Affiliate Disclosure | Medical Disclaimer | Sources cited throughout
Need help now?
- SAMHSA National Helpline: 1-800-662-4357 (free, confidential, 24/7)
- Crisis and Suicide Lifeline: 988
- FindTreatment.gov — locate treatment near you
- This page is an educational resource, not a substitute for medical care.
GLP-1 and Addiction: What the Research Actually Shows Right Now
By WPG Research Team | Research Verified: March 9, 2026
GLP-1 and addiction — here is the most important thing we can tell you upfront: GLP-1 medications like Ozempic, Wegovy, and Mounjaro are not FDA-approved to treat addiction. But here's why researchers and patients alike are paying serious attention.
A March 2026 cohort study of 606,434 U.S. veterans with type 2 diabetes, published in The BMJ, compared people taking GLP-1 receptor agonists to those on SGLT2 inhibitors over three years. Among veterans with pre-existing substance use disorders, GLP-1 users were associated with 50% fewer substance-related deaths and 39% fewer overdoses. [1] These are associations, not proof of causation — but the signal was consistent across every major addictive substance tested.
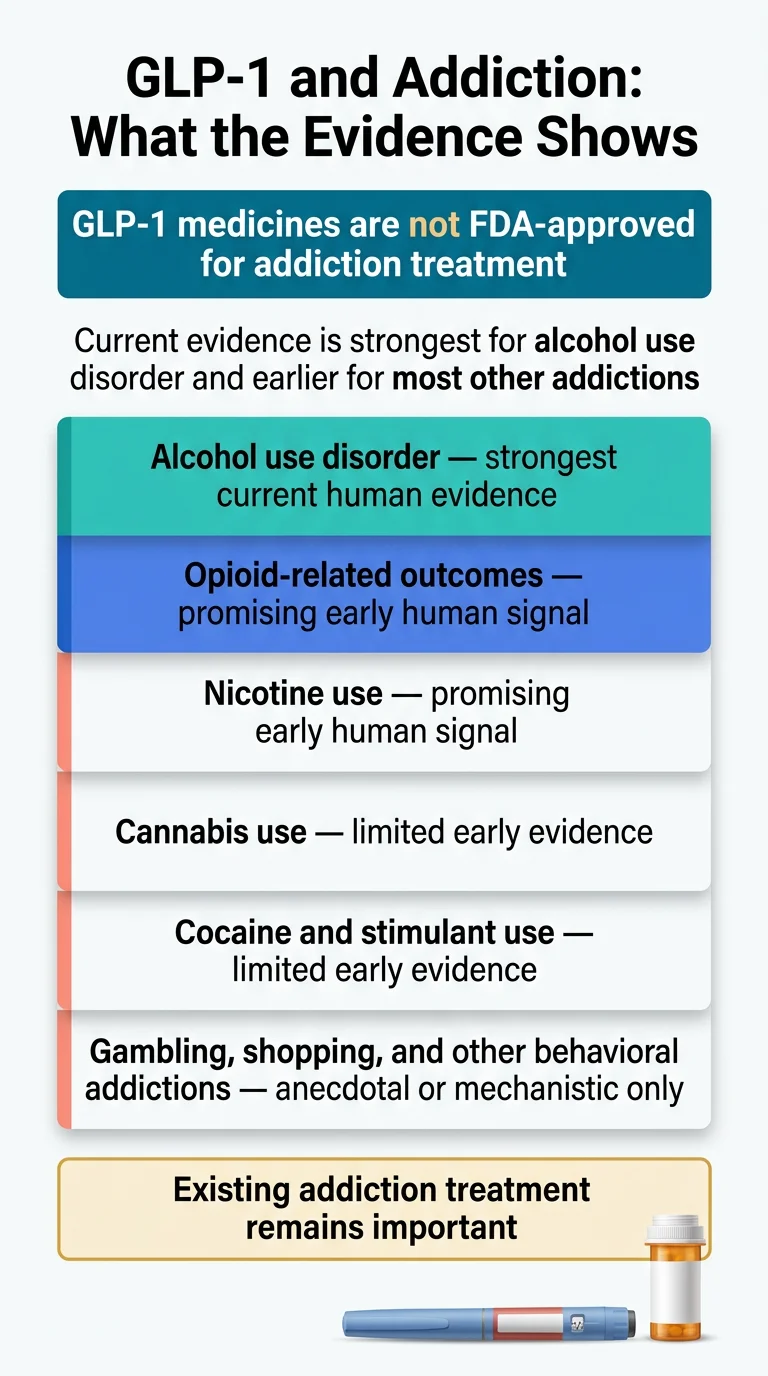
Here's how the current evidence actually breaks down: strongest human evidence for alcohol use disorder (observational studies + one positive randomized trial) [2]; promising but preliminary for opioid- and nicotine-related outcomes (large observational data, clinical trials underway); observational or preclinical only for cannabis and cocaine; anecdotal and mechanistic only for gambling, compulsive shopping, and other behavioral addictions.
