Disclosure: Some links on this site are affiliate links. If you purchase through these links, we may earn a commission at no extra cost to you. Thank you for supporting our site.·For informational purposes only—not medical advice.
Verified against FDA prescribing information | Sources: FDA.gov, NEJM, NCBI StatPearls | Written by WPG Research Team
Tirzepatide Dosing Schedule: Complete Week-by-Week Chart (2.5 mg to 15 mg)
The tirzepatide dosing schedule starts at 2.5 mg once per week and increases by 2.5 mg every four weeks until you reach your maintenance dose — typically somewhere between 5 mg and 15 mg. That starting dose isn't your treatment dose. It exists so your body can adjust to the medication gradually and side effects stay manageable.
Here's what most people actually want to know: the schedule is straightforward, the confusion around “units” is fixable (we'll clear that up below), and yes — tirzepatide works. In the largest clinical trial (SURMOUNT-1), people lost an average of 15–21% of their body weight depending on dose, over 72 weeks.
Below you'll find the official dosing chart, what each dose level actually does, how to convert mg to syringe units if you're using compounded tirzepatide, what to do if you miss a dose, and realistic expectations at every stage. Bookmark this page — it covers everything your provider explained in three minutes that you need to actually remember.
Image is for illustrative purposes only and does not constitute medical advice.
The Official Tirzepatide Dosing Schedule (FDA-Approved)
This is the standard dose escalation for both Zepbound (weight loss) and Mounjaro (type 2 diabetes). Your clinician may adjust the pace based on how you respond.
| Weeks | Weekly Dose | Purpose | Notes |
|---|---|---|---|
| 1–4 | 2.5 mg | Initiation only | Not a maintenance dose — your body is adjusting |
| 5–8 | 5 mg | First maintenance option | Lowest therapeutic dose for weight loss |
| 9–12 | 7.5 mg | Escalation (if needed) | Only increase if tolerated and more results needed |
| 13–16 | 10 mg | Maintenance option | Recommended maintenance for sleep apnea (OSA) |
| 17–20 | 12.5 mg | Escalation (if needed) | Some people find their sweet spot here |
| 21+ | 15 mg | Maximum dose | Highest approved dose for all indications |
Source: Zepbound prescribing information (FDA). Mounjaro follows the same escalation pattern.
Note: The 15 mg maximum applies to adults. For pediatric Mounjaro patients (ages 10+), the maximum recommended dose is 10 mg once weekly.
Three rules that matter most:
- Increase only by 2.5 mg at a time — never skip a dose level.
- Wait at least 4 weeks between increases.
- Maximum dose is 15 mg weekly — going higher doesn't help and increases risk.
Not everyone will reach 15 mg. Many people get excellent results at 5 mg or 10 mg, and your provider will find the dose that balances weight loss with how you feel. The “best” dose is the one you can sustain.
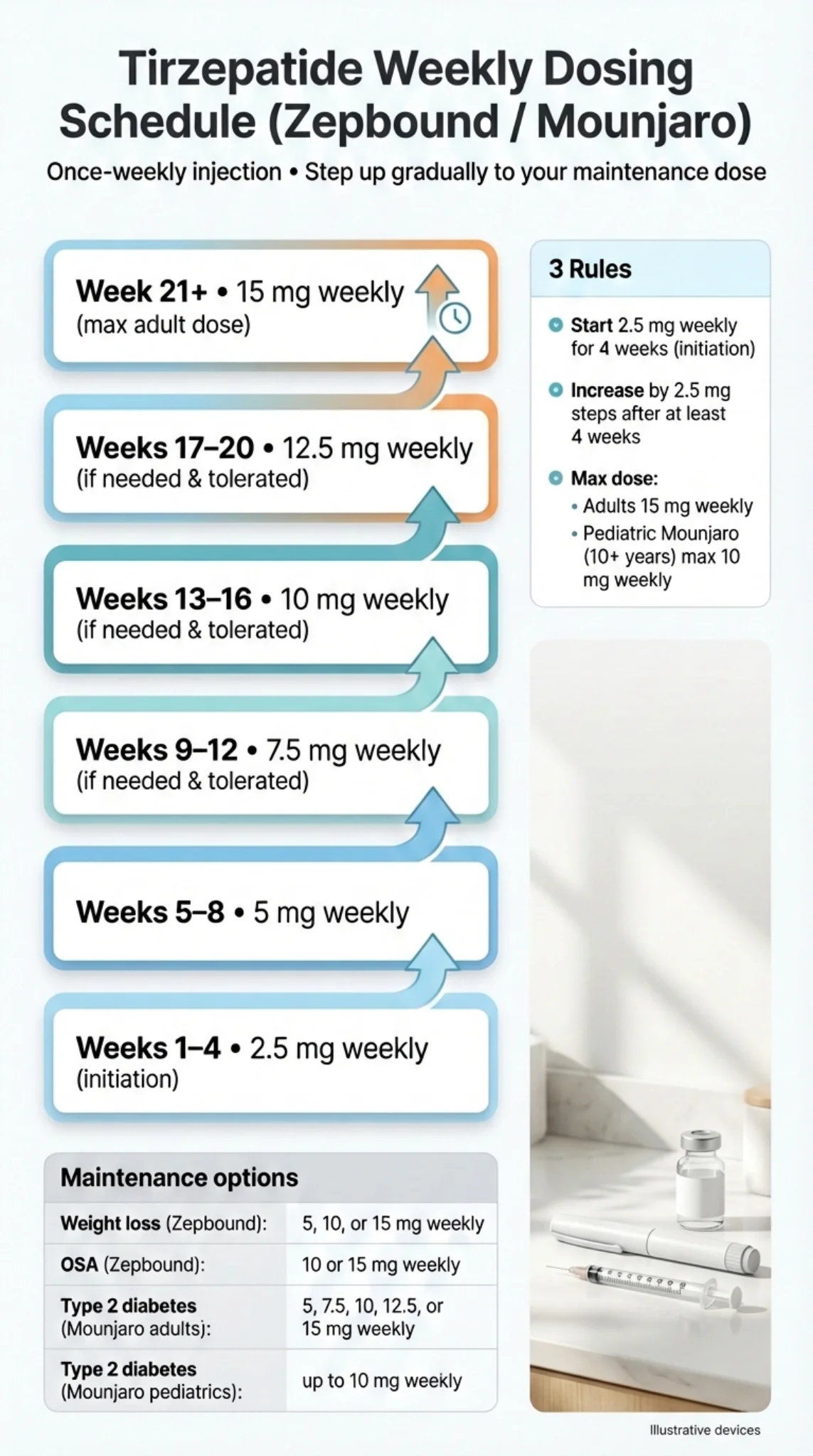
Image is for illustrative purposes only and does not constitute medical advice.
How Dose Escalation Actually Works (And Why You Start So Low)
If you're staring at your first 2.5 mg pen wondering whether it'll do anything — fair question. The honest answer: probably not much in terms of weight loss. And that's by design.
The 2.5 mg dose is explicitly not intended as a treatment dose. The FDA label for both Zepbound and Mounjaro states it's for “treatment initiation” only. Its job is to introduce tirzepatide to your system gradually so the GI side effects (mainly nausea and diarrhea) don't hit you full force.
Tirzepatide is a dual GIP/GLP-1 receptor agonist — it activates two hormone receptors simultaneously, which is part of why it's so effective but also why your digestive system needs time to adjust. The slow ramp-up reduces the likelihood of the intense nausea that made people quit older GLP-1 medications.
Here's how the escalation logic works:
Your provider starts you at 2.5 mg. After four weeks (minimum), they bump you to 5 mg. From there, every four weeks they assess two things: are you tolerating the current dose, and do you need more? If you're losing weight and side effects are manageable, they may hold you at your current dose. If results have plateaued and you're handling it well, they'll increase by 2.5 mg.
