GLP-1 Stomach Pain: When It’s Normal, When It’s a Red Flag, and What to Do Right Now
By Weight Loss Provider Guide Editorial Team · · · · Read time: ~12 min
Affiliate disclosure: Weight Loss Provider Guide is an independent comparison resource for GLP-1 telehealth providers. We may earn a commission if you choose a provider through a link on our site. That does not change our medical guidance, red flags, or what we tell you to do tonight.
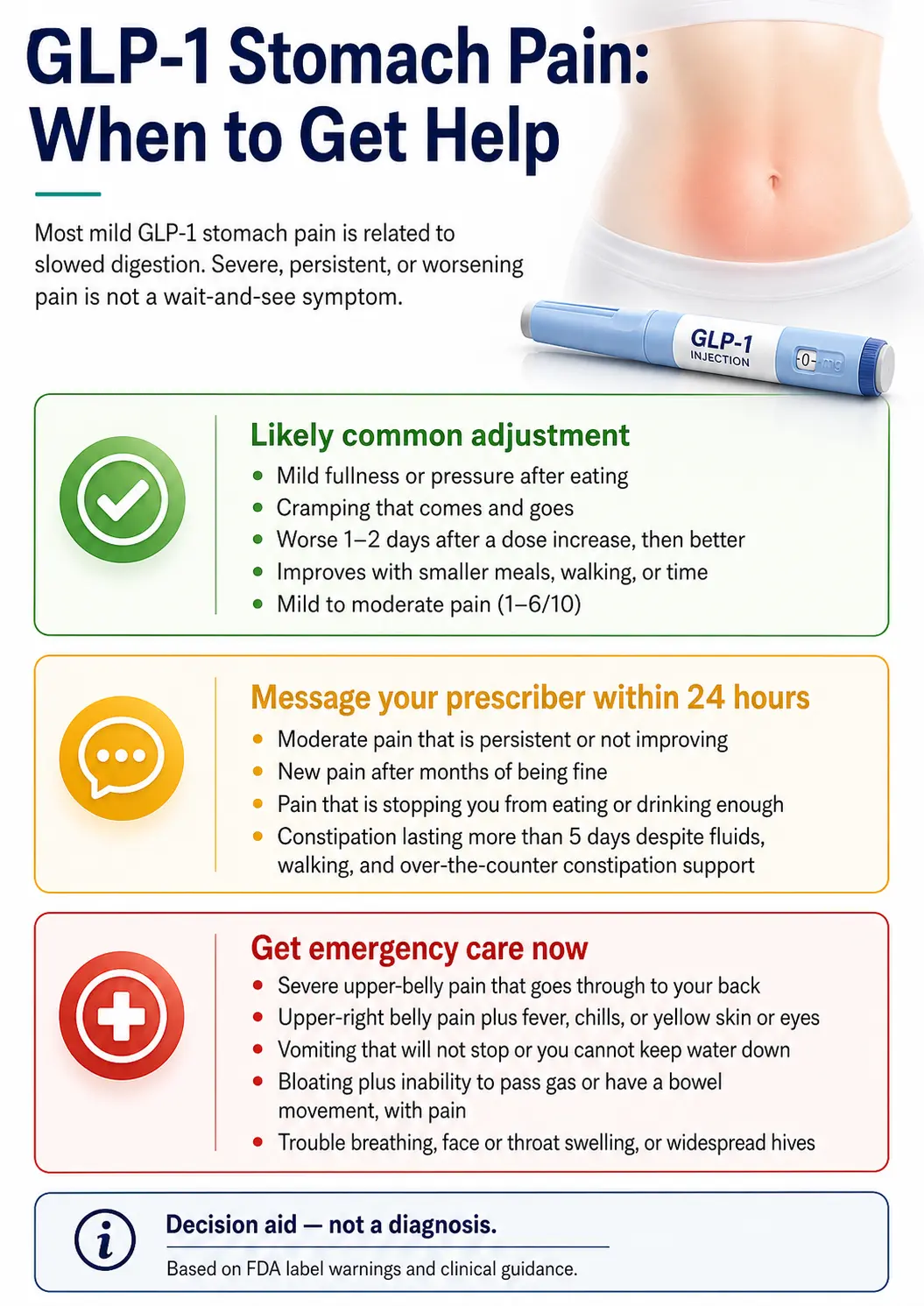
🚨 Stop and call 911 or go to the ER immediately if you have any of these:
- Severe pain in your upper belly that goes through to your back — the classic pancreatitis pattern flagged on every GLP-1 label
- Pain in the upper-right side of your belly plus fever, chills, or yellow skin or eyes — possible gallbladder
- Vomiting that won’t stop for 24+ hours, or you can’t keep water down — dehydration and kidney injury risk
- Bloating with the inability to pass gas or have a bowel movement, plus pain — possible obstruction or ileus
- Sudden severe pain that’s getting worse instead of better
- Trouble breathing, throat or face swelling, or hives all over — possible severe allergic reaction
Don’t tough it out. Don’t wait for your prescriber to call back.
Bottom line: Most GLP-1 stomach pain is your gut adjusting to a medicine that slows digestion on purpose. It usually shows up in the first few weeks, gets a little worse for a day or two after each dose increase, and fades. In FDA-approved clinical trials, abdominal pain hit about 9–10% of people on Zepbound, 5–7% on Ozempic, 10–11% on Rybelsus, 13–14% on Foundayo, and 20% on Wegovy. Most of it was mild. But pain that’s severe, won’t quit, and goes through to your back is a medical emergency — not a wait-and-see symptom.
60-Second Stomach Pain Triage
Three questions. Tells you whether to use the relief plan below, message your prescriber within 24 hours, or get medical help now. Built around FDA-stated red flags. Not a diagnosis — a decision aid.
60-Second Stomach Pain Triage
Decision aid based on FDA-published warnings. Not a diagnosis.
