GLP-1 for Beginners: How They Work, What to Expect, and How to Start Safely
Disclosure: Some links on this site are affiliate links. If you purchase through these links, we may earn a commission at no extra cost to you. Thank you for supporting our site.·For informational purposes only—not medical advice.
17 Sources Cited · Jump to Sources ↓
The short version: GLP-1 medications are prescription drugs that reduce appetite, slow digestion, and help with weight loss by mimicking a hormone your body already makes. The FDA-approved options for weight management — Wegovy (semaglutide) and Zepbound (tirzepatide) — have shown average weight loss of 15% to 22% of body weight in clinical trials.[1][2] As of 2026, they're available as weekly injections or a daily pill, and pricing depends on your insurance, dose, and whether you go brand-name or telehealth.
This is the guide we wish existed when we started researching GLP-1s. We reviewed FDA prescribing information, clinical trials, and current manufacturer and CMS pricing and coverage pages — so you don't have to open 30 browser tabs to figure out what this is, whether it's for you, and how to start without getting ripped off.
If you're short on time, use the jump links below. If you want the whole picture, keep reading.
In This Guide
What Is GLP-1 in Plain English?
GLP-1 stands for glucagon-like peptide-1. It's a hormone your gut releases after you eat. Its job is to tell your brain you're full, slow down digestion so nutrients absorb better, and help your pancreas manage blood sugar.
Your body makes GLP-1 on its own. The problem is that the natural version breaks down in minutes. It doesn't last long enough to make a significant difference for people dealing with obesity or type 2 diabetes.
GLP-1 medications are lab-engineered versions of that hormone designed to stick around much longer — hours or even days instead of minutes. That extended duration is what makes them powerful enough to meaningfully reduce appetite, change eating behavior, and produce real weight loss.
Here's the part that trips up most beginners: "GLP-1" is the category. The brand names are what you've actually heard of. Ozempic, Wegovy, Mounjaro, Zepbound — these are all GLP-1 medications (or closely related). Different brand names, different approved uses, but they all work on the same biological pathway.
Quick decoder:
| You've heard of... | The active drug is... | FDA-approved use most relevant to beginners |
|---|---|---|
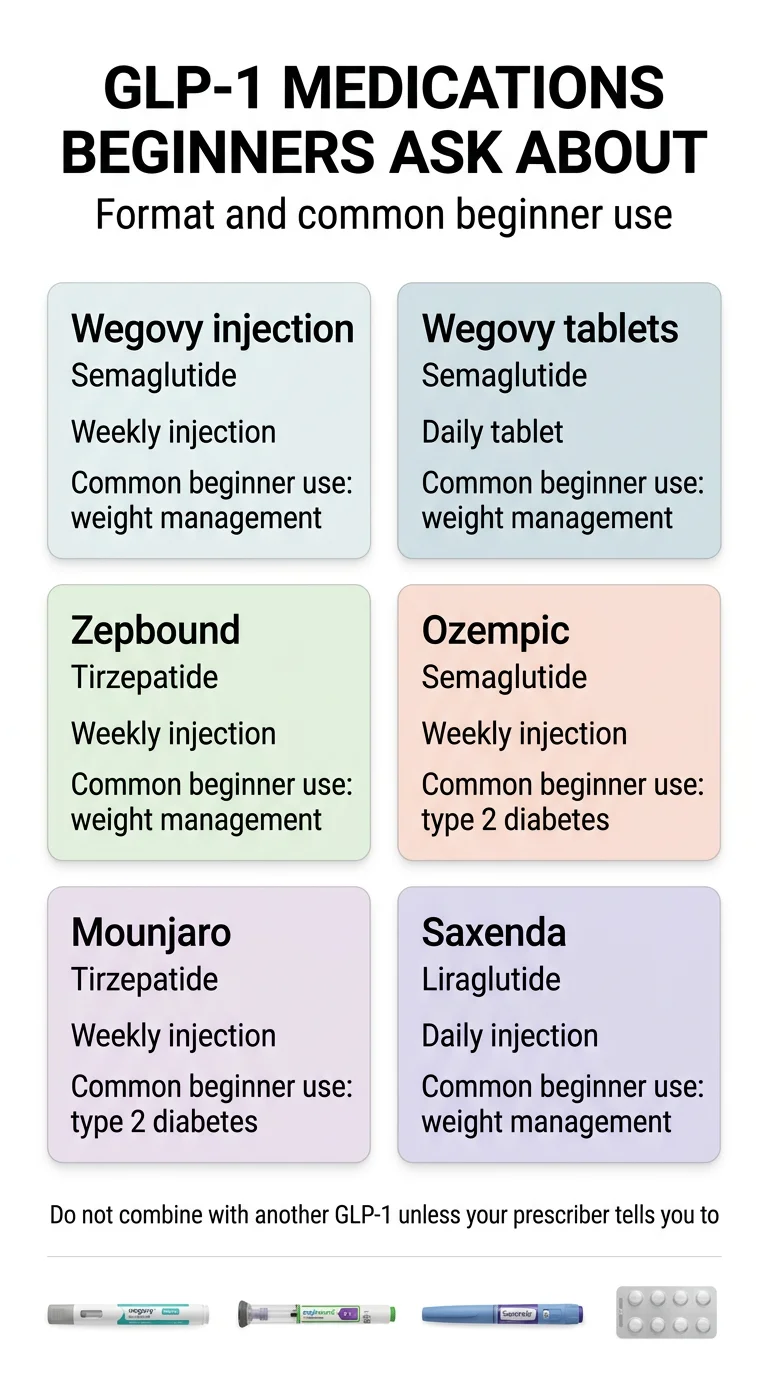
| Wegovy (injection) | Semaglutide | Weight management, cardiovascular risk reduction, and other indications |
| Wegovy (pill) | Semaglutide (oral) | Weight management and cardiovascular risk reduction |
| Ozempic | Semaglutide | Type 2 diabetes (also has CV and CKD risk-reduction indications) |
| Zepbound | Tirzepatide | Weight management and moderate-to-severe obstructive sleep apnea in adults with obesity |
| Mounjaro | Tirzepatide | Type 2 diabetes |
| Saxenda | Liraglutide | Weight management |
One thing worth understanding early: Ozempic and Wegovy both contain semaglutide, but they carry different FDA approvals and are dosed differently. Ozempic is approved for diabetes. Wegovy is approved for weight loss at a higher dose. A doctor can prescribe Ozempic off-label for weight loss, and many do. Same relationship with Mounjaro (diabetes) and Zepbound (weight loss) — both contain tirzepatide, but with different approved indications and dosing.
Sources: [3]–[8] FDA prescribing information for each medication
Why Is Everyone Talking About GLP-1 Right Now?
If it feels like GLP-1 medications went from niche diabetes drugs to front-page news overnight, you're not imagining it. A few things happened at once.
The weight loss data landed. Clinical trials published in the New England Journal of Medicine showed that semaglutide produced around 15% average body weight loss, and tirzepatide produced around 22% at higher doses.[1][2] For context, most previous weight-loss drugs struggled to hit 5–7%. These numbers changed the conversation.
