How to Switch GLP-1 Providers Mid-Treatment (2026)
By WPG Research Team · · ·
Weight Loss Provider Guide is an independent comparison resource for GLP-1 telehealth providers. We may earn a commission when readers start a program through our links. That never changes which providers we cover, what we say about them, or how we match them to your switch reason. Compounded GLP-1 medications are not FDA-approved. Only a licensed clinician can decide what is appropriate for you.
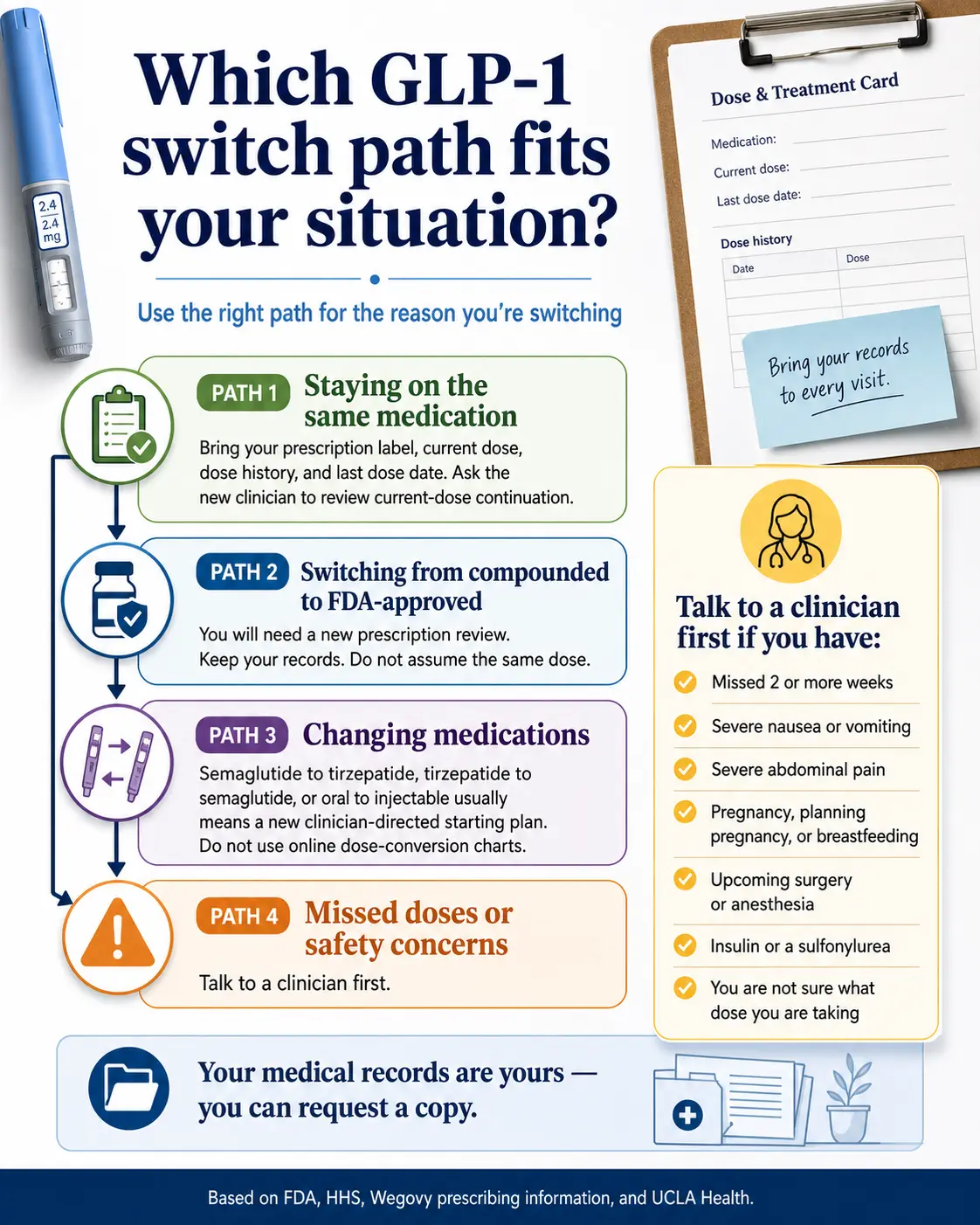
Bottom line: Yes, you can switch GLP-1 providers mid-treatment — and the new clinician decides whether to continue, lower, or restart your dose after reviewing your records. The order is what matters. Cancel last. Document first. Save your prescription label, dose history, and last dose date before you click cancel anywhere. Plan around your normal dosing interval and ask the new clinician what gap to use — many weekly-injection switches are timed around the next scheduled dose. The new clinic reviews your records; you don’t auto-continue.
Quick navigation by your situation:
- 🟦 Switch from compounded to a different compounded provider → Scenario A
- 🟩 Switch from compounded to FDA-approved brand-name → Scenario C
- 🟧 Try tirzepatide after semaglutide (or vice versa) → Cross-molecule switches
- 🟥 BMI is lower now and worried about qualifying → Maintenance switchers
- 🟪 Not sure what you need → Take the 60-second GLP-1 Switch Quiz →
Build your switch plan before you cancel anything
Get a personalized records checklist, timing window, and provider lane in 60 seconds.