This process can take anywhere from 4 weeks (if you settle at 5 mg) to 20+ weeks (if you titrate all the way to 15 mg). There's no rush. Faster escalation doesn't mean faster weight loss — it usually just means worse nausea.
One thing nobody tells you early enough: the first 2–4 weeks on any new dose are typically the roughest for side effects. If you increase to 7.5 mg and feel terrible for a week, that doesn't mean you need to drop back — it usually means your body is still adapting. Most side effects fade significantly by week 2–3 at a given dose. Your provider can help you decide whether to push through or step back.
Tirzepatide Dosing for Weight Loss (Zepbound)
Zepbound is the FDA-approved brand of tirzepatide specifically for weight management. It's indicated for adults with a BMI of 30 or higher (obesity), or BMI of 27 or higher (overweight) with at least one weight-related condition like high blood pressure, type 2 diabetes, or sleep apnea.
Maintenance doses for weight loss: 5 mg, 10 mg, or 15 mg weekly.
Maintenance doses for obstructive sleep apnea (OSA): 10 mg or 15 mg weekly. The 5 mg maintenance option is not approved for OSA — you'll need to reach at least 10 mg.
Available Forms
| Format | Dose Strengths | Volume Per Dose | Key Detail |
|---|---|---|---|
| Single-dose pen | 2.5, 5, 7.5, 10, 12.5, 15 mg | 0.5 mL each | One injection, then discard |
| Single-dose vial | 2.5, 5, 7.5, 10, 12.5, 15 mg | 0.5 mL each | Used with a separate syringe |
| KwikPen (multi-dose) | 2.5, 5, 7.5, 10, 12.5, 15 mg | 0.6 mL per dose | Contains 4 weekly doses |
| Multi-dose vial | 2.5, 5, 7.5, 10, 12.5, 15 mg | 0.6 mL per dose | Contains 4 weekly doses |
Source: Zepbound prescribing information, FDA.gov. Eli Lilly manufactures all forms.
If you're using a single-dose pen, dosing is simple — each pen delivers one fixed dose and there's nothing to measure. If you're using a single-patient-use KwikPen, it contains four weekly doses — follow the KwikPen Instructions for Use for each injection. If you're using a vial, you'll draw the correct volume (0.5 mL for single-dose vials, 0.6 mL for multi-dose vials) using a syringe your provider prescribes.
Tirzepatide Dosing for Type 2 Diabetes (Mounjaro)
Mounjaro uses the same active ingredient (tirzepatide) and follows the same escalation pattern, but it's FDA-approved for type 2 diabetes, not weight loss.
The key difference: with Mounjaro, dose escalation decisions are driven primarily by blood sugar control (A1C levels), not the scale. The 2.5 mg starting dose is explicitly “not intended for glycemic control” per the label — it's still just an initiation dose.
Mounjaro is also now approved for pediatric patients ages 10 and older with type 2 diabetes, following the same dose escalation logic. However, the maximum recommended dose for pediatric patients is 10 mg once weekly (adults can go up to 15 mg).
Bottom line: if your doctor prescribed Mounjaro, the dosing schedule chart above applies to you too. The titration steps and timing are identical. The only difference: adults can go up to 15 mg, while pediatric patients max out at 10 mg.
How Much Weight Can You Realistically Expect to Lose?
This is the question behind the question. People searching “tirzepatide dosing schedule” aren't just looking for numbers on a chart — they want to know if those numbers will actually change their life. Here's what the clinical evidence says.
SURMOUNT-1 Trial Results (72 Weeks)
The SURMOUNT-1 trial enrolled 2,539 adults with obesity (without diabetes) and tracked outcomes over 72 weeks. All participants combined tirzepatide with a reduced-calorie diet and 150 minutes of weekly physical activity.
| Dose | Average Weight Loss | ≥10% | ≥20% |
|---|---|---|---|
| 5 mg | 15.0% (~34 lbs*) | 68.5% | 30.0% |
| 10 mg | 19.5% (~44 lbs*) | 78.1% | 50.1% |
| 15 mg | 20.9% (~48 lbs*) | 83.5% | 56.7% |
| Placebo | 3.1% (~7 lbs*) | 18.8% | 3.1% |
*Approximate pounds based on the trial's average starting weight of ~231 lbs. Your actual results depend on starting weight, adherence, diet, exercise, and individual biology.
Source: Jastreboff AM, et al. “Tirzepatide Once Weekly for the Treatment of Obesity.” New England Journal of Medicine. 2022;387:205-216.
Tirzepatide vs. Semaglutide (Head-to-Head)
The SURMOUNT-5 trial directly compared tirzepatide to semaglutide (Wegovy/Ozempic) at maximum tolerated doses over 72 weeks. Tirzepatide produced a mean weight loss of 20.2% compared to 13.7% with semaglutide. Both are effective medications — tirzepatide consistently outperformed in this comparison.
Source: “Tirzepatide as Compared with Semaglutide for the Treatment of Obesity.” New England Journal of Medicine. 2025.
What This Actually Means For You
Higher dose generally means more weight loss, but with diminishing returns. The jump from 5 mg to 10 mg is bigger than the jump from 10 mg to 15 mg. If you're doing well at 10 mg, the extra bump to 15 mg may not be worth the additional side effects.
Even the lowest maintenance dose (5 mg) produced significant results. A 15% average body weight loss is meaningful — for a 230-pound person, that's about 35 pounds. Don't assume you “need” to reach 15 mg.
Results aren't instant. Most people notice reduced appetite and “food noise” quieting within 1–3 weeks. Visible weight loss typically starts showing around weeks 4–8. Results continue accumulating for up to 72 weeks in clinical data.
The medication doesn't work alone. Every trial combined tirzepatide with diet and exercise changes. The participants who lost the most weight weren't just injecting — they were eating a reduced-calorie diet and moving regularly.
Ready to start tirzepatide? Compare licensed telehealth providers offering clinician-guided dosing support — including side-effect management and regular check-ins through your entire titration.
Compare Tirzepatide ProvidersTirzepatide Dosing in Units and mL — The Confusion That Actually Matters
If you've been prescribed compounded tirzepatide (or you're using a vial with a syringe), you've probably hit the wall that trips up almost everyone: your prescription says milligrams, but your syringe is marked in “units.” They are not the same thing.
This confusion isn't just annoying — it's a safety issue. Drawing the wrong number of units from a vial can mean taking half your intended dose (wasted money, poor results) or double your intended dose (serious side effects).
The Basics: mg vs. mL vs. Units
Milligrams (mg) = the amount of medication. This is what your doctor prescribes: “Take 5 mg weekly.”
Milliliters (mL) = the volume of liquid you inject. How many mL you need depends on the concentration of your vial.
Units = markings on an insulin syringe that measure volume. On a standard U-100 insulin syringe, 100 units = 1 mL. So 50 units = 0.5 mL, 25 units = 0.25 mL, and so on.
Units are not a measure of medication strength. They're just a way to measure how much liquid you're drawing into the syringe.
Why There's No Safe “Universal Units Chart”
Here's the part most websites get wrong — and it matters.
Different vials have different concentrations (mg/mL). A vial labeled 10 mg/mL contains 10 milligrams of tirzepatide in every milliliter of liquid. A vial labeled 20 mg/mL contains 20 milligrams per milliliter — it's twice as concentrated.
That means 25 units from a 10 mg/mL vial gives you 2.5 mg of tirzepatide. But 25 units from a 20 mg/mL vial gives you 5 mg — double the dose from the same syringe reading.
If you switch pharmacies or your pharmacy changes concentrations, using the same number of units will give you a completely different dose. This is why any website that gives you a single units chart without asking for your concentration is potentially dangerous.
