GLP-1 Pros and Cons (2026): Benefits, Risks & Costs
 Medically Reviewed by Dr. Jillian Foglesong Stabile, MD, FAAFP, DABOM
Medically Reviewed by Dr. Jillian Foglesong Stabile, MD, FAAFP, DABOMDisclosure: Some links on this site are affiliate links. If you purchase through these links, we may earn a commission at no extra cost to you. Thank you for supporting our site. For informational purposes only—not medical advice.
On this page
The Verdict (Read This First)
Looking for the real GLP-1 pros and cons? Here's the evidence-based trade-off: these medications can produce substantial weight loss and improve cardiometabolic risk—but side effects, cost, and long-term maintenance matter.
GLP-1-based anti-obesity medications work. In clinical trials for chronic weight management, Wegovy (semaglutide) — available as both a weekly injection and a daily pill — and Zepbound (tirzepatide) produced large average weight loss (roughly mid-teens to low-20% depending on dose and trial). Ozempic is the same medication as Wegovy (semaglutide) and Mounjaro is the same medication as Zepbound (tirzepatide) — they're just approved for different purposes (type 2 diabetes rather than weight loss). Both are sometimes prescribed off-label for weight loss; outcomes can differ by dose and population.
But they're not for everyone. GI side effects are common (especially during dose increases). In pivotal trials, rates for individual symptoms—like nausea, diarrhea, constipation, and vomiting—varied by medication and dose, often from the teens up to ~40%. Costs range from $149 to $1,000+ per month depending on your insurance and which medication you choose. Most people regain weight if they stop taking the medication. And some people have medical conditions that make these drugs unsafe.
Who should consider GLP-1s: Adults with a BMI of 30 or higher, OR a BMI of 27+ with weight-related health problems like type 2 diabetes, high blood pressure, or sleep apnea—who haven't succeeded with diet and exercise alone.
Who should NOT use GLP-1s: Anyone with a personal or family history of medullary thyroid cancer or MEN2 syndrome. Anyone who is pregnant, trying to become pregnant, or breastfeeding. Anyone with a history of severe allergic reactions to these medications.
Use the decision tools below to figure out if GLP-1s might be right for your situation—then talk to your doctor.
Quick Pros and Cons Summary
| PROS | CONS |
|---|---|
| ✅ Significant weight loss (mid-teens to low-20% in trials) | ❌ Common GI side effects (nausea, constipation, diarrhea) |
| ✅ Reduces appetite and "food noise" | ❌ Expensive ($149-$1,000+/month) |
| ✅ Improves blood sugar control | ❌ Insurance coverage is inconsistent |
| ✅ Lowers blood pressure and cholesterol | ❌ Weight often returns if you stop |
| ✅ Semaglutide 2.4 mg (Wegovy) reduces heart attack/stroke risk in adults with established cardiovascular disease | ❌ Requires long-term commitment |
| ✅ Multiple options (pills and injections) | ❌ Rare but serious risks (pancreatitis, gallbladder) |
| ✅ FDA-approved and well-studied | ❌ Not safe for some people (see contraindications) |
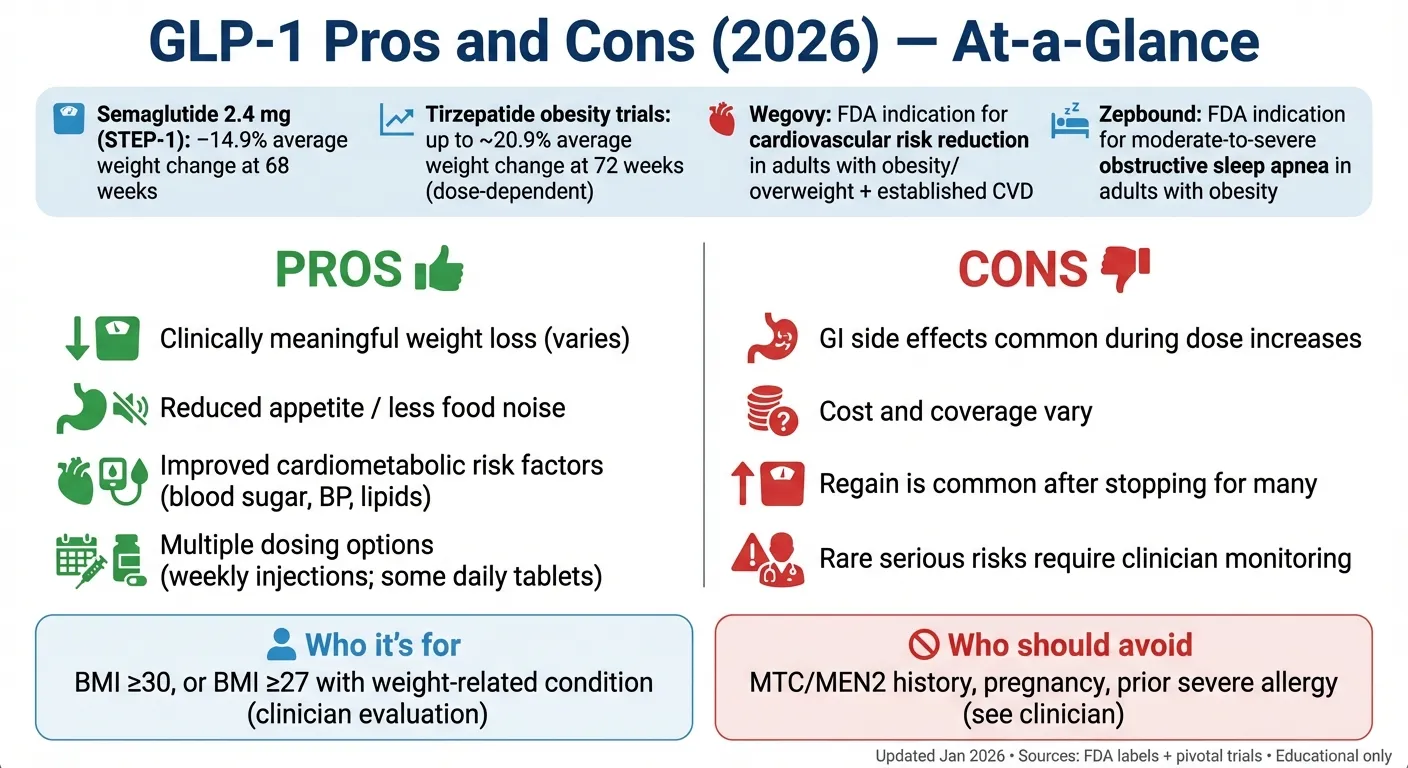
Table of Contents
- What Are GLP-1 Medications?
- FDA-Approved GLP-1 Medications
- The Benefits (Pros)
- The Downsides (Cons)
- Who Should Consider GLP-1s
- Which GLP-1 Is Best for Weight Loss?
- GLP-1 Pills Pros and Cons
- GLP-1 Patch Pros and Cons
- GLP-1 Before and After
- GLP-1 With the Least Side Effects
- GLP-1 Weight Loss Oral Solution
- Is GLP-1 a Scam?
- Managing Side Effects
- What Happens If I Stop?
- Cost and Coverage
- GLP-1s Without Diabetes
- FAQs
- The GLP-1 Decision Kit
What Are GLP-1 Medications?
GLP-1 stands for "glucagon-like peptide-1." GLP-1 medications are called GLP-1 receptor agonists (GLP-1 RAs). That's a mouthful, so here's what it actually means:
Your body naturally makes a hormone called GLP-1 when you eat. This hormone tells your brain you're full, signals your pancreas to release insulin, and slows down how fast food leaves your stomach. GLP-1 medications mimic this natural hormone—but in a stronger, longer-lasting way. Learn more about how GLP-1 works for weight loss.
The result? You feel satisfied with less food. The constant mental chatter about what to eat next (what patients call "food noise") quiets down. You don't feel like you're white-knuckling your way through every meal.
Important distinction: Tirzepatide (Mounjaro, Zepbound) is technically a dual GIP/GLP-1 receptor agonist — it mimics both GLP-1 and another hormone called GIP, giving it a slightly different mechanism of action than GLP-1-only drugs like semaglutide. This dual mechanism may account for why tirzepatide often produces more weight loss and may have a somewhat different side effect profile. People commonly group all of these medications under "GLP-1s" in conversation, and we'll do the same here — but it's worth knowing tirzepatide works on two receptors, not just one.
Same medications, different names: Ozempic and Wegovy both contain semaglutide — Wegovy is approved for weight management and cardiovascular risk reduction, while Ozempic is approved for type 2 diabetes. Similarly, Zepbound and Mounjaro both contain tirzepatide — Zepbound is approved for weight loss and obstructive sleep apnea, while Mounjaro is approved for type 2 diabetes. The active ingredient is the same; the brand name and FDA indication are different.