Build My GLP-1 Switch Plan →Why So Many People Are Searching This Right Now
Three things converged in spring 2026 to push patients into the switching market.
| Date | Event |
|---|---|
| April 1, 2026 | FDA approves Foundayo (orforglipron), an oral once-daily GLP-1 from Eli Lilly for chronic weight management. It joins Wegovy tablets as an FDA-approved oral GLP-1 weight-management option. |
| April 30, 2026 | FDA proposes excluding semaglutide, tirzepatide, and liraglutide from the 503B Bulks List. |
| June 29, 2026 | Public comment period closes on the 503B proposal. |
| July 1, 2026 | Medicare GLP-1 Bridge launches — see the Medicare section below. |
In March 2026, Hims and Hers also announced direct partnerships with Novo Nordisk for FDA-approved Wegovy and Ozempic, and both have largely deprioritized compounded GLP-1 advertising. Add the standard reasons people switch — refill price jumps, billing problems, slow shipping, dose escalation pricing — and you’ve got a very active mid-treatment switching market.
The One Decision This Page Helps You Make
“Can I leave my current GLP-1 provider without losing my dose, my progress, my money, or my safety?”
The answer is yes — if you do four things in the right order:
- Document your current dose and treatment history before you cancel
- Time the switch around your normal dosing interval
- Match your reason for switching to the right next provider
- Verify the new provider can actually review your dose continuation (not just promise to)
Will My New Provider Continue My Current Dose?
Quick answer: It depends on the molecule, your records, your last dose, and the new clinician’s review. Same-molecule switches are usually easier to review than cross-molecule switches, but dose continuation is not automatic. Cross-molecule switches (semaglutide ↔ tirzepatide ↔ orforglipron) commonly require a restart or re-titration plan because there is no validated direct dose-conversion chart between them. The clinician sets the starting dose.
The Dose-Continuation Evidence Ladder
How likely a new clinician is to review continuation of your current dose tracks closely with how much documentation you can show them.
Prescription label + current dose + last fill date + full dose history + clinician notes/messages
→ Clean review for same-molecule continuation
Prescription label + current dose only
→ Reviewable, but clinician may ask follow-up questions
Self-reported dose with no label or fill record
→ Many providers will treat this as a re-initiation
Missed two or more weeks, severe side effects, gallbladder/pancreatitis-type symptoms, or unknown medication source
→ Talk to a clinician before switching anything
Same-molecule switches (easier review)
Moving from compounded semaglutide to brand-name Wegovy, or compounded tirzepatide to brand-name Zepbound — same underlying molecule. Makes clinical review simpler. Not automatic — the new clinician still has to review your prescription label, dose history, and last dose date.
Cross-molecule switches (need re-titration)
Semaglutide and tirzepatide work differently. No validated dose-conversion chart exists between them. Clinician sets the starting dose. Re-titration commonly takes 8 to 16 weeks. This is the safe way to do it.
Switching to or from Foundayo (the new oral pill)
Foundayo (orforglipron) is an oral once-daily GLP-1, FDA-approved April 1, 2026. It is a different molecule from semaglutide and tirzepatide. Switching to or from Foundayo follows cross-molecule rules — the new clinician sets the starting dose with structured supervision. Compounded oral or sublingual products are not FDA-approved and are not the same as Foundayo or Wegovy tablets.
What new providers actually need from you
- Photo of your current prescription label
- Your dose history (every dose, every escalation date)
- Your last dose date
- Any side effects you’ve had
- Records of any lab work your prior provider ran
- Your reason for switching
The “Don’t Cancel Yet” Records Checklist
Quick answer: Once you cancel, portal access may be limited or harder to retrieve, so save your records first. Federal HIPAA guidance gives you the right to a copy of your medical records, and providers normally have up to 30 days to provide it — though many can deliver sooner.
The 12-Item Pre-Cancel Continuity Checklist
| # | What to gather | Why it matters |
|---|---|---|
| 1 | Screenshot of your current prescription label | Shows medication name, dose, fill date, prescriber, and pharmacy — everything a new clinician needs |
| 2 | Your full dose history | Every dose, every escalation date — this is the strongest evidence for continuation |
| 3 | Your last dose date | Drives the washout decision and whether the new clinician retitrates |
| 4 | Weight log from start of treatment to today | Demonstrates response and supports the continuation case |
| 5 | Side effect notes and how they were managed | Helps the clinician decide whether to continue, lower, or change medications |
| 6 | The compounding pharmacy's name and accreditation status (if compounded) | New provider may want to verify source quality |
| 7 | Any lab work (baseline, A1c, thyroid, lipid panels) | Avoids redundant lab orders at the new provider |
| 8 | Your full billing history with the current provider | Spot pending charges, prepay terms, and renewal dates |
| 9 | The exact wording of the cancellation policy | Notice periods, minimum-term rules, and refund cutoffs vary widely |
| 10 | Tracking number for your most recent shipment | If something's still in transit, you don't want to cancel yet |
| 11 | Messages with your clinician that include dosing rationale | These become medical records the new clinician can review |
| 12 | Your remaining supply count | Drives the timing of when to start the new intake |
The records request script (copy-paste this)
If your current provider’s portal doesn’t make all of this downloadable, send a written records request. Federal HIPAA rules give your provider up to 30 days to respond.

What’s the Right Gap Between Providers When Switching?
Quick answer: Plan around your normal dosing interval and let the new clinician set the gap. After five to seven days, the amount of medication in the body decreases by about half, but GLP-1 medications such as Wegovy or Zepbound may not completely leave the system for 30 days. (UCLA Health.) Many weekly-injection switches are timed around the next scheduled dose.
GLP-1 medications have long half-lives. That long tail is also why a “treatment gap” is rarely a sharp cliff — your medication keeps working at reduced concentrations for weeks after the last dose. Pharmaceutical Journal guidance describes a range of approaches clinicians use, including timing the new medication around the next scheduled dose, a one-to-two-week observation period, or a longer washout depending on patient factors.