The Formula (Memorize This)
Volume (mL) = Prescribed Dose (mg) ÷ Concentration (mg/mL)
Syringe Units = Volume (mL) × 100 (for a standard U-100 insulin syringe)
That's it. Two steps. Works for every vial you'll ever encounter.
Units Conversion Table: 10 mg/mL Concentration
If your vial label says 10 mg/mL:
| Prescribed Dose | Volume to Draw | Insulin Syringe Units |
|---|---|---|
| 2.5 mg | 0.25 mL | 25 units |
| 5 mg | 0.50 mL | 50 units |
| 7.5 mg | 0.75 mL | 75 units |
| 10 mg | 1.00 mL | 100 units (full syringe) |
| 12.5 mg | 1.25 mL | Exceeds 1 mL (100-unit U-100 syringe capacity) |
| 15 mg | 1.50 mL | Exceeds 1 mL (100-unit U-100 syringe capacity) |
If your calculated volume exceeds your syringe capacity, ask your prescriber or pharmacist whether to use a larger syringe or divide the dose into two injections.
Units Conversion Table: 20 mg/mL Concentration
If your vial label says 20 mg/mL:
| Prescribed Dose | Volume to Draw | Insulin Syringe Units |
|---|---|---|
| 2.5 mg | 0.125 mL | 12.5 units |
| 5 mg | 0.25 mL | 25 units |
| 7.5 mg | 0.375 mL | 37.5 units |
| 10 mg | 0.50 mL | 50 units |
| 12.5 mg | 0.625 mL | 62.5 units |
| 15 mg | 0.75 mL | 75 units |
Units Conversion Table: 30 mg/mL Concentration
If your vial label says 30 mg/mL:
| Prescribed Dose | Volume to Draw | Insulin Syringe Units |
|---|---|---|
| 2.5 mg | 0.083 mL | ~8 units |
| 5 mg | 0.167 mL | ~17 units |
| 7.5 mg | 0.25 mL | 25 units |
| 10 mg | 0.333 mL | ~33 units |
| 12.5 mg | 0.417 mL | ~42 units |
| 15 mg | 0.50 mL | 50 units |
For FDA-Approved Pens (Zepbound/Mounjaro)
If you're using a pre-filled pen, you do not need to calculate anything. Each pen delivers a fixed dose in 0.5 mL. The pen does the measuring for you.
If you're using the KwikPen (multi-dose), each dose is 0.6 mL — the pen also delivers this automatically.
The Safety Rule That Overrides Everything
If you are ever unsure about your dose, stop and call your prescriber or pharmacist before injecting. Never estimate. Never use someone else's conversion chart without confirming your vial's concentration matches. The few minutes it takes to verify could prevent a serious dosing error.
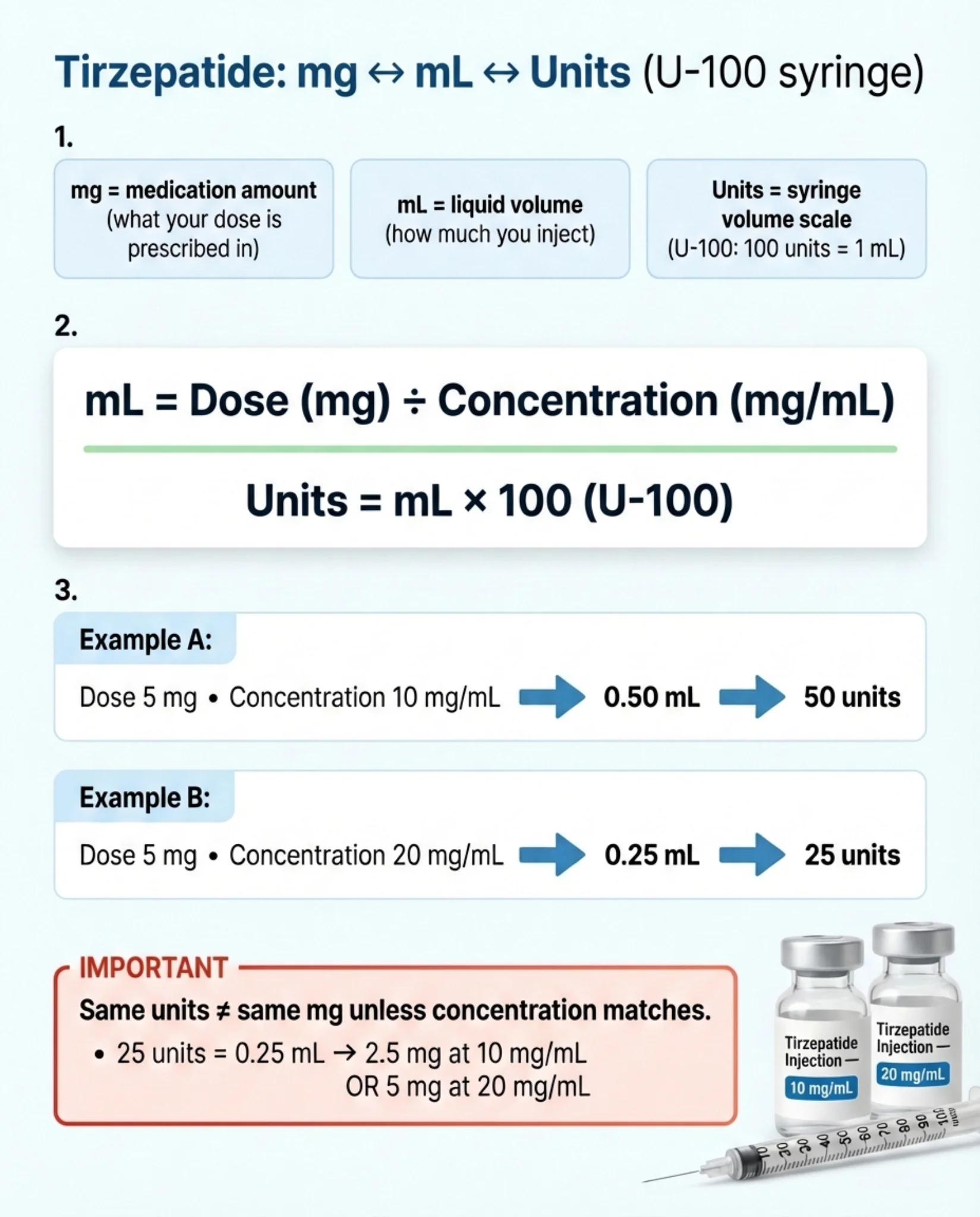
Image is for illustrative purposes only and does not constitute medical advice.
Compounded vs. Brand-Name Tirzepatide — What Changes With Dosing
Compounded tirzepatide contains the same active ingredient as Zepbound and Mounjaro, but it's mixed by a compounding pharmacy rather than manufactured by Eli Lilly. The dose escalation logic (2.5 mg → 5 mg → up to 15 mg, increasing by 2.5 mg every 4+ weeks) is the same in terms of milligrams.
What's different:
- Not FDA-approved. Compounded tirzepatide hasn't been tested in the large clinical trials that Zepbound and Mounjaro went through. Quality can vary between pharmacies.
- Concentrations aren't standardized. One pharmacy might compound at 10 mg/mL, another at 20 mg/mL, another at 60 mg/mL. This is exactly why the units-to-mg conversion is so confusing (and why the tables above exist).
- No pre-filled pens. Compounded tirzepatide typically comes in multi-dose vials that require drawing the correct volume with a syringe.
- Instructions may come in “units” only. Some pharmacies give dosing instructions as “inject 25 units” without telling you what that equals in mg. This is where mistakes happen. Always ask: “What is my dose in milligrams, and what is the concentration of my vial in mg/mL?”
- Regulatory landscape is changing. The FDA has taken steps regarding compounded GLP-1 medications. Check with your provider about current availability and regulations.
