Switching From Semaglutide to Tirzepatide: Dosing Guide
Disclosure: Some links on this site are affiliate links. If you purchase through these links, we may earn a commission at no extra cost to you. Thank you for supporting our site. For informational purposes only—not medical advice.
On this page
If you're thinking about switching from semaglutide to tirzepatide, you're probably not here because things are going great. Maybe your weight loss has stalled. Maybe the appetite suppression that once felt like a superpower has quietly faded. Or maybe you've seen the head-to-head clinical data — tirzepatide produced nearly 50% more weight loss than semaglutide in the largest direct comparison ever conducted — and you're wondering if you're leaving results on the table.
Here's the short answer: Yes, you can switch. It's safe, it's common, and most people do it in about a week.
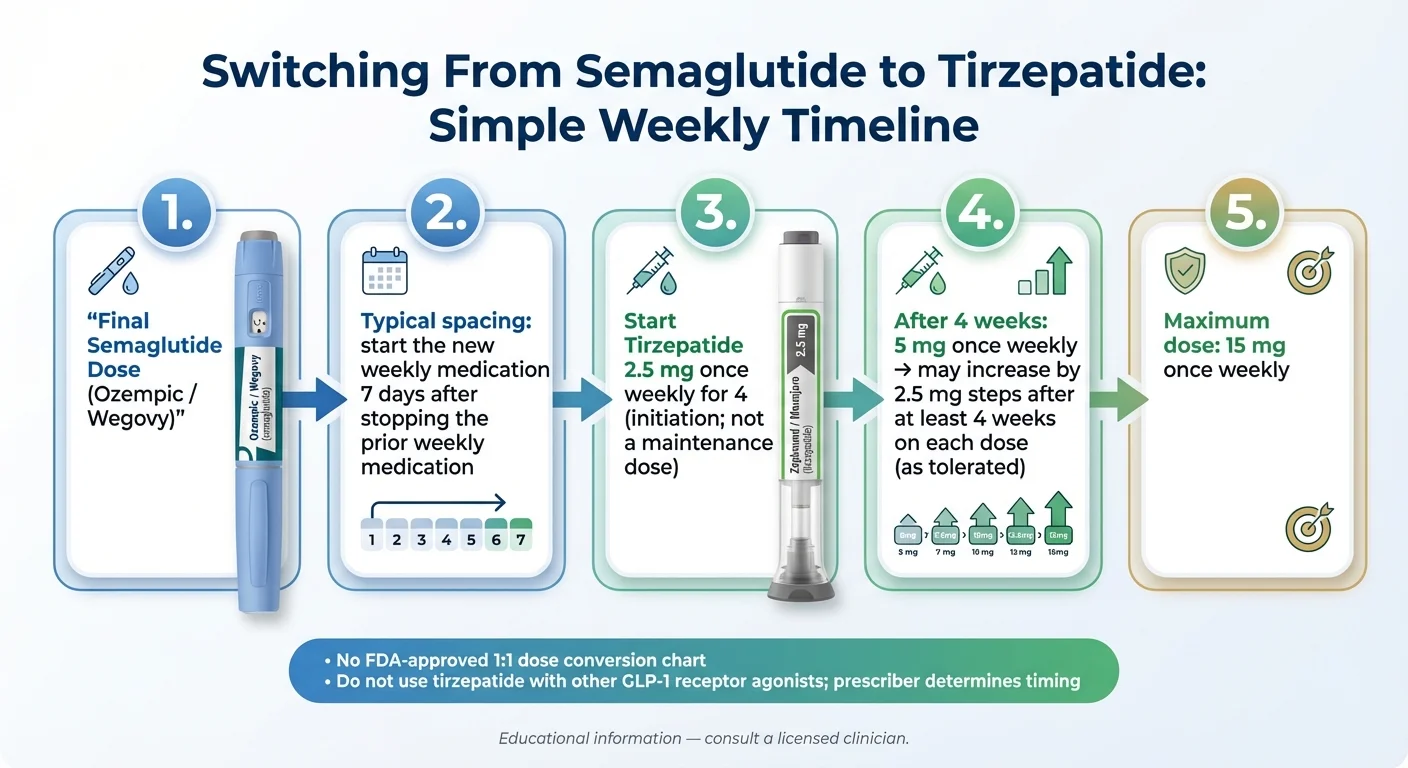
The typical process: take your final semaglutide dose, wait roughly seven days, and start tirzepatide at 2.5 mg on your next injection day. No lengthy washout. No complicated taper. Your provider sets the pace from there.
But there's a catch — and it's the reason most "conversion chart" pages on the internet get this wrong.
There is no FDA-approved dose conversion between semaglutide and tirzepatide. They work through different mechanisms, and starting at too high a dose is the number-one reason people feel terrible after switching. We'll show you exactly why — and what to do instead.
The good news? When you follow labeled titration and a simple timeline, the switch is straightforward. This guide covers everything: the safe timeline, what dose to start, what to expect week by week, real clinical data, side effects, cost, and where to get tirzepatide affordably in 2026.
Let's get into it.
Switch at a Glance
Before we go deep, here's the quick reference. Bookmark this section.
| What You Need to Know | The Answer |
|---|---|
| Can you switch? | Yes — with medical supervision |
| How long to wait | ~7 days after your last semaglutide dose (your next scheduled injection day) |
| Starting dose | 2.5 mg tirzepatide weekly — regardless of your prior semaglutide dose |
| Dose escalation | Increase by 2.5 mg every 4+ weeks as tolerated |
| Maximum dose | 15 mg/week (tirzepatide) |
| Can you overlap both? | The Zepbound label states it is not recommended for use with other GLP-1 receptor agonists; your prescriber determines timing |
| When to expect results | Appetite changes in 2-4 weeks; measurable weight loss by weeks 4-8 |
| Biggest mistake | Starting at too high a dose or skipping the 2.5 mg initiation |
Sources: Zepbound prescribing information (FDA, 2025); Ozempic/Wegovy prescribing information (FDA); Whitley et al., Clinical Diabetes, 2023.
Should You Switch From Semaglutide to Tirzepatide?
Not everyone needs to switch. And switching too early can actually slow you down. So let's be honest about when it makes sense — and when it doesn't.
Three Legitimate Reasons People Switch
1. You've plateaued on semaglutide. You gave it a real shot — months at a therapeutic dose — and the scale stopped moving. This is the most common reason people end up on this page. Plateaus on semaglutide are real, especially after 6-12 months, and they don't mean you failed. They often mean your body has adapted to a single-receptor approach and may respond to tirzepatide's dual-action mechanism.
2. Side effects haven't resolved. Persistent nausea, vomiting, or GI issues that never settled down — even after dose adjustments — can make semaglutide unsustainable long-term. Here's what surprises most people: some actually tolerate tirzepatide better. In the landmark SURMOUNT-5 trial, GI side effects caused fewer people to discontinue tirzepatide than semaglutide. We'll show you the exact numbers below.
3. You want greater results. This isn't vanity. If you started at a higher BMI and need more significant weight loss for health reasons — sleep apnea, joint damage, cardiovascular risk — the data consistently shows tirzepatide delivers meaningfully more. That's a legitimate medical reason to switch.
When Switching Is Premature (The Hard Truth)
If you haven't reached your maintenance dose of semaglutide yet, switching might be a mistake.
Semaglutide takes time. The titration schedule for Wegovy runs about 16-20 weeks before you reach the full 2.4 mg dose. If you're still at 1.0 mg and frustrated with results, you haven't given the medication a fair trial. The therapeutic effect at maximum dose is substantially different from what you experience at lower doses.
This is the kind of thing a page trying to sell you something won't tell you. We're telling you because getting this right matters more than a click.
When Extra Caution Is Needed
Switching requires more careful oversight if you have any contraindications or risk factors:
- A personal or family history of medullary thyroid carcinoma (MTC) or MEN2 syndrome
- A history of pancreatitis
- Severe gastrointestinal disease (gastroparesis, inflammatory bowel disease)
- Diabetes managed with insulin or sulfonylureas (hypoglycemia risk increases during transitions — doses must be adjusted)
- Kidney disease (dehydration from GI effects can worsen renal function)
- Pregnancy or plans to become pregnant (tirzepatide may cause fetal harm; if pregnancy is recognized, discontinue immediately and contact your prescriber)
- Diabetic retinopathy (rapid blood sugar improvement can temporarily worsen eye disease)
When in doubt, your prescriber makes the call. This guide is educational, not a prescription.
Quick Brand Translation (Because the Names Are Confusing)
| Active Ingredient | For Weight Loss | For Type 2 Diabetes | Manufacturer |
|---|---|---|---|
| Semaglutide | Wegovy | Ozempic | Novo Nordisk |
| Tirzepatide | Zepbound | Mounjaro | Eli Lilly |
Both also exist in compounded versions, prepared by licensed compounding pharmacies. Compounded products are not FDA-approved. More on that in the cost section.
How Does Tirzepatide Work Differently Than Semaglutide?
Understanding this helps everything else in this guide make sense — especially why there's no simple dose conversion. For a deeper dive into the science, see our guide on how GLP-1 medications work for weight loss.
Semaglutide is a GLP-1 receptor agonist. It activates one hormone pathway (GLP-1) that reduces appetite, slows stomach emptying, and improves insulin response. It does this well. Millions of people have lost meaningful weight on it.