When a longer gap is recommended
- You’re switching across molecules (semaglutide ↔ tirzepatide ↔ orforglipron)
- You had significant GI side effects (nausea, vomiting, dehydration)
- You had any gallbladder or pancreatitis-type symptoms during prior treatment
- You missed multiple doses before deciding to switch
In any of those cases, the new clinician decides. Don’t improvise.
How to time the switch so you don’t have a gap
Submit your new provider’s intake form 10 to 14 days before your final dose with the old provider. That gives the new clinician time to review your records, ship medication, and have it ready before the gap window opens. Most telehealth platforms ship in 2 to 5 days after approval. Approval takes 1 to 3 days.
What If I Miss a Dose Before I Get the Switch Done?
Quick answer: A short gap may not require a restart for some patients, but the prescriber should decide — especially if the gap approaches two weeks or more. UCLA Health’s published guidance specifically advises patients who’ve been off a GLP-1 for more than 2 weeks to contact their prescribing clinician before resuming their old dose, because some patients may have adverse effects if they restart at the same dose.
The medication doesn’t fall off a cliff at day 8. Pharmacokinetically, you’re partially covered for weeks after your last dose because the molecule clears slowly. That’s a buffer, not a license to wait. If you missed two or more weeks before you started shopping for a new provider, start the new intake first and tell the new clinician about the gap.
The Provider Switch Readiness Matrix
Quick answer: The right next provider depends on the molecule you’re on, the format you want, and whether you want compounded or FDA-approved brand. Here is what we verified about the major options on May 4, 2026, with sources cited and unverified items flagged so you can spot-check.
Commercial facts were verified live at each provider’s website during the first week of May 2026. Anything we could not independently verify is flagged [NEEDS VERIFICATION].
| Provider | Best for switchers who… | Transfer policy signal | Verified pricing (May 2026) | Important caveat |
|---|---|---|---|---|
| Embody | Are self-pay, want a low first-month price, and want weekly injections or a needle-free GLP-1 gum option | ⚠️ Public transfer policy not specifically published. Online intake collects current medication and dose so a licensed provider can review continuation. [NEEDS VERIFICATION] | Compounded semaglutide injection: $99 first month, then $299/mo ongoing. Tirzepatide injection: $149 first month, then $399/mo. Needle-free GLP-1 gum option available. Cash-pay; HSA/FSA accepted. | Refills rise after the intro month. No insurance billing. Broad U.S. availability — confirm your state at intake. Compounded = not FDA-approved. |
| Ro | Want FDA-approved brand-name medication, insurance support, or the new oral pill (Foundayo) | ⚠️ Public transfer policy not specifically published. Intake reviews prior treatment history. [NEEDS VERIFICATION] | Membership $39 first month, then $149/mo — or as low as $74/mo with annual plan. Cash-pay: Foundayo, Wegovy pill/pen, Zepbound KwikPen, Ozempic. Insurance: Zepbound pen, Ozempic, Wegovy pen. | Membership is on top of medication cost. Insurance concierge handles prior-auth paperwork. |
| MEDVi | Want broad cash-pay menu, lowest entry month, and month-to-month billing | ⚠️ Public transfer policy not found. [NEEDS VERIFICATION] | Compounded semaglutide $179 first month, then $299/mo. Tirzepatide: verify at checkout. | ⚠️ FDA issued MEDVi a warning letter on Feb 20, 2026 (Warning Letter 721455) for misbranding. MEDVi remains active and LegitScript-certified. Compounded = not FDA-approved. |
| SHED | Want needle-free formats — drops, lozenges, oral tablets — alongside injection options | ⚠️ Public transfer policy not found. [NEEDS VERIFICATION] | Semaglutide injections $299/mo, tirzepatide $399/mo. Lozenges from $199/mo. Drops from $229/mo. Brand-name via $99 membership. | Compounded oral/sublingual formats require extra scrutiny — not FDA-approved and may differ by pharmacy and formulation. |
| Sesame Care | Want clinician choice with brand-name FDA-approved options | ⚠️ Public transfer policy not found. Marketplace model. [NEEDS VERIFICATION] | Ongoing care from $59/mo. Medication separate. Brand-name: Wegovy pill/pen, Zepbound pen/vial/KwikPen, Foundayo, Ozempic. | Pay per visit plus medication at pharmacy. Best for patients who want clinician choice. |
| Enhance MD | Are switching due to a plateau, want lab-guided care, or want a more clinical feel | ⚠️ Public transfer policy not found. [NEEDS VERIFICATION] | Core (sema) $49/$212. Advanced (tirze) $99/$280. Elite (sema + tirze + labs) $189/$322. First month/ongoing. | Higher-touch model with labs. Elite tier is provider-stated program info, not editorial endorsement. Compounded = not FDA-approved. |
| Yucca Health | Want async, no-live-visit, approval-first onboarding | ⚠️ Public transfer policy not found. [NEEDS VERIFICATION] | GLP-1 injections from $146/mo for new patients on semaglutide 6-month plan. Klarna/Affirm/Afterpay available. Exact ongoing price [NEEDS VERIFICATION at checkout]. | Async = messaging-based. No synchronous video visit. Compounded = not FDA-approved. |
| Hims | Want familiar male-coded consumer brand with FDA-approved Novo Nordisk medications | ⚠️ Public transfer policy not found. [NEEDS VERIFICATION] | FDA-approved Wegovy pill, Wegovy pen, and Ozempic via March 2026 Novo Nordisk partnership. Pricing varies by plan. | Has largely deprioritized compounded GLP-1 advertising. Not the match if you specifically want a compounded path. |
| Hers | Want familiar female-coded consumer brand with FDA-approved Novo Nordisk medications | ⚠️ Public transfer policy not found. [NEEDS VERIFICATION] | Same FDA-approved formulary as Hims via the Novo Nordisk partnership. Pricing varies by plan. | Same caveat as Hims — compounded path is not the strength here. |
| Direct Meds | Want oral or sublingual specialty pricing | ⚠️ Public transfer policy not found. [NEEDS VERIFICATION] | Sublingual liquid sema $179.10/mo. Compounded sema $297/mo. Tirze options $224.10 and $399/mo. | Niche specialty fit. Verify formulation, prescribing model, and ongoing pricing before committing. |
Editorial conclusion
For self-pay switchers staying on a compounded path, Embody is a strong low-cost first comparison — a low first-month price, semaglutide and tirzepatide injections, and a needle-free GLP-1 gum option for needle-averse switchers. Bring your prescription label and dose history so a licensed provider can review continuation at intake.