If you're using compounded tirzepatide, a safety checklist:
I know my prescribed dose in milligrams (not just units)
I know my vial's concentration in mg/mL (it's on the label)
I've calculated or confirmed the correct volume to draw
My pharmacy is licensed and follows sterile compounding standards
My vial has a clear beyond-use date and storage instructions
If you can't check all five, talk to your prescriber before your next injection.
What to Expect Week by Week on Tirzepatide
One of the biggest sources of anxiety is not knowing what “normal” looks like at each stage. Here's a realistic timeline based on clinical data and what providers commonly report.
Weeks 1–4 (2.5 mg — Initiation Phase)
What's happening: Your body is being introduced to tirzepatide for the first time. The medication is beginning to activate GLP-1 and GIP receptors.
What you'll likely notice: Mild appetite reduction in some people. Possibly some nausea, especially in the first few days. Many people feel almost nothing at this dose — and that's completely normal.
What you won't notice yet: Major weight loss. The scale might budge a few pounds (often water weight and reduced food intake), but don't expect dramatic changes. That's not what this phase is for.
Your job this month: Get into the routine. Pick your injection day, practice the injection, note any side effects to discuss with your provider, and start building the diet and exercise habits that will amplify your results at higher doses.
Weeks 5–8 (5 mg — First Therapeutic Dose)
What's happening: This is where the medication starts doing real work. Most people notice a meaningful reduction in appetite and food noise at this level.
What you'll likely notice: Eating less without trying as hard. Smaller portions feel satisfying. Some people describe this as “the volume gets turned down on food thoughts.” GI side effects may return or intensify briefly after the dose increase.
What to watch for: If nausea is significant, it usually peaks in the first week at 5 mg and improves by week 2–3. This is the dose where most people first feel the medication is “doing something.”
Weight loss: Many people start seeing 1–3 pounds per week of actual weight loss from this point forward.
Weeks 9–16 (7.5 mg → 10 mg — Escalation Phase)
What's happening: Your provider is titrating toward your optimal maintenance dose. Each 2.5 mg increase may bring a brief round of GI adjustment followed by stronger appetite suppression and continued weight loss.
What you'll likely notice: Progressively less hunger. Some people find they need to set reminders to eat because they simply don't think about food. Energy levels may improve as weight drops. Clothes start fitting differently.
Key decision point: Around 10 mg, many people and their providers assess whether the results justify continuing upward or staying put. If you're losing weight steadily with manageable side effects, 10 mg may be your long-term dose.
Weeks 17–24+ (12.5 mg → 15 mg — Maximum Phase)
What's happening: These are the highest approved doses. Not everyone reaches this phase — many stabilize earlier.
What you'll likely notice: Maximum appetite suppression. Some people report that eating becomes almost mechanical at these doses — you eat because you should, not because you're hungry. Side effects may be more pronounced than at lower doses.
Important: The jump from 10 mg to 15 mg produces less additional weight loss than the jump from 5 mg to 10 mg. If side effects are significantly worse at 12.5 or 15 mg, dropping back to 10 mg is completely reasonable and still produces excellent results.
The 5 Tirzepatide Dosing Rules Worth Memorizing
Save this. Screenshot it. Tape it to your fridge. These five rules cover 90% of the dosing questions that come up during treatment.
Start at 2.5 mg for 4 weeks.
This is for adjustment, not weight loss. Don't skip it.
Increase by 2.5 mg at a time.
Never jump from 5 mg to 10 mg. Always step up one level (2.5 mg increment) at a time.
Wait at least 4 weeks between increases.
Your body needs time to adjust at each dose. Rushing the escalation doesn't speed up weight loss — it just makes side effects worse.
Missed a dose? Use the 96-hour rule.
Less than 4 days missed? Take it now. More than 4 days? Skip it and resume on your regular day. Never double up.
Maximum dose is 15 mg per week.
Period. More isn't better — it just increases side effects without additional benefit.
These rules come directly from the FDA prescribing information and apply whether you're using Zepbound, Mounjaro, or compounded tirzepatide.
Storage, Travel, and Practical Tips
At Home
- •Store in the refrigerator between 36°F and 46°F (2°C to 8°C)
- •Keep in the original carton to protect from light
- •Never freeze. If your pen or vial has been frozen, discard it — the medication may be damaged
- •Don't store in the fridge door (temperature fluctuates too much) — keep it on a middle shelf
Traveling
- •Single-dose pens and single-dose vials: may be stored at room temperature (up to 86°F / 30°C) for up to 21 days. Multi-dose vials and KwikPens: follow the multi-dose discard rules below (discard after 30 days at room temp, 30 days after first use, or after 4 doses — whichever comes first)
- •Use a small insulated pouch with an ice pack for longer trips (don't let the ice pack directly touch the pen)
- •Bring your full prescription information and a letter from your provider if flying internationally
- •TSA allows injectable medications in carry-on bags — they do not need to go through checked luggage
- •If traveling across time zones, adjust your injection day if needed (remember: at least 72 hours between doses)
- •Never leave tirzepatide in a hot car — even briefly. Summer temperatures inside a parked car can exceed 150°F
Multi-Dose Vials (KwikPen or Multi-Dose Vial)
- •After first use, the multi-dose vial can be stored at room temperature (up to 86°F) or refrigerated
- •Discard after 30 days at room temperature, 30 days after first use, or after taking 4 weekly doses — whichever comes first, even if medication remains
Side Effects by Dose Level — What to Actually Expect
Here's the part that matters when you're deciding whether to move up to the next dose. Side effects are real, they're common, and they're almost always worst during the first few weeks of each dose increase.
Side Effect Rates From Clinical Trials
| Side Effect | 5 mg | 10 mg | 15 mg | Placebo |
|---|---|---|---|---|
| Nausea | 25% | 29% | 28% | 8% |
| Diarrhea | 19% | 21% | 23% | 8% |
| Vomiting | 8% | 11% | 13% | 2% |
| Constipation | 17% | 14% | 11% | 5% |
| Injection site reactions | 6% | 8% | 8% | 2% |
| Fatigue | 5% | 6% | 7% | 3% |
Source: Zepbound prescribing information, FDA label Table 1 (pooled Study 1 and Study 2).