Tirzepatide is a dual GIP/GLP-1 receptor agonist. It activates the same GLP-1 pathway plus a second one — GIP (glucose-dependent insulinotropic polypeptide). That second pathway enhances insulin sensitivity, may improve how your body metabolizes fat, and creates a broader metabolic effect that GLP-1 alone can't achieve.
Think of it this way: semaglutide pulls one lever. Tirzepatide pulls two. That's why tirzepatide consistently outperforms semaglutide in clinical trials — and why you can't simply convert milligrams between them. They're doing fundamentally different things at the receptor level.
The Head-to-Head Data
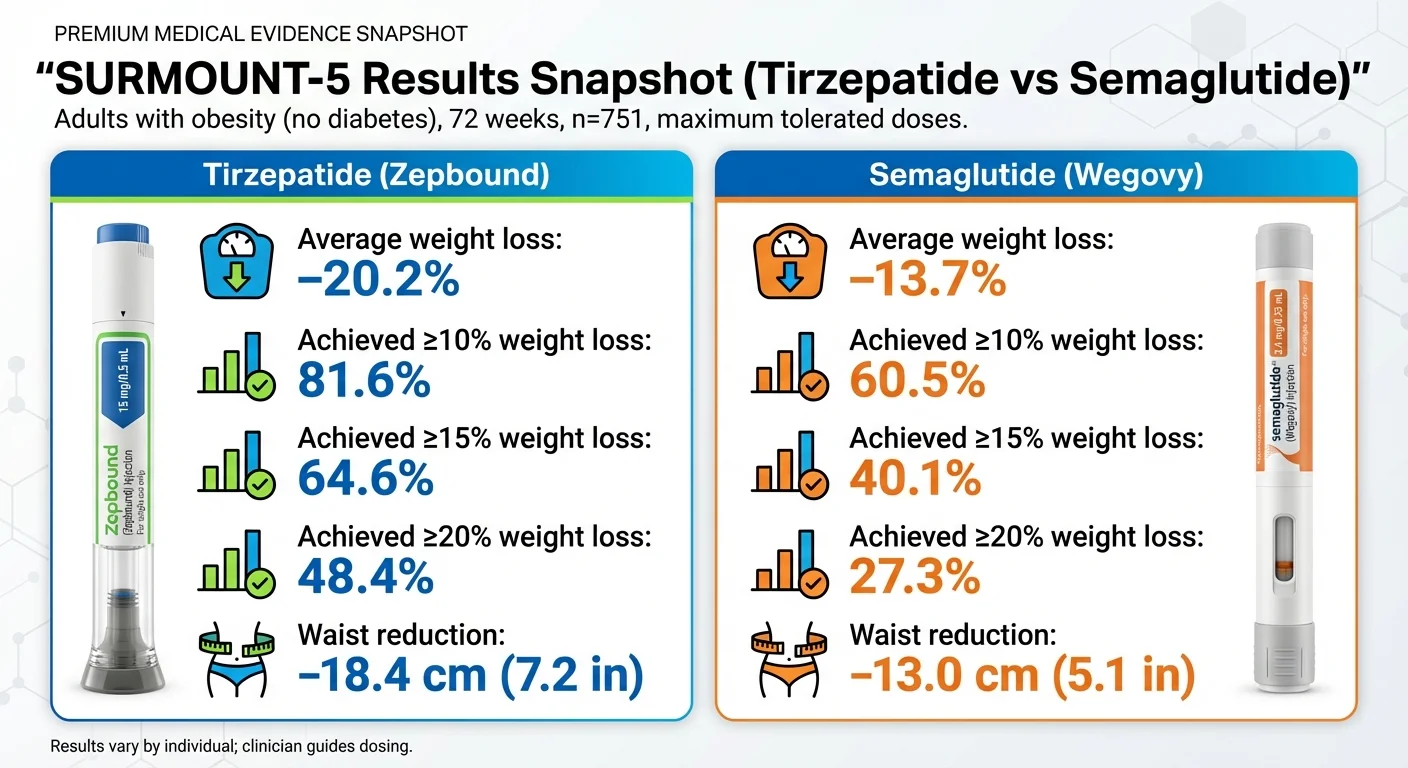
The SURMOUNT-5 trial — published in the New England Journal of Medicine (online May 11, 2025; print July 3, 2025) — is the gold standard. It's the first and only direct head-to-head comparison of tirzepatide vs. semaglutide for weight loss in people with obesity.
Study design: 751 adults with obesity (no diabetes), randomized 1:1, treated for 72 weeks at maximum tolerated doses.
| Outcome | Tirzepatide | Semaglutide | Difference |
|---|---|---|---|
| Average body weight loss | -20.2% | -13.7% | 6.5 percentage points |
| Average pounds lost (250 lb person) | ~50 lbs | ~34 lbs | ~16 lbs more |
| Waist circumference reduction | -7.2 inches | -5.1 inches | 2.1 inches more |
| Achieved 15% or more weight loss | 64.6% | 40.1% | Significantly more |
| Achieved 20% or more weight loss | 48.4% | 27.3% | About 1.8x more |
| Quit due to GI side effects | 2.7% | 5.6% | Tirzepatide lower |
Source: Aronne LJ, et al. N Engl J Med. 2025;393(1):26-36. doi:10.1056/NEJMoa2416394
Look at that last row again. Fewer people quit tirzepatide due to side effects than quit semaglutide. That surprises almost everyone — and it's one of the strongest data points in favor of switching.
Real-World Confirmation
Clinical trials are controlled environments. So what happens in the real world?
A study of over 18,000 patients published in JAMA Internal Medicine found the same pattern:
| Timeframe | Tirzepatide (avg loss) | Semaglutide (avg loss) |
|---|---|---|
| 3 months | -5.9% | -3.6% |
| 6 months | -10.1% | -5.8% |
| 12 months | -15.2% | -8.3% |
Tirzepatide users were 76% more likely to achieve at least 5% weight loss, and more than three times as likely to reach 15%.
Source: Rodriguez PJ, et al. JAMA Intern Med. 2024;184(9):1056-1064.
What This Means If You're Switching
More average weight loss doesn't guarantee your specific result. Genetics, lifestyle, starting weight, sleep, protein intake, and activity all matter.
But the trend is clear and consistent across every study: people who switch from semaglutide to tirzepatide tend to continue losing weight — not stall. In a prospective study by Jabbour et al. (Endocrine Practice, 2024), patients switching from a GLP-1 to tirzepatide 5 mg lost an average of 2.15 kg (about 4.7 lbs) of additional weight in just the first 12 weeks.
You're not starting over. You're upgrading the tool.
Switching Timeline: How Long After Semaglutide Can You Start Tirzepatide?
This is the question that causes the most anxiety. And the answer is simpler than the internet makes it seem.
The Standard Approach: Wait About 7 Days
For most people switching between weekly injectables, the standard approach is to start the new medication approximately one week after the last dose of the previous one — essentially on your next scheduled injection day.
This is supported by published switching guidance and aligns with the pharmacokinetics of both drugs.
You do NOT need:
- A lengthy "washout period" of weeks or months
- To gradually taper semaglutide down
- To wait until semaglutide is completely eliminated from your system (that would take ~5 weeks — far too long)
You DO need:
- To NOT overlap — never inject both in the same week
- To start tirzepatide at 2.5 mg regardless of your prior dose
- Medical supervision throughout the transition
Same-Day Switch vs. 7-Day Gap vs. Longer Pause
Your provider will decide which approach fits your situation. Here's the general framework:
7-day gap (most common): You take your last semaglutide shot, skip one week, and start tirzepatide on what would have been your next injection day. This is the default for most people and the approach supported by published switching literature.
Same-day switch (less common): Some clinicians, particularly for patients with diabetes where blood sugar control is critical, may start tirzepatide on the same day the next semaglutide dose would have been due — effectively zero gap. This is a clinical judgment call based on your risk profile.
Longer pause (rare): If you had severe side effects on semaglutide or have specific medical concerns, your provider may want a longer washout. This is uncommon but appropriate in certain situations.
For the vast majority of people switching for weight loss: 7 days is the sweet spot.
Why Not Wait Longer?
Semaglutide has a half-life of approximately 7 days. That means it's still circulating at low levels for roughly 5 weeks after your last injection. But waiting that long creates problems:
- Appetite suppression fades and hunger spikes return
- Blood sugar control drifts (especially important for people with diabetes)
- You risk regaining weight during the gap
- Motivation and momentum suffer
The 7-day approach keeps you on a consistent weekly rhythm while giving enough spacing to avoid stacking GLP-1 activity.
What If You Missed Your Last Semaglutide Dose?
If it's been more than 2 weeks since your last semaglutide injection, the approach may differ. Your provider needs to know:
- How long it's actually been since your last dose
- Whether you're still experiencing any medication effects (appetite suppression, GI symptoms)
- Whether your blood sugar has shifted (for diabetes patients)
Don't guess here. A quick message to your prescriber clarifies the right timing.
Semaglutide to Tirzepatide Dosing: Is There a Conversion Chart?
This is the section that separates trustworthy information from everything else on the internet. Pay attention.