The uses keep expanding. Beyond weight loss, the FDA has approved Wegovy to reduce major cardiovascular events in certain adults with obesity or overweight and established heart disease.[9] Zepbound received FDA approval for moderate-to-severe obstructive sleep apnea in adults with obesity.[6] Researchers are studying GLP-1 medications for kidney disease, liver disease, and even addiction. Every new headline creates more "Could this work for me?" searches.
A pill version arrived. In December 2025, the FDA approved the first oral GLP-1 for weight management — the Wegovy pill.[4] It launched in January 2026. For people who don't want injections, this changed everything. Eli Lilly's oral version (orforglipron) may get FDA approval later in 2026.
Pricing started shifting. New manufacturer self-pay programs, the federal TrumpRx pricing initiative, and upcoming Medicare coverage for obesity indications through the CMS BALANCE model and Medicare GLP-1 Bridge are all making these medications more accessible than they were even a year ago.[10]
But the confusion grew, too. Brand names vs. generics. Injections vs. pills. Insurance vs. cash pay vs. compounded. FDA-approved vs. telehealth programs. Celebrity endorsements vs. medical reality. It's a lot. That confusion is exactly why we built this guide — to help you cut through the noise and understand what actually matters for your situation.
How Do GLP-1 Medications Actually Work?
GLP-1 medications do three things at once, and understanding all three helps explain why they produce results that dieting alone often can't.
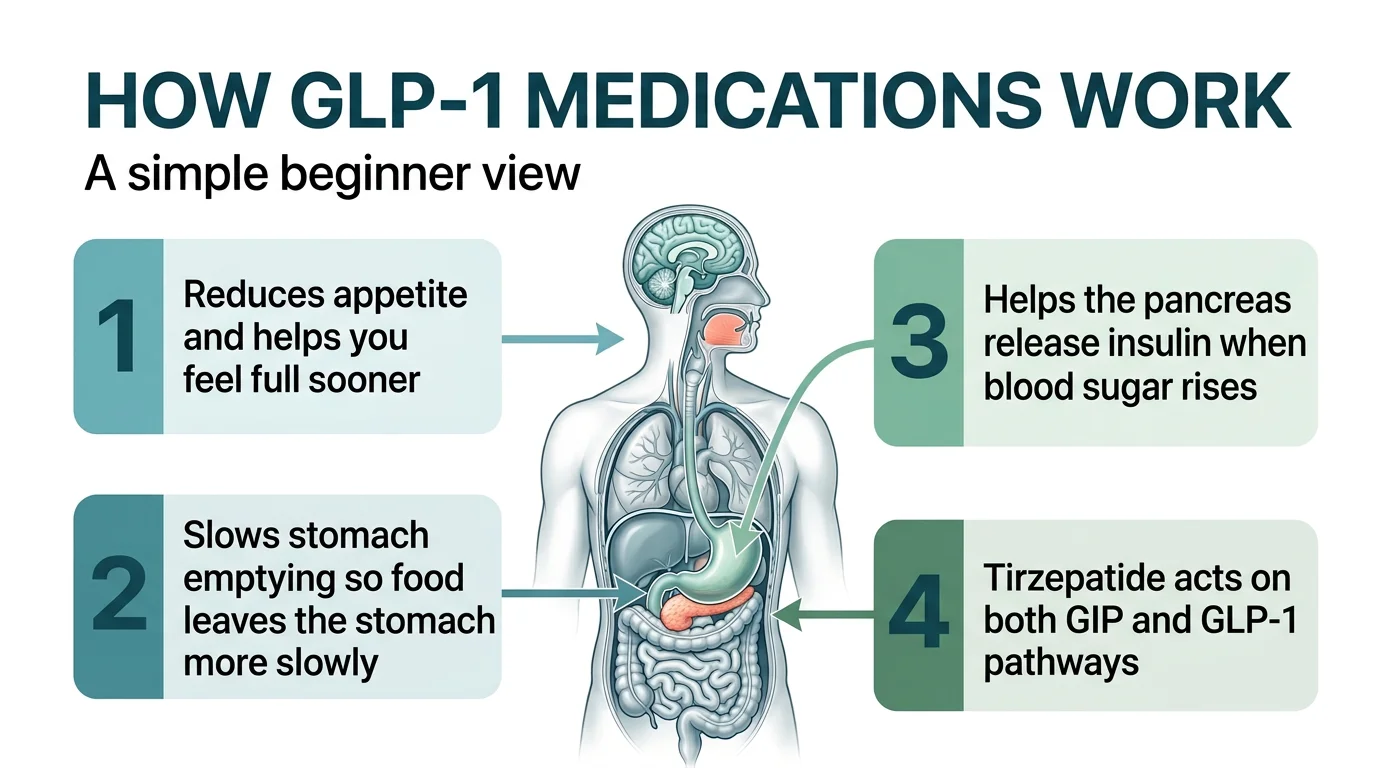
1. Quiet the hunger
GLP-1 medications act on receptors in your brain that regulate appetite. Many people describe this as the disappearance of "food noise" — that constant background hum of thinking about food. The medication doesn't make food disgusting. It turns down the volume on the urge to eat.
2. Slow your stomach
GLP-1 medications delay gastric emptying, which means food stays in your stomach longer. You feel full sooner and stay full longer after smaller meals. This is also why some common side effects (nausea, bloating) happen — your digestive system is literally moving at a different pace.
3. Improve blood sugar
GLP-1 medications help your pancreas release insulin more effectively when blood sugar rises after a meal and reduce the amount of sugar your liver dumps into your bloodstream. This is why GLP-1s were originally developed for type 2 diabetes.
Tirzepatide (Mounjaro, Zepbound) goes a step further. It works on both GLP-1 and GIP receptors — a dual mechanism that appears to produce stronger weight loss and metabolic effects than GLP-1 alone. This is why tirzepatide has shown higher average weight loss in trials.[2]
The result of all three mechanisms working together: you eat less without feeling deprived, your body processes food differently, and your metabolic health improves. It's not a magic pill or injection — but it addresses the biology of weight gain in ways that willpower and calorie counting alone often can't.
The Main GLP-1 Medications Beginners Ask About
This is the section we wish every other beginner guide included. Most pages describe one or two medications. We're putting the ones you'll most commonly encounter in one place so you can see the landscape.
GLP-1 Beginner Comparison Table
| Medication | Drug | FDA-Approved For | Format | Frequency | Avg. Weight Loss | Typical Beginner Concern |
|---|---|---|---|---|---|---|
| Wegovy (injection) | Semaglutide | Weight management, CV risk reduction, other indications | Weekly injection | Once/week | ~15% (STEP 1) | Strongest overall evidence base, including heart benefits |
| Wegovy (pill) | Semaglutide (oral) | Weight management, CV risk reduction | Daily pill | Once/day | ~13.6% (OASIS 4) | People who prefer pills over needles |
| Zepbound | Tirzepatide | Weight management, obstructive sleep apnea | Weekly injection | Once/week | ~22.5% at highest dose (SURMOUNT-1) | Highest average weight loss in trials |
| Ozempic | Semaglutide | Type 2 diabetes, CV risk reduction, CKD risk reduction | Weekly injection | Once/week | Not FDA-approved for weight management | People with diabetes who also want weight loss (off-label) |
| Mounjaro | Tirzepatide | Type 2 diabetes | Weekly injection | Once/week | Not FDA-approved for weight management | People with diabetes + insulin resistance (off-label) |
| Saxenda | Liraglutide | Weight management | Daily injection | Once/day | ~8% | Generic now available — most affordable FDA-approved option |
Important notes:
- Ozempic and Mounjaro are FDA-approved for diabetes, not weight loss. They are frequently prescribed off-label for weight management.