About compounded GLP-1 products: You may encounter cheaper "compounded" versions of semaglutide or tirzepatide from telehealth providers or compounding pharmacies. These are not FDA-approved, and the FDA has issued multiple warnings about safety concerns including dosing errors and fraudulent labels. We cover this in detail in our safety section below.
What GLP-1s Are NOT
Before we go further, let's clear up some confusion:
GLP-1 medications are not supplements. They're prescription drugs that require a doctor's evaluation and ongoing monitoring. No supplement can replicate what these medications do.
GLP-1 "patches" are not FDA-approved medications. Products marketed as "GLP-1 patches" typically contain herbal ingredients like berberine—not actual GLP-1 drugs. They haven't been proven to work and shouldn't be considered alternatives to prescription medications. More on this in our safety section.
GLP-1s are not instant fat burners. They work gradually over months. They require lifestyle changes (nutrition and movement) for best results. They're tools, not magic.
FDA-Approved GLP-1 Medications
This matters more than most people realize. Medications are approved for specific uses based on clinical trials. Using a drug "off-label" (for something it wasn't approved for) isn't necessarily wrong, but it affects insurance coverage and what we know about safety.
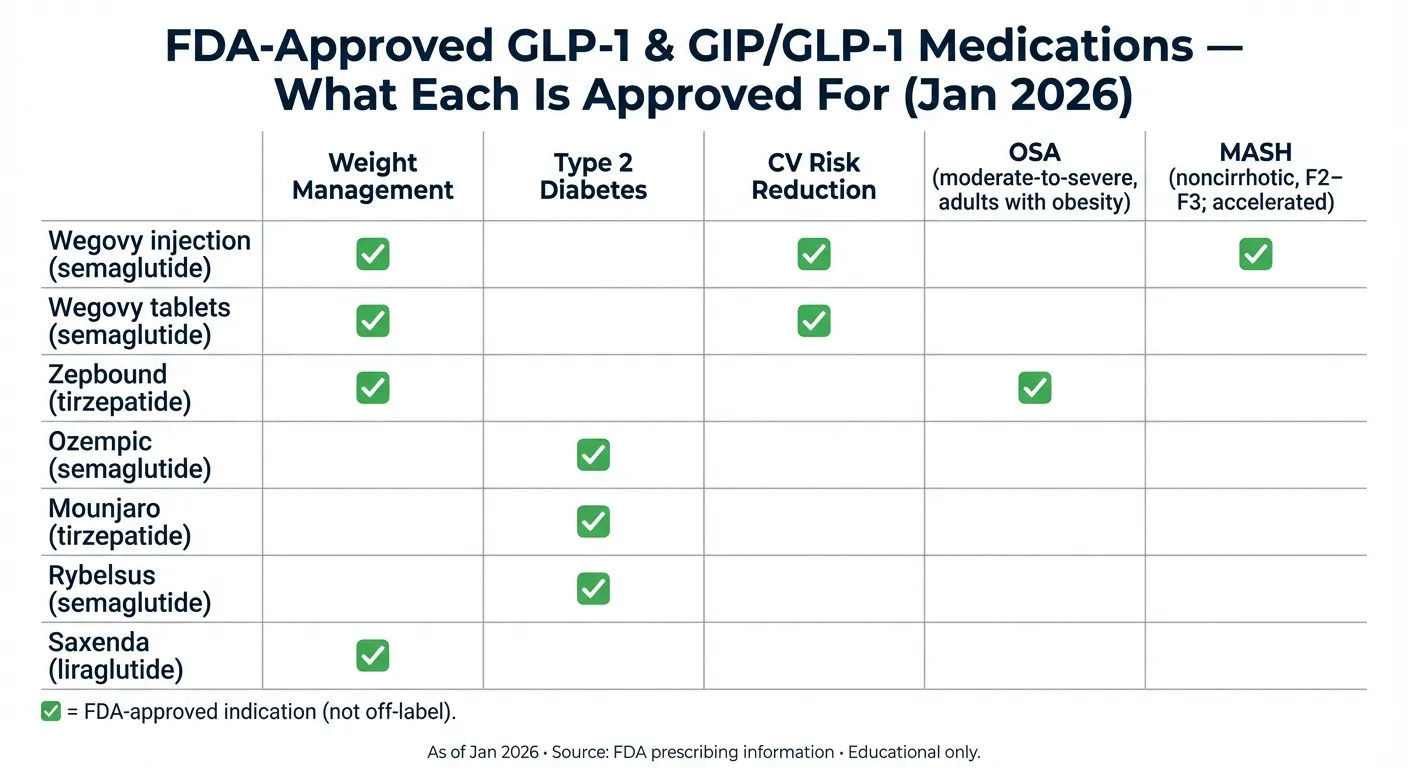
Key FDA-Approved GLP-1 / GIP-GLP-1 Medications (January 2026)
| Medication | Generic Name | Type | Form | FDA-Approved For | Key Notes |
|---|---|---|---|---|---|
| Wegovy | Semaglutide | GLP-1 | Weekly injection | Weight management, CV risk reduction | Also has FDA accelerated approval for noncirrhotic MASH (metabolic dysfunction–associated steatohepatitis) with moderate-to-advanced liver fibrosis (F2–F3) |
| Wegovy tablets | Semaglutide | GLP-1 | Daily tablet | Weight management, CV risk reduction | Approved Dec 22, 2025; available early Jan 2026. Self-pay pricing reported as $149/month starter dose and up to $299/month for higher doses (program-dependent) |
| Zepbound | Tirzepatide | GLP-1/GIP | Weekly injection | Weight loss, Sleep apnea (OSA) | Highest weight loss in trials |
| Ozempic | Semaglutide | GLP-1 | Weekly injection | Type 2 diabetes | Often used off-label for weight loss |
| Mounjaro | Tirzepatide | GLP-1/GIP | Weekly injection | Type 2 diabetes | Often used off-label for weight loss |
| Rybelsus | Semaglutide | GLP-1 | Daily tablet | Type 2 diabetes | Lower dose than Wegovy tablet |
| Saxenda | Liraglutide | GLP-1 | Daily injection | Weight loss | Older medication; daily dosing (not weekly); less weight loss than semaglutide or tirzepatide |
| Victoza | Liraglutide | GLP-1 | Daily injection | Type 2 diabetes | Same active ingredient as Saxenda; daily dosing |
Sources: FDA prescribing information for each medication (accessdata.fda.gov)
What This Means for You
If your goal is weight loss: Wegovy (injection or pill) and Zepbound are FDA-approved specifically for this purpose. Insurance coverage may be easier to obtain with these.
If you have type 2 diabetes: Ozempic, Mounjaro, Rybelsus, and Victoza are approved for diabetes management. Weight loss is a beneficial side effect.
If you have sleep apnea: Zepbound is now specifically approved to treat moderate-to-severe obstructive sleep apnea in adults with obesity. This is a newer indication that may help with insurance coverage.
The "approved vs. off-label" reality: Many doctors prescribe Ozempic or Mounjaro for weight loss even though they're technically approved only for diabetes. This is common and generally safe, but it can create insurance headaches.
The Benefits of GLP-1 Medications (Pros)
Pro #1: Clinically Meaningful Weight Loss
This is what brings most people to GLP-1s, so let's look at the real numbers.
What clinical trials show:
| Medication | Average Weight Loss | Timeframe | Trial |
|---|---|---|---|
| Liraglutide 3mg (Saxenda) | ~8% (~5-6% more than placebo) | 56 weeks | SCALE |
| Semaglutide 2.4mg (Wegovy) | 14.9% | 68 weeks | STEP 1 |
| Tirzepatide 5mg | 15.0% | 72 weeks | SURMOUNT-1 |
| Tirzepatide 10mg | 19.5% | 72 weeks | SURMOUNT-1 |
| Tirzepatide 15mg | 20.9% | 72 weeks | SURMOUNT-1 |
| Oral semaglutide 25mg (Wegovy tablet) | 13.6% | 64 weeks | Study 7 / OASIS 4 |
Sources: New England Journal of Medicine (STEP 1, SURMOUNT-1, SURMOUNT-5)
What this means in real pounds: For a 200-pound person, 15% weight loss equals 30 pounds. For a 250-pound person, 20% equals 50 pounds. These are significant, life-changing amounts for most people.
Real-world results are slightly lower. A 2025 Cleveland Clinic study found that patients who stayed on treatment for a full year lost an average of 11.9% of their body weight—still excellent, but less than clinical trials. Why the difference?
- Clinical trials provide intensive support and monitoring
- Real-world adherence is messier
- Cost causes some people to quit early or skip doses
- Side effects lead some to discontinue
The honest timeline: Most people notice reduced appetite within the first 1-2 weeks. Visible weight loss typically becomes apparent at 4-8 weeks. Maximum results usually occur around 12-18 months, followed by a plateau (which is normal, not failure).