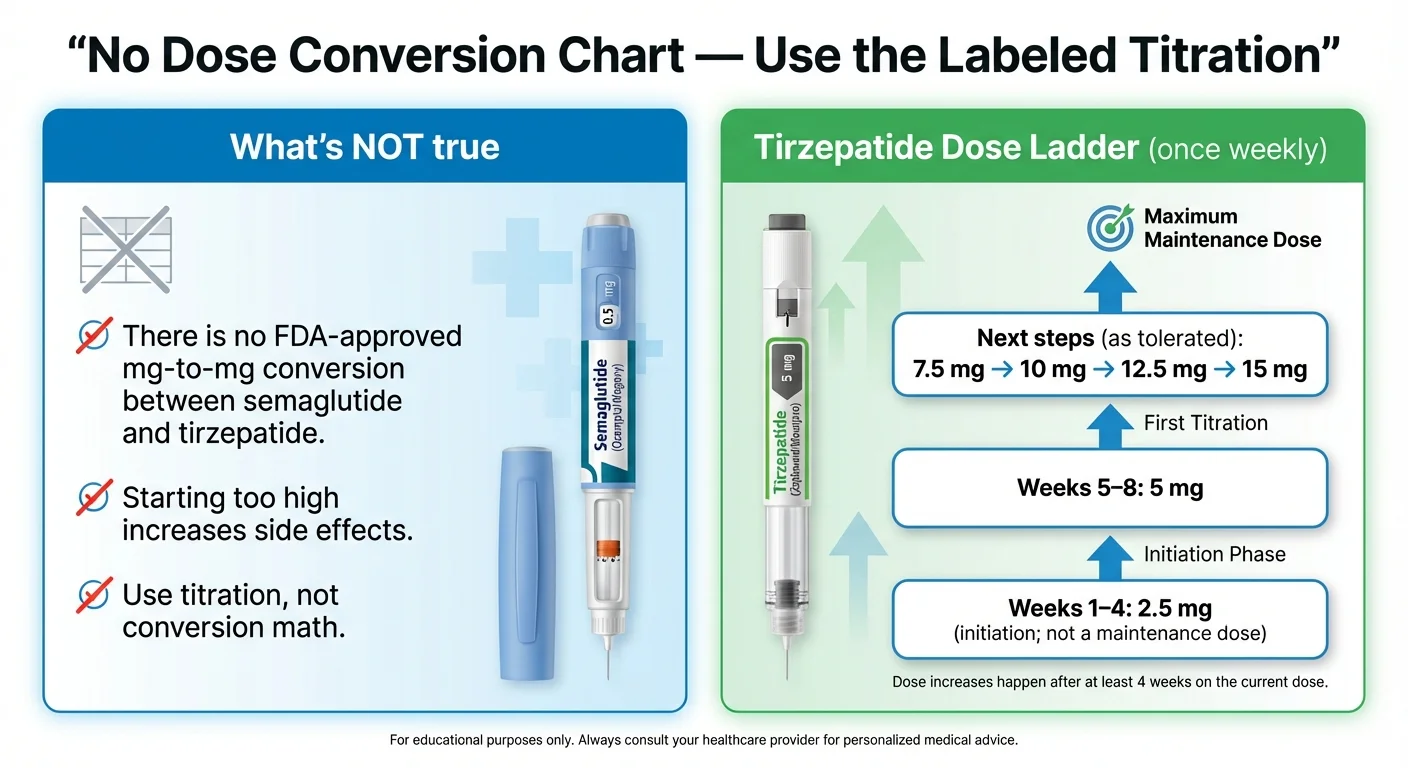
The Truth: There Is No FDA-Approved Dose Conversion
Semaglutide and tirzepatide have different receptor profiles, different potency curves, and different dose ranges. You cannot say "2.4 mg of semaglutide equals X mg of tirzepatide." That math doesn't exist.
The FDA labeling for tirzepatide (Zepbound/Mounjaro) is explicit: all patients begin at 2.5 mg weekly for at least 4 weeks, then increase by 2.5 mg increments based on tolerability and response.
That includes you. Even if you were on the maximum 2.4 mg of Wegovy, you start tirzepatide at the bottom.
Why "Conversion Charts" Online Often Mislead
You've probably seen tables claiming Ozempic 1.0 mg "equals" Mounjaro 5.0 mg, or similar. These are approximations created for clinical discussion about glycemic effect in diabetes patients — not weight-loss equivalence, and not switching instructions.
Using them to pick your own starting dose is how people end up with severe nausea, vomiting, and the conviction that tirzepatide "doesn't agree with them" — when the real problem was starting too high.
Why Starting Low Isn't a Step Backward
It feels counterintuitive. You were on a high dose, and now you're starting over? But here's why it works:
1. Different mechanism. Tirzepatide activates GIP receptors that semaglutide never touched. Your body has zero experience with this pathway in medication form.
2. GI protection. The most common side effects happen during dose escalation. Starting low gives your digestive system time to adjust to a drug that works differently than what it's used to.
3. GLP-1 tolerance doesn't transfer cleanly. Being tolerant of 2.4 mg semaglutide says nothing about how you'll respond to 10 mg tirzepatide. Different drug, different receptors, different dose-response curve.
Some experienced providers do start GLP-1-adapted patients at 5 mg (skipping the 2.5 mg initiation) when the patient tolerated semaglutide well and had minimal GI issues. That's a clinical judgment call — not something to decide on your own or ask for because you're impatient.
Tirzepatide Titration Schedule
| Weeks | Dose | What to Expect |
|---|---|---|
| 1-4 | 2.5 mg | Initiation dose. Not therapeutic for weight loss — your body is adjusting. |
| 5-8 | 5.0 mg | First maintenance-eligible dose. Many people feel real appetite suppression here. |
| 9-12 | 7.5 mg | Increased efficacy. Weight loss typically accelerates. |
| 13-16 | 10.0 mg | Strong response for most patients. Many stay here. |
| 17-20 | 12.5 mg | Near-maximum. Only if needed for continued progress. |
| 21+ | 15.0 mg | Maximum approved dose. Not everyone needs it. |
Source: Zepbound prescribing information (FDA, 2025). Minimum 4-week intervals between increases.
Not everyone needs 15 mg. If you're getting good results at 7.5 or 10 mg with tolerable side effects, your provider may keep you there. Higher isn't automatically better — it's about the dose that works best for your body.
Side-by-Side Dose Reference (Not a Conversion)
This shows the labeled dose ranges side by side. Use it as a conversation starter with your prescriber, not as a switching recipe.
| Semaglutide (Wegovy) | Semaglutide (Ozempic) | Tirzepatide (Zepbound/Mounjaro) |
|---|---|---|
| 0.25 mg (start) | 0.25 mg (start) | 2.5 mg (start) |
| 0.5 mg | 0.5 mg | 5.0 mg |
| 1.0 mg | 1.0 mg | 7.5 mg |
| 1.7 mg | 2.0 mg (max) | 10.0 mg |
| 2.4 mg (max) | — | 12.5 mg |
| — | — | 15.0 mg (max) |
Warning: These are NOT equivalent doses. They are separate titration schedules as labeled by the FDA. Rows are aligned by escalation step, not by clinical equivalence.
Adapted from Whitley HP, et al. Clinical Diabetes. 2023;41(3):467-473.
How to Switch: The Step-by-Step Process
Print this. Screenshot it. Bring it to your appointment.
Step 1: Confirm What You're Switching From — and To
This matters more than you'd think:
- From Ozempic? That's semaglutide for type 2 diabetes. If you're switching to Zepbound (tirzepatide for weight loss), your indication changes. Insurance coverage may differ.
- From Wegovy? That's semaglutide for weight management. Switching to Zepbound keeps you in the same indication category.
- From compounded semaglutide? Verify your exact dose with your provider before switching — compounded formulations may be measured or concentrated differently than brand-name products.
Step 2: Set Your "Last Dose" Date
Take your final semaglutide injection on your normal schedule. Mark that date. Your tirzepatide start will be approximately 7 days later.
Step 3: Start Tirzepatide at 2.5 mg
On your next scheduled injection day (~7 days later), take your first tirzepatide dose. Same injection areas work — abdomen, thigh, or upper arm. Rotate sites.
If your provider starts you at 5 mg based on your history and tolerability, follow their guidance.
Step 4: Track What Matters for the First 4 Weeks
Keep a simple daily log. Nothing fancy — notes app, journal, spreadsheet. Track:
- Appetite level (1-10)
- Any nausea or GI symptoms
- Water intake
- Protein intake
- Energy and mood
- Weight (weekly, same conditions)
- Blood sugar (if you have diabetes — this is critical)
This log is invaluable at your first dose-adjustment appointment. Providers can make much better decisions with real data.
Step 5: Escalate Based on Tolerability
After at least 4 weeks at 2.5 mg, your provider decides whether to increase to 5 mg. The pattern continues every 4+ weeks. Don't push for faster escalation — the research is clear that tolerance-guided titration produces better outcomes and fewer dropouts.
Your Switching Checklist
- Confirmed current semaglutide dose and brand with your provider
- Discussed contraindications and medication interactions
- Received tirzepatide prescription with titration plan
- If on insulin or sulfonylureas: discussed dose adjustments to prevent hypoglycemia
- Taken last semaglutide dose on your normal day
- Waited ~7 days
- Started tirzepatide at 2.5 mg (or 5 mg per provider)
- Set up a tracking system
- Scheduled a follow-up at 4 weeks
- Stocked up on protein sources, water, and ginger (for nausea)
What to Expect After Switching: Week by Week
This is the section that replaces the 2 AM forum spiral. Here's what actually happens, based on clinical data, provider reports, and patient accounts.
Week 1: The Gap Week
You've taken your last semaglutide shot. Semaglutide is still active in your body — it has a ~7-day half-life, so blood levels are declining but present. Most people feel normal this week. Appetite suppression may even continue.
What to do: Stay hydrated. Eat normally. Prep your tirzepatide supplies. Don't panic that nothing has changed yet — nothing should change yet.