Question 1 of 3: Where is the pain?
If you prefer a table version, the “Where does it hurt?” section below covers the same routing logic.
What we actually verified for this guide
- ✅FDA prescribing information for Wegovy (revised 8/2025), Zepbound (revised 4/2026), Mounjaro, Ozempic, Rybelsus, and Foundayo — cross-checked rates and warnings
- ✅Wharton et al. multidisciplinary clinical-management consensus on GLP-1 GI side effects (Postgraduate Medicine, 2022)
- ✅NIH All of Us cohort cross-sectional analysis — GLP-1 GI adverse events in real-world patients
- ✅FAERS pharmacovigilance disproportionality analysis of GLP-1 GI adverse events, including pancreatitis signal by agent
- ✅FDA postmarket safety info on compounded GLP-1 products, including the April 30, 2026 proposed 503B bulks list exclusion
- ✅JAMA Network Open 2025 retrospective on GLP-1 discontinuation rates
Last verified: May 4, 2026.
Is GLP-1 stomach pain normal?
Short answer: Yes — for most people, mild-to-moderate stomach pain is a normal part of starting a GLP-1, and it usually gets better as your body adapts. It is not normal and not safe to ignore when the pain is severe, lasts for hours without easing, goes through to your back, or comes with vomiting that won’t stop.
Read both columns. Be honest with yourself about which one fits you better right now.
| Probably normal adjustment | Probably not normal — get help |
|---|---|
| ✓ Mild fullness or pressure after eating | ⚠ Severe pain (7+ on a 10 scale) |
| ✓ Cramping that comes and goes | ⚠ Constant pain that won't fluctuate |
| ✓ Worse 1–2 days after your shot, better after | ⚠ Pain that's getting steadily worse over hours |
| ✓ Improves with smaller meals, walking, or just waiting | ⚠ No relief from sitting, walking, or eating bland food |
| ✓ Mild to moderate (1–6 out of 10) | ⚠ Wakes you up from sleep with sharp pain |
| ✓ Pain stays in one area | ⚠ Pain that radiates from upper belly through to your back |
| ✓ You can still keep fluids down | ⚠ Vomiting that won't stop, or can't keep water down |
| ✓ No fever, no jaundice, no blood | ⚠ Fever, yellow skin or eyes, or blood in vomit/stool |
Mild belly pain on a GLP-1 is so common that the FDA puts it on the label of every approved GLP-1 covered here. In Wegovy’s adult weight-loss trials, severe GI reactions hit 4.1% of patients vs. 0.9% on placebo — meaning the vast majority of pain people felt was mild or moderate, not severe. The honest test: if the pain is interfering with your ability to eat, drink, sleep, or work — even at “moderate” — that’s enough reason to message your prescriber.
Why GLP-1s cause stomach pain in the first place
GLP-1 medications work by slowing how fast your stomach empties food into your small intestine. That same slowdown is what helps you feel full longer and lose weight — and it’s also what causes most stomach pain on these drugs. Slower digestion means food sits in your stomach longer, which can cause fullness, gas, cramping, constipation, and reflux.
Imagine your stomach is a bucket with a small hole in the bottom. Normally, food drips out at a steady rate. A GLP-1 makes the hole smaller. Food piles up. The bucket stretches. That stretch is what you’re feeling.
1. Slowed stomach emptying
Food stays in your stomach longer than your body is used to. You feel full after a few bites. You feel full six hours later. Pressure and fullness in your upper belly are the most common pain signal here.
2. Slowed transit through the gut → constipation
When digestion slows down everywhere, stool sits in your colon longer, and your colon pulls more water out of it. Hard stool. Cramping in the lower belly. Trapped gas. This is especially common because most people on GLP-1s also drink less and eat less fiber.
3. Higher rates of gallbladder and pancreas events
GLP-1s are associated with a small but real increase in gallstone problems and pancreatitis. In Wegovy’s adult trials, cholelithiasis was reported in 1.6% of patients vs. 0.7% on placebo, and cholecystitis in 0.6% vs. 0.2% (Wegovy prescribing information, 8/2025). Real, documented, on the label. We cover the warning signs in detail below.
GLP-1 stomach pain after your shot
Short answer: Stomach pain in the 24–72 hours after your weekly injection is the most common pattern, especially in the first weeks of treatment and right after a dose increase. The medication’s effect on stomach emptying is strongest during this window.
Most weekly GLP-1s — Wegovy, Zepbound, Mounjaro, Ozempic — reach peak effect a couple of days after injection, then taper. That timing matches what most people describe: feeling fine the day of the shot, then waking up uncomfortable on day 2 or 3.
What helps in this window:
- Eat smaller portions than feels “normal.” Half of what you’d usually eat is a good starting point.
- Stick to easier foods: eggs, broth, yogurt, plain toast, banana, plain rice.
- Walk a little after meals.
- Don’t lie flat for 2–3 hours after eating.
- Save anything fried, fatty, spicy, or carbonated for later in the week.
If your shot-day pain is severe, sudden, persistent, or paired with any red flag from the list above, the rule changes. Don’t wait it out — get medical care.
GLP-1 stomach pain after a dose increase
Short answer: Dose increases are the second most common pain trigger on GLP-1s. Symptoms usually return for 3–7 days after each step up, then settle as your body adapts to the higher dose.
Every FDA-approved GLP-1 uses a step-up dosing schedule for a reason: jumping straight to a maintenance dose causes severe GI reactions in too many people. The escalation lets your body adapt one step at a time. But the schedule on the box is a starting point, not a law.
The script is short:
“My stomach pain hasn’t fully resolved from the last increase. Can we stay at this dose another 4 weeks before going up?”
Most clinicians will say yes. Clinical-management guidance supports pausing escalation, holding at a lower dose, or slowing titration when GI symptoms are persistent or more severe.