Pro #2: Reduced Appetite and "Food Noise"
Many patients describe this as the most life-changing benefit—even more than the number on the scale.
"Food noise" is the constant mental chatter about eating: What should I have for lunch? Should I have that cookie? Why can't I stop thinking about food? For people who struggle with their weight, this mental burden is exhausting.
GLP-1 medications act on appetite centers in the brain. Most users report that food simply becomes less interesting. They can eat a reasonable portion and feel genuinely satisfied. They can walk past the break room donuts without a mental battle.
This isn't willpower—it's biochemistry. And for many people, it makes sustainable lifestyle changes finally feel achievable.
Pro #3: Blood Sugar Control and Metabolic Health
GLP-1 medications were originally developed for type 2 diabetes, and they're remarkably effective for blood sugar control.
What the evidence shows:
- Average HbA1c reduction of 1.0-2.0% (significant)
- Improved fasting glucose levels
- Enhanced insulin sensitivity
- Reduced need for other diabetes medications in some patients
Even for people without diabetes, GLP-1s improve metabolic health. A Cleveland Clinic study found that 53.9% of patients with prediabetes who used GLP-1s converted to normal blood sugar levels within one year.
Pro #4: Heart and Blood Vessel Benefits
This might be the most important benefit that people don't hear enough about.
The SELECT trial (published in 2023) showed that semaglutide reduced major cardiovascular events—heart attacks, strokes, and cardiovascular death—by 20% in people with obesity who didn't have diabetes.
GLP-1s also improve other cardiovascular risk factors:
- Lower blood pressure
- Improved cholesterol profiles (especially triglycerides)
- Reduced inflammation markers
- Potential kidney protection
Wegovy now has an FDA-approved indication for cardiovascular risk reduction—meaning it's officially recognized as a heart-protective medication, not just a weight loss drug.
Pro #5: Specific Benefits for Sleep Apnea (New)
As of 2024, Zepbound became the first GLP-1-based medication approved to treat moderate-to-severe obstructive sleep apnea (OSA) in adults with obesity.
This is significant because:
- OSA affects an estimated 30 million Americans
- Weight loss is one of the most effective treatments for OSA
- This indication may help with insurance coverage for patients who have both obesity and sleep apnea
Zepbound doesn't replace CPAP machines for everyone, but it provides another treatment option—especially for patients who can't tolerate CPAP.
Pro #6: Emerging Benefits Under Investigation
Important: Many of these findings come from observational analyses (associations in large datasets). They do not prove GLP-1 drugs prevent or treat these conditions, but they help researchers decide what to test in randomized trials.
Research suggests GLP-1s may be associated with benefits in conditions beyond weight and diabetes:
- Cognitive function: A January 2025 Washington University study found GLP-1s were associated with reduced risk of Alzheimer's disease and dementia
- Addiction: Some users report reduced cravings for alcohol, nicotine, and other substances (research is ongoing)
- Liver disease: Wegovy now has accelerated approval for MASH (metabolic dysfunction-associated steatohepatitis), a form of fatty liver disease
- Inflammation: GLP-1s appear to reduce inflammatory markers throughout the body
These associations are still being studied, but they help explain why GLP-1s are generating excitement beyond weight loss.
The Downsides of GLP-1 Medications (Cons)
Every medication has downsides. Being honest about these helps you make a realistic decision.
Con #1: Gastrointestinal Side Effects (Very Common)
Let's be direct: most people experience some GI side effects, especially in the first weeks and during dose increases.
Hair Loss
Hair loss is a frequent concern patients raise with their clinicians. Some people experience noticeable hair thinning while on GLP-1 medications. This is most likely telogen effluvium — a stress response to rapid weight change that pushes hair follicles into a resting phase prematurely. It is not unique to GLP-1 medications and can occur with any significant weight loss.
What typically happens: Hair shedding increases noticeably 2–4 months after rapid weight loss begins. In most cases, it is temporary and resolves as weight stabilizes — though the timeline can be several months.
What may help: Adequate protein intake, a balanced diet with sufficient micronutrients (iron, zinc, biotin), and avoiding crash-level calorie restriction. If hair loss is persistent or severe, discuss with your clinician — they may want to check for other contributing factors.
Side Effect Frequency and Management Table
| Side Effect | How Common | When It Usually Happens | How to Manage It |
|---|---|---|---|
| Nausea | ~25-44% (varies by dose and drug; see FDA label adverse reactions tables) | First weeks, dose increases | Eat smaller meals, avoid fatty foods, try ginger or peppermint |
| Vomiting | ~8-24% (varies by dose and drug) | First weeks, dose increases | Stay hydrated, eat bland foods, don't lie down after eating |
| Diarrhea | ~18-30% (varies by dose and drug) | Variable | Stay hydrated, avoid dairy temporarily, consider probiotics |
| Constipation | ~11-24% (varies by dose and drug) | Often ongoing | Increase fiber gradually, drink more water, stay active |
| Abdominal distension/bloating | ~3-7% (label data shown) | Often ongoing | Smaller meals, eat slowly, avoid carbonated drinks |
| GERD/acid reflux | ~4-5% (dyspepsia may be higher) | Variable | Don't eat close to bedtime, avoid trigger foods |
| Belching/eructation (sometimes described as "sulfur burps") | ~4-7% (label data shown) | Variable | Smaller meals, avoid eggs and cruciferous vegetables temporarily |
The good news: These side effects usually improve within 4-8 weeks as your body adjusts. Slow dose escalation (titration) significantly reduces their severity. Most people find them manageable, though some do discontinue treatment because of them.
The warning signs to watch for: If you experience severe abdominal pain (especially radiating to your back), persistent vomiting, or signs of dehydration, contact your healthcare provider promptly. These could indicate more serious issues.
Con #2: Serious But Rare Risks
Every GLP-1 medication carries warnings about potential serious risks. These are uncommon, but you should understand them.
Serious Risk Table
| Risk | What FDA Labels Show (Examples) | Warning Signs | What to Do |
|---|---|---|---|
| Acute pancreatitis | Uncommon (e.g., 0.2% in pooled Zepbound weight reduction trials) | Severe upper abdominal pain (may radiate to back), persistent vomiting | Seek urgent medical care |
| Gallbladder disease (gallstones/cholecystitis) | Uncommon (Wegovy adult weight-loss trials: cholelithiasis 1.6% vs 0.7% placebo; Zepbound pooled trials: 1.1% vs 1.0% placebo) | Right upper abdominal pain, fever, jaundice | Contact clinician promptly; urgent care if severe |
| Kidney injury (often dehydration-related) | Risk increases if severe vomiting/diarrhea causes dehydration | Very low urine output, confusion, swelling | Seek medical care |
| Severe allergic reaction | Very rare | Facial swelling, trouble breathing, hives | Emergency care |
| Hypoglycemia | Usually low risk alone; higher with insulin/sulfonylureas | Shaking, sweating, confusion | Treat per clinician plan |
Sources: FDA prescribing information (accessdata.fda.gov)
About the thyroid cancer warning: All GLP-1 medications carry a boxed warning (the FDA's most serious warning) about thyroid C-cell tumors. In animal studies, these medications caused thyroid tumors in rodents. This has NOT been confirmed in humans, but out of caution, these medications are contraindicated if you or a close family member has ever had medullary thyroid carcinoma or MEN2 syndrome.
About suicidal thoughts: FDA reviews have not found evidence of an increased risk; in January 2026, FDA requested removal of suicidal behavior/ideation warning language from Wegovy, Saxenda, and Zepbound labeling. Patients should still report new or worsening mood symptoms to their prescriber.
Con #3: The Cost Problem
Let's be honest: these medications are expensive, and affording them is a real barrier for many people.
Important note about insurance: Costs for GLP-1 medications may be significantly lower if your insurance covers medication for weight loss — or if you have another health condition for which these medications are approved (such as Zepbound for moderate-to-severe obstructive sleep apnea). However, in clinical experience, most insurance plans still do not cover medications strictly for weight loss. If your insurance does cover a GLP-1, your out-of-pocket cost could be well under $149/month with copay assistance programs. Always check your specific plan before assuming you need to pay full cash price.
Price Ranges by Pathway (January 2026)
| Pathway | What It Means | Typical Range / Examples (verify before purchasing) |
|---|---|---|
| Retail cash (list price) | Paying without discounts/programs | Often $1,000+/month for branded GLP-1/GIP injections (varies by product/pharmacy) |
| Cash-pay / federal pricing deals | Program-based pricing | Reported examples include Wegovy injection ~$349/month cash price and Wegovy tablets $149/month starter dose up to $299/month for higher doses (program dependent) |
| Insurance copay | Copay after coverage/PA | Can be low for some plans, but coverage is inconsistent and often requires prior authorization |
Prices vary by pharmacy, dose, and eligibility; verify with your pharmacy/insurer.