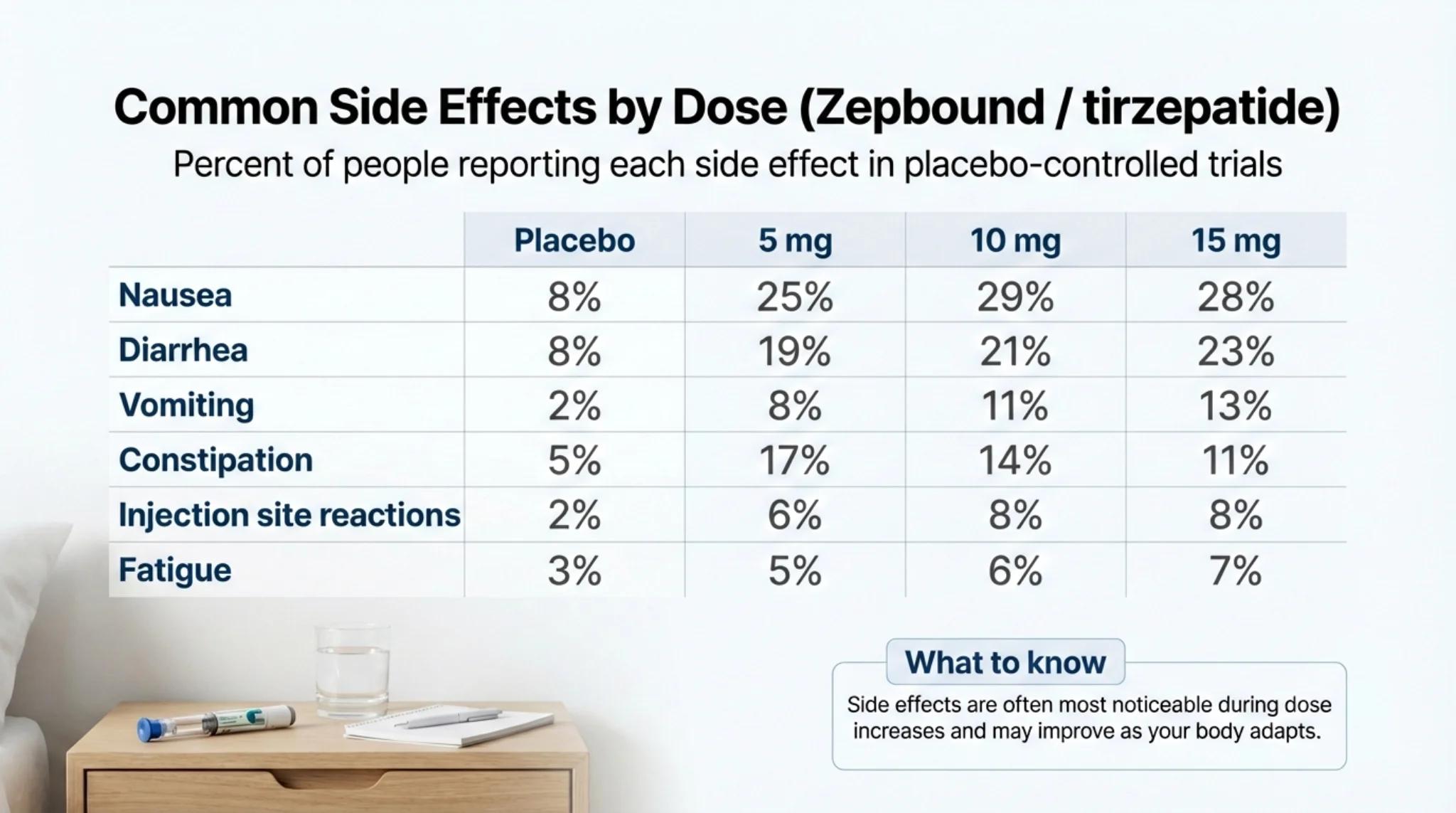
Image is for illustrative purposes only and does not constitute medical advice.
The Honest Take on Side Effects
In placebo-controlled trials, 6.7% of people on the highest dose (15 mg) discontinued Zepbound due to adverse reactions, compared to 3.4% with placebo. For the other 93%+, the side effects were manageable and usually temporary — peaking during dose escalation and fading as the body adjusted.
The most common experience: mild-to-moderate nausea for 3–7 days after increasing your dose, gradually fading by week 2–3. Some people describe it as “feeling full when you haven't eaten” rather than “about to be sick.” Others get more intense nausea that genuinely disrupts their day for a few days.
What usually helps:
- •Eat smaller, more frequent meals (4–5 small meals instead of 2–3 large ones)
- •Avoid greasy, fried, or heavy foods — especially during the first week at a new dose
- •Stay hydrated. This sounds obvious, but diarrhea and reduced food intake can dehydrate you faster than you'd expect
- •Eat slowly. Your stomach is emptying more slowly now. Eating fast can make nausea worse.
- •Ginger tea or ginger supplements may help with nausea (many providers recommend this)
When to call your provider immediately:
Severe abdominal pain that doesn't go away (could indicate pancreatitis)
Persistent vomiting that prevents you from keeping liquids down
Signs of an allergic reaction (rash, swelling, difficulty breathing)
Signs of low blood sugar if you're also on insulin or sulfonylureas (shakiness, confusion, sweating)
Yellowing of the skin or eyes (potential gallbladder or liver issue)
Can You Stay at a Lower Dose If Side Effects Are Bad?
Yes. This is an important point that gets lost in the “dose escalation” framing.
The FDA-approved maintenance doses for weight loss are 5 mg, 10 mg, or 15 mg. Not just 15 mg. If you're getting good results at 5 mg with minimal side effects, there's no requirement to go higher. If you escalated to 10 mg and the side effects are significantly worse, your provider may step you back to 7.5 mg or hold you at a dose that works.
The goal is finding the lowest effective dose that you can maintain long-term — not racing to the maximum.
What If You Miss a Dose?
This happens to everyone eventually. Here's the rule, directly from the prescribing information:
Less than 4 days (96 hours) since your missed dose? → Take it as soon as you remember. Then resume your regular schedule next week.
More than 4 days since your missed dose? → Skip it entirely. Take your next dose on your normal scheduled day.
Never take two doses within 3 days (72 hours) of each other. Never double up to make up for a missed dose.
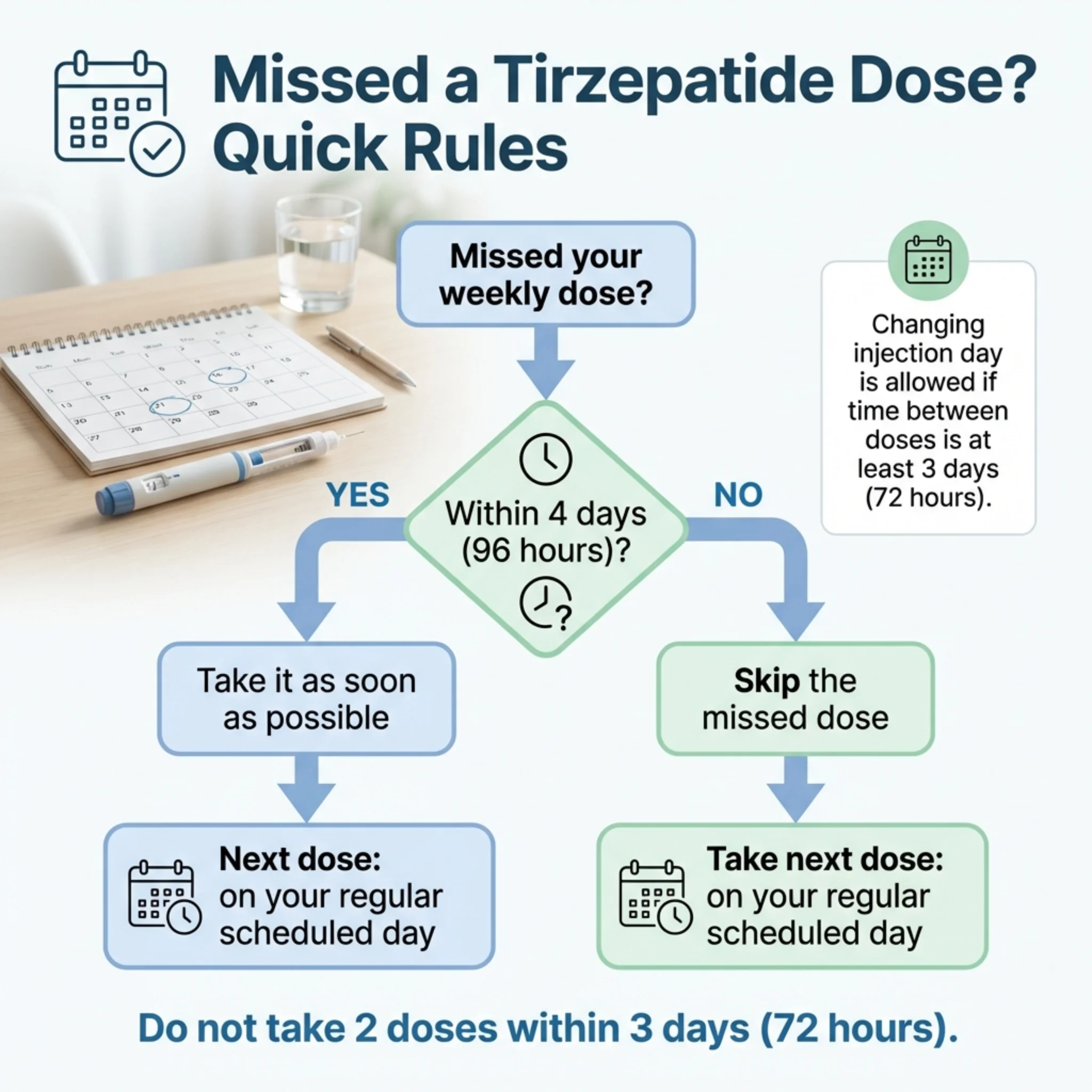
Image is for illustrative purposes only and does not constitute medical advice.