Stomach pain rates by GLP-1 — what the FDA labels actually say
Short answer: Every FDA-approved GLP-1 lists abdominal pain as a common side effect. In clinical trials, the rates ran from about 5% on Mounjaro at lower doses up to 20% on Wegovy. But these aren’t apples-to-apples — different drugs, different doses, different patient populations, different trial designs.
GLP-1 abdominal pain rates from FDA-approved clinical trials
| Medication | Active ingredient | Trial population | Abdominal pain (drug vs. placebo) | Severe GI (drug vs. placebo) | GI discontinuation |
|---|---|---|---|---|---|
| Wegovy (injection) | semaglutide 2.4 mg/wk | Adults with obesity or overweight | 20% vs. 10% | 4.1% vs. 0.9% | — |
| Zepbound (injection) | tirzepatide 5/10/15 mg/wk | Adults with obesity or overweight | 9% / 9% / 10% vs. 5% | 1.7% / 2.5% / 3.1% vs. 1% | 1.9% / 3.3% / 4.3% vs. 0.5% |
| Mounjaro (injection) | tirzepatide 5/10/15 mg/wk | Adults with type 2 diabetes | 6% / 5% / 5% vs. 4% | 1.3% / 0.4% / 1.2% vs. 0.9% | 3.0% / 5.4% / 6.6% vs. 0.4% |
| Ozempic (injection) | semaglutide 0.5 / 1 mg/wk | Adults with type 2 diabetes | 7.3% / 5.7% vs. 4.6% | 0.4% / 0.8% vs. 0% | — |
| Rybelsus (oral) | oral semaglutide 7 / 14 mg/day | Adults with type 2 diabetes | 10% / 11% vs. 4% | 0.6% / 2.0% vs. 0.3% | 4% / 8% vs. 1% |
| Foundayo (oral) | orforglipron 5.5 / 9 / 17.2 mg/day | Adults with obesity or overweight | 13% / 14% / 14% vs. 7% | ~3% vs. 1% | 3% / 6% / 6% vs. 0.7% |
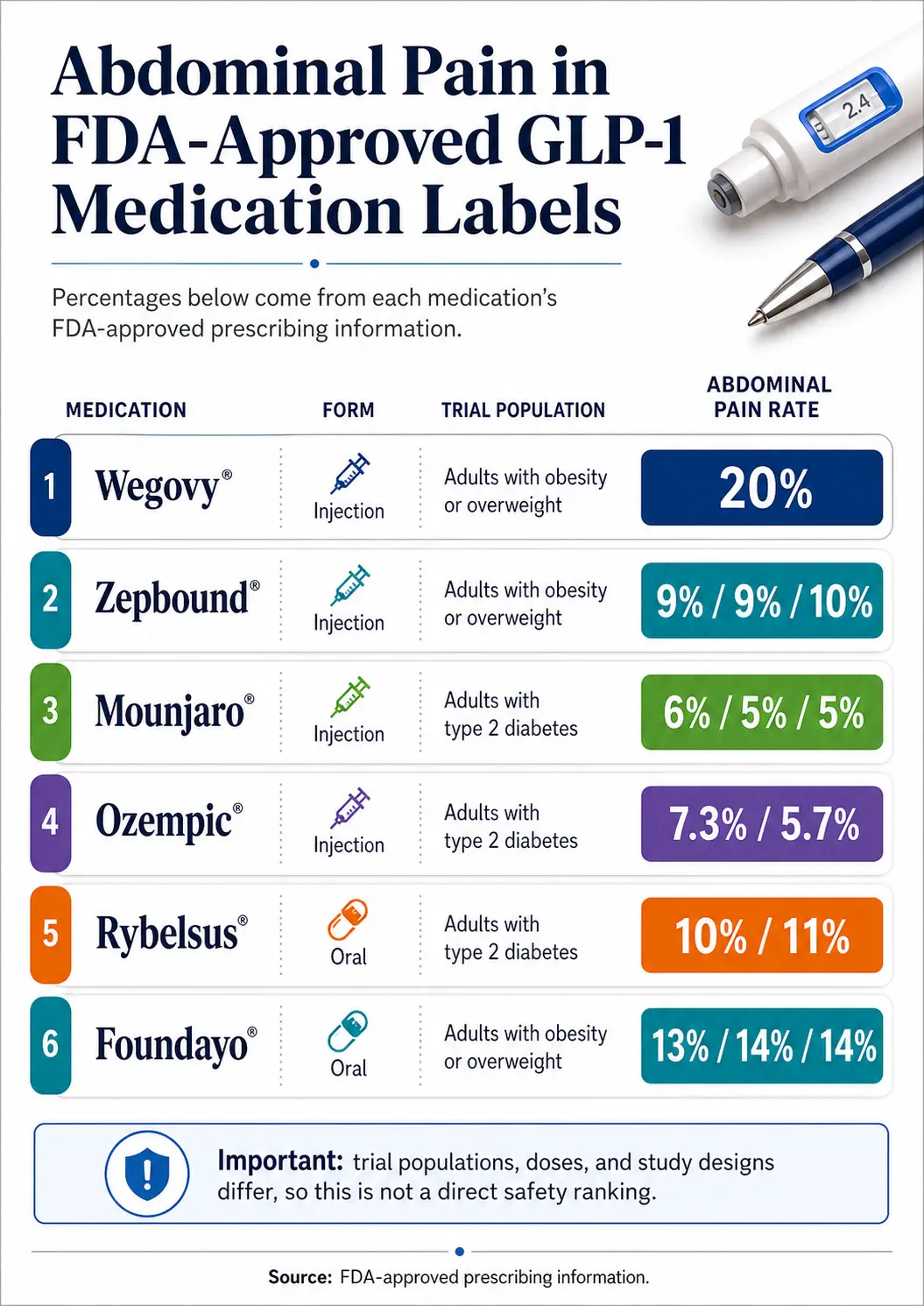
These trials measured different populations. Wegovy’s rate (20%) comes from weight-loss trials in adults with obesity. Mounjaro’s rate (5–6%) comes from diabetes trials. You can’t say “Wegovy is more dangerous than Mounjaro” from this table. You can say each label honestly reports abdominal pain at higher rates than placebo.