- Weight loss percentages are averages from clinical trials under controlled conditions. Individual results vary significantly.
- A generic version of liraglutide (from Teva) became available in August 2025 — it is currently the only marketed generic GLP-1 indicated for weight loss in the U.S.[12]
Do You Qualify for GLP-1 Medication?
Here's what the FDA guidelines say, translated into plain language.
You likely qualify if:
- Your BMI is 30 or higher (classified as obesity), OR
- Your BMI is 27 or higher AND you have at least one weight-related health condition — such as high blood pressure, type 2 diabetes or prediabetes, high cholesterol, or obstructive sleep apnea
What a clinician will also evaluate:
- Your full medical history and current medications
- Family history (particularly thyroid cancer)
- Previous weight loss attempts
- Whether you're pregnant, breastfeeding, or planning to become pregnant
The two hard stops (FDA contraindications):
- Personal or family history of medullary thyroid carcinoma (MTC) or Multiple Endocrine Neoplasia syndrome type 2 (MEN2)
- Known severe allergic reaction to the specific medication or its ingredients
Everything else — history of pancreatitis, kidney issues, gallbladder problems — falls under warnings and precautions that require a conversation with your provider, not an automatic "no." We cover this in detail in our GLP-1 contraindications guide.
Not sure where you stand? Most people fall somewhere in the "probably eligible but need a provider to confirm" zone. A good clinician will evaluate your full picture — not just your weight.
Not sure if a GLP-1 is right for you? Our free eligibility quiz takes about 60 seconds. Answer a few questions about your health, goals, and budget — and we'll show you which GLP-1 options fit your situation, including what you'd likely pay.
Take the Free Eligibility QuizWhich GLP-1 Option Makes the Most Sense for Beginners?
There is no universal "best" GLP-1. There's a best fit for your situation. Here's how to think about it.
If maximum weight loss is your top priority →
Look at tirzepatide (Zepbound). Clinical trials showed the highest average weight loss — up to 22.5% of body weight at the highest dose over 72 weeks.[2] It's a weekly injection.
If you have heart disease risk or history →
Semaglutide (Wegovy) has the most robust cardiovascular evidence. The SELECT trial — one of the largest CV outcomes trials ever conducted with over 17,000 participants — showed it reduces major adverse cardiovascular events in adults with obesity or overweight and established heart disease.[9]
If you have sleep apnea →
Zepbound (tirzepatide) is the first pharmacologic therapy FDA-approved for moderate-to-severe obstructive sleep apnea in adults with obesity.[6] See our full sleep apnea guide.
If you don't want needles →
The Wegovy pill (oral semaglutide 25mg) launched in January 2026.[4] It's the first FDA-approved oral GLP-1 for weight management. Clinical data shows similar weight loss to the injection.[11] The trade-off: you take it daily (not weekly), on an empty stomach, with minimal water, and wait 30 minutes before eating or drinking anything else. Eli Lilly's oral option (orforglipron) is expected to receive an FDA decision later in 2026 — and notably, it won't require those fasting restrictions.
If cost is your biggest barrier →
A few paths worth exploring. The Wegovy pill starts at $149/month for the 1.5 mg dose through self-pay.[13] Generic liraglutide (Teva's version of Saxenda) is currently the only marketed generic GLP-1 indicated for weight loss in the U.S.[12] Verified telehealth programs are another path many beginners find accessible. Among the programs we've reviewed, MEDVi stands out for a clear entry price ($179 first month), 24/7 support, and a high volume of verified third-party reviews (TrustPilot 4.5/5, 8,400+ reviews as of early 2026).
If you have diabetes AND want to lose weight →
Talk to your endocrinologist about Ozempic or Mounjaro. Both address blood sugar management and produce significant weight loss — potentially covering both needs with a single medication.
The bottom line for most beginners: Start with a conversation with a licensed clinician who can evaluate your specific health profile, goals, and budget. The "best" GLP-1 is the one you can access, afford, tolerate, and stay on long enough to see results.
How to Start a GLP-1 Safely (Step by Step)
Once you've decided you want to explore GLP-1 medication, here's the practical path from "interested" to "first dose."
Step 1: Choose your prescribing path
You have three main options:
Your primary care doctor or specialist. If you already have a doctor you trust, this is often the simplest starting point. They know your full medical history. The downside: some PCPs aren't experienced with GLP-1 prescribing, wait times can be long, and not every clinic stocks or coordinates these medications efficiently.
An obesity medicine specialist or endocrinologist. Ideal if you have complex health conditions. These providers manage GLP-1 medications daily and can navigate insurance prior authorizations. The downside: long wait times for new patient appointments in many areas.
A telehealth GLP-1 program. This is how many beginners start — especially when local provider access is limited or they're paying out of pocket. A reputable telehealth program includes a licensed physician consultation, a health assessment, an ongoing care plan, and medication shipped to your door. Full comparison: Best GLP-1 Online Programs (2026).
Step 2: Get evaluated
Whether in-person or online, a good initial evaluation should cover:
- Your weight history and previous weight loss attempts
- Current medications and health conditions
- Blood pressure, relevant lab work
- A discussion of which GLP-1 medication fits your goals, health profile, and budget
- Clear information about side effects, titration schedule, and what to expect
Questions to ask before saying yes:
- • Which pharmacy fills the prescription, and is it licensed?
- • What's my total monthly cost at each dose level?
- • What happens if I experience side effects — who do I contact?
- • Is there a cancellation policy if this isn't working for me?
- • Do you provide nutrition guidance or just the medication?
Step 3: Handle the money part
- If you have insurance: Call the number on your card and ask specifically about the medication your provider recommends. Ask about prior authorization requirements. Be prepared for potential denials and appeals.
- If you're paying cash: Compare manufacturer self-pay programs (NovoCare, LillyDirect), TrumpRx pricing, and telehealth providers. Get the full monthly cost at each dose level, not just the introductory price.
- If you're on Medicare: A Medicare GLP-1 Bridge demonstration launches in July 2026, giving eligible Part D beneficiaries access to certain GLP-1 medications at $50/month. The longer-term BALANCE Medicare Part D model has been delayed — check cms.gov for the current launch date. Medicaid access through BALANCE can begin as early as May 2026 in participating states.[10]
Step 4: Start your first dose
- Injectable: Store properly (refrigerate before first use). Pick a consistent day and time each week. Inject into fatty tissue — belly, thigh, or upper arm.