For switchers moving to FDA-approved brand-name medication, Ro leads because it publishes a broad FDA-approved GLP-1 menu, brand-name pricing, and dedicated insurance-concierge support. Sesame Care is the secondary brand path when you want clinician choice or self-pay flexibility.
We do not lead this page with MEDVi despite competitive entry pricing because the February 20, 2026 FDA warning letter is the kind of trust signal mid-treatment switchers should weigh up front. MEDVi is still an active, operating, LegitScript-certified provider — but for a search where confidence matters, we want you to make that call with full information.
What Should You Ask a New GLP-1 Provider Before You Pay?
Quick answer: Ten questions, all answerable before you hand over a credit card. If a provider can’t or won’t answer them in writing, that’s data. The right provider answers calmly and completely.
| # | Question to ask | Why it matters |
|---|---|---|
| 1 | "Will your clinician review my current-dose continuation if I provide my prescription label, dose history, and last dose date?" | The single highest-leverage question. The answer separates a real switch from a forced restart. |
| 2 | "What happens if I'm not approved? Is the first month refundable?" | Refund policies vary widely. Get this in writing. |
| 3 | "Which pharmacy or medication source do you use?" | You should be able to verify the dispensing pharmacy. |
| 4 | "Is the medication FDA-approved or compounded?" | These are different products with different regulatory status. Don't let anyone blur them. |
| 5 | "What states do you serve?" | State availability can change without notice. |
| 6 | "Are labs required, and at what cost?" | Lab requirements vary by provider. |
| 7 | "How long from intake to first shipment, on average?" | Drives your switching timeline. |
| 8 | "What's the cancellation policy and notice period?" | Notice periods, minimum-term rules, and refund cutoffs vary. |
| 9 | "What is my total cost in month two, including any membership fees?" | The first-month price is rarely the ongoing price. |
| 10 | "Can you handle prior authorization if I want to use insurance?" | Brand-name paths get a lot easier with concierge support. |
If a provider passes all 10 with confident, written answers, you’ve found the right next provider. If they dodge two or more, keep shopping.
Scenario A: Switch Compounded → Compounded with a Better Provider
Quick answer: Embody is a strong low-cost match for self-pay switchers — a low first-month price, weekly semaglutide or tirzepatide injections, and a needle-free GLP-1 gum option for needle-averse patients. It’s cash-pay (no insurance) with 24/7 support. Bring your prescription label, dose history, and last dose date so a licensed provider can review whether to continue, lower, or restart your dose.
Embody pricing (Start Program):
- Semaglutide injection: from $99 first month, then $299/month ongoing
- Tirzepatide injection: $149 first month, then $399/month ongoing
- Needle-free GLP-1 gum available as an alternative to injections. Cash-pay; HSA/FSA accepted. No insurance billing.
How Embody reviews a transfer
Embody’s online intake collects your current medication, current dose, and prescription details so a licensed provider can review whether to continue, lower, or restart your dose. There is no validated direct dose-conversion chart between molecules, so confirm your continuation plan during intake. Complete records improve your odds of a smoother review.
Embody’s shipped compounded GLP-1 options are not FDA-approved finished drugs. A licensed provider determines whether treatment is medically appropriate, and prices, pharmacy availability, shipping timelines, and state eligibility can change and should be confirmed during intake.
One thing to know up front: Refills rise after the intro month, and Embody offers month-to-month as well as 3-, 6-, and 12-month bundles. Review the renewal terms before you prepay multiple months. If you prefer pure month-to-month with no prepay commitment, see Scenario A-2 below (MEDVi).
Resolved objection: “Will I lose my dose, pay a high entry price, or restart from zero?”
Embody’s low first-month price and licensed-provider review of your dose history are the matching answers. Bring your records so the provider can evaluate continuation.
Check Embody Eligibility →Start Embody’s online intake to confirm pricing, state availability, and your dose-continuation plan before you commit. Compounded medications are not FDA-approved.
Scenario A-2: Lowest Entry Price and Month-to-Month Flexibility
Quick answer: MEDVi has one of the lowest entry-month prices among major compounded providers ($179 first month) and bills month-to-month with no commitment. Refills jump to $299 starting month two — a $120 climb you should know about up front. We’ll also disclose the FDA warning letter so you can decide with full information.