Most pain in trials was mild or moderate. Across all six drugs, severe GI reactions ran around 1–4% — meaning if you’re one of the 20% on Wegovy who had abdominal pain, the math says it was probably manageable, not severe.
Real-world rates look much higher. A cross-sectional analysis in the NIH All of Us database found chart-coded abdominal pain in 57.6% of patients. It’s retrospective coding, not adjudicated trial events, but it tells you that experiencing some abdominal pain on a GLP-1 is common.
The drug with the highest pancreatitis signal in pharmacovigilance is liraglutide. A FAERS analysis found liraglutide had a much higher reporting odds ratio for pancreatitis than newer agents. If you’re on liraglutide (Saxenda, Victoza) and have severe upper-belly pain, that’s an extra reason to take it seriously.
How long does GLP-1 stomach pain last?
Short answer: For most people, GLP-1 stomach pain peaks in the first 4–8 weeks and within 1–2 days after each dose increase, then fades as your body adapts. Pain that lasts more than 8–12 weeks at a stable dose, gets worse over time, or shows up brand new after months of being fine — that needs a prescriber conversation.
Week 1–2 (your first doses): Mild fullness, cramping, sometimes nausea. Most intense in the 24–72 hours after the first injection.
Week 3–4: Symptoms usually quiet down. Many people feel close to baseline.
Week 4 — first dose increase: Symptoms often come back for 3–7 days, then fade again. This is the most common “wait, is something wrong?” moment for new users. Usually nothing is wrong.
Each future escalation (weeks 8, 12, 16, 20): Same pattern — short-lived flare, then settles.
Maintenance dose (after week 20–24): Most people are largely symptom-free. If pain is still happening at maintenance, that’s worth flagging.
Pancreatitis timing is different and worth knowing
A pharmacovigilance review found the median time to onset was about 2.5 months, with a range from a few days up to three years. About 26% of those cases happened within three months of a dose increase. That’s why a sudden severe new pain after a dose change isn’t automatically “just power through” — it can be the early signal of something more serious.
The line between “expected” and “tell my prescriber”
- → Pain still present at the same dose for 3+ weeks without improvement message your prescriber
- → Pain getting worse over time at a stable dose message your prescriber
- → Brand-new pain after months of being asymptomatic message your prescriber
- → Pain stopping you from eating, drinking, or working message your prescriber
- → Severe, sudden, or red-flag-list pain don’t wait — get medical care now
Where does it hurt? The pain-location decision map
Short answer: Where the pain lives on your belly is one of the strongest clues to what’s happening. Upper-middle pain is usually slowed digestion. Upper-right pain with fever points at the gallbladder. Pain that radiates from your upper belly straight through to your back is the pancreatitis pattern. Lower-belly cramping is usually constipation and gas.
| Where it hurts | Most likely cause | Serious cause to rule out | First action |
|---|---|---|---|
| Upper middle, under the breastbone | Slowed gastric emptying, gastritis, reflux | Pancreatitis (especially if it radiates to your back) | If radiating to back → ER. Otherwise → small bland meals, antacid, walk. |
| Upper right, under the rib cage | Trapped gas | Gallbladder (cholecystitis or gallstones) — especially with fever, jaundice, or pain after fatty meals | If fever or yellowing → ER. Otherwise → gas relief, hydration. |
| Around the belly button or middle | Gas, distension from slowed transit | Bowel obstruction (rare, with vomiting + can't pass gas) | If can't pass gas + vomiting → urgent care or ER. Otherwise → walk + simethicone (Gas-X). |
| Lower belly / cramping | Constipation from slowed motility | C. diff or other infection (with diarrhea + fever) | Stool softener (MiraLAX), hydration, fiber slowly. |
| Anywhere → radiates to your back | Less likely a normal side effect | Pancreatitis | ER now. Don't take your next dose. |
| Generalized, all over | Often slowed everything + dehydration | Severe constipation, obstruction, or another systemic issue | Hydrate, rest, message prescriber within 24 hours. ER if severe. |
Built from FDA label warnings on pancreatitis, gallbladder disease, severe GI reactions, ileus, and obstruction. This map is decision support, not diagnosis. When in doubt, call your prescriber or 911.
Red flags: when to call your doctor vs. go to the ER
The FDA prescribing information tells patients to stop the medication and seek immediate care for severe abdominal pain that may radiate to the back — that’s the pancreatitis signal. Other red flags include upper-right pain with fever or jaundice (gallbladder), persistent vomiting (dehydration risk), and bloating with the inability to pass gas (possible obstruction).
🚨 The four scenarios that mean “ER now”
Scenario 1 — Possible pancreatitis
What it looks like: Severe, persistent upper-belly pain that spreads through to your back, with or without nausea or vomiting. The pain often gets worse lying flat and can feel a bit better leaning forward.
Why it’s serious: Pancreatitis is inflammation of the pancreas. It can become hemorrhagic or necrotizing. Mortality goes up the longer you wait.
What to do: Stop the medication. Don’t take another dose. Get to an ER. Ask for blood tests (lipase, amylase) and abdominal imaging.
Scenario 2 — Possible gallbladder problem
What it looks like: Pain in the upper-right side of your belly, often worse after a fatty or heavy meal, plus any of: fever, chills, yellowing of skin or eyes, dark urine, or pale/clay-colored stools.
Why it’s serious: Rapid weight loss raises gallstone risk. In Wegovy’s adult trials, cholelithiasis was reported in 1.6% of treated patients vs. 0.7% on placebo (Wegovy prescribing information, 8/2025). Real, documented, on the label.
What to do: Same-day ER. Bloodwork plus an abdominal ultrasound.
