.
Most insurance companies require one of two things for GLP-1 coverage:
- A type 2 diabetes diagnosis (for Ozempic, Mounjaro, Trulicity, Rybelsus)
- An obesity diagnosis with BMI ≥30 or BMI ≥27 with a weight-related comorbidity (for Wegovy, Zepbound, Saxenda)
Prediabetes alone typically doesn’t trigger coverage. But here’s the workaround that many people with prediabetes already qualify for: the obesity indication. If your BMI is 30+ (or 27+ with prediabetes as a comorbidity), you may qualify for Wegovy or Zepbound under the chronic weight management indication.
What to Do if You Want Insurance Coverage
- Ask your doctor about diagnosis coding. An obesity diagnosis (ICD-10: E66) with prediabetes as a comorbidity gives insurance the codes they need.
- Request prior authorization if required. Your doctor’s office can handle this.
- Check your formulary. Some plans cover Wegovy or Zepbound; many don’t. The landscape is changing quickly.
- If denied: Appeal. Ask about patient assistance programs from Novo Nordisk (for Wegovy) or Eli Lilly (for Zepbound). Or consider telehealth compounded options as an affordable alternative.
HSA/FSA
Most telehealth GLP-1 platforms accept HSA and FSA cards. This lets you use pre-tax dollars, which effectively gives you a 20–35% discount depending on your tax bracket. Read our HSA/FSA guide for GLP-1.
GLP-1 vs. Metformin for Prediabetes
Your doctor might suggest metformin first. That’s not wrong — it’s just a different trade-off.
Metformin is the classic prediabetes treatment. It’s been around for decades, it’s generic, and it costs $4–$30/month. The Diabetes Prevention Program showed it reduces diabetes risk by 31%. Side effects are usually mild (GI issues), and most doctors are extremely comfortable prescribing it.
GLP-1 medications are newer, more expensive, and more effective — particularly for weight loss and blood sugar normalization. The STEP trials show 81–89% normoglycemia with semaglutide vs. the DPP’s 58% with lifestyle alone. GLP-1s also produce significantly more weight loss (13–22% vs. 5–7% with metformin).
The practical path for most people:
- Start with lifestyle changes (the DPP approach — 7% weight loss, 150 min/week activity)
- If that’s not enough, add metformin
- If you’re still not at goal, or if you have significant obesity alongside prediabetes, consider adding or switching to a GLP-1
For people with BMI ≥30 and prediabetes, there’s a growing case for starting GLP-1 therapy earlier in the sequence — especially given the STEP 10 and SURMOUNT-1 data showing outcomes that far exceed what metformin delivered in the DPP. This is a conversation to have with your provider. The right answer depends on your specific numbers, your weight, your budget, and how aggressively you want to intervene.
What Happens If You Stop Taking GLP-1?
This is one of the most important questions people don’t ask until it’s too late. And the answer deserves a straight conversation. Learn more in our complete guide to stopping GLP-1.
The STEP 10 trial gives us the clearest picture: normoglycemia dropped from 81% while on semaglutide to 44% after 28 weeks off the medication. Weight regain is common — participants regained about two-thirds of the weight they lost. Blood sugar tends to drift back toward prediabetic levels.
Does that mean it “didn’t work”? Not at all. The semaglutide group still had 2.4 times the normoglycemia rate of the lifestyle-only group even after stopping. The medication created a head start — a significant one — that persisted even after discontinuation. You’re still better off for having taken it.
But let’s be real: if you stop without making other changes, you’ll likely see some regression. This is not unique to GLP-1s. It’s how weight and metabolism work. Blood pressure medications work the same way — stop them, and your blood pressure goes back up.
Three Strategies to Consider
Strategy 1: Plan for long-term use. A growing number of obesity medicine specialists now view GLP-1 therapy the way we view blood pressure or cholesterol medication — something you stay on because the underlying biological drivers don’t disappear when you stop the pill. At $146–$179/month through telehealth, long-term treatment is more financially feasible than the brand-name era made it seem.
Strategy 2: Use the treatment window to build your foundation. While on a GLP-1, your appetite is suppressed and weight loss comes easier. This is a window of opportunity. Use it to establish the habits that will carry you if you do come off: consistent exercise (especially strength training to preserve muscle), protein-focused nutrition, better sleep patterns, and stress management.
Strategy 3 (the hybrid most providers recommend): Use full-dose GLP-1 therapy for 6–12 months to reach your goals, then work with your provider to step down to a lower maintenance dose. Not everyone needs to stay at the maximum dose forever. Some patients do well on a lower dose that maintains most of the benefit at a lower cost and with fewer side effects.