MEDVi offers compounded semaglutide and tirzepatide, holds LegitScript certification, and according to the company’s site has served 500,000+ patients. Trustpilot displays roughly a 4.4/5 TrustScore — verify on the day you click. Compounded medications are not FDA-approved.
| Item | Status |
|---|---|
| Current public pricing | Verified at MEDVi.org (May 4, 2026) |
| FDA warning letter | ⚠️ Verified. FDA issued MEDVi a warning letter on February 20, 2026 (Warning Letter 721455) citing misbranding violations related to marketing of compounded GLP-1 medications. |
| Patient-count claim | MEDVi site states 500,000+ patients (provider-stated, May 4, 2026) |
| Trustpilot rating | Roughly 4.4/5 displayed, May 4, 2026. Recheck on publish day. |
| Transfer policy | Public transfer-and-dose-continuation policy not found. [NEEDS VERIFICATION] |
Pivot: if a recent FDA warning letter is a dealbreaker for you, see Embody in Scenario A above for a low-cost compounded provider without that disclosure.
Resolved objection: “Can I try a new provider without locking in?”
Verify MEDVi Current Pricing and Start Eligibility →Scenario C: Switch from Compounded to FDA-Approved Brand-Name
Quick answer: This is the most common GLP-1 switch in 2026 because of the FDA’s April 30 proposal and new oral options. Ro is the strongest fit: it publishes a broad FDA-approved GLP-1 menu, includes a dedicated insurance concierge that handles prior-authorization paperwork, and offers a free GLP-1 Insurance Coverage Checker. Get started for $39, then as low as $74/month with annual plan paid upfront.
Ro’s brand-name route table (verified May 4, 2026)
| Path | Medications listed by Ro |
|---|---|
| Cash-pay | Foundayo (orforglipron), Wegovy pill, Zepbound KwikPen, Wegovy pen, Ozempic |
| Insurance-mediated | Zepbound pen, Ozempic, Wegovy pen |
One real downside: Ro requires a $39 first-month membership and then $149/month ongoing — on top of medication cost. Pivot: if you want zero subscription, the brand-name path through Sesame Care (Scenario C-2) lets you pick a clinician and pay per visit. The Ro membership is worth it for the insurance concierge. If you’re paying cash with no insurance, Sesame may be the better fit.
Resolved objection: “Can I make this transition smooth even with insurance involved?”
The insurance concierge is the answer. They handle the prior-auth paperwork; you handle taking the medication.
Check FDA-Approved GLP-1 Coverage with Ro →Get started for $39, then as low as $74/month with annual plan paid upfront. Medication cost is separate.
Scenario C-2: Maximum Brand Choice with Clinician Selection
Quick answer: Sesame Care is a marketplace model — you pick your specific clinician — with FDA-approved brand options including Wegovy pill, Wegovy pen, Zepbound pen/vial/KwikPen, Foundayo, and Ozempic. Ongoing care starts as low as $59/month. Medication cost is separate.
You pay for the clinician visit, an ongoing care subscription if you want it, and the medication at the pharmacy. More variable than Ro on cost — but you’re choosing your clinician and paying transparently per piece.
Compare Sesame Care Brand-Name GLP-1 Options →Scenario D: Mainstream Consumer Brand with FDA-Approved Medication
Quick answer: Following the March 2026 partnership with Novo Nordisk, both Hims and Hers now offer FDA-approved Wegovy pill, Wegovy pen, and Ozempic. Hims fits male-coded mainstream brand intent. Hers fits female-coded mainstream brand intent. Both have largely deprioritized compounded GLP-1 advertising.
Scenario E: Switching Because of Side Effects, Plateau, or Bad Support
Quick answer: If your last provider was too hands-off — no labs, no follow-up, no clinician access when you needed it — your next provider should be more clinical, not just cheaper. Enhance MD positions itself as a higher-touch, lab-guided alternative for plateau and side-effect cases.
Enhance MD pricing tiers (verified at enhance.md, May 2026):
- Core (compounded semaglutide): $49 first month / $212/month ongoing
- Advanced (compounded tirzepatide): $99 first month / $280/month ongoing
- Elite (program involving semaglutide + tirzepatide and repeat labs): $189 first month / $322/month ongoing
One important caveat: if your “side effects” are severe — persistent vomiting, signs of dehydration, severe abdominal pain, or symptoms that could be gallbladder or pancreatitis-related — don’t shop providers. Talk to a clinician now. Switching providers is not a substitute for medical care during an acute issue.
Resolved objection: “I need actual clinical involvement, not just a refill machine.”
Check If Enhance MD Fits Your Switch Reason →Cross-Molecule Switches: Semaglutide ↔ Tirzepatide ↔ Orforglipron
Quick answer: Cross-molecule switches commonly require a restart or re-titration plan, with the new clinician setting the starting dose. There is no validated direct dose-conversion chart between semaglutide and tirzepatide. Plan for 8 to 16 weeks to titrate back up to a comparable maintenance dose. Do not use online dose-conversion charts as dosing instructions.
Stop the current medication.
Observe a clinician-set washout.
Start the new medication at a clinician-determined dose with structured titration.
Titrate up over 8 to 16 weeks.
For Foundayo (orforglipron), the path is similar — the clinician sets the starting dose with structured supervision. The new clinician makes every dose decision. Your job is to give them complete records.
How to Switch GLP-1 Providers Mid-Treatment: Step by Step
Quick answer: Six steps, in this exact order. (1) Gather records. (2) Check insurance coverage if applicable. (3) Submit intake at a brand-capable provider. (4) Observe a clinician-set washout. (5) Start the new medication at a clinician-determined dose. (6) Cancel the old provider after the new shipment is in hand.