Weeks 2-3: First Tirzepatide Doses (2.5 mg)
You've started tirzepatide. Mild GI effects are possible — similar to what you felt when you first started semaglutide. Nausea, slight stomach upset, maybe looser stools.
Some people feel almost nothing because their body is already GLP-1-adapted. Others feel a definite shift because the GIP pathway is new territory. Both responses are normal.
What to do: Eat smaller meals. Prioritize protein. Don't force food if you're not hungry, but don't skip meals entirely — you still need nutrition. Four to five small meals beats two or three large ones during this phase.
Weeks 4-6: "Is It Working?"
Appetite suppression becomes more noticeable. Many people describe it as steadier and more consistent than what semaglutide felt like. The food noise — that constant background hum of thinking about food — quiets. Carb cravings often drop noticeably.
If your provider increases you to 5 mg around week 5, you'll feel a meaningful step up. This is typically where weight loss begins in earnest for switchers.
What to do: Don't obsess over the daily scale. Weigh weekly, same time, same conditions. Take progress photos. Notice how clothes fit. The trend matters more than any single number.
Weeks 8-12: Finding Your Stride
This is the window where most people feel the full benefit of switching. Weight loss accelerates compared to late-stage semaglutide. Energy often improves. The hunger that crept back during the semaglutide plateau? Gone for most.
GI side effects — if you had any — have usually resolved by now.
What to do: Stay consistent. This is where the compound effect kicks in. Keep protein high (aim for 0.7-1.0 g per pound of your goal body weight), stay active, and hydrate aggressively.
Months 3-6: Compounding Results
As your dose titrates through 7.5 mg, 10 mg, and potentially higher, results continue building. In SURMOUNT-5, the average weight loss at 72 weeks was 20.2% — roughly 50 pounds for someone starting at 250 lbs.
But the benefits go well beyond the scale:
- Waist circumference drops (average 7+ inches in SURMOUNT-5)
- Blood pressure improves
- Blood sugar and HbA1c improve
- Lipid profiles improve (triglycerides, cholesterol)
- Sleep quality improves — Zepbound is FDA-approved for moderate-to-severe obstructive sleep apnea in adults with obesity, in combination with a reduced-calorie diet and increased physical activity
- Cardiovascular risk decreases — a SURMOUNT-5 post-hoc analysis showed a 2.4% absolute 10-year CVD risk reduction with tirzepatide vs. 1.4% with semaglutide
- Quality of life scores increase across the board
Sources: Aronne LJ, et al. NEJM 2025; Mamas MA, et al. European Heart Journal Open, 2025.
The Realistic Expectation
Most people who switch from semaglutide to tirzepatide after a plateau see the trend line move again within 4-8 weeks. Not everyone has a dramatic 50-pound result. Some see steady, gradual improvement rather than a sudden cliff drop. That's normal and still represents success.
The key question at 12 weeks: Is the trend moving in the right direction? If yes, you're on track.
Side Effects: What's Normal vs. What's a Red Flag
Tirzepatide has side effects. Same drug class, same general profile. But the specifics might surprise you.
The Common GI Cluster
These typically appear during dose escalation and improve as your body adjusts:
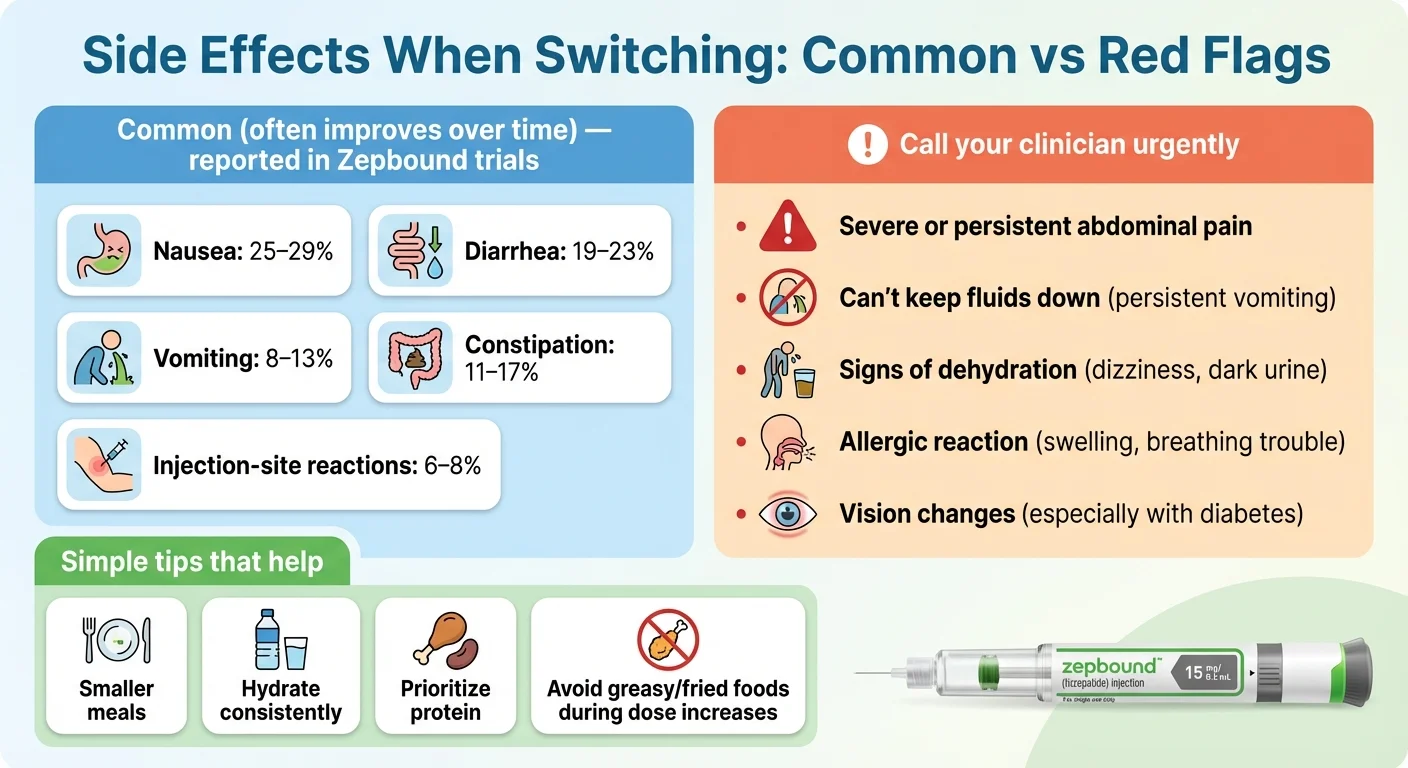
| Side Effect | Incidence | What It Feels Like | Usually Resolves |
|---|---|---|---|
| Nausea | 25-29% | Mild queasiness, especially after meals | 2-4 weeks after each dose increase |
| Diarrhea | 19-23% | Looser/more frequent stools | 1-3 weeks |
| Constipation | 11-17% | Less frequent or harder stools | Ongoing for some; manageable |
| Decreased appetite | Expected | Feeling full faster, reduced food noise | This is the desired effect |
| Vomiting | 8-13% | Occasional, usually early in titration | 1-2 weeks |
| Injection site reaction | 6-8% | Mild redness or itching | Hours to days |
The key stat: In SURMOUNT-5, gastrointestinal side effects caused 2.7% of tirzepatide users to stop treatment, vs. 5.6% of semaglutide users. The side effects exist, but fewer people find them intolerable compared to semaglutide.
For a comprehensive look at what to expect, see our complete GLP-1 side effects guide.
The Side-Effect Minimization Playbook
These practical strategies make the first few weeks significantly more manageable:
- Eat smaller, more frequent meals. Four to five small meals beats two to three large ones. Your stomach empties slower on this medication — don't overwhelm it.
- Prioritize protein at every meal. Protein digests slower, stabilizes blood sugar, and helps preserve muscle during weight loss. Aim for 25-30g per meal.
- Stay aggressively hydrated. Minimum 64 oz of water daily, more if active. Dehydration worsens every GI side effect.
- Avoid high-fat, greasy, and fried foods during dose escalation. These amplify nausea more than anything else. You can reintroduce them gradually later.
- Ginger helps. Ginger tea, ginger chews, or ginger supplements reduce nausea for many people. It's not just folklore — there's clinical evidence behind it.
- Stop eating before you feel full. The "full" signal is delayed on GLP-1 medications. By the time you feel stuffed, you've already overeaten.
- Fiber for constipation. Psyllium husk (Metamucil) or magnesium citrate, with plenty of water.
- Eat slowly. This single change prevents half the GI complaints. Set your fork down between bites. It sounds basic because it works.
When to Call Your Provider (Red Flags)
Most side effects are temporary nuisances. But contact your healthcare provider immediately for:
- Severe, persistent abdominal pain — especially pain that radiates to your back (possible pancreatitis)
- Persistent vomiting that prevents you from keeping liquids down for 24+ hours
- Signs of dehydration — dark urine, dizziness, rapid heartbeat, dry mouth
- Signs of allergic reaction — rash, swelling, difficulty breathing
- Vision changes (especially important for people with diabetes)
- A lump or swelling in your neck
- Significant mood changes, depression, or suicidal thoughts — suicidal behavior and ideation have been reported in clinical trials with other weight management products; monitor for changes and report to your provider
Switching Because Semaglutide "Stopped Working"? Read This First
If you're here because you hit a plateau, welcome to the majority. Plateaus on semaglutide are genuinely common — and they don't mean you failed.