- Pill: Take first thing in the morning on an empty stomach with no more than 4 ounces of plain water. Wait at least 30 minutes before eating, drinking, or taking other medications.[4]
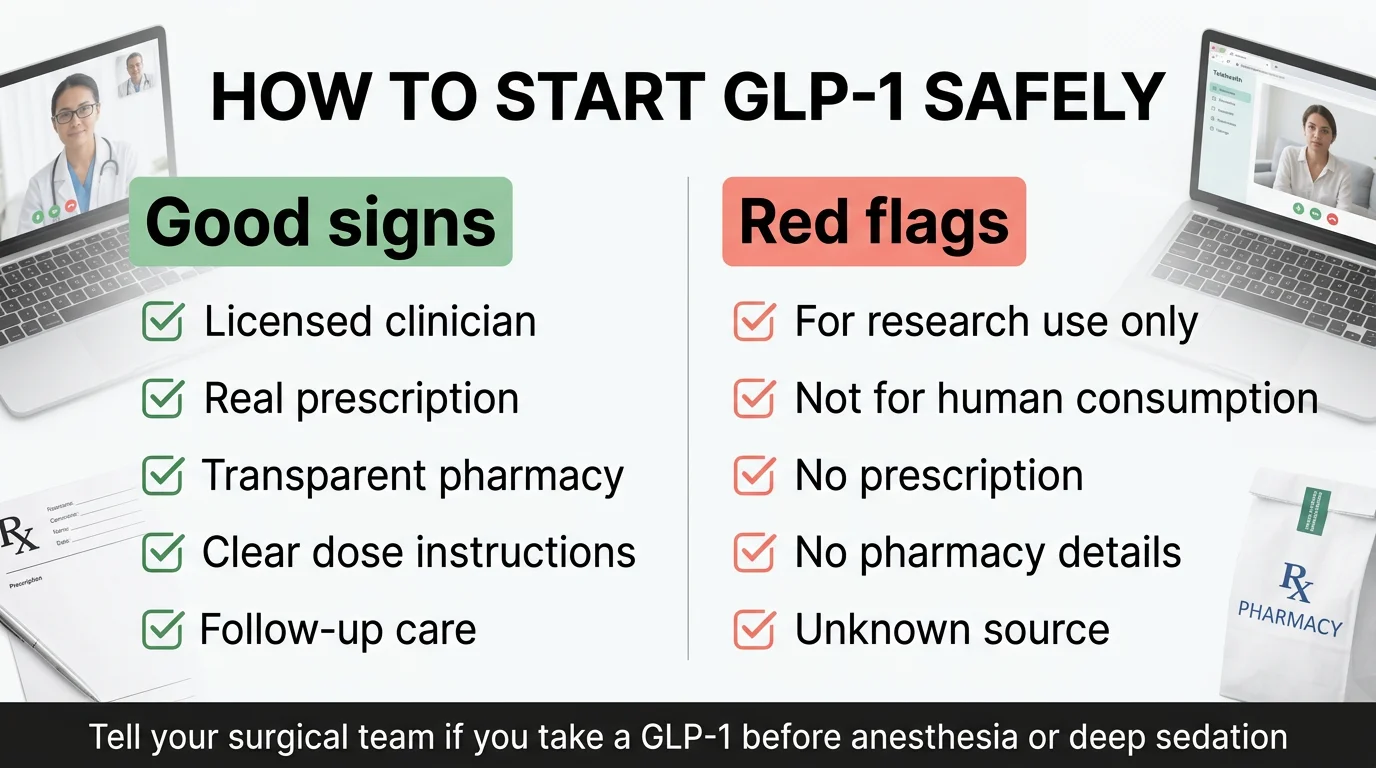
- Important — tell your surgical/dental team: If you have any upcoming procedure requiring anesthesia or sedation, tell your surgeon, anesthesiologist, dentist, or endoscopy team that you take a GLP-1 medication. Current Wegovy and Zepbound labeling warns about rare reports of pulmonary aspiration during general anesthesia or deep sedation.[3][6]
- Start a simple tracker: weight, how you feel, what you ate, any side effects. This data is incredibly useful at your first follow-up.
Step 5: Plan your follow-ups
Don't just start and disappear. Schedule check-ins at roughly 4 weeks, 8 weeks, and 12 weeks. Your provider needs to evaluate side effects, adjust dosing, and make sure the medication is working safely for you. Ongoing care is what separates good outcomes from mediocre ones.
Red flags to avoid:
- Any seller offering GLP-1s without a medical consultation or prescription
- Products labeled "for research use only" or "not for human consumption" — the FDA has explicitly warned about these[14]
- Providers who can't tell you which pharmacy fills your medication
- Unusually low prices with no clear information about source, pharmacy licensing, or clinical oversight
“Lost 16 lbs in 10 weeks — no side effects. Down two sizes. I wish I’d started sooner.”
— Verified MEDVi patient on ConsumerAffairs ★★★★★
What to Expect in Your First 30 Days on GLP-1 (Week by Week)
This is the section we wish someone had given us before starting. The first month is mostly about adjustment — not dramatic results. Here's what actually happens.
Week 1: Learning the new normal
You're on the lowest starter dose. Some people notice a clear appetite reduction within the first few days. Others feel almost nothing — and that's fine. The starter dose is intentionally low.
If you're injecting, the first time is the hardest. The needle is small — much smaller than what you'd picture. Most people say it barely stings. Pick a spot (belly is most common, a few inches from your navel), pinch the skin, and inject. It gets routine fast.
If you're on the pill, your new morning ritual starts now: wake up, take the tablet with a small sip of water, set a 30-minute timer, then go about your morning before eating or drinking anything else.
What to do: Eat smaller meals. Focus on protein. Stay hydrated. Don't try to power through a full plate of food. Your body will tell you when it's had enough — listen to it.
Week 2: The adjustment window
GI side effects are most common early and after dose increases — nausea, in particular, tends to peak in the first few days after an injection and then fade. By week two, many people describe the appetite reduction as noticeable — "I just... forgot to eat lunch." That's the medication working on your brain's hunger signaling.
Common mistake here: Not eating enough. Your body still needs fuel, especially protein. Even if food doesn't sound appealing, eat something. Small, protein-rich meals. Greek yogurt. Eggs. A protein shake when solid food feels like too much.
Weeks 3–4: Finding your rhythm
Side effects usually start to ease. Your eating patterns are settling into something new. You're learning what your body tolerates and what it doesn't (greasy food is almost universally the first thing to go).
At the end of month one, check in with your provider. Discuss how you're tolerating the medication, review any side effects, and confirm the plan for your next dose increase. Most protocols increase the dose at 4-week intervals, but your provider may adjust based on how you're responding.
The bigger picture: dose titration
Here's something most beginners don't realize until they're in it. GLP-1 medications use a gradual dose-escalation schedule. You start low and step up every 4 or more weeks until you reach the target maintenance dose. For semaglutide, this process takes about 16–20 weeks. For tirzepatide, it's similar.[3][6]
What we'd tell a friend starting their first month: Track everything, drink more water than you think you need, prioritize protein at every meal, be patient with the dose schedule, and don't compare your week-two results to someone else's month-six transformation on social media.