Step 1 — Gather records
All 12 items from the checklist above. Don't skip this. Portal access may disappear after you cancel.
Step 2 — Check insurance coverage
If you have coverage or want to use it, run Ro's free GLP-1 Insurance Coverage Checker or verify your current plan's prior-auth criteria. Do this before paying a new provider.
Step 3 — Submit intake at the new provider
Upload your prescription label and dose history. Ask explicitly whether the clinician can review your current-dose continuation.
Step 4 — Observe the clinician-set washout period
For same-molecule switches, this is often timed around the next scheduled dose. For cross-molecule switches, the clinician sets the gap.
Step 5 — Start the new medication
At the dose the new clinician sets — not your old dose, unless the clinician specifically confirms it.
Step 6 — Cancel the old provider
Only after the new shipment is confirmed and in hand. Verify the cancellation notice period. Save the confirmation email. Watch for unexpected charges for 30 days.
Insurance Carryover When You Switch GLP-1 Providers
| Switch type | Deductible / out-of-pocket carries over? | Likely PA impact |
|---|---|---|
| Same provider, same medication | Yes | Usually none |
| New provider, same medication | Yes | Plan may require updated prescriber information |
| New provider, new medication (cross-molecule) | Yes | Likely new PA submission |
| Compounded → brand-name | Yes | New PA submission |
| Commercial insurance → Medicare GLP-1 Bridge | Plan-specific | New eligibility and prior-auth criteria apply |
What carries over
- Plan-year deductible and out-of-pocket maximum
- HSA/FSA reimbursement eligibility
- Manufacturer copay savings cards for the same medication
What does NOT carry over
- Prior authorization if you switch medications, compounded to brand, or across molecules
- Manufacturer copay cards if you switch to a different manufacturer’s medication
- Prepaid telehealth memberships — most are non-refundable once medication has shipped
The Medicare GLP-1 Bridge (launched July 1, 2026)
If you’re on Medicare Part D, mark your calendar. The Medicare GLP-1 Bridge launches July 1, 2026 and runs through December 31, 2027 as a short-term demonstration program:
- Manufacturer net price: $245 per monthly supply
- Beneficiary-facing copay: $50 per fill, collected at the pharmacy
- The $50 copay does not count toward TrOOP (true out-of-pocket spending) under Part D
- Eligibility requires prior-authorization criteria and a qualifying Part D plan
Source: CMS.gov Medicare GLP-1 Bridge. If you’re considering a switch in summer 2026 and you’re on Medicare, factor this in. The economics may shift.
A Real-World Switching Timeline (Day-by-Day)
Quick answer: A typical mid-treatment switch takes 10 to 14 days from “I’m going to switch” to “I just took my first dose with the new provider.” Same-molecule switches can compress to 7 to 10 days. Cross-molecule switches and brand transitions with prior authorization can stretch to 21 to 28 days.
| Day | Action |
|---|---|
| Day 0 | Decide to switch. Don't cancel anything yet. |
| Day 0–1 | Gather your 12-item continuity checklist. Save everything. |
| Day 1–2 | Submit intake at your new provider. Upload prescription label and dose history. |
| Day 2–5 | New provider clinician review and approval. Some send approval same-day. |
| Day 5–7 | First shipment arrives from new provider. |
| Day 7+ (your normal next dose date) | Take first dose with new provider, on the schedule the clinician sets. |
| Day 7+ | Cancel old provider per their cancellation policy. Verify the notice period in your terms. |
| Day 7–14 | Watch your billing. Save the cancellation confirmation. |
If your new shipment is delayed: don’t double-dose, don’t use research peptides, don’t improvise. Contact the new provider and ask whether to delay your first dose. If the gap will exceed two weeks, ask whether your dose plan changes.
What You Should Compare Besides Monthly Price
Quick answer: Don’t compare only the landing-page price. Compare ongoing cost after intro pricing ends, dose-based price increases, membership fees, lab costs, shipping costs, support quality, cancellation rules, and whether the provider will review your current dose history.
The real cost calculation
(First-month price) + (11 × ongoing monthly price) + (any membership fee × 12) + (lab costs) + (shipping fees if not included) + (any visit fees)
Why transfer-readiness can beat lower price: A cheaper provider is not a bargain if the transfer process creates an avoidable restart, a treatment gap, or unclear clinical review. Documentation-first providers — the ones with published transfer policies — are often the better practical choice even at higher monthly prices.
Honest Tradeoffs: When You Should NOT Switch Right Now
Not every dissatisfaction warrants a switch. Five situations where staying with your current provider is probably the better move:
2 to 4 weeks into a dose escalation and side effects are the issue
GI side effects are common during dose changes. Ask your clinician whether to wait, adjust, or switch before changing providers.
At a stable maintenance dose and price is your only complaint
Manufacturer savings cards, HSA/FSA pre-tax routing, and direct manufacturer cash pricing (NovoCare or LillyDirect) may close the gap without a switch.
A pending prior authorization at your current provider
Let it complete. Switching mid-PA wastes the work that's already in flight.
Your current provider is mid-shipping your refill
Wait until it arrives. Don't double-pay.
You're traveling internationally in the next 30 days
Timing a switch around international travel — with cold-chain shipping, time-zone delays, and pharmacy logistics — is a logistics nightmare. Switch when you're home.
What If My BMI Is Lower Now or I’m Switching for Maintenance?
Quick answer: Some providers may evaluate maintenance patients, but the criteria vary by provider. Don’t hide your current weight or medical history. Bring your starting BMI, current BMI, weight history, comorbidities, current dose, and treatment response so the new clinician can evaluate whether ongoing care or maintenance is appropriate.