But before you switch, it's worth 60 seconds checking whether something else is going on. Sometimes the plateau isn't the medication.
The 5 Most Common Plateau Causes
- Calorie creep. Appetite suppression faded, portions slowly grew, and you didn't notice. Happens to everyone eventually.
- Protein dropped. Many people on GLP-1s eat less overall but also eat less protein. Less protein means more muscle loss means slower metabolism means plateau.
- Movement decreased. Your NEAT (non-exercise activity thermogenesis) naturally drops as you lose weight. Fewer pounds to carry means fewer calories burned doing everything.
- Sleep and stress. Poor sleep and chronic stress increase cortisol, which promotes fat storage and hunger — even on medication.
- You're at the dose ceiling. Semaglutide maxes out at 2.4 mg (Wegovy). If you need more, it literally can't give you more.
The "Before You Switch" Self-Check
Answer honestly:
- Are you at the maximum dose (2.4 mg Wegovy or 2.0 mg Ozempic)?
- Are you eating at least 100g of protein per day?
- Are you walking 7,000-10,000+ steps daily?
- Are you sleeping 7+ hours most nights?
- Have you been consistent with injections — no missed doses?
- Are you drinking enough water?
- Have you checked for constipation (which can mask true weight on the scale)?
If you answered "no" to several of these, fixing those issues might restart progress without switching. Protein and sleep alone account for a shocking number of GLP-1 plateaus.
If you answered "yes" to all of them and you're still stuck after 3+ months at max dose? Tirzepatide is very likely the right next move.
When Switching Is the Right Call
Switching makes the most sense when:
- You've been at maximum semaglutide dose for 3+ months with no meaningful progress
- You've addressed the lifestyle factors above
- Your provider agrees you've maximized semaglutide's potential
- The clinical data supports a better outcome with dual-agonist therapy
At that point, switching isn't giving up. It's what a well-informed patient does with good data.
Ready to discuss the switch with a provider? If cost or access is a barrier, MEDVi connects you with a licensed physician who can evaluate your history and prescribe tirzepatide — starting at $279/month with medication, evaluations, and shipping included.
Check if You Qualify for Tirzepatide Through MEDViSpecial Populations: Diabetes, Pregnancy, and Other Considerations
Not everyone switching is in the same situation. Here's what you need to know if any of these apply to you.
Switching With Type 2 Diabetes
If you're on Ozempic (semaglutide for diabetes) and switching to Mounjaro (tirzepatide for diabetes), there are additional considerations:
Blood sugar monitoring is non-negotiable. Tirzepatide may improve blood sugar control more aggressively than semaglutide, especially as doses increase. If you're also on insulin or a sulfonylurea, there's real hypoglycemia risk during the transition.
Your provider will likely:
- Reduce insulin doses preemptively to prevent low blood sugar
- Ask you to monitor blood glucose more frequently during the first 4-8 weeks
- Adjust other diabetes medications based on your response
The good news: The SURPASS-2 trial (published in NEJM, 2021) showed tirzepatide produced superior HbA1c reduction compared to semaglutide in patients with type 2 diabetes. Better blood sugar control is likely on the other side of this switch.
Pregnancy and Family Planning
Tirzepatide may cause fetal harm. If pregnancy is recognized, stop tirzepatide and contact your prescriber immediately.
Important for women using oral birth control: Because tirzepatide can affect absorption of oral contraceptives during dose changes, the Zepbound label advises switching to a non-oral contraceptive method or adding a barrier method (such as condoms) for 4 weeks after starting tirzepatide and for 4 weeks after each dose increase. Talk to your provider about contraception planning before and during treatment.
Kidney Disease
GLP-1 medications (including tirzepatide) can cause nausea, vomiting, and diarrhea that lead to dehydration — which can worsen kidney function or trigger acute kidney injury. If you have pre-existing kidney disease, your provider will:
- Monitor kidney function labs during the transition
- Emphasize hydration more aggressively
- Potentially titrate more slowly
Gallbladder Issues
GLP-1 medications, including tirzepatide, are associated with gallbladder-related events (cholelithiasis, cholecystitis). Rapid weight loss itself also increases gallstone risk. If you have a history of gallbladder problems, mention this to your provider before switching.
7 Myths About Switching (and What's Actually True)
There's a lot of bad information floating around forums, social media, and even some clinic websites. Let's clean it up.
Myth 1: "You need a washout period of several weeks before starting tirzepatide."
Reality: No. The standard approach is approximately 7 days — your next scheduled injection day. Waiting weeks means losing appetite control, potential blood sugar drift, and possible weight regain. Published switching guidance supports the weekly-to-weekly approach for most patients.
Myth 2: "There's a dose conversion chart — you just match your semaglutide dose to the equivalent tirzepatide dose."
Reality: There is no FDA-approved dose conversion. These are different drugs with different receptor targets. Every patient starts tirzepatide at 2.5 mg for at least 4 weeks, then titrates based on individual response. The "conversion charts" circulating online were created for glycemic-control discussions in diabetes — not for weight-loss dose matching.
Myth 3: "If semaglutide made you nauseous, tirzepatide will be worse."
Reality: Not necessarily. In the SURMOUNT-5 trial, gastrointestinal side effects caused 2.7% of tirzepatide users to stop treatment — compared to 5.6% of semaglutide users. Some people who couldn't tolerate semaglutide do fine on tirzepatide. Starting at 2.5 mg and titrating slowly is the key.
Myth 4: "You're basically starting over when you switch."
Reality: You're not starting from zero. Your body has been on a GLP-1 agonist — it's adapted to that pathway. The 2.5 mg starting dose is there to introduce the new GIP pathway safely, not because your prior treatment doesn't count. Most switchers see results faster than someone starting GLP-1 therapy for the first time.
Myth 5: "Compounded tirzepatide is dangerous."
Reality: The picture is more nuanced than "safe" or "dangerous." Compounded tirzepatide is not FDA-approved, and FDA has issued warnings about unapproved GLP-1 products marketed for weight loss — including quality and dosing concerns. However, compounding from licensed, accredited US pharmacies through a legitimate prescriber is a legal and established practice across many drug classes. The key is sourcing: work only with a licensed provider who can verify their pharmacy's credentials (look for PCAB accreditation or USP 797/800 compliance). For help evaluating providers, see our best compounded tirzepatide providers guide.
Myth 6: "You'll regain all your weight during the switch."
Reality: The transition period is typically one week. Semaglutide is still active in your body during that window (it has a ~7-day half-life), so appetite control doesn't vanish overnight. Short-term fluctuations of 1-3 lbs are possible, but meaningful regain in a 7-day gap is unlikely — and studies show switchers continue losing weight, not gaining.
Myth 7: "Tirzepatide is just a 'stronger' version of semaglutide."
Reality: It's not just more of the same thing. Tirzepatide activates an entirely different receptor (GIP) in addition to GLP-1. This dual mechanism affects appetite, insulin sensitivity, and fat metabolism through pathways that semaglutide doesn't touch. Calling it "stronger semaglutide" is like calling a hybrid car a "faster gas car" — it's a fundamentally different approach.
What Your Provider Will Want to Know (Be Ready)
Walking into the switching conversation prepared saves time and leads to better decisions. Here's what your prescriber will likely ask — and what you should have ready.
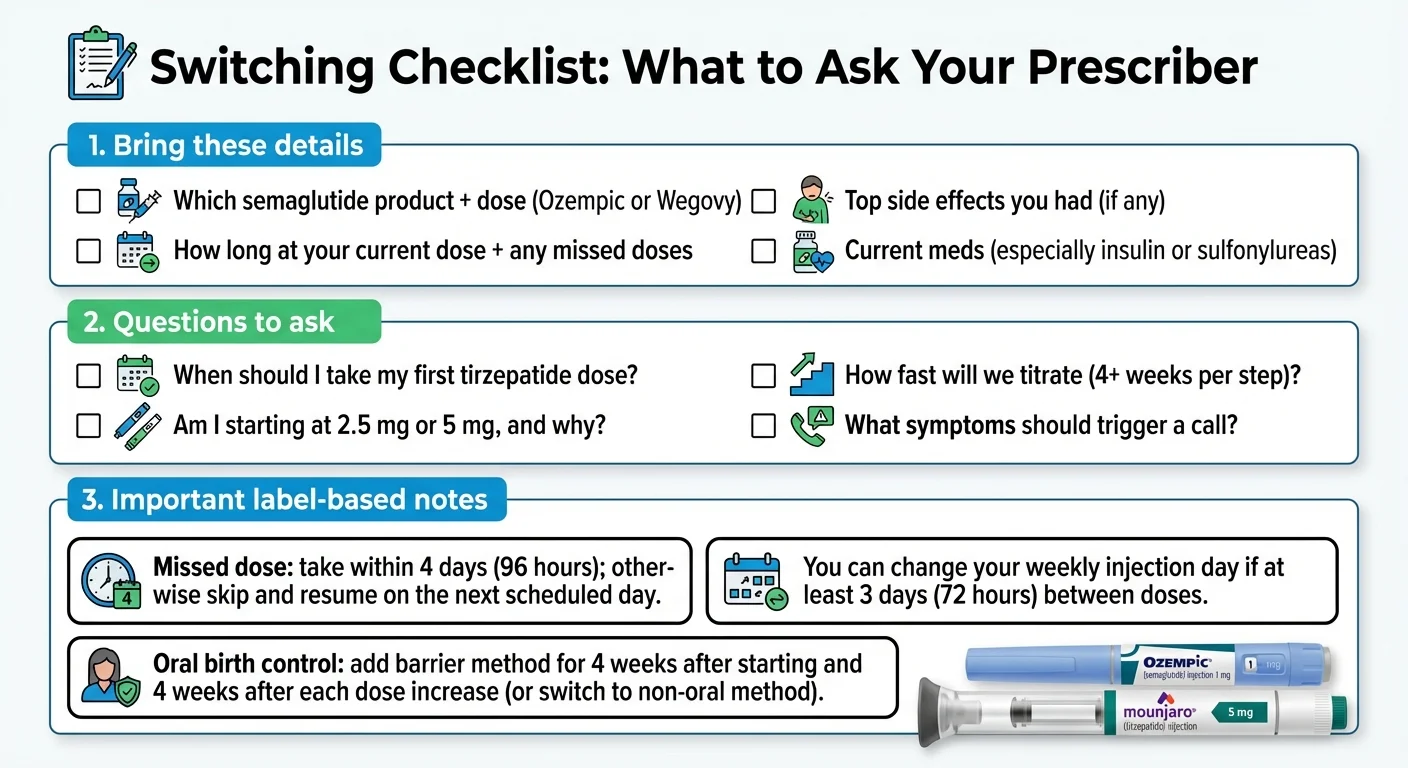
Your Medication History
- Current medication and exact dose (Ozempic 1.0 mg? Wegovy 2.4 mg? Compounded 1.5 mg?)