The insurance reality:
Coverage varies widely. In one 2025 employer survey, 36% reported covering GLP-1 drugs for both diabetes and weight loss, while 55% covered them for diabetes only. Other analyses (focused on large firms' largest plans) have found lower coverage rates for weight loss, so you should check your specific plan.
- Many plans require prior authorization, step therapy, or documentation of failed alternatives
- Coverage varies dramatically by state for Medicaid
Recent pricing changes: The Trump administration announced deals with Eli Lilly and Novo Nordisk in November 2025 to lower GLP-1 prices. Eligibility and rollout details vary, and the pricing applies under specific program terms (for example, Medicare beneficiary copay levels and cash-pay pricing via the program site). These changes are rolling out in 2026.
Con #4: Weight Regain After Stopping (The Uncomfortable Truth)
This is something you need to understand before starting: most people regain weight if they stop taking GLP-1 medications.
What the research shows:
The STEP 1 extension study followed patients after they stopped semaglutide. Within one year of stopping:
- Participants regained approximately two-thirds of the weight they had lost
- Appetite returned to pre-medication levels
- Cardiometabolic improvements partially reversed
The SURMOUNT-4 trial showed similar results for tirzepatide: patients who switched to placebo after 36 weeks regained weight, while those who continued the medication maintained their loss.
Why this happens: GLP-1s don't "fix" the underlying biology that made weight loss difficult in the first place. They work by overriding that biology. When you stop the medication, your natural appetite signals return—and for most people, so does the weight.
What this means practically: GLP-1 medications should generally be viewed as long-term (potentially lifelong) treatment, similar to blood pressure or cholesterol medications. Some patients may be able to reduce to a lower maintenance dose. Very few can stop entirely without regain.
This isn't a moral failing—it's physiology. But it's important to understand before committing to treatment.
Con #5: The Muscle Loss Concern
When you lose weight—by any method—you lose both fat and lean mass. With GLP-1 medications, studies suggest that ~25-40% of weight lost may come from lean mass (varies by study).
Why this matters:
- Muscle supports your metabolism
- Muscle loss can lead to weakness and frailty, especially in older adults
- Muscle is harder to rebuild than fat
What you can do about it: Research and clinical experience show that muscle loss can be significantly reduced by:
- Resistance training (strength training) 2-3 times per week
- Adequate protein intake (aim for 1.0-1.5 grams per kilogram of body weight daily)
- Staying physically active in general
Case studies show that patients who prioritize exercise and protein can lose mostly fat while maintaining or even building muscle on GLP-1s. This requires effort, but it's achievable.
Con #6: Unknowns About Very Long-Term Use
GLP-1 medications have been used for diabetes since 2005, so we have nearly two decades of safety data in that population. However, their widespread use for weight loss at higher doses is newer (Wegovy was approved in 2021; Zepbound in 2023).
What we're still learning:
- Effects on bone density with sustained weight loss
- Potential impacts on brain function, vision, or other organ systems over decades
- Optimal strategies for long-term maintenance
- Whether some people can safely discontinue after reaching goals
This doesn't mean the medications are unsafe—they've passed rigorous FDA review. It means we should remain humble about what we don't yet know and continue monitoring for new information.
Who Should Consider GLP-1 Medications
FDA Eligibility Criteria
For Weight Loss (Wegovy, Zepbound, Saxenda):
- BMI of 30 or higher (obesity), OR
- BMI of 27 or higher with at least one weight-related health condition such as:
- Type 2 diabetes or prediabetes
- High blood pressure
- High cholesterol
- Obstructive sleep apnea
- Heart disease
- Fatty liver disease
Check your GLP-1 eligibility with our quick assessment tool.
For Type 2 Diabetes (Ozempic, Mounjaro, Rybelsus):
- Diagnosis of type 2 diabetes
- As an addition to diet and exercise
Good Candidates (Beyond Just BMI)
You may be a particularly good candidate if:
✅ Diet and exercise alone haven't worked despite consistent effort over 6+ months
✅ You have weight-related health conditions that would improve with weight loss
✅ You understand this is likely a long-term commitment, not a quick fix
✅ You're willing to make lifestyle changes (nutrition, activity) alongside the medication
✅ You can access and afford the medication (or have a plan for coverage)
✅ You're able to attend regular follow-up appointments
✅ You don't have any contraindications (see below)
Who Should NOT Use GLP-1 Medications (Hard Stops)
Note: Per FDA labeling, formal contraindications are MTC/MEN2 history and serious hypersensitivity. The items below (pregnancy, breastfeeding, type 1 diabetes/DKA, etc.) are situations where these drugs are not recommended or not indicated.
Do NOT use:
❌ Personal or family history of medullary thyroid carcinoma (MTC) — a rare type of thyroid cancer. This includes parents, siblings, and children with MTC.
❌ Multiple Endocrine Neoplasia syndrome type 2 (MEN2) — a genetic condition that increases thyroid cancer risk.
❌ Previous severe allergic reaction to the specific GLP-1 medication or any of its ingredients.
❌ Currently pregnant or planning pregnancy — These medicines are not recommended in pregnancy. For semaglutide products, labeling recommends stopping at least 2 months before a planned pregnancy (due to drug persistence). For other agents, follow the product label and your clinician's guidance.
❌ Type 1 diabetes — GLP-1s are not indicated for T1D and should not be used.
❌ Diabetic ketoacidosis — a serious diabetes complication requiring different treatment.
Learn more about GLP-1 contraindications for complete details.
Proceed with Caution (Requires Careful Discussion with Your Doctor)
These conditions don't necessarily rule out GLP-1 therapy, but they require careful discussion with your prescriber and potentially closer monitoring:
⚠️ History of pancreatitis — GLP-1 medications carry a labeled warning for pancreatitis. Clinicians are generally more reluctant to prescribe in this group, and closer monitoring is warranted. If you have a history of pancreatitis, make sure your prescriber knows before starting.
⚠️ Gastroparesis — Since GLP-1 medications slow gastric emptying, they can worsen symptoms in people who already have delayed stomach emptying. This group requires careful evaluation and may need modified dosing or closer monitoring.
⚠️ Severe GI disease — Conditions that affect gut motility or absorption may interact unpredictably with GLP-1 medications.
⚠️ Severe kidney disease — dose adjustment is usually not required, but close monitoring is important (especially if vomiting/diarrhea causes dehydration)
⚠️ History of gallbladder disease — rapid weight loss increases gallstone risk
⚠️ Diabetic retinopathy — rapid blood sugar improvement can temporarily worsen eye disease
Which GLP-1 Is Best for Weight Loss?
The "best" GLP-1 depends on your priorities. Here's how the options compare:
The Weight Loss Results Ranking
Based on clinical trial data:
- Tirzepatide 15mg (Zepbound) — ~21% average weight loss
- Tirzepatide 10mg (Zepbound) — ~19.5% average weight loss
- Semaglutide 2.4mg (Wegovy injection) — ~15% average weight loss
- Tirzepatide 5mg (Zepbound) — ~15.0% average weight loss
- Oral semaglutide 25mg (Wegovy tablet) — ~13.6% average weight loss
- Liraglutide 3mg (Saxenda) — ~8% average weight loss
Choosing Based on Your Priorities
| If You Prioritize... | Consider... | Why |
|---|---|---|
| Maximum weight loss | Zepbound (tirzepatide) | Highest weight loss in trials |
| Heart protection | Wegovy (semaglutide) | Strongest CV outcome data (SELECT trial) |
| Lowest cost | Oral Wegovy | $149-299/month vs $400-1000+ for injections |
| No needles | Oral Wegovy | Daily pill; similar effectiveness |
| Less frequent dosing | Any injectable | Once weekly vs daily |
For a detailed comparison, see our semaglutide vs tirzepatide guide.
GLP-1 Pills Pros and Cons
With oral Wegovy now available, many people are weighing pills versus injections.
Oral GLP-1 Pros
✅ No needles — Important for needle-phobic patients
✅ Lower cost — $149-299/month vs $400-1000+ for injections
✅ Travel-friendly — No refrigeration required; easier to carry
✅ Similar effectiveness — ~13% weight loss (comparable to mid-dose injections)
✅ Privacy — No visible injection supplies
Oral GLP-1 Cons
❌ Daily dosing — Must take every morning vs weekly injection
❌ Strict timing requirements — Take on empty stomach with minimal water, wait 30 minutes before eating/drinking anything else
❌ Reduced flexibility — Morning routine must accommodate the timing
❌ GI side effects may differ — Some patients report more stomach discomfort
❌ Absorption variability — Food reduces effectiveness significantly
Who Should Consider Pills vs. Injections?