Scenario 3 — Severe dehydration / kidney injury risk
What it looks like: Vomiting that won’t stop, can’t keep fluids down for 24+ hours, dizziness on standing, dark urine, urinating much less than usual, dry mouth that won’t fix itself.
Special note for diabetes patients: If you take insulin or a sulfonylurea (like glipizide or glimepiride) along with your GLP-1, vomiting and not eating raises your hypoglycemia risk on top of dehydration risk. Check your blood sugar more often.
What to do: Urgent care or ER for IV fluids and electrolytes. Bring a current medication list.
Scenario 4 — Possible bowel obstruction or ileus
What it looks like: Severe bloating with the inability to pass gas or have a bowel movement, plus vomiting and worsening pain.
Why it’s serious: Slowed motility plus impaction can become surgical. Postmarketing reports for Mounjaro specifically include ileus and intestinal obstruction.
What to do: Same-day ER.
When to message your prescriber within 24 hours (not the ER)
- Pain at moderate level (4–6 out of 10) that’s persistent and not improving with the relief plan
- Brand-new pain after months of being symptom-free at a stable dose
- Pain that’s stopping you from eating or drinking enough
- Constipation lasting more than 5 days despite fiber, fluids, and walking
- Anything that just feels off and won’t quit
Some telehealth GLP-1 programs answer messages within an hour, 24/7. Others take 2–3 business days. If you’re in pain at 11 PM on a Sunday and can’t reach a clinician through your program, that’s information about your program — not a sign that your symptoms don’t matter.
The next-8-hours plan: what actually helps GLP-1 stomach pain
Short answer: If your symptoms aren’t on the red-flag list, this hour-by-hour plan combines the relief tactics most consistently recommended in clinical management guidelines and FDA label patient-counseling sections. The goal is simple: give your stomach less to do, hydrate, and reassess.
| Time | What to do | Why |
|---|---|---|
| Hour 0 — right now | Stop eating. Sip 4–8 oz of room-temperature water slowly. Sit up. Don't lie flat. | Reduces stomach pressure and lets the stomach work without adding load. |
| Hour 0–1 | Walk slowly for 10–15 minutes if you can. | Gentle movement may help gas pass and ease bloating. |
| Hour 1 | OTC: simethicone (Gas-X) for trapped gas; an antacid (Tums) or famotidine (Pepcid) if it feels like reflux. Don't use NSAIDs — see safety note below. | Targets the most common immediate cause. |
| Hour 2 | If hungry, eat half a cup of bland low-fat food: plain crackers, plain toast, banana, plain rice, broth. | Low-fat, low-fiber foods clear the stomach faster. |
| Hour 2–4 | Keep sipping water. Try ginger tea. (Peppermint can worsen reflux for some — switch if so.) | Hydration helps prevent constipation. Ginger has modest evidence for nausea and indigestion. |
| Hour 4 | If pain is improving — eat small bland meals every 2–3 hours rather than one bigger meal. | Smaller portions = less stomach distension. |
| Hour 8 | If pain is not improving, message your prescriber. If pain is getting worse, recheck the red-flag list or seek care. | Persistent worsening at hour 8 means a clinician needs to be in the loop. |
Safety note on pain relievers
Don’t use ibuprofen, naproxen, or aspirin for GLP-1 stomach pain unless your clinician says they’re safe for you. NSAIDs can irritate the stomach lining and make symptoms worse. Do not stop prescribed aspirin or any other prescribed medication on your own. Acetaminophen (Tylenol) is generally a safer over-the-counter pain option for most people, but ask your prescriber or pharmacist what fits your medical history.
Avoid for at least 24–48 hours
- Greasy, fried, or high-fat foods (fast food, pizza, fries, heavy cheese)
- Spicy food
- Carbonated drinks (more gas)
- Alcohol (irritates stomach lining, worsens dehydration)
- Large meals — even of healthy food
- Lying down within 2–3 hours of eating
- Eating and drinking at the same time
Longer-term moves that break the cycle
- Ask your prescriber about pausing your next dose increase
- Talk to your prescriber about injecting in the evening (sleep through the peak window)
- Consider switching agents with prescriber guidance if one drug isn’t working
- Walk daily — light movement after meals helps gas and constipation
Copy-paste this message to your prescriber
Fill in the brackets and send through your patient portal or telehealth app. Gives your clinician everything they need to triage you fast — no back-and-forth.
If your symptoms include any of the ER red flags above, don’t wait for a reply. Call 911 or go to the emergency room first.
Should you skip your next GLP-1 dose?
Short answer: Don’t make dose changes on your own unless you have a red-flag symptom or unless an emergency clinician tells you to. For ordinary GLP-1 stomach pain, the smarter moves are to slow your dose-escalation schedule, apply the relief plan, and message your prescriber.
The FDA labels don’t tell people to discontinue GLP-1s for ordinary GI symptoms. They do tell people to discontinue if pancreatitis is suspected.
Real discontinuation context from research
A 2025 JAMA Network Open retrospective found GLP-1 discontinuation among patients without type 2 diabetes was 64.8% at 1 year and 84.4% at 2 years. Among patients with type 2 diabetes it was 46.5% at 1 year and 64.1% at 2 years. You’re not alone if this is a struggle. But people who do well long-term are usually the ones who slow down titration when their bodies tell them to — not the ones who power through.
If you and your prescriber agree to pause: the typical restart is to resume at your previously tolerated dose — not your peak dose — and re-titrate slowly. Restarting at your old high dose after even a short break can produce the same intense early-week symptoms you had at the start.
Injection-site soreness vs. GLP-1 stomach pain
Injection-site reaction (on the skin)
- Pain, redness, or a small bump where the needle went in
- On your belly, thigh, or upper arm surface
- Mild, stays in one spot, fades in a few days
- You can press the spot and it’s tender
- Usually resolves on its own
Fix: Rotate sites with each shot. Let the pen warm to room temperature before injecting.