Most legitimate platforms use clinical thresholds (BMI 30+, or BMI 27+ with a weight-related condition) for new patients. For transferring patients, treatment history matters — but maintenance-specific transfer policies should be verified with each provider before you pay.
If your BMI dropped below 27, your safest move is a provider with: (1) an intake that explicitly reviews your current dose and treatment history, (2) a clinician (not just a chatbot) reviewing that history, and (3) flexibility to prescribe at lower maintenance doses. Embody’s intake collects your current dose and history for licensed-provider review; Ro and Sesame also route through real clinicians who can review treatment history.
Resolved objection: “Will my new provider still accept me at maintenance?”
Check Embody Eligibility →Red Flags: When the New Provider Isn’t Safe
Avoid any provider that skips clinician review, hides the pharmacy source, guarantees results, blurs compounded with FDA-approved, requires long prepay before you’ve been approved, or sells research peptides or non-prescribed products.
| Red flag | Why it matters |
|---|---|
| 🚩 Claims compounded medication is FDA-approved | Compounded drugs are not FDA-approved as finished products. |
| 🚩 Says compounded is "the same as" Ozempic, Wegovy, or Zepbound | FDA has objected to misleading compounded GLP-1 marketing claims. |
| 🚩 Questionnaire with no licensed clinician review | Async intake is fine when a licensed clinician actually reviews it. The red flag is no clinician review at all. |
| 🚩 No pharmacy disclosure | You should be able to verify the dispensing pharmacy. |
| 🚩 No cancellation terms | Double-billing risk. |
| 🚩 Guaranteed weight-loss claims | Unsupported and a major trust signal. |
| 🚩 Sells research peptides or non-prescribed products | Outside legitimate care entirely. |
| 🚩 Requires long prepay before approval | Financial risk if you're not approved. |
FDA has specifically warned consumers about fraudulent compounded GLP-1 products, dosing errors, and misleading claims. Use FDA.gov’s BeSafeRX tool to verify any pharmacy before paying.
Higher-Risk Scenarios: Talk to a Clinician First
Some situations are clinical decisions, not shopping decisions. If any of these apply to you, talk to a licensed clinician before you switch:
Do not overlap GLP-1 medications unless a licensed clinician specifically directs it. Wegovy’s prescribing information warns against use with other semaglutide-containing products or other GLP-1 receptor agonists.
What We Actually Verified (And What We Couldn’t)
| Claim type | Acceptable source |
|---|---|
| Pricing | Provider pricing page, checkout page, customer support confirmation |
| Transfer / dose-continuation policy | Provider published policy, support documentation |
| Cancellation terms | Provider cancellation page, terms of service |
| FDA / regulatory status | FDA.gov, manufacturer prescribing information, Federal Register |
| Medical safety | FDA, prescribing information, major medical institutions (UCLA, etc.) |
| Customer experience | Trustpilot, Consumer Affairs, BBB — used as service-experience signals only |
Still pending verification:
- Dose-continuation policies for Ro, MEDVi, SHED, Sesame, Enhance MD, Yucca, Hims, Hers, and Direct Meds (flagged in matrix above)
- Final Medicare GLP-1 Bridge implementation details (CMS publishing further guidance ahead of July 1 launch)
- Final outcome of the FDA 503B exclusion proposal (comment period closes June 29, 2026)
We commit to refreshing this page monthly for pricing and regulatory updates, and quarterly for full content review.
Frequently Asked Questions
- Can I switch GLP-1 providers without starting over?
- You can switch providers, but the new clinician decides whether to continue, lower, or restart your dose after reviewing your records. Same-molecule switches are usually easier to review than cross-molecule switches. Cross-molecule switches commonly require a restart or re-titration plan because there is no validated direct dose-conversion chart between semaglutide and tirzepatide.
- Should I cancel my current GLP-1 provider before applying to a new one?
- No. Gather your records and start the new intake first. Cancel only after you understand the new provider's approval, cost, and refill timeline — and ideally only after the new medication has shipped and arrived. Verify your current provider's cancellation notice period in your terms before doing anything.
- What documents do I need to switch GLP-1 providers?
- Your prescription label, current dose, full dose history, last dose date, side effects, any lab work, prior authorization documents, pharmacy information, billing history, and your current cancellation terms. Print or screenshot everything before you cancel — portal access may become limited after.
- Will a new provider honor my current dose?
- Some providers will review continuation; others may lower or restart. The strongest signal is whether the provider has a published transfer policy or an intake that explicitly collects your current medication and dose for clinician review. Most handle it case-by-case. Your odds of a smoother review improve with complete records.
- How long should I wait between providers when switching?
- Plan around your normal dosing interval and let the new clinician set the gap. Many weekly-injection switches are timed around the next scheduled dose. Cross-molecule changes, missed doses, side effects, and oral medications can change the plan. After five to seven days, the amount of medication in the body decreases by about half, but GLP-1 medications may not completely leave the system for 30 days per UCLA Health guidance.
- Can I switch from compounded semaglutide to brand-name Wegovy without restarting at 0.25 mg?
- Both products may involve the same molecule, but compounded semaglutide is not FDA-approved and is not automatically interchangeable with Wegovy. The new clinician decides whether to continue, lower, or restart based on your dose history, last dose date, tolerance, and medication source.
- What happens if I miss two weeks of my GLP-1 before switching?