Most providers recommend at least 6–12 months of treatment, with individualized decisions about duration based on your response and goals.
How We Ranked These GLP-1 Medications
We want to be upfront about how we made these rankings — and where our incentives lie.
Medication Rankings (Based on Clinical Evidence)
We ranked medications on: strength of prediabetes-specific clinical evidence (weighted heaviest), normoglycemia reversion rates, diabetes prevention rates, weight loss magnitude, length of available data, and safety profile. Primary sources: PubMed, NEJM, The Lancet, JAMA, FDA prescribing information, and ADA Standards of Care 2025. See our full ranking methodology.
Our medication rankings are based purely on published clinical trial data. No affiliate relationship influenced which medication ranked #1 or #5.
Telehealth Provider Rankings
We evaluated providers on: verified pricing transparency (40%), safety and legitimacy signals (20%), clinical support quality (15%), medication options and convenience (10%), cancellation friction (10%), and extras like labs and coaching (5%).
We verified pricing, auto-renewal policies, and cancellation processes for each provider. Timestamps are noted in the comparison table.
Our Affiliate Disclosure
We are an affiliate site. We earn a commission if you start treatment through our links. This is how we fund our research. See our full advertising disclosure.
This does NOT influence which medication we rank highest (clinical evidence determines that). It does influence which telehealth providers we feature — we can only recommend providers that have affiliate programs. We believe the providers listed offer genuine value, but we encourage you to compare options beyond our recommendations.
Your Next Step
You came here with a question: what’s the best GLP-1 for prediabetes? Now you have the answer — backed by clinical trial data, not marketing.
The evidence says tirzepatide and semaglutide can reverse prediabetes in 81–95% of patients. The data is strong. The medications are available. The cost barrier — while still real — is lower than it’s ever been through telehealth.
The only thing left is the decision to start.
MEDVi
$179 first month
Budget priority?
Yucca Health — $146/month on a 6-month plan. Lowest per-month cost we’ve found.
Want guaranteed results framing?
TrimRX — Results guarantee with terms plus comprehensive nutritional support included.
Low first-month price or a needle-free option?
Embody — $99 first month for the semaglutide injection (then $299/mo), plus a needle-free GLP-1 gum option, cash-pay, and 24/7 support.
Medication format options matter?
SkinnyRX — Injectable, sublingual, and tablet options. No dosage price increases.
“She was very nice and efficient with the cancellation and did not pressure me at all.” — SkinnyRX Trustpilot reviewer
The fact that a cancellation review is positive tells you something about a company’s character. Nobody celebrates cancellations — but handling them with grace is a sign that a platform isn’t just in it for the recurring charge.
All platforms require a medical evaluation by a licensed provider. You’re only charged if approved for treatment.
Frequently Asked Questions
What is the best GLP-1 for prediabetes?
Tirzepatide (Mounjaro/Zepbound) has the strongest single-trial evidence, with 95% of prediabetic patients achieving normal blood sugar in SURMOUNT-1. Semaglutide injection (Ozempic/Wegovy) is the most studied option, with 81–89% normoglycemia across the STEP trials. The best choice depends on your specific A1C level, BMI, budget, and preferences.
Are GLP-1 medications FDA-approved for prediabetes?
No. As of 2026, no medication of any kind is FDA-approved specifically for treating prediabetes or preventing type 2 diabetes. GLP-1s are FDA-approved for type 2 diabetes and/or chronic weight management and are prescribed off-label for prediabetes based on strong clinical trial evidence.
How much do GLP-1 medications cost?
Brand-name GLP-1s cost $900–$1,500/month without insurance. Compounded versions through telehealth platforms run $146–$299/month. Insurance rarely covers GLP-1s specifically for prediabetes, but you may qualify under the obesity indication if your BMI is 30+ or 27+ with comorbidities.
Can GLP-1 medications actually reverse prediabetes?
Yes. Clinical trials show 81–95% of patients reverted to normal blood sugar after 52–72 weeks of treatment with semaglutide or tirzepatide. However, some benefit fades after stopping medication, and ongoing use or sustained lifestyle changes are important for maintaining results.
What are the most common side effects?
Nausea (20–44%), diarrhea (15–30%), vomiting, and constipation — primarily during dose escalation. Most side effects are mild to moderate and improve within 4–8 weeks. Slow dose titration significantly reduces severity.
Is Rybelsus approved for prediabetes?