GLP-1 stomach pain (internal)
- Pressure, cramping, or sharp pain inside your abdomen
- Often after eating or after a dose increase
- Coming from somewhere your finger can’t reach
- May radiate to different areas
- Use the location map and red-flag list above
This is the GI side-effect pattern this whole page is about.
What to eat (and avoid) when your stomach hurts on a GLP-1
Smaller, slower, lower-fat meals are easier on a stomach that’s emptying slowly. Big greasy meals are not.
Easier on a sore GLP-1 stomach
- Plain rice, plain toast, plain crackers
- Bananas, applesauce, soft pears
- Eggs (scrambled, soft-boiled, or poached)
- Plain Greek yogurt
- Broth or clear soup
- Lean grilled chicken or fish in small portions
- Oatmeal (plain, not loaded with sugar)
- Smoothies (low-sugar, with protein)
Harder on a sore GLP-1 stomach
- Pizza, fried food, anything heavy in cheese
- Steak, ribs, and other dense fatty meats
- Spicy food
- Raw cruciferous vegetables in big quantities
- Carbonated drinks
- High-sugar desserts and sweets
- Big late-night meals
- Anything you’d describe as “rich”
Shot-day food trigger map
| If you’re feeling… | Likely trigger | Easier swap | Avoid | When to message |
|---|---|---|---|---|
| Stuffed and crampy after a normal-sized meal | Portion size for slowed emptying | Half-portion of the same meal | Large plates, all-you-can-eat | If it lasts more than a day at a stable dose |
| Burning under the breastbone | Reflux from food sitting longer | Smaller meals, stay upright after | Lying down within 2–3 hours of eating | If antacid doesn't help after 48 hours |
| Trapped gas, lower-belly cramping | Slowed transit + carbonation | Still water, simethicone, walking | Carbonated drinks, gas-producing foods | If you can't pass gas at all |
| Sharp pain a few hours after a fatty meal | Possible gallbladder | Lower-fat plate | Fried/greasy/heavy food | Same day, especially with fever or jaundice |
| "Eggy" or sulfur burps | Food fermenting in slow gut | Smaller portions of slower-digesting protein | Heavy red meat right after your shot | If paired with severe pain or vomiting |
Does compounded vs. brand-name GLP-1 matter for stomach pain?
Short answer: The red flags are exactly the same. Severe, persistent, back-radiating, vomiting, fever, jaundice, blood, or obstructive symptoms need medical care no matter where your medication came from. The difference is verification: brand-name GLP-1s are FDA-approved as finished drug products with quantified clinical-trial side-effect rates. Compounded semaglutide and tirzepatide are not FDA-approved as finished products.
A current regulatory update: On April 30, 2026, the FDA proposed excluding semaglutide, tirzepatide, and liraglutide from the 503B bulks list after finding no clinical need for outsourcing facilities to compound those products from bulk drug substances. Public comments were open through June 29, 2026. If finalized, this changes which compounded GLP-1 products outsourcing facilities can legally produce. Your provider should be able to tell you what specifically changes for you, if anything.
If you’re on compounded GLP-1 and have stomach pain:
- Keep your medication label, vial or pen, pharmacy name, prescriber name, and dose readily available. If you end up in an ER, they’ll need this info.
- If your symptoms are red-flag severe, treat them the same way you would on any GLP-1 — get medical care.
- If you’re getting product from a source that won’t tell you the pharmacy’s state license, won’t put a prescriber’s name on the label, or sells “research only” products, stop using it.
- Patients and clinicians can report adverse events or product-quality concerns to FDA MedWatch at fda.gov/medwatch or 1-800-FDA-1088.
What if GLP-1 stomach pain keeps happening every week?
Short answer: Recurring stomach pain isn’t a willpower problem. It usually means the dose is too high for you right now, the titration schedule is too fast, constipation isn’t being managed, the food plan doesn’t match the medication, or your program isn’t supporting you. All of those are fixable.
The four-question check on your current program
- When you message about side effects, do you hear back the same day?
- Has your clinician offered to slow titration, hold at your current dose, or step down?
- Are anti-nausea or constipation tools (like Zofran, MiraLAX) part of the conversation?
- If you needed help at 10 PM on a Saturday, is there a way to reach a real clinician?
If most of those answers are no, your current program isn’t doing its job. That’s not your fault. But it is information.
What “good” looks like — programs with strong side-effect support
We are Weight Loss Provider Guide, an independent comparison resource. We have affiliate relationships with the programs below — clearly disclosed, and placed here at the end of the page after all medical content. We’ve left some commonly mentioned providers off this specific page intentionally given ongoing FDA regulatory activity around compounded GLP-1 marketing. See our full provider comparison.
| Provider | Medication paths | Side-effect support | Pricing (verify at checkout) | Type |
|---|---|---|---|---|
| Embody | Compounded semaglutide & tirzepatide (injections or needle-free GLP-1 gum) | 24/7 care-team messaging and clinician oversight; fast online intake | Starting at $99 first month (semaglutide injection) then $299/mo ongoing; tirzepatide starts at $149 first month then $399/mo | Compounded |
| Ro (Ro Body) | FDA-approved brand-name only — Foundayo, Wegovy pill, Wegovy pen, Zepbound pen, Zepbound KwikPen, Ozempic | Insurance concierge handles prior-authorization paperwork; free GLP-1 Insurance Coverage Checker | Get started for $39, then as low as $74/month with annual plan paid upfront (or $149/month standard ongoing). Medication cost is separate from membership. | FDA-approved only |
Embody — fast intake, needle-free GLP-1 gum option
Embody is a cash-pay telehealth GLP-1 program for people who want a low starting price, fast online intake, and 24/7 support. They offer weekly semaglutide or tirzepatide injections, plus a needle-free GLP-1 gum option for those who are needle-averse. Plans start at $99 for the first month of semaglutide injection; standard refills run $299–$449/month depending on medication and form. HSA/FSA accepted.