- Contact a licensed prescriber before resuming your old dose. UCLA Health's published guidance specifically recommends provider contact for gaps approaching two weeks, because some patients may have adverse effects if they restart at the same dose. The clinician decides whether to continue, lower, or restart.
- Can I use two GLP-1 providers at once?
- Do not overlap GLP-1 medications unless a licensed clinician specifically directs it. Wegovy's prescribing information warns against use with other semaglutide-containing products or other GLP-1 receptor agonists.
- Will switching providers reset my insurance deductible?
- No. Your deductible and out-of-pocket maximum track with your plan year, not your prescriber. Prior authorization may need to be resubmitted, but your accumulator resets do not.
- Will my prior authorization carry over?
- Prior authorization rules are plan-specific. Staying on the same medication may avoid a brand-new medication PA, but the plan may still require updated prescriber information, documentation, or a new submission. Brand-capable providers like Ro have insurance concierges that handle this.
- What is the cheapest way to switch GLP-1 providers in 2026?
- Depends on your path. For continuing on a compounded path with a low first-month price: Embody (from $99 first month for semaglutide injection, then $299 per month ongoing; compounded tirzepatide injection $149 first month, then $399 per month). For switching to brand-name through telehealth: Ro ($39 first month, then $74 per month with annual prepay) for the membership, plus medication cost. For direct cash-pay brand: NovoCare Wegovy at $149 to $349 per month depending on formulation, or LillyDirect Zepbound vials from $299 per month.
- Does the April 2026 FDA proposal force me to switch right now?
- No. The proposal is in a public comment period through June 29, 2026, and it specifically targets the 503B Bulks List — the bulk-substance pathway for outsourcing facilities. Broad mass-compounded availability is narrowing, and switching to a provider that gives you durable access to FDA-approved brand-name medication if compounded availability tightens further is the practical move.
- What if I am on a prepaid 3-month plan?
- Most prepaid plans do not refund unused months once medication has shipped. Time your switch for the end of your current paid cycle to avoid double-paying. If you are more than 30 days from your renewal date, you can usually use your remaining shipped medication while the new provider's onboarding completes.
- Can I switch from injection to a GLP-1 pill?
- Yes. Foundayo (orforglipron) was FDA-approved on April 1, 2026 as an oral once-daily GLP-1 for chronic weight management. Wegovy is also available as an FDA-approved oral tablet. Both are FDA-approved. Compounded oral or sublingual products are not FDA-approved and are not the same as those approved oral medications.
- What if my current provider will not release my records?
- Federal HIPAA rules give you the right to a copy of your medical records, and providers normally have up to 30 days to provide it per HHS Office for Civil Rights guidance. Most telehealth platforms allow direct download from the patient portal — get this before you cancel. If they refuse, you can file a complaint with HHS Office for Civil Rights at hhs.gov/ocr.
- Can I switch if my BMI is lower now?
- Some providers may evaluate maintenance patients; criteria vary. The qualifying conversation is different for transferring patients than new patients. Bring your starting BMI, current BMI, treatment history, dose response, and maintenance goal. Providers whose intake explicitly collects your current dose and treatment history for licensed-provider review make this smoother than providers without one.
What Happens After You Click
Four primary paths based on your scenario:
Still not sure which GLP-1 program is right for you?
Answer 5 questions about your current medication, your reason for switching, your insurance status, and your timeline — and we’ll match you with the provider lane that fits your specific situation. No email required.
Take the 60-Second GLP-1 Switch Quiz →Free. No email required. No pressure.
Whatever you do next, do it in this order: document, time, match, verify. That’s how you switch GLP-1 providers mid-treatment without losing dose continuity, paying twice, or restarting from zero.
Related guides
Key Sources Cited on This Page
- FDA Press Announcement: Foundayo (orforglipron) approval, April 1, 2026
- FDA Press Announcement: Proposed exclusion of semaglutide, tirzepatide, and liraglutide from 503B Bulks List, April 30, 2026
- Federal Register: List of Bulk Drug Substances for Which There Is a Clinical Need Under Section 503B, May 1, 2026
- FDA Warning Letter 721455 issued to MEDVi LLC, February 20, 2026
- FDA: “FDA’s Concerns with Unapproved GLP-1 Drugs Used for Weight Loss”
- Hims & Hers Strategic Shift announcement, March 2026
- Embody (joinem.co): program pricing, plan details, and intake information
- Ro Weight Loss Pricing (ro.co/weight-loss/pricing, May 2026)
- Wegovy Prescribing Information (wegovy.com/prescribing-information)
- Zepbound Prescribing Information (accessdata.fda.gov)
- UCLA Health: “Missed a dose or more of your GLP-1 medication? Here’s what to do.”
- HHS Office for Civil Rights: HIPAA right of access guidance (hhs.gov/hipaa)
- Pharmaceutical Journal, January 2026: “Switching between weight-loss medications”
- PMC: “Switching Between Glucagon-Like Peptide-1 Receptor Agonists: Rationale and Practical Guidance”
- CMS: Medicare GLP-1 Bridge program details
Medical disclaimer: Weight Loss Provider Guide is not a medical practice and this is not medical advice. This guide is informational. Only a licensed clinician can determine whether any GLP-1 medication — compounded or FDA-approved — is appropriate for you. Compounded GLP-1 medications are prepared by licensed compounding pharmacies and are not FDA-approved as finished products.
Weight Loss Provider Guide is an independent comparison resource for GLP-1 telehealth providers. We may earn a commission when readers start a program through our links. Editorial decisions and provider rankings are based on fit for the specific search intent and verified facts — not affiliate payout.
Last verified: .