What to Eat on GLP-1 Medication (and What to Avoid)
Your appetite is going to change. What you eat with that smaller appetite matters more than ever — because when you're eating less overall, every bite needs to count.

The core framework: protein first, always
This is the single most important nutrition rule on a GLP-1. When your stomach capacity shrinks, whatever you eat first is what your body gets the most of. Make it protein.
A common starting strategy is prioritizing protein at each meal — many providers and dietitians suggest aiming for roughly 25–30 grams per meal as a starting point. Exact protein, fluid, and activity needs vary by body size, age, kidney function, medications, and goals — so work with your provider or a registered dietitian to dial in the right targets for you.[15]
Practical plate structure:
- Eat protein first (before touching anything else on the plate)
- Then non-starchy vegetables
- Then complex carbs if you still have room
Foods that work well
- • Eggs — versatile, high-protein, gentle on the stomach
- • Greek yogurt and cottage cheese
- • Lean chicken, turkey, fish (baked or grilled)
- • Soups and broths — hydrating, easy to tolerate
- • Oatmeal — fiber-rich, gentle, filling
- • Berries, bananas — easy to eat, provide fiber
- • Beans and lentils — excellent protein + fiber
- • Whole grain toast, quinoa, sweet potatoes
Foods that cause problems
- • Greasy/fried foods — #1 nausea trigger
- • Very large meals — your stomach can't handle it
- • Sugary drinks and sodas — empty calories, bloating
- • Highly processed snacks — low nutrition density
- • Alcohol — tolerance decreases on GLP-1s
Key habits that make a real difference
Eat slowly. 20–30 minutes per meal, minimum. On GLP-1 medication, the difference between "satisfied" and "uncomfortably stuffed" can be just three or four more bites.
Don't skip meals even when you're not hungry. Your body still needs nutrients. Try smaller portions more frequently — 4–5 mini-meals instead of three big ones.
Consider a daily multivitamin. When you're eating significantly less food, you're also getting fewer vitamins and minerals.
Sample beginner day:
- Breakfast: 2 scrambled eggs with spinach, 1 slice whole-grain toast
- Snack: ¾ cup Greek yogurt with a handful of berries
- Lunch: 4 oz grilled chicken over mixed greens with quinoa
- Snack: String cheese and an apple
- Dinner: 5 oz baked salmon with steamed broccoli and ½ cup brown rice
This is an example, not a universal prescription — adjust based on your appetite and what your provider recommends.
How to Protect Your Muscle, Energy, and Nutrition While Eating Less
Muscle loss is one of the most discussed concerns with rapid weight loss — and it's a legitimate one. When you lose weight quickly, some of that loss comes from lean muscle, not just fat. The good news: you can minimize muscle loss significantly with the right habits.
1
Protein intake
Prioritize protein at every meal. This is the single most impactful thing you can do to preserve lean mass.[15]
2
Resistance training
2–3 sessions per week of basic strength training. Even 20–25 minutes per session counts.[16]
3
Walking
Regular daily walking helps with weight management and blood sugar regulation. Walking after meals can also reduce post-meal nausea.
A realistic minimum for beginners:
- • Strength training: 2–3 times per week, 20–25 minutes
- • Daily walking: build gradually toward a level that feels sustainable
- • Protein: prioritize it at every meal
- • Hydration: stay ahead of thirst throughout the day
- • Sleep: 7–9 hours (recovery matters more when you're eating less)
Don't overdo it in month one. Your caloric intake is reduced and your body is adjusting. Start moderate. Increase intensity gradually.
Side Effects: What's Normal, What's Not, and What Actually Helps
Side effects are the most common reason people stop GLP-1 medications — but most of them are manageable once you know what to expect and how to respond.
Common side effects (usually temporary, usually improve)
| Side Effect | What It Feels Like | What Often Helps |
|---|---|---|
| Nausea | Queasiness, especially after eating or in the morning | Smaller meals, bland foods, eat slowly, avoid greasy food, ginger tea |
| Constipation | Less frequent bowel movements, harder stools | More water, fiber-rich foods, daily walking, stool softener if needed |
| Diarrhea | Loose or frequent stools | Avoid high-fat meals, stay hydrated, usually resolves within days |
| Bloating/fullness | Feeling overly full even after small amounts | Eat less per sitting, eat more slowly |
| Heartburn/reflux | Burning sensation in chest or throat | Avoid eating close to bedtime, sleep slightly elevated |
| Fatigue | Low energy, especially first 1–2 weeks | Often improves as your body adjusts; ensure adequate hydration and nutrition |
| Injection site reactions | Mild redness or tenderness | Rotate injection sites, let medication reach room temperature |
Timing note: Side effects are most common during the first few weeks on a new dose. Every time your dose increases, you may experience a brief return of GI symptoms. This typically eases within 1–2 weeks.[3][6]
Less common but worth knowing
- Hair thinning: Related to rapid weight loss itself, not the medication directly. Usually temporary. Adequate protein and nutrition help.
- "Ozempic face": Facial volume loss that happens with significant weight loss. Not unique to GLP-1s — it happens with any major weight loss.
- Gallbladder issues: Weight loss of any kind increases gallbladder risk. Watch for sudden severe abdominal pain, especially in the upper right area.
- Very low appetite: Sometimes appetite drops so much that people struggle to eat at all. This deserves a conversation with your provider.
When to contact your clinician
- • Nausea or vomiting that doesn't improve after a few days
- • Constipation that doesn't respond to hydration, fiber, and movement
- • Side effects that significantly impact daily life
- • Any concern that feels "off" to you — trust your instincts
When to seek urgent medical attention
- • Severe, persistent abdominal pain (possible pancreatitis)
- • Repeated vomiting or inability to keep fluids down
- • Yellowing of skin or eyes
- • Difficulty breathing, facial swelling, hives
- • Severe low blood sugar symptoms
The key message: side effects are common, usually mild to moderate, and typically temporary. Most people who stick through the first few weeks of each dose adjustment find that things settle down. Work with your provider to manage them rather than quitting before it has a chance to work.
Related: Tirzepatide Side Effects Guide · Mounjaro Side Effects
Serious Risks and Who Should NOT Take GLP-1 Medications
Honesty about risks is how trust gets built, so here's the full picture.
Absolute contraindications (hard stops):
- Personal or family history of medullary thyroid carcinoma (MTC) or Multiple Endocrine Neoplasia syndrome type 2 (MEN2). All GLP-1 medications carry a boxed warning about thyroid C-cell tumors observed in rodent studies.
- Known severe hypersensitivity to the medication or its components.
Conditions requiring careful provider discussion:
- History of pancreatitis. GLP-1s carry a warning, but past pancreatitis doesn't automatically rule you out. Your provider will weigh the risks.
- Kidney disease. GLP-1 medications can affect hydration, and dehydration can worsen kidney function. Close monitoring is needed.