Check Embody Eligibility →Ro (Ro Body) — FDA-approved only with insurance concierge
If you want the FDA-approved-only path with real insurance support — for any reason, including peace of mind around side effects — Ro is the cleanest route. Their insurance concierge is genuinely useful, especially if you have a plan that might cover Wegovy or Zepbound but the prior-authorization paperwork has been the wall. Get started for $39, then as low as $74/month with annual plan paid upfront; medication is billed separately.
Check GLP-1 Insurance Coverage with Ro (Free) →Not sure which GLP-1 program fits your situation?
Most people reading this aren’t ready to switch providers tonight. They’re trying to figure out what’s wrong and what to do. This quiz matches you to a program that fits your medication preferences, side-effect support needs, and budget. Takes 60 seconds. No login required.
Take the Free 60-Second Matching Quiz →Before you start a GLP-1: what to disclose to your prescriber
Short answer: Your baseline GI history matters. GLP-1 medications can worsen certain pre-existing digestive issues. Disclose any history of pancreatitis, gallbladder disease, gastroparesis, severe reflux, severe constipation, kidney disease, prior abdominal surgery, pregnancy plans, and any other GLP-1 you’ve taken before.
Tell your prescriber if you have or have had:
- Pancreatitis (any kind, any time)
- Gallstones, gallbladder removal, or any gallbladder surgery
- Gastroparesis or other delayed-emptying issues
- Severe acid reflux or known hiatal hernia
- Severe constipation, prior bowel obstruction, or chronic IBS-C
- Kidney disease or any prior episode of kidney injury
- Type 2 diabetes plus insulin or sulfonylurea use (hypoglycemia risk goes up)
- Pregnancy, breastfeeding, or plans to become pregnant — and ask for the drug-specific timing rule
- A prior bad reaction to any GLP-1
- An upcoming surgery or procedure with general anesthesia (GLP-1s slow stomach emptying and can affect anesthesia plans)
Five questions worth asking before your first dose:
- What stomach symptoms should I expect, and when?
- What symptoms mean I should stop the medication?
- Who do I message after hours if I’m worried?
- How slowly can we titrate?
- What’s the plan if I can’t tolerate the next dose increase?
If your prescriber doesn’t have clear answers to those five questions, you have a program problem, not a medication problem.
Frequently asked questions about GLP-1 stomach pain
- Is GLP-1 stomach pain dangerous?
- Usually not. Most GLP-1 stomach pain is mild to moderate and resolves as your body adapts. It becomes dangerous when it is severe, persistent, and radiates to your back — that is the pancreatitis pattern. It is also dangerous in combination with high fever, yellowing of the skin or eyes, persistent vomiting, blood, or the inability to pass gas or stool.
- Why does my stomach hurt right after my GLP-1 shot?
- GLP-1 medications slow how fast your stomach empties food into your small intestine. The effect is strongest in the 24 to 72 hours after each dose, especially after dose increases. Larger meals, fatty foods, lying flat after eating, and dehydration all make it worse during this window.
- How long does GLP-1 stomach pain last?
- For most people, it peaks in the first 4 to 8 weeks and within 1 to 2 days after each dose increase, then fades. Pain that lasts longer than 8 to 12 weeks at a stable dose, or that gets worse over time, warrants a prescriber conversation.
- What does GLP-1 pancreatitis feel like?
- Severe, persistent upper-belly pain that goes through to your back, often with nausea or vomiting that does not improve. The pain can get worse lying flat and feel slightly better leaning forward. It is a medical emergency. Stop the medication and go to the ER.
- Which GLP-1 has the least stomach pain?
- There is no GLP-1 that is stomach-pain-free. Across FDA-approved trial data, Mounjaro at lower doses had abdominal pain rates around 5 to 6 percent, and Wegovy at the 2.4 mg weight-loss dose had rates around 20 percent. But these are not apples-to-apples comparisons — different drugs in different patient populations at different doses. Personal tolerability varies a lot, and switching agents with prescriber guidance can sometimes help if one drug is not working for you.
- Can I take ibuprofen for GLP-1 stomach pain?
- Do not use ibuprofen, naproxen, or aspirin for stomach pain unless your clinician says they are safe for you. NSAIDs can irritate the stomach lining and make GI symptoms worse. Do not stop prescribed aspirin or any prescribed medication on your own. Acetaminophen (Tylenol) is generally a safer over-the-counter option for most people, but ask your prescriber or pharmacist what fits your medical history.
- Does GLP-1 stomach pain mean I have gastroparesis?
- Not necessarily. All GLP-1s slow gastric emptying — that is the mechanism. True gastroparesis (severe persistent delayed emptying with vomiting and inability to eat) is rare. If your symptoms are severe or persistent, your prescriber may order a gastric emptying study to look at it directly.
- Should I eat before or after my GLP-1 injection?
- The FDA labels for the major weekly GLP-1s allow once-weekly dosing at any time of day, with or without meals. Some patients find that injecting in the evening helps them sleep through the strongest peak-effect window. On shot day and the day after, smaller, lower-fat meals are typically better tolerated than heavy or fatty ones.
- Can compounded GLP-1s cause more stomach pain than brand-name?
- There is not equivalent clinical-trial data for compounded products, so a fair direct comparison cannot be made. The FDA has flagged dosing errors and safety concerns with compounded GLP-1 products, and on April 30, 2026 proposed excluding semaglutide, tirzepatide, and liraglutide from the 503B bulks list. If you are on compounded medication and your symptoms are severe, raise that specifically with your prescriber.
- Will my stomach pain go away if I lower my dose?
- Often, yes — at least partially. Pausing dose escalation or stepping back to your last tolerated dose, with prescriber guidance, is one of the standard management strategies in clinical guidelines. Do not change your own dose without a clinician in the loop.