Pills may be better if:
- You have needle phobia
- Cost is a major factor
- You travel frequently
- You have a consistent morning routine
Injections may be better if:
- You want maximum weight loss (higher tirzepatide doses)
- Your mornings are unpredictable
- You forget daily medications
- You want the flexibility of once-weekly dosing
GLP-1 Patch Pros and Cons
Important Warning
There are currently NO FDA-approved GLP-1 patches. Products marketed as "GLP-1 patches" are typically supplements containing herbal ingredients like berberine—not actual GLP-1 medications.
What "GLP-1 Patches" Actually Are
Products marketed online as "GLP-1 patches" are:
- Not prescription medications
- Not FDA-approved for weight loss
- Not clinically proven to produce GLP-1-like effects
- Often contain ingredients like berberine, green tea extract, or other supplements
Why This Matters
- No clinical trials support their effectiveness
- They cannot replicate what prescription GLP-1 medications do
- Claims of "natural GLP-1 activation" are not backed by FDA-reviewed evidence
- Buying them may delay seeking treatments that actually work
If you're interested in GLP-1 therapy, work with a licensed healthcare provider to access FDA-approved medications.
GLP-1 Before and After
What to Realistically Expect
Month 1:
- Appetite reduction begins (often within 1-2 weeks)
- Some side effects (nausea, GI symptoms)
- Weight loss: typically 2-5 pounds
- Adjustment period
Months 2-3:
- Side effects usually improving
- More noticeable appetite control
- Weight loss accelerating
- Weight loss: typically 5-10% of starting weight
Months 4-6:
- Approaching target doses
- Significant weight loss visible
- Energy levels often improving
- Weight loss: typically 10-15% of starting weight
Months 6-12:
- Approaching maximum weight loss
- Side effects typically minimal
- New eating patterns established
- Weight loss: typically 15-22% of starting weight (varies by medication)
Year 2 and Beyond:
- Weight maintenance phase
- May be able to reduce to maintenance dose
- Continued medication typically needed
- Focus shifts to maintaining results
Real-World vs. Clinical Trial Results
Clinical trials show impressive numbers, but real-world results are typically slightly lower:
- Clinical trials: 15-21% average weight loss
- Real-world studies: 10-12% average weight loss
Why the gap?
- Clinical trials have intensive monitoring and support
- Real-world adherence is imperfect
- Cost causes some to discontinue early
- Side effects lead to dropouts
GLP-1 With the Least Side Effects
All GLP-1 medications cause similar side effects through similar mechanisms. However, there are ways to minimize your experience.
Which Medication Has Fewer Side Effects?
No clear winner. Studies comparing semaglutide and tirzepatide show similar overall side effect profiles. Individual responses vary significantly—some people tolerate one medication better than another.
How to Minimize Side Effects (Regardless of Medication)
1. Slow Titration Is Key
- Start at the lowest dose
- Wait the recommended time before increasing
- If side effects are severe, ask about staying at current dose longer
2. Dietary Adjustments
- Eat smaller portions
- Avoid high-fat, greasy foods
- Reduce spicy foods
- Eat slowly and chew thoroughly
- Stop eating when satisfied (not stuffed)
3. Stay Hydrated
- Drink plenty of water throughout the day
- Avoid carbonated beverages
- Limit alcohol
4. Medication Timing
- Take at the same time each week (injections)
- Take on empty stomach with minimal water (oral)
- Some patients find certain times of day work better
5. Work with Your Provider
- Report side effects promptly
- Ask about dose adjustments if needed
- Consider switching medications if one doesn't work
For more strategies, see our complete GLP-1 side effects management guide.
GLP-1 Weight Loss Oral Solution
Despite the common search term "oral solution," the FDA-approved oral option is a tablet (Wegovy pill).
Oral Wegovy (semaglutide tablets) represents the newest option for GLP-1 weight loss:
Key Facts About Oral Wegovy
- FDA approved: December 22, 2025
- Available: Early January 2026
- Dosing: Daily tablet (vs weekly injection)
- Effectiveness: 13.6% weight loss at 64 weeks (Study 7 / OASIS 4)
- Cost: $149/month (starter dose) to $299/month (higher doses)
How Oral GLP-1 Works
The tablet uses a technology called SNAC (sodium N-[8-(2-hydroxybenzoyl) amino] caprylate) to enhance absorption in the stomach. This requires:
- Taking on an empty stomach
- Swallowing with minimal water (no more than 4 oz)
- Waiting 30 minutes before eating, drinking, or taking other medications
Who Is Oral Wegovy Best For?
✅ People who want to avoid needles ✅ Those seeking the most affordable brand-name option ✅ Patients with consistent morning routines ✅ People who travel frequently
Is GLP-1 a Scam?
Short answer: No. FDA-approved GLP-1 medications are among the most studied and effective weight loss treatments ever developed. However, there are scams in the GLP-1 space you should avoid.
What's NOT a Scam
✅ FDA-approved medications (Wegovy, Zepbound, Ozempic, Mounjaro, etc.) ✅ Prescriptions from licensed providers filled at licensed pharmacies ✅ Legitimate telehealth companies with proper medical oversight
What IS a Scam (Or High Risk)
❌ "GLP-1 patches" — No FDA-approved GLP-1 patches exist
❌ "Research peptides" — Products labeled "not for human consumption"
❌ No-prescription-needed offers — All GLP-1s require prescriptions
❌ Dramatically low prices — If it seems too good to be true, it is
❌ Unverifiable online pharmacies — Can't confirm licensing
FDA Warnings About Compounded GLP-1s
"Compounded" medications are custom-made by compounding pharmacies rather than manufactured by drug companies. They became popular during GLP-1 shortages because they're often cheaper.
The FDA has issued multiple warnings about compounded semaglutide and tirzepatide:
-
Dosing errors: The FDA received reports of hospitalizations related to patients measuring and administering incorrect doses from compounded vials. Unlike manufacturer pens with pre-measured doses, vials require patients to calculate and draw up doses—leading to dangerous mistakes.
-
Fraudulent labels: The FDA found compounded products with labels listing pharmacies that don't exist, or pharmacies that didn't actually make the product.
-
Unapproved salt forms: Some compounded products contain "semaglutide sodium" or "semaglutide acetate"—different chemical forms than the FDA-approved drug. The FDA hasn't confirmed these are equivalent or safe.
-
Quality concerns: The FDA established import alerts to stop GLP-1 ingredients with "potential quality concerns" from entering the U.S.
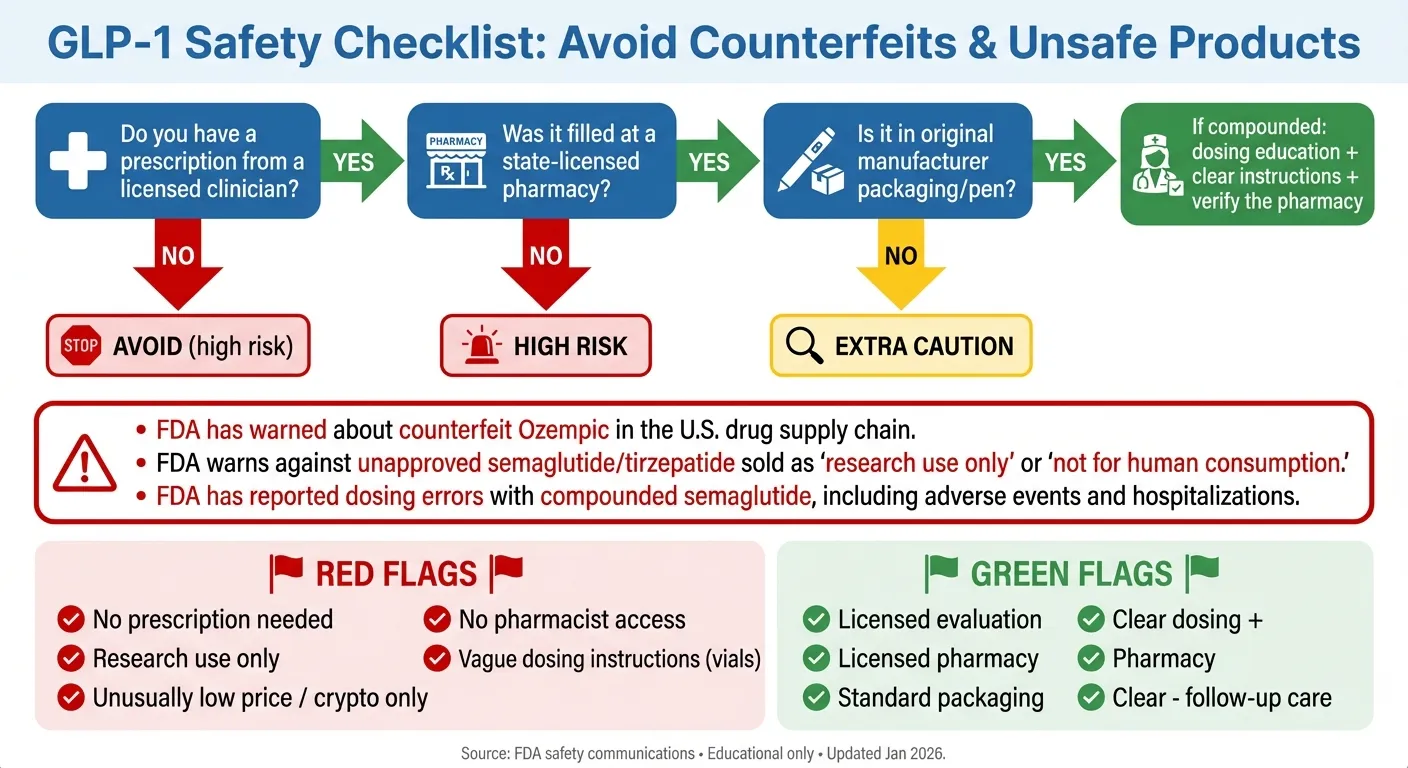
The "Legit Prescription Path" Checklist
To get GLP-1 medications safely:
LEGITIMATE PATH: ✅ Evaluation by a licensed healthcare provider (in-person or legitimate telehealth) ✅ Discussion of medical history, current medications, and contraindications ✅ Prescription written for an FDA-approved medication ✅ Prescription filled at a licensed pharmacy (verify at nabp.pharmacy) ✅ Medication arrives in original manufacturer packaging ✅ Ongoing follow-up with your provider
RED FLAGS (AVOID): ❌ "No prescription needed" ❌ Prices dramatically below market rates ❌ Claims of "research grade" or "peptides for research only" ❌ Pressure to buy immediately ❌ Unable to verify the pharmacy's license ❌ Product arrives in non-standard packaging ❌ Unable to reach customer service with questions
What About Telehealth Companies?