- Gallbladder disease. Rapid weight loss increases gallstone risk. This is a monitoring issue, not necessarily a contraindication.
- History of eating disorders. The appetite-suppressing effects require careful evaluation in this context.
- Pregnancy and planning for pregnancy. GLP-1 medications are generally not recommended during pregnancy. Prescribing information typically advises stopping at least 2 months before a planned pregnancy (Wegovy) or when pregnancy is recognized (Zepbound).[3][6]
Medication interactions to know about:
- If you take insulin or a sulfonylurea, your clinician may need to lower that dose to reduce hypoglycemia risk.
- Tirzepatide can affect absorption of oral medications. Its label advises people using oral hormonal contraceptives to switch to a non-oral method or add a barrier method for 4 weeks after starting and after each dose increase.[6]
- Wegovy tablets can affect oral-medication exposure. The label notes increased levothyroxine exposure and advises monitoring for oral medications that require close dosing control.[4]
Surgery and anesthesia: Tell any surgical, anesthesia, dental, or endoscopy team that you take a GLP-1 medication. Current labeling warns about rare reports of pulmonary aspiration during general anesthesia or deep sedation because GLP-1s delay gastric emptying.[3][6]
Mental health — an update: As of January 2026, the FDA completed a comprehensive review — including a meta-analysis of 91 placebo-controlled trials with over 107,000 patients — and found no increased risk of suicidal thoughts or behaviors with GLP-1 receptor agonists. The FDA has requested that manufacturers remove the suicidal ideation and behavior warning from labels that currently include it.[17] Patients should still tell their clinician about new or worsening depression, suicidal thoughts, or any unusual changes in mood or behavior.
What about compounded GLP-1 products?
The regulatory landscape for compounded GLP-1 medications has tightened significantly. The FDA has said both the semaglutide injection shortage and tirzepatide shortage are resolved, and the agency has stated it may take action against mass-marketed non-FDA-approved compounded GLP-1 products.[14] A 503A pharmacy is state-licensed; a 503B outsourcing facility is FDA-registered. Those labels alone do not make a compounded product equivalent to an FDA-approved drug. Avoid products sold as "for research use only," "not for human consumption," or made with semaglutide salt forms (such as semaglutide sodium or acetate).
If you're considering a compounded option through a telehealth program, verify that the provider is transparent about which pharmacy fills the medication and whether that pharmacy is properly licensed and inspected.
For a deep dive: GLP-1 Contraindications Guide · Is Compounded Semaglutide Safe?
How Much Do GLP-1 Medications Cost in 2026? (Every Path Explained)
Let's talk money — because cost is the #1 barrier for most people considering a GLP-1, and the pricing landscape in 2026 is more complex (and more accessible) than most guides explain.
Note: All prices below reflect manufacturer self-pay program terms as of March 2026. Offers have eligibility requirements, may change without notice, and actual out-of-pocket costs vary.
Path 1: Brand-name with insurance
If your insurance covers GLP-1 medications for weight loss, you may pay as little as $25/month with a commercial savings card for Wegovy or Zepbound.[13][6] Reality check: many employer plans exclude weight-loss medications. Even plans that do cover them often require prior authorization, specific BMI thresholds, or step therapy.
Path 2: Brand-name without insurance (manufacturer self-pay)
| Medication | Self-Pay Pricing (March 2026) |
|---|---|
| Wegovy pill | 1.5 mg and 4 mg: $149/mo (4 mg pricing available through August 31, 2026, then $199/mo) |
| Wegovy injection | New patients: $199/mo for 0.25–0.5 mg (intro, up to 2 fills through December 31, 2026). After: $349/mo |
| Zepbound | 2.5 mg: $299/mo · 5 mg: $399/mo · 7.5–15 mg: $449/mo (Self Pay Journey Program) |
| Ozempic (NovoCare) | New patients: $199/mo for 0.25–0.5 mg (intro, up to 2 fills), then $349/mo up to 1 mg, $499/mo for 2 mg |
Some major retailers (Costco, Walmart) have partnered with manufacturers for similar cash-pay pricing.
Path 3: TrumpRx (federal pricing initiative)
TrumpRx is a federal platform that connects patients to manufacturer discount pricing. It doesn't sell medications directly — it directs you to the drugmakers' discount programs. The platform has announced expected pricing around $350/month for injectable GLP-1s and $149/month for pill starting doses, though exact availability and terms continue to evolve.
Path 4: Medicare and Medicaid (expanding 2026–2027)
Medicare: A Medicare GLP-1 Bridge demonstration begins in July 2026, operating nationwide and outside the normal Part D structure. Eligible Part D beneficiaries will pay $50/month for covered GLP-1 medications. The Bridge has been extended through December 2027 after CMS delayed BALANCE Part D implementation. Check cms.gov for the BALANCE launch date.[10]
Medicaid: Access through the BALANCE model can begin as early as May 2026 in states that opt to participate.[10]
Path 5: Telehealth programs with compounded medications
Verified telehealth providers offer GLP-1 programs ranging from about $149 to $399 per month, typically including the physician consultation, care plan, and medication. MEDVi, for example, starts at $179 for the first month with physician oversight, ongoing check-ins, and 24/7 support per their site.
These programs typically provide compounded GLP-1 medications. Compounded products are not FDA-approved as finished products, and the FDA regulatory landscape is tightening — see the risks section for critical details on verifying pharmacy credentials.
Path 6: Generic options
Generic liraglutide (Teva's version of Saxenda) became available in August 2025.[12] It is currently the only marketed generic GLP-1 indicated for weight loss in the U.S. Generics for semaglutide and tirzepatide are still years away.
HSA/FSA
GLP-1 medications are generally HSA and FSA eligible when prescribed by a physician. Keep itemized receipts. Confirm with your specific plan administrator.
Bottom line on cost: GLP-1 medications are more accessible in 2026 than they've ever been, but they're still not cheap. The "right" path depends on your insurance situation, budget, and comfort level with different medication sources. Compare at least 2–3 options before committing, and always get the full monthly cost at each dose level — not just the introductory price.
Related: Can You Use HSA for GLP-1? · Cheapest Tirzepatide Online
Navigating GLP-1 costs can be confusing. Our quiz helps you figure out the most affordable path based on your specific coverage and budget.
Check Your Eligibility — Free, 60 SecondsPill vs. Injection: Which Is Better for Beginners?
This is a real question now — not a hypothetical. With the Wegovy pill on the market and another oral option (orforglipron from Eli Lilly) expected in 2026, beginners genuinely have to decide.
| Factor | Weekly Injection | Daily Pill |
|---|---|---|
| Frequency | Once per week | Once per day |
| Needle involved? | Yes (small, subcutaneous) | No |
| Fasting required? | No | Yes — empty stomach, 4 oz water, 30-min wait |
| Refrigeration needed? | Usually (before first use) | No |
| Average weight loss | ~15% (Wegovy 2.4mg, STEP 1) | ~13.6% (oral semaglutide 25mg, OASIS 4) |
| Side effects | GI effects common during titration | Similar profile; may intensify initially |
| Best for | People comfortable with injections, want once-weekly simplicity | People who prefer no needles, travel frequently, want lower entry cost |
The weight-loss difference between pill and injection is relatively modest in clinical data. The bigger differentiator for most people comes down to lifestyle: do you prefer a once-weekly shot you don't think about for 7 days, or a daily pill that requires a specific morning routine?