- What over-the-counter options can help GLP-1 stomach pain?
- For trapped gas: simethicone (Gas-X). For reflux: antacids (Tums, Rolaids) or H2 blockers (famotidine/Pepcid). For constipation: osmotic laxatives like MiraLAX or stool softeners like Colace, with hydration and walking. Do not use NSAIDs (ibuprofen, naproxen, aspirin) for the stomach pain itself.
- Can I drink alcohol on a GLP-1?
- Alcohol is not formally contraindicated, but it can make stomach pain, dehydration, and reflux significantly worse. Many GLP-1 users find they no longer want it. If you do drink, keep amounts small and not on shot day or the day after.
- Does dehydration cause GLP-1 stomach pain?
- Indirectly, yes. Dehydration makes constipation worse, and constipation cramps are one of the most common pain drivers on GLP-1s. It also raises kidney injury risk — Wegovy, Ozempic, Zepbound, and Mounjaro labels all carry warnings about acute kidney injury in patients with GI reactions causing volume depletion. Sip water throughout the day, even when you are not thirsty. Your thirst signal is partially blunted on a GLP-1.
- Is sulfur burping on a GLP-1 a sign of something serious?
- Usually not on its own. Sulfur burps come from food fermenting longer in your gut because digestion is slowed. They are unpleasant, but they are not an emergency. They become worth flagging when paired with severe pain, vomiting, or any of the red flags above.
Most GLP-1 stomach pain is your gut adapting to a medication that’s working. Some of it is a warning sign of something serious. The difference matters — and now you know what each one looks like.
If you’re still feeling the pain right now and you’ve already ruled out the red flags, work the next-8-hours plan and message your prescriber in the morning. If the pain is severe and won’t quit, especially if it goes through to your back — close this tab and get to an ER.
Still not sure which GLP-1 program is right for you?
We’ll match you to programs that fit your medication preferences, side-effect support needs, and how you want to pay. No login required. No surprise charges. Less than a minute.
Find My GLP-1 Path →Free. No spam. No pressure.
Sources
- Wegovy (semaglutide injection) prescribing information — revised 8/2025
- Zepbound (tirzepatide) prescribing information — revised 4/2026
- Mounjaro (tirzepatide) prescribing information
- Ozempic (semaglutide) prescribing information
- Rybelsus (oral semaglutide) prescribing information
- Foundayo (orforglipron) prescribing information following FDA approval, April 1, 2026
- Wharton et al., “Managing the gastrointestinal side effects of GLP-1 receptor agonists in obesity.” Postgraduate Medicine, 2022
- González-Lleó et al., “Clinical Recommendations to Manage GI Adverse Events in Patients Treated with GLP-1 RAs.” Journal of Clinical Medicine, 2023
- NIH All of Us cohort cross-sectional analysis — GLP-1 RA-associated GI adverse events. Pharmaceuticals, 2024
- FAERS pharmacovigilance disproportionality analysis of GLP-1 RA GI adverse events
- Discontinuation and reinitiation of dual-labeled GLP-1 receptor agonists — JAMA Network Open, 2025
- FDA postmarket drug safety information on unapproved/compounded GLP-1 drugs
- FDA proposed rule excluding semaglutide, tirzepatide, and liraglutide from the 503B bulks list, April 30, 2026
- NIDDK symptom resources for gallbladder disease and gastroparesis
Related guides
How this guide was built and why
This page exists because none of the top results for “GLP-1 stomach pain” combined what most people actually need: a triage decision they can use in the next 60 seconds, drug-by-drug FDA-label rates side by side, an hour-by-hour relief plan, and a prescriber message script — all in one place.
We pulled directly from the current FDA prescribing information for every major GLP-1 approved through May 2026. We cross-referenced trial rates against pharmacovigilance data and the NIH All of Us cohort study. We used the multidisciplinary clinical-management consensus paper as our framework for the relief plan. We used Reddit and forum posts only to capture how real people describe their symptoms — never as medical evidence.
Medical disclaimer: This guide is educational and is not a substitute for medical care from a licensed clinician. The triage tool is a decision aid, not a diagnosis. If you are experiencing a medical emergency, call 911 or go to your nearest emergency department. To report a side effect or product-quality concern with any GLP-1 medication, contact FDA MedWatch at fda.gov/medwatch or 1-800-FDA-1088.
Weight Loss Provider Guide is an independent comparison resource for GLP-1 telehealth providers. We may earn a commission if you sign up through our links. That does not change our medical guidance or our recommendations.
Last verified:
Related Articles
GLP-1 Sulfur Burps: Drug-by-Drug Data, Relief & Red Flags
On a GLP-1 and getting rotten-egg burps? Here's why it happens, what actually helps, and the FDA-label data drug by drug. Verified May 2026.
GLP-1 Vomiting: Normal, Dangerous, or an Emergency?
Throwing up on a GLP-1? 30-second triage, red flags, 48-hour recovery plan, and FDA-label vomiting rates by drug — fact-checked, no fluff.
GLP-1 Food Aversion: What to Eat When Nothing Sounds Good
Rescue Matrix matched to your exact trigger (smell, taste, texture, nausea, fullness), 24-hour tracks, FDA label dysgeusia data for all four drugs. Verified July 2026.
GLP-1 Took Too Much? What to Do Right Now
Took too much GLP-1? Call Poison Help at 1-800-222-1222. Exact 911 signs, what information to have ready, overdose symptoms by drug, half-life table, compounded-vial risks, and the Three-Check prevention system.
GLP-1 Fatigue: Why You're Tired + What Actually Helps
GLP-1 fatigue rates by medication, the four patterns that cause it, the 7-day reset, and when tiredness is a clinician call. Verified against FDA information.
Medical Necessity for Panniculectomy: Checklist
What insurers actually require to cover a panniculectomy in 2026: pannus grade, the 3-month treatment rule, photos, CPT 15830, and a free readiness check.