- How long you've been on it (weeks, months, years)
- Whether you've reached your maximum dose — and how long you've been there
- Any missed doses recently
- Side effects you've experienced — which ones, how severe, when they occurred
Your Weight Loss History
- Starting weight vs. current weight on semaglutide
- When weight loss stalled (specific timeframe)
- What you've already tried to break the plateau (protein changes, exercise, sleep optimization)
- Previous weight loss medications or programs if any
Your Health Profile
- All current medications — especially insulin, sulfonylureas, blood thinners, or thyroid medications
- Chronic conditions — diabetes, kidney disease, liver disease, gallbladder history, pancreatitis history
- Family history of thyroid cancer (specifically medullary thyroid carcinoma)
- Pregnancy status or plans
- Recent lab work — HbA1c, kidney function, lipid panel
What to Ask Your Provider
Don't just answer questions — ask them too:
- "Based on my history, should I start at 2.5 mg or 5 mg?"
- "Do any of my other medications need dose adjustments during the switch?"
- "What's our titration plan — how fast will we increase?"
- "What specific things should I monitor and report back?"
- "When should I schedule my next follow-up?"
- "If brand-name isn't covered by my insurance, what's your experience with compounded tirzepatide through telehealth providers?"
Having this conversation prepared turns a 30-minute appointment into a productive, efficient visit — and your provider will appreciate it.
Making the Most of the Switch: Lifestyle Adjustments
Switching medications is a tool change, not a strategy change. The people who get the best long-term results from tirzepatide aren't just taking the injection — they're building the foundation that makes the medication work harder.
The Four Pillars That Multiply Tirzepatide's Effect
1. Protein — the non-negotiable. Aim for 100-150g daily (or 0.7-1.0g per pound of your goal body weight). Protein preserves muscle mass during weight loss, which keeps your metabolism running. It also keeps you feeling satisfied between meals, which synergizes with tirzepatide's appetite effects. Every meal should have a meaningful protein source.
2. Movement — especially resistance training. Walking 7,000-10,000 steps daily handles the cardiovascular base. But adding 2-3 strength training sessions per week is what separates people who lose fat from people who lose both fat and muscle. You don't need a gym — bodyweight exercises, resistance bands, or dumbbells at home all work.
3. Sleep — the invisible multiplier. Poor sleep increases cortisol, increases hunger hormones (even on medication), reduces insulin sensitivity, and promotes fat storage. Seven to eight hours is the target. If you're not sleeping well, fixing this may matter more than any dose change.
4. Consistency over intensity. The people who keep the weight off aren't doing extreme diets or marathon training sessions. They're hitting their protein target most days, moving regularly, sleeping well, and taking their injection on schedule. Week after week. That boring consistency is what actually works.
Planning for the Long Haul
GLP-1 therapy is increasingly understood as long-term treatment — not a short course. When patients stop tirzepatide, studies show most regain roughly two-thirds of lost weight within a year. This isn't a character flaw. It's how these medications work: they modify the hormonal signals that drive hunger and metabolism. Remove the medication, and those signals return to baseline.
Think of it like blood pressure medication. You don't take it for six months and then expect your blood pressure to stay low forever. You take it because it keeps working as long as you're on it.
This framing matters because it affects how you think about cost. That $279/month through a program like MEDVi isn't a temporary expense — it's an ongoing investment in the version of yourself you're building. Most people find that the benefits — better health markers, more energy, improved confidence, fewer co-morbidity costs — justify the long-term commitment.
Cost, Insurance & Access in 2026
The best clinical data in the world doesn't matter if you can't afford the medication. Let's talk real numbers. For a broader look at pricing across all GLP-1 medications, see our GLP-1 cost guide or use our GLP-1 cost finder tool.
Brand-Name Tirzepatide Pricing
| Access Route | Monthly Cost | What's Included |
|---|---|---|
| Zepbound + commercial insurance + savings card | $25-$150 | Best-case; requires covered plan + Lilly savings card |
| Zepbound self-pay vials (LillyDirect) | $349/mo (2.5 mg), $499/mo (5 mg); 7.5-15 mg doses priced higher — refill within 35 days to maintain pricing | No insurance needed; single-dose vials from Lilly directly; prices subject to change |
| Zepbound at pharmacy (list price) | ~$1,086 | Standard price without any discounts |
| Mounjaro (diabetes indication) | ~$1,080 | Different FDA indication; insurance more likely to cover |
The 2026 reality: Many employer-sponsored plans have been dropping GLP-1 coverage. Medicare and Medicaid coverage is expanding on a specific timeline. Medicaid coverage for anti-obesity medications takes effect in May 2026 under the Inflation Reduction Act provisions. For Medicare, CMS launched the BALANCE model — a demonstration program beginning July 2026 that aims to reduce out-of-pocket costs for GLP-1 medications (target: roughly $2/day for eligible beneficiaries). Broader Medicare Part D coverage is expected to phase in starting January 2027. Coverage and eligibility will depend on your specific plan and program rules — verify benefits before assuming coverage. Always check with your insurer, as prior authorization requirements are common even when coverage exists.
Looking ahead: Oral GLP-1 options are also in development. Orforglipron, an oral GLP-1 receptor agonist currently in Phase 3 trials, could expand access further if approved — potentially offering a non-injection alternative at lower cost. No approval timeline has been set.
Telehealth Programs: A More Affordable Path
If brand-name tirzepatide is out of reach — and for many people, it is — physician-supervised telehealth programs offer legitimate access at significantly lower cost. These programs typically prescribe compounded tirzepatide and include medical supervision, the prescription, and the medication in one bundled price.
What to know about compounded tirzepatide:
- Compounded drugs are not FDA-approved and are not reviewed by FDA for safety, effectiveness, or manufacturing quality
- FDA has issued consumer warnings about unapproved and potentially fraudulent GLP-1 products marketed for weight loss, including dosing and quality risks
- FDA policy around compounding of tirzepatide has been tied to drug shortage status and enforcement discretion timelines — availability and regulatory status can change
- Quality varies significantly by pharmacy — reputable providers work with pharmacies that maintain PCAB accreditation or USP 797/800 compliance
- When obtained through a licensed provider who verifies pharmacy sourcing, compounded medications can be significantly less expensive than brand-name
- Always discuss compounded options with your clinician and verify the pharmacy's credentials before starting
Provider Comparison
| Route | What You Get | Monthly Cost | Turnaround | Best For |
|---|---|---|---|---|
| Your existing doctor | Brand-name Rx; may require specialist referral | Insurance copay or list price | Varies (days-weeks) | People with good insurance coverage |
| Weight management clinic | Specialized care, in-person monitoring | Varies widely | 1-2 weeks typically | Complex medical situations |
| MEDVi | Physician evaluation, compounded tirzepatide, metabolic report, 1:1 guidance, medication shipped to door, 24/7 provider messaging | From $279/mo | Ships within days | People without coverage who want all-inclusive pricing and ongoing support |
| Other telehealth programs | Varies by provider | $299-$699/mo | Varies | Depends on offerings |
Why we recommend MEDVi for most people making this switch: Their program bundles the medical evaluation, prescription, medication, shipping, and ongoing provider access into one transparent price — no surprise fees for consultations, dose changes, or check-ins. They work with licensed US compounding pharmacies and offer 24/7 messaging, which matters when you're navigating a medication transition and have a question at 10 PM on a Tuesday.
They also back it up with a satisfaction guarantee — review their current refund policy and guarantee terms for specific conditions and eligibility before enrolling.
MEDVi reports serving over 500,000 patients to date. Read our full MEDVi review for a detailed breakdown.
Check if You Qualify for Tirzepatide Through MEDViDisclosure: We earn a commission if you use our link. This doesn't change your cost or what we write. We recommend MEDVi because after evaluating dozens of telehealth GLP-1 programs, their pricing, support, and transparency consistently rank highest. Our full editorial policy is here.
Real Results: What People Experience After Switching
Clinical data is powerful. But hearing from people who've been exactly where you are? That makes the decision feel real.