For travelers, the pill has a practical edge — no refrigeration, no carrying needles through airport security. For people who struggle with daily medication adherence, the weekly injection may be simpler.
Something to watch: Eli Lilly's orforglipron, if approved, may change this comparison. Early trial data shows it doesn't require the fasting restrictions that the Wegovy pill does — which could make the daily pill option significantly more convenient.
What Happens If You Stop Taking GLP-1 Medication?
We'll give it to you straight: if you stop a GLP-1 medication without a plan, weight regain is common. Extension data from the STEP 1 trial showed that participants regained roughly two-thirds of their lost weight within a year after stopping semaglutide.
This isn't a failure of the medication or a failure of willpower. It reflects the biological reality that obesity is a chronic condition — the same way high blood pressure doesn't "cure" itself when you stop blood pressure medication.
What this means practically:
- Discuss any plan to stop or taper with your provider. Don't just quit on your own.
- The habits you build while on the medication matter enormously. Nutrition, exercise, sleep — these are what give you the best chance of maintaining results.
- Some people stay on GLP-1s long-term. Some transition to lower maintenance doses. Some taper off after reaching their goals. All are valid paths.
- Oral formulations may make long-term low-dose maintenance more practical and affordable for some patients.
The emerging consensus among obesity medicine specialists is that GLP-1 therapy is most effective when treated as an ongoing tool rather than a short-term fix. Think of it less like an antibiotic (take it, stop, done) and more like managing a chronic condition (ongoing, with adjustments over time).
Can You Boost GLP-1 Naturally Without Medication?
Yes — to a degree. Your body produces GLP-1 on its own, and certain foods and habits can support that natural production.
Foods that stimulate GLP-1
- • High-protein foods (eggs, lean meats, legumes, Greek yogurt)
- • Fiber-rich foods (oats, beans, lentils, vegetables, fruits)
- • Healthy fats (olive oil, avocado, nuts, fatty fish)
- • Fermented foods (may support gut bacteria that influence GLP-1)
Lifestyle factors
- • Regular physical activity
- • Adequate sleep
- • Stress management
Honest framing: Natural GLP-1 stimulation is real, and these are healthy habits everyone should pursue. But the effect is modest compared to prescription GLP-1 medications. Natural food-based GLP-1 production is measured in picomoles and lasts minutes. Prescription GLP-1s produce sustained pharmacological levels over hours or days. They're operating on completely different scales.
These habits are excellent complements to GLP-1 therapy — and they're the foundation that helps maintain results. But they are not a replacement for prescription treatment in people who meet the clinical criteria for medication.
One warning: Be skeptical of over-the-counter "GLP-1 booster" supplements. The FDA and medical experts have flagged that products marketed as "natural GLP-1 boosters" lack clinical evidence, aren't regulated as medications, and may carry risks — especially when combined with prescription GLP-1s.
The Biggest Beginner Mistakes to Avoid
After reviewing clinical guidance, provider recommendations, and thousands of real patient experiences, these are the patterns we see trip people up most often.
Expecting dramatic results in week one.
You're on the starter dose. The medication hasn't ramped up yet. Real momentum builds around months 3–6. Setting realistic first-month expectations prevents discouragement.
Not eating enough protein.
This is the most common nutrition mistake, and it's the most consequential. Inadequate protein during rapid weight loss leads to muscle loss, fatigue, hair thinning, and poorer long-term outcomes.
Ignoring hydration.
Constipation, headaches, fatigue, and even nausea can all be worsened by dehydration. Water needs increase when your eating patterns change.
Chasing the cheapest option without verifying safety.
The FDA has warned about unapproved GLP-1 products sold online. If a price seems too good to be true and the seller can't tell you which licensed pharmacy fills the medication, walk away.
No follow-up care.
Starting a GLP-1 without ongoing provider support is like flying without instruments. Dose adjustments, side effect management, and health monitoring all require regular check-ins.
Comparing your results to social media.
The six-month transformation photos you see online are often the most extreme results. Average weight loss is 15–22% of body weight over a year — that's exceptional by medical standards, but it happens gradually.
Self-adjusting your dose.
Don't increase your dose faster than your provider recommends. Don't decrease it without guidance. The titration schedule exists for a reason. Talk to your clinician before making any changes.
Having no food plan.
Starting a GLP-1 without thinking about nutrition is one of the most common regrets. Your appetite will change, and you need to be ready to make those smaller meals count.
What Should You Do Next?
You've just read more about GLP-1 medications than most people learn in months of scattered searching. Here's how to turn that knowledge into action.
If you're still learning →
Bookmark this page. Come back when you're ready. Explore our GLP-1 contraindications guide if safety is your top concern, or our provider comparison if you want to see specific program options.
If you think you might qualify →
The fastest next step is a 60-second eligibility check. Our free matching quiz considers your BMI range, health conditions, budget, and format preference to show you which GLP-1 paths fit your situation. No sales call, no credit card.
If you're ready to start →
Compare 2–3 providers before committing. Check insurance coverage first. If paying out of pocket, MEDVi offers one of the more straightforward entry points for beginners — starting at $179/month with physician oversight and 24/7 support. For a broader comparison, see our full Best GLP-1 Online Programs guide.
Still not sure which GLP-1 program is right for you?
Take our free 60-second matching quiz. We'll ask a few quick questions about your health profile, goals, and budget — then show you the GLP-1 options that actually fit your situation. No commitment. No credit card. Just clarity.
Take the Free QuizFrequently Asked Questions
Is GLP-1 the same thing as Ozempic?
No. GLP-1 is the category — it refers to a class of medications that mimic the GLP-1 hormone. Ozempic is one specific GLP-1 medication (semaglutide) that's FDA-approved for type 2 diabetes. Wegovy contains the same active drug but is approved for weight loss. Mounjaro, Zepbound, and Saxenda are other GLP-1-related medications with different active ingredients and approvals.
Which GLP-1 is best for weight loss?
Tirzepatide (Zepbound) has shown the highest average weight loss in clinical trials — around 22.5% of body weight at the highest dose. Semaglutide (Wegovy) has the broadest evidence base, including cardiovascular benefits. The "best" choice depends on your health profile, insurance, and preferences.
Can I get a GLP-1 prescription online?
Yes. Several telehealth platforms offer GLP-1 prescriptions through licensed physicians. You typically complete a health assessment, consult with a provider, and receive medication by mail. Verify the platform uses licensed physicians and pharmacies before proceeding.
Are GLP-1 pills available now?
Yes. The Wegovy pill (oral semaglutide 25mg) received FDA approval in December 2025 and became available in January 2026. It's the first oral GLP-1 approved for weight management. Another oral option, orforglipron from Eli Lilly, is expected to receive an FDA decision later in 2026.
What should I expect in the first week?