Many legitimate telehealth companies now prescribe GLP-1 medications. This can be convenient and appropriate if:
- They require a real medical evaluation (not just a questionnaire)
- They're staffed by licensed healthcare providers
- They prescribe FDA-approved medications (not compounded)
- They fill prescriptions through licensed pharmacies
- They provide ongoing follow-up care
Be cautious of companies that seem to approve everyone instantly or don't ask about your medical history.
Managing Side Effects
Most people experience some side effects on GLP-1s, especially during the first weeks. Here's how to handle them.
Side Effect Triage Table
| Symptom | Likely Cause | What to Try First | Call Your Doctor If | Seek Urgent Care If |
|---|---|---|---|---|
| Mild nausea | Normal adjustment | Smaller meals, ginger, peppermint | Lasts more than 2 weeks or prevents eating | Severe vomiting, can't keep fluids down |
| Constipation | Slowed gut motility | More fiber, water, gentle activity | No improvement after 1 week of trying remedies | Severe abdominal pain, no bowel movement for 5+ days |
| Diarrhea | GI adjustment | BRAT diet, hydration | Lasts more than a few days, signs of dehydration | Blood in stool, severe cramping |
| Fatigue | Common early side effect | Rest, stay hydrated, light activity | Persists beyond first few weeks | Confusion, severe weakness |
| Injection site reaction | Local irritation | Rotate injection sites, ice | Spreading redness, warmth | Signs of infection, severe swelling |
| "Sulfur burps" | Delayed gastric emptying | Smaller meals, avoid trigger foods | Very bothersome and not improving | N/A |
The Side Effect Reduction Playbook
Week 1-4 (Starting the medication):
- Eat smaller portions at each meal
- Avoid high-fat and greasy foods
- Stay very well hydrated
- Expect some nausea—it usually peaks and then improves
- Have bland foods available (crackers, toast, bananas)
During dose increases:
- Give your body 2-4 weeks to adjust at each dose before increasing
- If side effects are severe, ask your doctor about staying at the current dose longer
- Consider timing your dose increase for a weekend or when you can rest
Ongoing management:
- Learn your trigger foods and avoid them
- Eat slowly and stop when satisfied (you'll feel full faster)
- Don't lie down immediately after eating
- For constipation: fiber + water + movement is the formula
- For nausea: ginger tea, peppermint, small frequent meals
The Surgery/Procedure Warning (Important)
GLP-1 medications slow gastric emptying—meaning food stays in your stomach longer. This creates a risk during anesthesia: if your stomach isn't empty, you could aspirate (inhale stomach contents into your lungs).
What you must do:
- Tell ALL your healthcare providers that you take a GLP-1 medication
- Follow pre-procedure instructions carefully — your team may adjust the plan (e.g., medication hold or a pre-procedure liquid diet) depending on your risk
- Discuss with your surgeon or anesthesiologist about the best approach for your situation
The American Society of Anesthesiologists recommends discussing GLP-1 use with your surgical team before any procedure involving sedation or anesthesia.
What Happens If I Stop?
Let's address the elephant in the room: weight regain after stopping GLP-1 medications.
What the Research Shows
STEP 1 Extension Study (Semaglutide):
- Patients who stopped semaglutide regained about 2/3 of lost weight within 1 year
- Appetite returned to pre-medication levels
- Improvements in blood pressure, cholesterol, and blood sugar partially reversed
SURMOUNT-4 Study (Tirzepatide):
- Patients who switched to placebo after 36 weeks regained weight
- Patients who continued medication maintained their loss
- The difference was stark: continuation works, stopping doesn't
Why Regain Happens (It's Not Your Fault)
GLP-1 medications override your body's natural appetite signals. They don't permanently change those signals. When you stop the medication:
- Your appetite returns to baseline (or close to it)
- The "food noise" comes back
- Satiety signals weaken
- Your body's drive to regain lost weight kicks in
This is biology, not moral failure. Obesity is now recognized as a chronic disease that often requires ongoing treatment—just like high blood pressure or diabetes.
Strategies for Long-Term Success
If you stay on medication (most common approach):
- Some patients reduce to a lower "maintenance dose" after reaching their goal
- Continue lifestyle habits that support weight maintenance
- Regular follow-up with your provider
- Adjust dose as needed over time
If you want to try stopping (discuss with your doctor first):
- Taper gradually rather than stopping abruptly
- Have a solid nutrition and exercise foundation in place
- Consider working with a dietitian or behavioral coach
- Monitor weight closely and be prepared to restart if needed
- Set a "red line" weight where you'll consider resuming medication
Lifestyle factors that help either way:
- Resistance training (preserves muscle, supports metabolism)
- Adequate protein intake (1.0-1.5 g/kg body weight)
- Regular physical activity (150+ minutes/week)
- Sleep optimization (7-9 hours)
- Stress management
- Behavioral support or coaching
Cost and Coverage
Let's get practical about money. For complete pricing information, see our GLP-1 cost guide.
Understanding Your Options
Step 1: Check your insurance formulary
- Call your insurance company or check their website
- Ask specifically: "Is [medication name] covered for weight loss?"
- Ask: "What are the requirements?" (prior authorization, step therapy, etc.)
Step 2: Understand prior authorization
Most insurers require "prior authorization"—documentation that you meet their criteria. This often includes:
- Proof of BMI (from your doctor)
- Documentation of weight-related conditions
- Evidence of failed diet/exercise attempts
- Sometimes: proof of trying other treatments first ("step therapy")
Step 3: Work with your doctor's office
- They handle prior authorizations regularly
- They know what documentation insurers want
- They can appeal denials
Cost-Saving Options
Manufacturer savings programs:
- Novo Nordisk offers savings cards for Wegovy and Ozempic
- Eli Lilly offers savings for Zepbound and Mounjaro
- These can reduce copays significantly for commercially insured patients
Direct-to-consumer programs:
- LillyDirect: Zepbound self-pay vials at $299/month (2.5 mg), $399/month (5 mg), or $449/month (7.5-15 mg)
- Novo Nordisk direct programs: reported ~$349/month for Wegovy injection
- These bypass insurance but have fixed cash prices
The oral Wegovy advantage:
- At $149-299/month, it's the most affordable brand-name option
- May be worth considering even if your insurance covers injectables
Patient assistance programs:
- For uninsured or underinsured patients
- Income requirements vary
- Ask your doctor or contact manufacturers directly
What to avoid:
- Compounded versions (safety concerns, see above)
- "Too good to be true" online offers
- Products from unverified sources
The 2025-2026 Pricing Changes
The Trump administration announced deals with Eli Lilly and Novo Nordisk in November 2025:
- Target prices around $350/month for cash-pay patients
- Medicare/Medicaid coverage expansion for qualifying patients
- Target copays as low as $50/month for covered beneficiaries
Eligibility and rollout details vary, and the pricing applies under specific program terms. These changes are rolling out gradually. Ask your provider or pharmacist about current options.