No. Rybelsus (oral semaglutide) is FDA-approved for type 2 diabetes only. It can be prescribed off-label for prediabetes by a healthcare provider. It uses the same active ingredient as Ozempic but in pill form with lower bioavailability.
Is metformin or GLP-1 better for prediabetes?
Metformin is cheaper ($4–$30/month) and the established first-line option per ADA guidelines, with a 31% diabetes risk reduction. GLP-1s are more effective for weight loss and blood sugar normalization but cost more. Many people benefit from starting with metformin and adding a GLP-1 if goals aren’t met.
Do I need a prescription for GLP-1 medication?
Yes. GLP-1s are prescription-only. Telehealth platforms allow you to get a prescription online through a licensed provider after a medical evaluation — no in-person visit required.
How long do I need to take GLP-1 for prediabetes?
Evidence suggests benefits are maintained while on treatment and partially fade after stopping. Most providers recommend at least 6–12 months, with ongoing use for sustained results. The goal is to build lasting lifestyle changes alongside medication use.
What is compounded semaglutide?
Compounded semaglutide is a custom-prepared version of semaglutide made by compounding pharmacies. It is not FDA-approved as a finished product, and FDA has warned that some compounded versions use semaglutide salt forms that are considered different active ingredients than the approved drug. The clinical trial results cited on this page come from FDA-approved semaglutide, not compounded versions. Compounded products are prescribed by licensed providers when clinically appropriate.
Can I get GLP-1 for prediabetes through telehealth?
Yes. Platforms like MEDVi, TrimRX, Embody, Yucca Health, and SkinnyRX connect you with licensed providers who can prescribe GLP-1 medications for prediabetes (off-label) after a medical evaluation. Medication ships directly to your home.
Will GLP-1 medication lower my A1C?
Yes. In the STEP trials, semaglutide reduced A1C by approximately 0.4–0.5 percentage points in prediabetic patients. Tirzepatide showed similar or greater reductions. For many patients, this is enough to move from the prediabetic range (5.7–6.4%) back to normal (below 5.7%).
Are there GLP-1 pills (oral options)?
Yes. Rybelsus (oral semaglutide) is available for type 2 diabetes. Compounded oral and sublingual semaglutide is available through telehealth providers like TrimRX and SkinnyRX. Embody offers a needle-free GLP-1 gum as an alternative to injections (though it is not a swallowed pill). A new oral Wegovy tablet has been FDA-approved but availability is still limited.
Sources
- McGowan BM et al. “Semaglutide for obesity and prediabetes.” Lancet Diabetes Endocrinol. 2024;12:631-642.
- Wilding JPH et al. “Once-weekly semaglutide in adults with overweight or obesity (STEP 1).” N Engl J Med. 2021;384:989-1002.
- Jastreboff AM et al. “Tirzepatide for obesity and prediabetes (SURMOUNT-1).” N Engl J Med. 2024.
- le Roux CW et al. “3 years of liraglutide versus placebo for type 2 diabetes risk reduction (SCALE).” Lancet. 2017;389:1399-1409.
- Rubino DM et al. “Effect of semaglutide with intensive behavioral therapy (STEP 3).” JAMA. 2021;325:1414-1425.
- Kahn SE et al. “Semaglutide and glycemic status in SELECT.” Diabetes Care. 2024;47:1350-1359.
- Meta-analysis: “GLP-1 RAs for prediabetes.” Diabetology & Metabolic Syndrome. 2024.
- Tsironikos GI et al. “GLP-1 RAs and normoglycemia reversion.” Diabetes Metab Res Rev. 2026;42(1):e70114.
- Diabetes Prevention Program Research Group. N Engl J Med. 2002;346:393-403.
- ADA Standards of Care in Diabetes — 2025. American Diabetes Association.
- CDC. “Prediabetes — Your Chance to Prevent Type 2 Diabetes.” cdc.gov.
- FDA Prescribing Information: Wegovy, Ozempic, Mounjaro, Zepbound, Saxenda, Trulicity, Rybelsus.
- FDA. “FDA’s Concerns About Unapproved GLP-1 Drugs Used for Weight Loss.” fda.gov.
- ADA Statement on Compounded Incretin Drugs. diabetes.org.
This content is for informational purposes only and does not constitute medical advice. Always consult your healthcare provider before starting any medication. GLP-1 medications are prescription drugs with potential side effects and contraindications. Compounded medications are not FDA-approved as finished products. Individual results vary. See our full editorial policy and affiliate disclosure for details.
Looking for a GLP-1 provider? → Compare the top online GLP-1 providers — pricing, medical oversight, and medication sourcing verified.