On the starter dose, many people notice mildly reduced appetite, possible light nausea, and feeling full sooner than usual. Some people feel very little at all in week one — and that's normal. Side effects tend to increase with dose escalations.
Do I qualify if my BMI is under 30?
Possibly. The FDA-approved threshold is BMI 27+ with at least one weight-related health condition (high blood pressure, type 2 diabetes, high cholesterol, sleep apnea, etc.). If your BMI is between 27 and 30, talk to a provider about whether you meet eligibility criteria.
Can I take a GLP-1 if I don't have diabetes?
Yes. Wegovy, Zepbound, and Saxenda are FDA-approved specifically for weight management — no diabetes diagnosis required.
How much weight do people usually lose?
Clinical trial averages: ~15% of body weight with semaglutide (Wegovy) and up to ~22.5% with tirzepatide (Zepbound) at the highest dose over 12–16 months. Real-world results are often somewhat lower due to differences in adherence, dosing, and follow-up. Individual results vary significantly.
Do I need to stay on GLP-1 forever?
Not necessarily — but discontinuation often leads to weight regain. Some people stay on long-term, some transition to lower maintenance doses, and some taper off after reaching goals. This is a decision to make with your provider, not a one-size-fits-all answer.
What happens if I miss a dose?
Wegovy injection: if your next scheduled dose is more than 48 hours away, take the missed dose as soon as possible. Wegovy pill: skip the missed dose and take the next dose the following day. Ozempic: take it within 5 days of the missed dose. Zepbound/Mounjaro: take it within 4 days (96 hours). Do not take 2 doses within 72 hours of each other.
Are compounded GLP-1s safe?
Compounded GLP-1 medications are not FDA-approved as finished products. The FDA has said the semaglutide injection and tirzepatide shortages are resolved and has indicated it may act against mass-marketed non-FDA-approved compounded versions. If you use a compounded option, verify the pharmacy is a properly licensed 503A or 503B facility. Avoid any product sold without a prescription, labeled "for research use only," or from an unverifiable source.
Is nausea normal?
Yes. Nausea is the most commonly reported side effect, particularly during dose initiation and escalation. It usually improves within 1–2 weeks as your body adjusts to each new dose level. Eating smaller meals, avoiding greasy food, and eating slowly all help.
Can GLP-1 medications cause muscle loss?
Rapid weight loss from any cause can involve some muscle loss. This isn't unique to GLP-1s. The best protection: adequate protein intake and resistance training (2–3 times per week). These two habits make a significant difference in preserving lean mass.
Can I drink alcohol on a GLP-1?
Alcohol isn't contraindicated, but be cautious. Most people report reduced alcohol tolerance — effects hit faster and feel stronger. If you drink, start with less than you normally would, stay hydrated, and pay attention to how your body responds.
Can I take a GLP-1 if I'm trying to get pregnant?
GLP-1 medications are generally not recommended during pregnancy. Prescribing information advises stopping Wegovy at least 2 months before a planned pregnancy and discontinuing Zepbound when pregnancy is recognized. Tirzepatide (Zepbound) can affect oral contraceptive absorption — talk to your provider about contraception methods during treatment and after dose increases.
Do I need lab work before starting?
Many providers recommend baseline labs (blood panel, kidney function, thyroid, A1C) — though requirements vary. At minimum, expect a thorough health history review.
What is the cheapest safe way to get a GLP-1?
Generic liraglutide (Teva's version of Saxenda, available since August 2025) is the only marketed generic GLP-1 with a weight-loss indication in the U.S. The Wegovy pill starts at $149/month for the 1.5 mg dose through self-pay. Always verify pharmacy licensing and provider credentials, regardless of price.
Can I increase GLP-1 naturally instead of taking medication?
Certain foods (protein, fiber, healthy fats) and habits (exercise, sleep) can support your body's natural GLP-1 production. These are healthy habits worth pursuing, but the effect is modest compared to prescription medication. Natural strategies complement GLP-1 therapy — they don't replace it for people who meet clinical criteria.
Sources
- Wilding JPH, et al. "Once-Weekly Semaglutide in Adults with Overweight or Obesity." New England Journal of Medicine, 2021 (STEP 1)
- Jastreboff AM, et al. "Tirzepatide Once Weekly for the Treatment of Obesity." New England Journal of Medicine, 2022 (SURMOUNT-1)
- FDA Prescribing Information: Wegovy (semaglutide injection)
- FDA Prescribing Information: Wegovy (semaglutide tablets)
- FDA Prescribing Information: Ozempic (semaglutide injection)
- FDA Prescribing Information: Zepbound (tirzepatide injection)
- FDA Prescribing Information: Mounjaro (tirzepatide injection)
- FDA Prescribing Information: Saxenda (liraglutide injection)
- Lincoff AM, et al. "Semaglutide and Cardiovascular Outcomes in Obesity without Diabetes." New England Journal of Medicine, 2023 (SELECT)
- CMS: BALANCE Model announcement and Medicare GLP-1 Bridge demonstration (cms.gov)
- Wharton S, et al. "Oral Semaglutide at a Dose of 25 mg in Adults with Overweight or Obesity." New England Journal of Medicine, 2025 (OASIS 4)
- Teva: FDA Approval and Launch of Generic Saxenda (liraglutide injection), August 2025
- Wegovy.com: Current savings and self-pay pricing (accessed March 2026)
- FDA: Clarification on compounding policies as GLP-1 supply stabilizes; FDA consumer warning on unapproved GLP-1 products
- Ohio State Health & Discovery: Nutrition plan when on GLP-1 medication
- Mass General: Fitness for People Taking GLP-1 Agonists
- FDA Drug Safety Communication: FDA Requests Removal of Suicidal Behavior and Ideation Warning from GLP-1 RA Medications (January 13, 2026)
Related Articles
GLP-1 Medications Available in 2026: Pills, Shots & Costs
Every GLP-1 medication in 2026 — Foundayo, Wegovy HD, Wegovy pill. Verified costs, pill vs shot tradeoffs, who each one fits.
GLP-1 Pros and Cons: Benefits, Risks & Costs
GLP-1 pros and cons explained: expected weight loss, side effects, cost, safety risks, who qualifies, pills vs shots, and decision tools (2026).
GLP-1 Weight Loss Calculator: Wegovy, Zepbound & Foundayo
Estimate your weight loss on Wegovy, Zepbound, or Foundayo with our GLP-1 weight loss calculator. Anchored to FDA-label trial data. Verified May 2026.
GLP-1 Tips for Beginners: 30-Day Playbook
GLP-1 tips & tricks for beginners: injection-day routine, foods to eat/avoid, side-effect fixes, muscle protection + 30-day checklist. Updated 2026.
How GLP-1 Works for Weight Loss: Mechanism, Results & Risks
How GLP-1 medications like Ozempic and Wegovy work for weight loss. Mechanism map, clinical trial results, side effects, and decision framework.
Incretin: What It Is, How It Works & Drugs Explained
Incretin hormones (GLP-1 & GIP) explained: what they are, how they work, complete drug list, and why they matter for diabetes and weight loss.