GLP-1s Without Diabetes
Many people searching "GLP-1 pros and cons" don't have diabetes—they're interested purely in weight loss. Here's what's relevant for you.
FDA-Approved Options for Non-Diabetics
Specifically approved for weight loss (no diabetes required):
- Wegovy (semaglutide injection)
- Wegovy tablets (oral semaglutide)
- Zepbound (tirzepatide injection)
- Saxenda (liraglutide injection)
Approved for diabetes but often used off-label for weight loss:
- Ozempic (semaglutide injection)
- Mounjaro (tirzepatide injection)
What's Different for Non-Diabetics?
Blood sugar monitoring usually isn't needed. Unlike diabetes patients, you typically don't need to track your glucose levels.
Hypoglycemia risk is low. Without diabetes medications that lower blood sugar, the risk of dangerous low blood sugar is minimal.
Results may be similar or better. Some studies show non-diabetics have excellent weight loss results—possibly because there's no diabetes progression variable to complicate things.
Insurance may be harder. Many plans cover GLP-1s for diabetes but not for weight loss alone.
If You Have Prediabetes or Other Metabolic Risk Factors
If you have prediabetes or other metabolic risk factors, your clinician may discuss different medication options based on overall health risk—not just weight. Insurance coverage varies and typically depends on the drug's FDA indication and your plan's rules. Avoid any service that suggests misrepresenting diagnoses to obtain coverage.
Frequently Asked Questions
General Questions
Q: Are GLP-1 medications safe?
A: For most eligible adults, yes. GLP-1 medications are FDA-approved and have been studied extensively. Common side effects (nausea, constipation, diarrhea) are usually manageable. Serious side effects are uncommon. However, they're not safe for everyone—people with a history of medullary thyroid cancer, MEN2 syndrome, or severe allergic reactions should not use them. Always discuss your full medical history with your healthcare provider.
Q: How long do I have to take GLP-1 medications?
A: Current evidence suggests most people need to take them long-term—potentially for life—to maintain weight loss. Studies show that most patients regain weight within a year of stopping. Some patients may be able to reduce to a lower maintenance dose. Think of it like blood pressure medication: it works while you take it.
Q: Do GLP-1 medications cause cancer?
A: GLP-1 medicines carry a boxed warning about thyroid C-cell tumors in rodents; it's unknown whether this applies to humans. Because of this, these drugs are contraindicated if you or a close family member has medullary thyroid carcinoma (MTC) or MEN2. If you have concerns about cancer risk, discuss your personal and family history with your clinician.
Q: What happens if I stop taking my GLP-1?
A: Most people regain weight. In the STEP 1 extension study, participants regained about two-thirds of lost weight within one year of stopping semaglutide. Appetite returns to baseline. Cardiometabolic improvements may partially reverse. This is why these medications are typically considered long-term treatment.
Q: Can I drink alcohol while taking GLP-1 medications?
A: There's no direct drug interaction, but alcohol can worsen nausea and other GI side effects, adds empty calories, and may affect blood sugar if you have diabetes. Many patients report reduced interest in alcohol while on GLP-1s. Moderate consumption is generally acceptable, but discuss with your provider.
Side Effects and Safety
Q: What are the most common side effects?
A: Gastrointestinal effects: nausea (~25-44%, varies by dose and drug), vomiting, diarrhea, constipation, and bloating. These are usually worst during the first weeks and during dose increases, then improve as your body adjusts. Eating smaller, lower-fat meals and staying hydrated helps. Read our complete GLP-1 side effects guide for management strategies.
Q: What are the long-term side effects?
A: Most side effects are short-term. Long-term considerations include potential muscle loss (mitigated by exercise and protein), possible bone density changes with sustained weight loss, and uncommon serious events (pancreatitis, gallbladder disease). We're still learning about effects over decades of use.
Q: Do GLP-1s cause muscle loss?
A: Yes, 26-40% of weight lost on GLP-1s can be muscle rather than fat. This can be significantly reduced with resistance training and adequate protein intake. Patients who prioritize exercise can lose mostly fat while preserving or even gaining muscle.
Q: What is "Ozempic face" and is it a real side effect?
A: "Ozempic face" refers to facial volume loss and a gaunt appearance that some people notice after rapid weight loss on GLP-1 medications. It's not unique to semaglutide or any specific medication—it happens with any rapid weight loss. Slower weight loss, adequate protein intake, and maintaining hydration may help. Dermal fillers are an option for those concerned about facial volume loss. For a complete guide, see our detailed article on Ozempic face.
Q: Is it true GLP-1s can cause suicidal thoughts?
A: FDA reviews have not found evidence of an increased risk; in January 2026, FDA requested removal of suicidal behavior/ideation warning language from Wegovy, Saxenda, and Zepbound labeling. Patients should still report new or worsening mood symptoms to their prescriber.
Q: What should I do before surgery if I'm on a GLP-1?
A: Tell your surgical team that you take a GLP-1 medication. These drugs slow stomach emptying, which can increase aspiration risk during anesthesia. You may need to stop the medication before procedures and follow extended fasting instructions. Never skip this conversation.
Q: Are GLP-1 side effects worse for women?
A: Some real-world analyses suggest women report nausea/vomiting more often than men; the size of the difference varies by study. This may be due to differences in hormone levels and GLP-1 receptor expression. Despite higher side effect rates, women typically achieve greater weight loss.
Choosing and Using GLP-1s
Q: Which GLP-1 is best for weight loss?
A: Tirzepatide (Zepbound) produces the most weight loss in clinical trials (18-22%). Semaglutide (Wegovy) has the strongest cardiovascular protection data. Oral Wegovy is the most affordable. The "best" choice depends on your priorities, insurance coverage, and individual response.
Q: Which GLP-1 has the least side effects?
A: No clear winner. All GLP-1 medications cause similar GI side effects through similar mechanisms. Individual responses vary—some people tolerate one medication better than another. Slow dose titration (starting low and increasing gradually) is the most effective way to minimize side effects regardless of which medication you choose.
Q: Can I take GLP-1 medications if I don't have diabetes?
A: Yes. Wegovy, Zepbound, and Saxenda are FDA-approved specifically for weight loss in people without diabetes. Eligibility is based on BMI and weight-related health conditions, not diabetes status.
Q: Pills vs. injections—which is better?
A: Neither is objectively better; they have different trade-offs. The oral Wegovy pill is cheaper and more convenient for travel but requires strict timing (empty stomach, 30-minute wait before eating). Injections are once weekly and don't have timing restrictions but require refrigeration and needle use. Effectiveness appears similar.
Cost and Access
Q: How much do GLP-1 medications cost?
A: Without insurance: ~$1,000+/month for injections; $149-299/month for oral Wegovy. With good insurance: $25-150/month. Direct-pay programs: Zepbound self-pay vials are typically $299/month (2.5 mg), $399/month (5 mg), and $449/month (7.5-15 mg); Wegovy injection ~$349/month through manufacturer programs. Prices are changing with recent manufacturer deals—ask your provider about current options. See our complete GLP-1 cost guide for details.
Q: Does insurance cover GLP-1 medications?
A: It varies dramatically. In one survey, 36% of employer plans cover GLP-1s for both diabetes and weight loss; 55% cover them for diabetes only. Other analyses show different rates. Medicare is expanding coverage under new 2025-2026 policies. Medicaid coverage varies by state. Prior authorization is usually required. Check with your specific insurance plan.
Q: Are compounded GLP-1s safe?
A: The FDA has issued multiple warnings about compounded semaglutide and tirzepatide, including dosing errors causing hospitalizations, fraudulent labels, and unapproved chemical forms. If you choose a compounded product, understand you're accepting additional risks that don't exist with manufacturer products.
Q: How do I avoid counterfeit GLP-1 medications?
A: Get prescriptions from licensed healthcare providers. Fill prescriptions at licensed pharmacies (verify at nabp.pharmacy). Inspect packaging for errors. Be suspicious of dramatically low prices. Avoid "no prescription needed" offers. The FDA has documented counterfeit products in the U.S. supply chain.
Alternatives and Maintenance
Q: What if I can't afford or access GLP-1 medications?
A: Options include: oral Wegovy (most affordable brand-name), manufacturer savings programs, patient assistance programs, or discussing other weight loss medications with your doctor (phentermine, contrave, etc.). Bariatric surgery may be more cost-effective long-term for some patients. Lifestyle changes alone work for some people, though success rates are lower.
Q: Can I stop taking GLP-1s once I reach my goal weight?