Verified MEDVi patient (ConsumerAffairs):
Prescribed tirzepatide with B12 — went from 158 to 138 in two months. Weight came off daily. It made me feel full immediately, so I ate less. It pretty much resets how you look at food.
Verified Drugs.com user (Mounjaro):
Life-changing. I've been on it for months and the results keep coming.
Verified Drugs.com user (Zepbound):
If I have to deal with some nausea, I'll do it. The trade-off is worth it.
These aren't miracle stories. They're the common experience — renewed appetite control, steady weight loss, and the feeling that the medication is actually working again after a plateau. The nausea fades. The results don't.
Not everyone's experience is dramatic. Some see steady, gradual progress rather than a sudden shift. That's success too. The important metric is whether your trend line is moving at 8-12 weeks.
Frequently Asked Questions
Is there a semaglutide to tirzepatide conversion chart?
Not an FDA-approved one. These drugs work through different mechanisms (single vs. dual receptor), so a direct mg-to-mg conversion doesn't exist. The standard approach is starting tirzepatide at 2.5 mg regardless of your prior semaglutide dose, then titrating up. Any "conversion chart" online is an approximation for clinical discussion — not a switching instruction.
What is the equivalent dose of Ozempic to Mounjaro?
There is no established equivalence. Ozempic (semaglutide) and Mounjaro (tirzepatide) have different receptor targets and dose ranges. If you're switching from Ozempic, you start Mounjaro at 2.5 mg weekly for at least 4 weeks, then increase based on your response.
What is the equivalent dose of Wegovy to Zepbound?
Same answer — there's no FDA-approved equivalent. Even at maximum Wegovy (2.4 mg), you start Zepbound at 2.5 mg. The drugs produce different effects through different pathways, so dose matching isn't clinically meaningful.
How long after my last semaglutide shot can I start tirzepatide?
About 7 days — typically on your next scheduled injection day. This aligns with semaglutide's weekly dosing rhythm and is the most common approach in published switching guidance. No extended washout is needed.
Can I take semaglutide and tirzepatide at the same time?
The Zepbound label states it is not recommended for use with other GLP-1 receptor agonists. Your prescriber determines timing — overlapping could increase side-effect risk without added benefit.
Will I regain weight while switching?
Short-term fluctuations of 1-3 lbs are possible during the transition week as medication levels shift. But studies show people who switch from a GLP-1 to tirzepatide typically continue losing weight rather than regaining.
What if I had bad nausea on semaglutide — will tirzepatide be worse?
Not necessarily. Some people who struggled with semaglutide's GI effects actually tolerate tirzepatide better. In SURMOUNT-5, fewer people discontinued tirzepatide due to GI side effects (2.7%) than semaglutide (5.6%). Starting at 2.5 mg and titrating slowly gives your body the best chance to adjust.
What if I'm switching because semaglutide isn't working?
First confirm you've maximized semaglutide: reached max dose, given it 3+ months, optimized protein and lifestyle factors. If you've done all that and plateaued, switching to tirzepatide is a well-supported clinical decision. The dual-mechanism approach often breaks through single-agonist plateaus.
What if I'm switching for diabetes, not weight loss?
The process is similar — stop semaglutide, wait ~7 days, start tirzepatide at 2.5 mg. But blood sugar monitoring is critical. If you're on insulin or sulfonylureas, your provider must adjust doses to prevent hypoglycemia. The SURPASS-2 trial showed tirzepatide produced better blood sugar control than semaglutide for type 2 diabetes.
What dose of tirzepatide equals 2.4 mg of semaglutide?
There's no direct equivalence. They activate different receptors. Even at 2.5 mg (the lowest dose), tirzepatide activates GIP receptors that semaglutide doesn't touch at any dose. Your dose is set by response and tolerability — not by conversion math.
How fast will I lose weight after switching?
Most people notice appetite changes in 2-4 weeks. Measurable weight loss typically becomes clear by weeks 4-8, especially after the dose increases to 5 mg. In clinical trials, average weight loss reached ~20% by 72 weeks.
Is tirzepatide "stronger" than semaglutide?
In terms of average weight loss, consistently yes — across clinical trials and real-world data. But "stronger" doesn't mean right for everyone. The dual mechanism produces a broader metabolic effect, which is why average results are greater.
What if tirzepatide doesn't work for me?
If you've reached a therapeutic dose (typically 7.5-10+ mg) and maintained it for 8-12 weeks without meaningful results, discuss next steps with your provider. Options include dose adjustment, lifestyle changes, or alternative medications. No single drug works identically for every person.
Does insurance cover tirzepatide in 2026?
It depends on your plan, indication, and insurer. Commercial coverage is growing but often requires prior authorization. Medicare and Medicaid coverage is expanding on a defined timeline — Medicaid coverage for anti-obesity medications begins May 2026, the CMS BALANCE model demonstration starts July 2026 for Medicare beneficiaries, and broader Part D coverage is expected to phase in from January 2027. Coverage will depend on your specific plan and eligibility. Many employer plans have reduced GLP-1 coverage. Always verify before assuming.
If insurance doesn't cover it, telehealth providers like MEDVi offer physician-supervised tirzepatide starting at $279/month — no insurance required.
What's the difference between Mounjaro and Zepbound?
Same active ingredient (tirzepatide), same manufacturer (Eli Lilly), same injection. Different FDA indications: Mounjaro for type 2 diabetes, Zepbound for chronic weight management and obstructive sleep apnea.
Can I switch from Ozempic to Mounjaro?
Yes — same process described throughout this guide. Stop Ozempic, wait ~7 days, start Mounjaro at 2.5 mg. Your provider manages the transition with attention to blood sugar control.
What about switching from compounded semaglutide?
Same process. Confirm your exact compounded dose with your provider first (formulations may differ in measurement), then follow the standard timeline.
How long does semaglutide stay in your system?
Semaglutide has a ~7-day half-life. It takes roughly 5 half-lives (~5 weeks) to be essentially eliminated. You don't need to wait that long to start tirzepatide — some overlap at low levels is expected and clinically manageable.
What labs should I get before and during the switch?
This depends on your health profile. Standard monitoring includes weight, blood pressure, and periodic labs (fasting glucose, HbA1c, lipid panel, kidney function). For diabetes patients, more frequent glucose monitoring is essential. Your provider sets the specific schedule.
Can I switch my injection day when starting tirzepatide?
Yes. You can change your injection day as long as there are at least 3 days (72 hours) between doses. Don't take two doses within 3 days of each other.
What foods help with nausea during the transition?
Bland, easily digestible foods work best: plain crackers, toast, rice, bananas, broths, and anything with ginger. Avoid greasy, spicy, or heavy foods during dose escalation. Small frequent meals, cold foods, and eating slowly all help.
What about constipation?
Common on GLP-1 medications. Management: psyllium husk (Metamucil) or magnesium citrate daily, adequate water (64+ oz), high-fiber vegetables, regular walking. If persistent despite these measures, talk to your provider — they may recommend a stool softener or adjust your approach.
Can I drink alcohol while switching?
No direct drug interaction, but alcohol worsens nausea, adds empty calories, lowers food-choice inhibitions, and affects blood sugar. Most providers recommend limiting alcohol during the transition, especially during dose escalation periods.
Will I lose muscle mass?
Some muscle loss accompanies any significant weight loss — this applies to all methods, not just GLP-1s. Minimize it by eating adequate protein (0.7-1.0 g per pound of goal body weight), strength training 2-3 times weekly, and not creating extreme calorie deficits by skipping meals.
What if I miss a tirzepatide dose?
If you miss a dose and it's been less than 4 days (96 hours) since it was due, take it as soon as possible. If more than 4 days have passed, skip that dose and take the next one on your regular schedule. Don't double up.
What happens if I stop tirzepatide eventually?
Like semaglutide, stopping typically leads to weight regain. Studies show patients regain approximately two-thirds of lost weight within a year of stopping. This isn't weakness — it's biology. These medications work by modifying hormonal hunger signals, and when the medication stops, those signals return. Most providers frame GLP-1 therapy as long-term treatment, similar to blood pressure medication.
How do I inject tirzepatide? Is it different from semaglutide?
Both come as pre-filled single-dose pens. The injection technique is virtually identical: choose a site (abdomen, thigh, or upper arm), clean the area, inject subcutaneously, hold for a few seconds, dispose of the pen properly. If you've been injecting semaglutide, the mechanics will feel familiar. The needle gauge and pen design may differ slightly between brands. You can also explore our tirzepatide pills vs. shots comparison for more on oral formulations currently in development.
Can I travel with tirzepatide?
Yes. Keep medication refrigerated when possible (36-46 degrees F / 2-8 degrees C). Tirzepatide can be stored at room temperature (up to 86 degrees F / 30 degrees C) for up to 21 days if needed during travel. Bring your prescription label, carry it in your carry-on (never checked luggage), and consider a small insulated travel case for longer trips.
Should I change my diet when switching?
No dramatic overhaul needed. But the transition is a good time to optimize: prioritize protein at every meal (minimum 25-30g), stay hydrated, and eat smaller portions since your fullness signals may change. Many people find their food preferences shift naturally on tirzepatide — especially reduced cravings for refined carbs and sugary foods. Lean into that.
What if my insurance covers semaglutide but not tirzepatide?
This is common. Options include: requesting a prior authorization with documentation of semaglutide failure/plateau, appealing a denial with clinical evidence supporting the switch, exploring Eli Lilly's savings programs for commercially insured patients, or using a telehealth program like MEDVi for physician-supervised compounded tirzepatide at a lower out-of-pocket cost.