What About Missing Multiple Doses?
If you miss one dose, the rules above apply and you continue normally.
If you miss two or more doses in a row, contact your provider. There isn't a universal restart rule in the prescribing information — your clinician may recommend restarting at a lower dose to improve tolerability rather than resuming at your previous higher dose. This helps avoid the GI side effects that come with reintroducing the medication after a gap.
Can You Change Your Injection Day?
Yes. The only rule: at least 72 hours (3 days) must pass between doses.
So if your current injection day is Monday and you want to switch to Thursday, that works — there are more than 72 hours between Monday and Thursday. But switching from Monday to Wednesday doesn't work — only 48 hours apart.
Tips to Avoid Missing Doses
- •Pick a consistent day and time (many people choose Saturday or Sunday mornings)
- •Set a recurring phone alarm labeled “tirzepatide” or “injection day”
- •Keep your pens/vials in a visible spot in the fridge (not buried in the back)
- •If you travel frequently, remember: single-dose pens can be stored at room temperature (up to 86°F / 30°C) for up to 21 days
How to Inject Tirzepatide (Quick Reference)
Following the tirzepatide injection schedule is straightforward. If you're using a pre-filled pen, the process takes about 60 seconds:
- Remove from fridge 30 minutes beforehand — room-temperature medication is more comfortable to inject
- Check the liquid — it should be clear, colorless to slightly yellow, and free of particles. Don't use it if it's cloudy, discolored, or contains particles
- Choose your injection site — abdomen, front of thigh, or back of upper arm (someone else needs to do the arm). Rotate sites each week
- Clean the area with an alcohol swab, let it dry
- Inject following your pen's instructions (single-dose pens and KwikPens have slightly different mechanisms — follow the Instructions for Use that came with yours)
- Dispose of the used pen in a sharps container
For vial users: draw the correct volume (0.5 mL for single-dose vials, 0.6 mL for multi-dose vials, or calculated volume for compounded) using the syringe your provider prescribed. Inject subcutaneously at a 45–90° angle into pinched skin.
Timing: you can inject at any time of day, with or without food. Pick whatever time you'll consistently remember.
Storage: Refrigerate between 36°F and 46°F (2°C to 8°C). Do not freeze — if frozen, discard it. Single-dose pens and vials can stay at room temperature (up to 86°F / 30°C) for up to 21 days. Multi-dose products should be discarded after 30 days at room temperature.

Image is for illustrative purposes only and does not constitute medical advice.
“I'm Not Losing Weight on 2.5 mg — Is It Working?”
This is one of the most common questions in GLP-1 communities, and the answer is: yes, almost certainly.
Remember — 2.5 mg is an initiation dose, not a treatment dose. It's doing its job even if the scale hasn't moved. In those first four weeks, the medication is beginning to activate your GLP-1 and GIP receptors, starting to reduce appetite signals, and allowing your body to adjust to the medication's presence.
What you should be noticing at 2.5 mg:
- •Slightly reduced appetite or fewer cravings (not everyone notices this at 2.5 mg, and that's normal)
- •Possibly eating smaller portions without feeling deprived
- •Maybe some mild GI symptoms as your body adjusts
What you probably won't see yet:
- •Dramatic scale changes — clinically significant weight loss typically kicks in at 5 mg and above
- •Complete appetite suppression — that usually builds as the dose increases
If you've completed four weeks at 2.5 mg and haven't noticed much, that doesn't mean the medication isn't right for you. It means you're on the initiation dose and it's time to talk to your provider about moving to 5 mg. The real results start there.
Track these instead of just weight during the first month:
- •Are you thinking about food less often?
- •Are your portion sizes naturally smaller?
- •Do you feel satisfied sooner during meals?
- •Are you snacking less between meals?
These early signals predict success even before the scale moves significantly.
Zepbound vs. Mounjaro — Which Dosing Schedule Do You Follow?
Same medication. Same schedule. Different label.
| Zepbound | Mounjaro | |
|---|---|---|
| Active ingredient | Tirzepatide | Tirzepatide |
| Manufacturer | Eli Lilly | Eli Lilly |
| FDA approved for | Weight loss + sleep apnea | Type 2 diabetes |
| Starting dose | 2.5 mg weekly × 4 weeks | 2.5 mg weekly × 4 weeks |
| Escalation | +2.5 mg every 4+ weeks | +2.5 mg every 4+ weeks |
| Maintenance (weight loss) | 5, 10, or 15 mg | N/A (off-label for weight loss) |
| Maintenance (diabetes) | N/A | 5, 7.5, 10, 12.5, or 15 mg |
| Maintenance (sleep apnea) | 10 or 15 mg | N/A |
| Maximum dose | 15 mg | 15 mg (adults); 10 mg (pediatric) |
Source: Zepbound and Mounjaro prescribing information, FDA.
The dosing schedule you follow depends on which one your doctor prescribed, which depends on your diagnosis. If you're using tirzepatide for weight loss, your prescription is likely Zepbound. If it's for type 2 diabetes, it's Mounjaro. The mechanics of how you take it — same day each week, subcutaneous injection, dose escalation rules — are identical.
Insurance coverage is where the practical difference shows up. Some insurance plans cover Mounjaro for diabetes but not Zepbound for weight loss. Others cover neither. Your provider and pharmacy can help navigate this.
Image is for illustrative purposes only and does not constitute medical advice.
Important Safety Information
Tirzepatide is a powerful medication with real benefits and real risks. You should understand both.
Boxed Warning (From FDA Labeling)
In animal studies, tirzepatide caused thyroid C-cell tumors in rats. It's unknown whether this occurs in humans. Tirzepatide is contraindicated (do not use) if you or a family member has a history of medullary thyroid carcinoma (MTC) or Multiple Endocrine Neoplasia syndrome type 2 (MEN 2).
Other Important Safety Considerations
- Pancreatitis: Cases have been reported in clinical trials. Severe abdominal pain (sometimes radiating to the back) is a red flag — stop the medication and contact your provider immediately.
- Gallbladder problems: Rapid weight loss increases the risk of gallstones. Report symptoms like upper-right abdominal pain, especially after meals.
- Kidney issues: Dehydration from nausea, vomiting, or diarrhea can affect kidney function. Stay hydrated, especially during dose escalation.
- Low blood sugar (hypoglycemia): Tirzepatide alone doesn't typically cause low blood sugar, but combining it with insulin or sulfonylureas can. Your provider may lower the dose of those medications when starting tirzepatide.
- Oral contraceptives: Tirzepatide slows gastric emptying, which can reduce the effectiveness of birth control pills. Use a backup contraceptive method (condom, etc.) for 4 weeks after starting tirzepatide and for 4 weeks after each dose increase.
- Pregnancy: Tirzepatide may cause fetal harm. Discontinue tirzepatide when pregnancy is recognized. If you're planning to become pregnant, discuss timing with your provider.
- No dose adjustment needed for kidney or liver impairment (per current labeling), though your provider should monitor kidney function if you experience dehydration.