A: You can, but most people regain weight. If you want to try stopping, work with your doctor to taper gradually, have strong lifestyle habits in place, and monitor your weight closely with a plan to restart if needed.
The GLP-1 Decision Kit
Use this framework to organize your thinking before talking to your doctor.
Step 1: Confirm Basic Eligibility
Do you meet BMI criteria?
- BMI ≥30: Yes, you meet the primary criterion
- BMI 27-29.9: You may qualify if you have a weight-related condition (list below)
- BMI <27: GLP-1s are generally not indicated
Check your eligibility with our GLP-1 eligibility quiz.
Weight-related conditions that may qualify you with BMI 27-29.9:
- Type 2 diabetes or prediabetes
- High blood pressure
- High cholesterol or triglycerides
- Obstructive sleep apnea
- Heart disease or history of heart attack/stroke
- Fatty liver disease
- Osteoarthritis related to weight
- PCOS
Step 2: Check for Contraindications
Hard stops (do NOT use GLP-1s if you have any of these):
- Personal or family history of medullary thyroid cancer
- MEN2 syndrome
- Previous severe allergic reaction to a GLP-1 medication
- Currently pregnant or planning pregnancy (for semaglutide, stop at least 2 months before)
- Type 1 diabetes
- Diabetic ketoacidosis
Caution areas (requires discussion with your doctor):
- History of pancreatitis
- Severe gastroparesis or GI disease
- Severe kidney disease
- Gallbladder disease
- Diabetic retinopathy
- Taking insulin or sulfonylureas
- Breastfeeding
- History of depression or suicidal thoughts
Review the complete list of GLP-1 contraindications.
Step 3: Assess Your Readiness
Rate yourself 1-5 on each factor (5 = very ready):
| Factor | Your Score (1-5) |
|---|---|
| I've genuinely tried diet and exercise for 6+ months | ___ |
| I understand this is likely long-term treatment | ___ |
| I can afford the medication or have a coverage plan | ___ |
| I'm willing to make lifestyle changes alongside medication | ___ |
| I can commit to regular follow-up appointments | ___ |
| I'm prepared to manage potential side effects | ___ |
Total Score: ___/30
- 25-30: You're likely ready to discuss GLP-1s with your doctor
- 18-24: Consider which areas need attention before starting
- Below 18: You may benefit from addressing readiness factors first
Step 4: Choose Your Priority
What matters most to you? Rank these 1-5 (1 = most important):
| Priority | Your Rank |
|---|---|
| Maximum weight loss | ___ |
| Lowest side effects | ___ |
| Lowest cost | ___ |
| Proven heart protection | ___ |
| Convenience (pill vs. injection) | ___ |
Based on your #1 priority:
- Maximum weight loss → Discuss Zepbound (tirzepatide)
- Heart protection → Discuss Wegovy (semaglutide)
- Lowest cost → Discuss oral Wegovy
- Convenience (no needles) → Discuss oral Wegovy
Step 5: Questions for Your Doctor
Bring these questions to your appointment:
- Based on my health history, am I a good candidate for GLP-1 medications?
- Which specific medication do you recommend for my situation, and why?
- What will my insurance cover, and what will I pay out of pocket?
- How will we handle side effects if they occur?
- What lifestyle changes should I make alongside the medication?
- How often will I need follow-up appointments?
- What's the plan if this medication doesn't work for me?
- What should I do before any upcoming procedures or surgeries?
Our Methodology
Sources
This guide is based on:
- FDA prescribing information for each medication (accessdata.fda.gov)
- FDA safety communications about GLP-1 medications
- Peer-reviewed clinical trials (STEP, SURMOUNT, SELECT, SUSTAIN series)
- Published meta-analyses from medical journals
- Official statements from Novo Nordisk and Eli Lilly
- Guidelines from medical organizations (ADA, Obesity Society, WHO)
- Government sources (CMS, White House fact sheets on pricing)
How We Evaluate Evidence
| Evidence Type | How We Treat It |
|---|---|
| Large randomized controlled trials | Highest confidence |
| FDA prescribing information | Authoritative source |
| Published meta-analyses | High confidence |
| Observational studies | Moderate confidence; note limitations |
| Case reports/anecdotes | Low confidence; mentioned only for context |
| Expert opinion | Noted as opinion, not fact |
Update Policy
- This guide is reviewed monthly
- We update immediately when FDA labels or safety communications change
- Pricing is verified quarterly
- All updates are logged below
Update Log
| Date | What Changed |
|---|---|
| January 2026 | Initial publication |
The Bottom Line
GLP-1 medications represent a genuine breakthrough in weight management. For people who meet the eligibility criteria and don't have contraindications, they offer:
- Significant, clinically meaningful weight loss (mid-teens to low-20% in trials)
- Reduced appetite and "food noise"
- Improvements in blood sugar, blood pressure, and heart health
- Multiple options to fit different needs and budgets
But they're not magic pills. They come with:
- Common (though usually manageable) side effects
- Significant costs and insurance complexity
- The need for long-term commitment
- Uncommon but serious risks that require medical supervision
The decision framework is simple:
- Do you meet the eligibility criteria?
- Do you NOT have any contraindications?
- Are you ready for long-term treatment alongside lifestyle changes?
- Can you access and afford the medication?
- Are you willing to work with a healthcare provider for monitoring?
If you answered yes to all five questions, GLP-1 medications are worth discussing with your doctor.
If you answered no to any question, that's the area to address first—whether it's exploring different coverage options, building readiness for lifestyle changes, or finding a different approach altogether.
Either way, you now have the information you need to make an informed decision. That's what this guide was designed to provide.
Citations and Sources
- FDA Prescribing Information: Wegovy (semaglutide injection)
- FDA Prescribing Information: Wegovy (semaglutide tablets)
- FDA Prescribing Information: Zepbound (tirzepatide)
- FDA Prescribing Information: Ozempic (semaglutide)
- FDA Prescribing Information: Mounjaro (tirzepatide)
- Wilding JPH, et al. STEP 1: Semaglutide 2.4 mg for Weight Management. N Engl J Med. 2021
- Jastreboff AM, et al. SURMOUNT-1: Tirzepatide for Weight Management. N Engl J Med. 2022
- Aronne LJ, et al. SURMOUNT-5: Tirzepatide vs Semaglutide. N Engl J Med. 2025
- Lincoff AM, et al. SELECT: Semaglutide and Cardiovascular Outcomes. N Engl J Med. 2023
- Wilding JPH, et al. Weight regain after withdrawal of semaglutide. Diabetes Obes Metab. 2022
- Aronne LJ, et al. SURMOUNT-4: Tirzepatide maintenance. JAMA. 2024
- FDA: Concerns with Unapproved GLP-1 Drugs
- FDA: Counterfeit Ozempic Warning
- FDA: Dosing Errors with Compounded Semaglutide
- FDA: Requests Removal of Suicidal Behavior/Ideation Warning from GLP-1 RA Labels (Jan 2026)
- Washington University: Study Identifies Benefits, Risks Linked to Popular Weight Loss Drugs
- Gasoyan H, et al. Real-world GLP-1 outcomes. Obesity (Silver Spring). 2025.
- EBRI: GLP-1 Coverage and Impact on Employment-Based Health Plan Premiums
- Novo Nordisk: Wegovy Pill Availability Announcement (Jan 2026)
- Reuters: Novo Nordisk Wins US Approval for Weight-Loss Pill (Dec 2025)
How we rank + verify
Last verified: March 3, 2026
What we verified: FDA prescribing information for Wegovy, Ozempic, Rybelsus, Mounjaro, Zepbound, Saxenda, and Victoza. Clinical trial data from STEP, SURMOUNT, SCALE, and SELECT trials. FDA safety communications. Peer-reviewed research and meta-analyses.
Sources: FDA drug labels accessed January 2026, New England Journal of Medicine trial publications, JAMA meta-analyses, CMS and government pricing announcements, peer-reviewed studies from PubMed
Related Articles
Complete GLP-1 side effects guide from FDA labels: what's normal, what's serious, and how to manage symptoms on Ozempic, Wegovy, Mounjaro, Zepbound.
GLP-1 contraindications explained: FDA Section 4 lists MTC/MEN2 history and serious hypersensitivity. Learn what's a real contraindication vs warning.
How GLP-1 medications like Ozempic and Wegovy work for weight loss. Mechanism map, clinical trial results, side effects, and decision framework.
GLP-1 cost breakdown for 2026. Real prices for Wegovy, Zepbound, Ozempic with insurance, cash-pay, and Medicare options. Updated January 2026.
Compounded GLP-1 vs name brand: FDA approval, safety, real costs, and legality explained. Unbiased 2026 decision guide with pricing verified January 2026.
This content is educational only and does not replace professional medical advice. Always consult a qualified healthcare provider before starting any medication.