Is compounded tirzepatide the same as Zepbound?
Compounded tirzepatide is prepared by compounding pharmacies to individual prescriptions. It is not an FDA-approved product and has not been reviewed by FDA for safety, effectiveness, or manufacturing quality. Brand-name Zepbound goes through FDA manufacturing and quality oversight. Compounded versions obtained through licensed, accredited pharmacies can be a more affordable option for many patients, but they are not interchangeable in a regulatory sense. FDA has issued warnings about unapproved GLP-1 products — always work with a licensed provider who can verify pharmacy sourcing.
How much weight will I lose per month on tirzepatide?
Individual results vary significantly. In SURMOUNT-5, the average was roughly 20% of body weight over 72 weeks — which works out to about 3-4 pounds per month on average. But it's not linear. Most people see slower loss in the first month (during dose initiation), acceleration during months 2-6, and gradual slowing as they approach a new equilibrium. Some months you'll lose 6 lbs, others 1 lb. Focus on the 3-month trend, not the weekly number.
Do I need to exercise on tirzepatide?
You don't need to exercise for the medication to work. But exercise — particularly resistance training — dramatically improves outcomes. It preserves lean muscle mass (critical during rapid weight loss), improves insulin sensitivity, boosts mood and energy, and helps maintain results long-term. Even 20-30 minutes of resistance training 3 times per week makes a measurable difference.
Can my primary care doctor prescribe tirzepatide, or do I need a specialist?
Most primary care physicians can prescribe tirzepatide. You don't necessarily need an endocrinologist or weight management specialist, though complex cases (diabetes requiring insulin adjustment, multiple comorbidities) may benefit from specialist involvement. Telehealth providers like MEDVi also have licensed physicians who can prescribe and manage tirzepatide remotely.
What's the success rate of switching from semaglutide to tirzepatide?
"Success rate" depends on how you define success. In SURMOUNT-5, 64% of tirzepatide users achieved 15% or more weight loss and about 48% achieved 20% or more. In real-world data (18,000+ patients), tirzepatide users were 76% more likely to achieve clinically significant weight loss compared to semaglutide. For people switching specifically after a semaglutide plateau, published case series report the majority resume losing weight after transitioning.
Why This Switch Is Becoming So Common
Five years ago, switching between GLP-1 medications was unusual. Today, it's one of the most common medication changes in weight management.
Here's why: the data got clearer, access got easier, and patients got smarter.
When semaglutide (Ozempic/Wegovy) launched, it was revolutionary. Average weight loss of 12-15% was unprecedented for a medication. But tirzepatide changed the math. The dual-agonist mechanism consistently delivers 15-20% weight loss in real-world settings — and the SURMOUNT-5 trial showed it beating semaglutide head-to-head by a wide margin.
At the same time, telehealth platforms have made access dramatically simpler. You no longer need an in-person specialist appointment, a months-long referral process, and a cooperative insurance company to get tirzepatide. Programs like MEDVi can evaluate your history, prescribe the medication, and ship it to your door — often faster than your local pharmacy can fill a brand-name script.
The combination of better data + easier access has made the semaglutide-to-tirzepatide switch the single most common medication transition in the GLP-1 space. If you're considering it, you're not an early adopter anymore. You're following a well-worn, well-studied path.
The question isn't really "can I switch?" anymore. The question is whether you've given semaglutide a fair trial, whether the data supports a better outcome with tirzepatide for your situation, and whether you have a clear path to access it. If the answer to all three is yes — the decision is straightforward.
Important Safety Information
Boxed Warning: Tirzepatide carries a warning regarding thyroid C-cell tumors. In animal studies, tirzepatide caused these tumors. It is not known whether this occurs in humans. Tirzepatide is contraindicated in patients with a personal or family history of medullary thyroid carcinoma (MTC) or Multiple Endocrine Neoplasia syndrome type 2 (MEN2).
Contraindications: Known serious hypersensitivity to tirzepatide or any formulation component; personal or family history of MTC or MEN2.
Warnings and precautions include: pancreatitis, gallbladder-related events, hypoglycemia (with insulin or sulfonylureas), acute kidney injury, diabetic retinopathy complications, hypersensitivity reactions, and suicidal behavior and ideation (reported in clinical trials with other weight management products; monitor for mood changes).
Pregnancy: Tirzepatide may cause fetal harm. If pregnancy is recognized, discontinue and contact your prescriber.
This guide is for informational purposes only and does not constitute medical advice. Always consult a licensed healthcare provider before starting, stopping, or changing any medication.
Sources: Zepbound prescribing information (FDA, 2025); Mounjaro prescribing information (FDA, 2025).
Ready to Make the Switch?
If you've read this far, you're more informed about switching from semaglutide to tirzepatide than most patients — and honestly, many providers.
Here's what you now know:
- The switch is safe, well-studied, and increasingly common
- Tirzepatide produced roughly 50% more average weight loss than semaglutide in the only head-to-head trial
- The timeline is simple: last semaglutide dose, wait ~7 days, start tirzepatide at 2.5 mg
- There's no dose conversion — you start low and titrate up
- Side effects are manageable, and fewer people quit tirzepatide than semaglutide due to side effects
- The biggest real-world obstacle is cost and access
You're not starting over. You're not failing. You're making a data-driven decision to use a better tool.
The science is on your side. The clinical data is on your side. And the path is clearer than you probably thought when you started researching.
If you're ready to take the next step: The fastest route is connecting with a licensed provider who can evaluate your history and prescribe tirzepatide. If cost is a barrier, MEDVi offers physician-supervised tirzepatide starting at $279/month — medication, evaluations, and shipping included. No insurance needed.
Check if You Qualify for Tirzepatide Through MEDViOur Sources & Editorial Standards
What We Used
This guide is built on primary medical sources:
- Aronne LJ, et al. "Tirzepatide as Compared with Semaglutide for the Treatment of Obesity." N Engl J Med. 2025;393(1):26-36. doi:10.1056/NEJMoa2416394. — PubMed
- Rodriguez PJ, et al. Real-world weight loss comparison (n=18,386). JAMA Internal Medicine. 2024;184(9):1056-1064. — JAMA
- Mamas MA, et al. SURMOUNT-5 cardiovascular risk analysis. European Heart Journal Open. 2025. — PubMed
- Jabbour S, et al. "Switching to Tirzepatide 5 mg From GLP-1 Receptor Agonists: Clinical Expectations in the First 12 Weeks." Endocrine Practice. 2024;30(8):701-709. — PubMed
- Whitley HP, et al. GLP-1/GIP agonist dosing strategies. Clinical Diabetes. 2023;41(3):467-473. — PMC
- Frias JP, et al. SURPASS-2 (tirzepatide vs. semaglutide, type 2 diabetes). NEJM. 2021. — NEJM
- Zepbound prescribing information. FDA, 2025. — FDA
- Ozempic prescribing information. FDA, 2025. — FDA
- Wegovy prescribing information. FDA, 2023. — FDA
- Mounjaro prescribing information. FDA, 2022. — FDA
- Switching between GLP-1 receptor agonists: rationale and practical guidance. — PMC
What We Did NOT Do
- We did not provide personalized medical advice
- We did not accept payment from any medication manufacturer or provider to influence rankings or coverage
- We did not fabricate patient testimonials — all quotes are from verified third-party review platforms
- We did not present compounded medications as equivalent to FDA-approved products
How We Keep This Current
This page is reviewed monthly. It's updated when FDA labeling changes, major clinical trial data is published, or pricing and access information shifts materially. The "last updated" date at the top always reflects the most recent review.
Editorial Standards:
- All clinical claims cite peer-reviewed or FDA sources
- Provider pricing verified February 2026
- Patient quotes from verified third-party review platforms (ConsumerAffairs, Drugs.com)
- Affiliate relationships disclosed per FTC guidelines
- Updated when new data, pricing, or regulatory changes occur
How we rank + verify
Last verified: March 20, 2026
What we verified: FDA prescribing information for Zepbound/Mounjaro and Wegovy/Ozempic, SURMOUNT-5 head-to-head trial data (NEJM 2025), SURPASS-2 diabetes data (NEJM 2021), JAMA Internal Medicine real-world study (18,000+ patients), Endocrine Practice switching guidance, provider pricing as of February 2026.
Sources: FDA labels, NEJM (SURMOUNT-5, SURPASS-2), JAMA Internal Medicine, Endocrine Practice, Clinical Diabetes, PubMed, ConsumerAffairs reviews, Drugs.com reviews
Related Articles
Tirzepatide pills vs shots compared — efficacy, cost, side effects, and which form fits you. Updated February 2026.
How GLP-1 medications like Ozempic and Wegovy work for weight loss. Mechanism map, clinical trial results, side effects, and decision framework.
Complete GLP-1 side effects guide from FDA labels: what's normal, what's serious, and how to manage symptoms on Ozempic, Wegovy, Mounjaro, Zepbound.
GLP-1 cost breakdown for 2026. Real prices for Wegovy, Zepbound, Ozempic with insurance, cash-pay, and Medicare options. Updated January 2026.
Best compounded tirzepatide providers compared on pharmacy quality, real pricing, clinical oversight, and verified reviews. MEDVi ranked #1 for 2026.
MEDVi Reviews: verified pricing, 11,498+ Trustpilot reviews analyzed, updated product lineup, cancellation policies, and legitimacy check. Updated March 2026.
This content is educational only and does not replace professional medical advice. Always consult a qualified healthcare provider before starting any medication.