- Suicidal behavior and ideation: Monitor for depression or suicidal thoughts. Discontinue tirzepatide if these symptoms develop. Avoid use in patients with a history of suicidal attempts or active suicidal ideation.
- Pulmonary aspiration during anesthesia: Tirzepatide delays gastric emptying. If you have any planned surgeries or procedures requiring general anesthesia or deep sedation, tell your surgical and anesthesia team that you use tirzepatide.
Do Not Use (Contraindications)
- •Personal or family history of medullary thyroid carcinoma (MTC) or Multiple Endocrine Neoplasia syndrome type 2 (MEN2)
- •Serious hypersensitivity to tirzepatide or any component of the formulation
Do Not Use / Avoid Without Clinician Guidance
- •Avoid if you have a history of suicidal attempts or active suicidal ideation
- •Do not use in combination with another GLP-1 receptor agonist
- •Tirzepatide has not been studied in people with a history of pancreatitis — discuss risks and alternatives with your clinician
- •Not indicated for people with type 1 diabetes
Source: FDA prescribing information for Zepbound and Mounjaro. NCBI StatPearls: Tirzepatide.
When You Should NOT Increase Your Tirzepatide Dose
Your provider makes the call on dose increases, but there are clear situations where escalating is the wrong move. Knowing these in advance helps you advocate for yourself.
Don't increase if you're still having significant GI side effects at your current dose. If nausea, vomiting, or diarrhea haven't settled after 4+ weeks at a dose, adding more medication will likely make things worse. Your provider should hold you at your current dose (or drop you back) until side effects are manageable.
Don't increase if you're losing weight consistently at your current dose. If you're dropping 1–2 pounds per week at 7.5 mg, there may be no reason to go to 10 mg. Higher doses carry more side effect risk. The goal is the lowest effective dose, not the highest tolerated one.
Don't increase if you're experiencing dehydration. Persistent diarrhea or vomiting that affects your hydration is a reason to pause, not escalate. Dehydration can lead to kidney problems, which tirzepatide prescribing information specifically warns about.
Don't self-increase. This sounds obvious, but it happens — especially with compounded vials where it's physically possible to draw a larger dose. Never change your dose without your provider's direction.
Do talk to your provider if: you've been at the same dose for 8+ weeks and weight loss has completely stalled, your appetite suppression has noticeably weakened, or you feel the medication “isn't doing as much” anymore. These may be reasons to increase — but the decision should come from your provider, not the internet.
Tirzepatide Microdosing — What's Real and What's Internet Talk
You'll find mentions of “tirzepatide microdosing” online — starting at doses like 0.5 mg or 1 mg instead of the standard 2.5 mg. This is not part of the FDA-approved dosing protocol.
Some providers, particularly those prescribing compounded tirzepatide, do start patients at sub-standard doses to minimize GI side effects in people who are especially sensitive to medications. This approach has logic behind it (slower introduction = less nausea), but it hasn't been studied in clinical trials and there's no standardized microdosing schedule.
If your provider recommends microdosing, the same safety principles apply: know your dose in milligrams, know your vial concentration, increase gradually under supervision, and don't self-adjust.
If you came across microdosing advice on social media — don't change your dosing without talking to your prescriber first. The approved titration schedule was designed with tolerability in mind, and most people do fine following it.
For a deeper look, see our full guide: Microdosing Tirzepatide: Chart, Dosage & Complete Guide.
Drug Interactions and Timing With Other Medications
Tirzepatide slows gastric emptying — that's part of how it reduces appetite. But it also means oral medications you take around the same time may be absorbed differently.
Medications that need special attention:
- Oral contraceptives (birth control pills): effectiveness may be reduced. Use backup contraception for 4 weeks after starting tirzepatide and after each dose increase.
- Insulin and sulfonylureas: increased risk of low blood sugar. Your provider may reduce the dose of these when starting tirzepatide.
- Warfarin and other drugs with a narrow therapeutic index: your provider should monitor levels more closely when you start or change tirzepatide doses.
- Any oral medication you take daily: ask your provider whether timing adjustments are needed. This is particularly important for medications where precise absorption matters.
General timing advice: if you take other medications by mouth, mention tirzepatide when discussing timing with your doctor or pharmacist. They may recommend taking time-sensitive medications at a different time of day than your injection.
How to Get Started With Tirzepatide
If you've read this far, you probably have a solid understanding of how tirzepatide dosing works. The next question is practical: how do you actually begin treatment?
Three paths:
1. Through your primary care doctor or endocrinologist. If you have an existing relationship with a provider, this is often the simplest route. They can prescribe Zepbound or Mounjaro based on your diagnosis and insurance coverage.
2. Through a telehealth weight loss provider. If you want faster access or your PCP isn't comfortable prescribing GLP-1 medications, telehealth platforms offer virtual consultations with licensed providers who specialize in weight management. Providers like MEDVi offer clinician-guided dosing support through the entire titration process — from your first 2.5 mg injection through finding your maintenance dose — plus ongoing side-effect management and regular check-ins. This can be especially valuable if dosing questions or side effects come up between regular doctor visits.
3. Through a local weight loss clinic. In-person clinics may offer both branded and compounded options, with direct oversight.
A note on cost: Brand-name Zepbound lists at over $1,000/month without insurance. Eli Lilly offers a savings card for eligible commercially insured patients, and LillyDirect offers Zepbound single-dose vials starting at $399/month for self-pay patients (verify current pricing at zepbound.lilly.com). Telehealth providers sometimes offer more affordable pathways through compounded alternatives. Insurance coverage is expanding but varies significantly by plan and diagnosis.
MEDVi
From $279/mo
What Real Patients Say About Tirzepatide
Clinical trial data tells you what happens on average. Patient experiences tell you what it actually feels like. Below are summaries of user-submitted reviews (moderated by Drugs.com). Experiences vary, and these do not replace medical advice.
From a user-submitted review (Drugs.com, rated 10/10): A 63-year-old woman reported going from 206 pounds to 130 pounds over about eight months on tirzepatide. She described the appetite suppression as dramatic — food simply became less interesting — and her only side effect was mild constipation. She described tirzepatide as transformative for her relationship with food.
From a user-submitted review (Drugs.com, rated 9/10): A 58-year-old woman who started at 270 pounds reported losing 26 pounds in her first eight weeks. Her primary side effect was fatigue the day after each injection. She emphasized that she was approaching it as a long-term lifestyle change, not a quick fix.
From SURMOUNT-4 clinical trial exit interviews (published in Patient — Patient-Centered Outcomes Research): Among 86 participants interviewed at the end of the trial, 91% reported decreased appetite and 62% reported increased energy levels. Participants described wanting to eat less and feeling satisfied sooner. One participant described the shift as moving to “eating to live, instead of living to eat.”
As of February 2026, tirzepatide has an average rating of ~8.7 out of 10 from over 1,300 reviews on Drugs.com, with approximately 81% of reviewers reporting a positive experience. Individual results vary. Always use tirzepatide under medical supervision alongside diet and exercise.
How long will I need to take tirzepatide?
Tirzepatide is intended as a long-term treatment. Clinical data shows weight regain commonly occurs after discontinuation. Your provider will help you develop a sustainable plan, which may include ongoing medication, dose reduction for maintenance, or transition to other approaches.
What if I stop tirzepatide for two weeks — do I restart at 2.5 mg?
There's no universal restart rule in the prescribing information. If you've been off for two weeks, your clinician may recommend restarting at a lower dose to improve tolerability rather than resuming at your previous higher dose. The longer the gap, the more likely you'll need to step back further. Always consult your provider — don't guess.
Can I split my tirzepatide dose into two smaller injections per week?
This is not the FDA-approved dosing protocol. Some providers experiment with split dosing for patients who have trouble tolerating a full weekly dose, but there's no clinical trial data supporting this approach. Don't change your injection frequency without your provider's guidance.
Why do I have “sulfur burps” on tirzepatide?
Sulfur-tasting burps are a commonly reported side effect in patient communities, though they're not prominently featured in clinical trial data. They're believed to relate to tirzepatide's effect on gastric emptying. Eating slowly, avoiding carbonated drinks, and reducing high-sulfur foods (eggs, broccoli, garlic) may help. They typically improve over time.
Is it normal to feel tired on tirzepatide?
Fatigue is a recognized side effect, affecting roughly 5% or more of patients in clinical trials. It's most common during dose escalation and often improves as your body adjusts. If you're significantly reducing caloric intake, make sure you're still eating enough protein and staying hydrated — extreme calorie restriction can worsen fatigue independent of the medication.
Does the injection site matter for tirzepatide?
The three approved sites are the abdomen, front of the thigh, and back of the upper arm (which requires someone else to inject). Absorption is generally consistent across sites. Most people find the abdomen easiest for self-injection. The key is to rotate sites each week to prevent skin irritation or lumps at the injection site.
How We Verified This Guide (And How Often We Update It)
Everything on this page is sourced from primary medical references:
- •Dosing schedule: FDA-approved prescribing information for Zepbound (revised January 2026) and Mounjaro (revised December 2025)
- •Weight loss data: Peer-reviewed clinical trials published in the New England Journal of Medicine (SURMOUNT-1, SURMOUNT-5)
- •Side effect rates: FDA Zepbound prescribing information, Table 1 (pooled Study 1 and Study 2)
- •Clinical reference: NCBI StatPearls: Tirzepatide (last updated 2024)
- •Patient experiences: User-submitted reviews from Drugs.com (moderated); published exit interviews from SURMOUNT-4 (PMC, 2025)
We verify all dosing information, side effect data, and safety warnings against the current FDA-approved prescribing information. When Eli Lilly updates the label (new dosage forms, new indications, safety updates), we update this page.
This page was last verified against FDA prescribing information in February 2026.
This guide is not medical advice. It's a reference to help you understand your treatment and have informed conversations with your healthcare provider. Always follow your prescriber's specific instructions — they know your health history and can tailor dosing to your situation.
About This Article
This guide was researched and written by the WPG Research Team — a group of health and wellness writers who specialize in weight management medications. All dosing information, clinical data, and safety warnings were verified against the current FDA-approved prescribing labels for Zepbound (revised January 2026) and Mounjaro (revised December 2025).
We do not have medical credentials and this content is not medical advice. Our editorial process requires that every factual claim links back to a primary source (FDA labels, peer-reviewed studies, or official clinical trial data). When sources conflict, we defer to the FDA prescribing information as the authoritative reference.
Last verified: February 2026 — Next scheduled review: Upon any FDA label revision or new clinical data publication.
Sources
- FDA prescribing information for Zepbound (revised January 2026)
- FDA prescribing information for Mounjaro (revised December 2025)
- Jastreboff AM, et al. “Tirzepatide Once Weekly for the Treatment of Obesity.” NEJM. 2022;387:205-216. [PubMed]
- “Tirzepatide as Compared with Semaglutide for the Treatment of Obesity.” NEJM. 2025 (SURMOUNT-5). [NEJM]
- NCBI StatPearls: Tirzepatide (last updated 2024)
- User-submitted reviews from Drugs.com (moderated)
- SURMOUNT-4 exit interviews. Patient — Patient-Centered Outcomes Research. [PMC]
Frequently Asked Questions
What is the tirzepatide dosing schedule?
The standard tirzepatide dosing schedule is: start at 2.5 mg once weekly for 4 weeks, then increase to 5 mg. From there, your provider may increase by 2.5 mg every 4+ weeks based on your response and tolerability, up to a maximum of 15 mg weekly. This schedule applies to both Zepbound (weight loss) and Mounjaro (type 2 diabetes).
What is the starting dose of tirzepatide?
The starting dose is 2.5 mg injected once weekly for 4 weeks. This is an initiation dose only — it’s not intended as your ongoing treatment dose. After 4 weeks, your provider will increase you to 5 mg.
How long do you stay on 2.5 mg of tirzepatide?
A minimum of 4 weeks. Your provider may keep you at 2.5 mg longer if you’re experiencing side effects, but most people move to 5 mg at the four-week mark.
What are the maintenance doses for weight loss?
For Zepbound (weight loss), the recommended maintenance doses are 5 mg, 10 mg, or 15 mg once weekly. Your provider will choose based on your response and tolerability.
What are the maintenance doses for sleep apnea?
For obstructive sleep apnea, maintenance doses are 10 mg or 15 mg once weekly. The 5 mg option is not approved as a maintenance dose for this indication.
What is the maximum dose of tirzepatide?
15 mg once weekly for all indications. Do not exceed this dose.
Can you take tirzepatide twice a week?
No. Tirzepatide has a half-life of approximately 5 days, meaning it stays active in your body between weekly doses. Once weekly is the approved and studied frequency.
What does "25 units" of tirzepatide equal in milligrams?
It depends entirely on your vial’s concentration. At 10 mg/mL, 25 units = 2.5 mg. At 20 mg/mL, 25 units = 5 mg. Always check your vial label and confirm with your pharmacist.
What if I miss a dose of tirzepatide?
If it’s been less than 4 days (96 hours), take it as soon as you remember. If more than 4 days have passed, skip it and take your next dose on your regular day. Never double up.
Can I change my tirzepatide injection day?
Yes, as long as at least 72 hours (3 days) have passed between doses. You can then continue on your new day each week.
How long does it take for tirzepatide to start working?
Most people notice appetite changes within 1–3 weeks. Significant weight loss typically becomes visible around weeks 4–8. In the SURMOUNT-1 trial, results continued to accumulate for the full 72 weeks of the study, with the greatest rate of loss occurring between weeks 4 and 24.
Is compounded tirzepatide safe?
Compounded tirzepatide is not FDA-approved and hasn’t been tested in clinical trials. Quality depends on the compounding pharmacy. If using compounded, ensure it’s prescribed by a licensed provider and sourced from an accredited pharmacy. Know your dose in mg and your vial’s concentration.
Does tirzepatide cause hair loss?
Some patients report hair thinning. This is generally associated with rapid weight loss and nutritional deficiency rather than the medication itself. Adequate protein intake (at least 60–80g daily) and a multivitamin may help.
Can I drink alcohol on tirzepatide?
Tirzepatide doesn’t directly interact with alcohol. However, alcohol can worsen GI side effects, contribute to dehydration, and lower blood sugar (especially if you’re also on diabetes medications). Most providers recommend limiting alcohol, particularly during dose escalation.
What happens if I stop taking tirzepatide?
Weight regain is common. In the SURMOUNT-4 trial, participants who switched from tirzepatide to placebo regained a significant portion of their lost weight over 52 weeks. Tirzepatide is intended for long-term use. Discuss any changes with your provider.
Is tirzepatide better than semaglutide for weight loss?
In the SURMOUNT-5 head-to-head trial, tirzepatide produced significantly more weight loss than semaglutide (20.2% vs. 13.7% at maximum tolerated doses over 72 weeks). Both are effective — your provider can help determine which is better for your specific situation.
Do I need dose adjustments for kidney or liver problems?
Per current FDA labeling, no dose adjustment is recommended for hepatic or renal impairment. However, your provider should monitor kidney function if you experience dehydration from GI side effects.
Should I eat before taking tirzepatide?
Tirzepatide can be taken with or without food, at any time of day. There’s no requirement to eat before or after injection.
What is the starting dose of compounded tirzepatide?
The milligram-based schedule is the same — typically 2.5 mg weekly for 4 weeks, then escalating. The difference is how it’s measured (vials vs. pens) and that concentrations vary between compounding pharmacies. Always confirm your dose in mg and your vial’s concentration with your provider.