GLP-1 and Addiction: Evidence at a Glance
GLP-1 medications are showing real signals for craving reduction across multiple substances. The strongest evidence is for alcohol use disorder. For other addictions, the research is earlier but growing fast.
| Addiction Type | Best Human Evidence | Evidence Strength | FDA-Approved? | Practical Takeaway |
|---|---|---|---|---|
| Alcohol | Large observational studies + Phase 2 RCT | Strongest current human signal | No | Talk to your doctor if you have both AUD and obesity/metabolic issues. |
| Opioids | Large observational studies; trials underway | Promising but preliminary | No | Encouraging data on overdose reduction. Don't replace buprenorphine/methadone. |
| Nicotine | Observational + small trials | Promising but preliminary | No | May reduce cigarettes/day. May prevent post-quit weight gain. |
| Cocaine | Observational only; one small negative trial | Early | No | No FDA-approved cocaine addiction med exists, so interest is high. |
| Cannabis | Observational only | Early | No | Some signal, but thin. No clinical trials yet. |
| Gambling / Shopping | Anecdotal + mechanistic plausibility | Anecdotal only | No | Intriguing reports, but no formal studies. |
| Appetite / food preoccupation | Obesity and weight-management trials | Established for weight management | Yes, for obesity/weight management only | “Food noise” reduction is common, but that is not the same as an addiction indication. |
Evidence graded by WPG Research Team based on study type, sample size, and replication. Research verified March 2026.
Exploring GLP-1 treatment for an approved reason like obesity or type 2 diabetes? Take our free 60-second eligibility quiz to compare legitimate care options. Any craving-related effects are not an FDA-approved addiction indication.
Why Is Everyone Suddenly Talking About GLP-1s and Addiction?
The conversation didn't start in a lab. It started in doctor's offices, Reddit threads, and kitchen tables.
People prescribed Ozempic or Mounjaro for diabetes or weight loss started noticing something unexpected: they didn't just lose interest in food. They lost interest in alcohol. In cigarettes. In the compulsive pull of online shopping. Some described it as the moment the “noise” in their head went quiet — not just food noise, but all of it.
“I didn't set a quit date. I simply lost interest,”
one veteran told his doctor after starting a GLP-1 for diabetes, describing how he'd tried to stop smoking for over a decade. That doctor was Ziyad Al-Aly, MD, a clinical epidemiologist at Washington University in St. Louis — and those conversations eventually led him to design one of the largest addiction studies ever conducted.
These weren't isolated stories. A 2024 analysis of nearly 70,000 Reddit posts about GLP-1 medications found that among 1,580 posts mentioning alcohol, 71% reported reduced cravings and decreased desire to drink. That's a striking number, even accounting for self-selection bias (people who didn't notice a change are less likely to post about it).
For years, the evidence was mostly patient stories, animal studies, and small observational datasets. Then, in rapid succession, larger studies arrived. A Swedish nationwide analysis of 227,000 people. Cohort studies at major U.S. institutions. And in early March 2026, the WashU study — 600,000+ patients, published in The BMJ — delivered the most comprehensive signal yet.
Here's what the internet often gets wrong: the stories are real, but they're getting ahead of the science. What we have is a strong, growing, and biologically plausible signal — not a proven treatment. The distinction matters, and we'll be precise about it throughout this guide.
Are GLP-1 Drugs FDA-Approved for Addiction Treatment?
No. As of March 2026, no GLP-1 medication has FDA approval for any addiction indication. Not for alcohol. Not for opioids. Not for nicotine. Not for any other substance or behavioral addiction.
This is the single most important fact to anchor in your mind as you read everything that follows. GLP-1 medications are currently FDA-approved for the following primary uses:
| Drug (Generic) | Brand Names | Key FDA-Approved Uses | Approved for Addiction? |
|---|---|---|---|
| Semaglutide (injection) | Ozempic, Wegovy | Type 2 diabetes, cardiovascular risk reduction, chronic kidney disease risk (Ozempic); Chronic weight management, cardiovascular risk reduction (Wegovy) [12] | No |
| Semaglutide (oral) | Rybelsus | Type 2 diabetes | No |
| Tirzepatide (dual GIP/GLP-1) | Mounjaro, Zepbound | Type 2 diabetes (Mounjaro); Chronic weight management, obstructive sleep apnea (Zepbound) [12] | No |
| Liraglutide | Victoza, Saxenda | Type 2 diabetes, cardiovascular risk reduction (Victoza); Chronic weight management (Saxenda) | No |
| Dulaglutide | Trulicity | Type 2 diabetes, cardiovascular risk reduction | No |
| Exenatide | Byetta, Bydureon | Type 2 diabetes | No |
Source: FDA prescribing information for each medication.
Any use of a GLP-1 for addiction is considered off-label — meaning a doctor can legally prescribe it for this purpose, but insurance usually won't cover it for that reason alone, and the evidence doesn't yet meet the bar for FDA approval.
Some addiction specialists are already prescribing GLP-1s off-label, particularly for patients who also qualify for weight management. Dr. Anna Lembke, professor of psychiatry at Stanford Medicine and author of Dopamine Nation, has said she currently uses GLP-1s to treat addiction related to alcohol and food. But she's also been clear: the evidence is early, and not everyone responds.
Multiple clinical trials are underway that could eventually support an FDA application. For now, know this: promising is not the same as proven, and association is not causation. We'll be honest about where the line is throughout this guide.
How Could GLP-1 Medications Affect Addiction in the Brain?
This is where things get genuinely fascinating — and where the biological plausibility for the craving-reduction reports becomes harder to dismiss.
What GLP-1 Does in Your Body
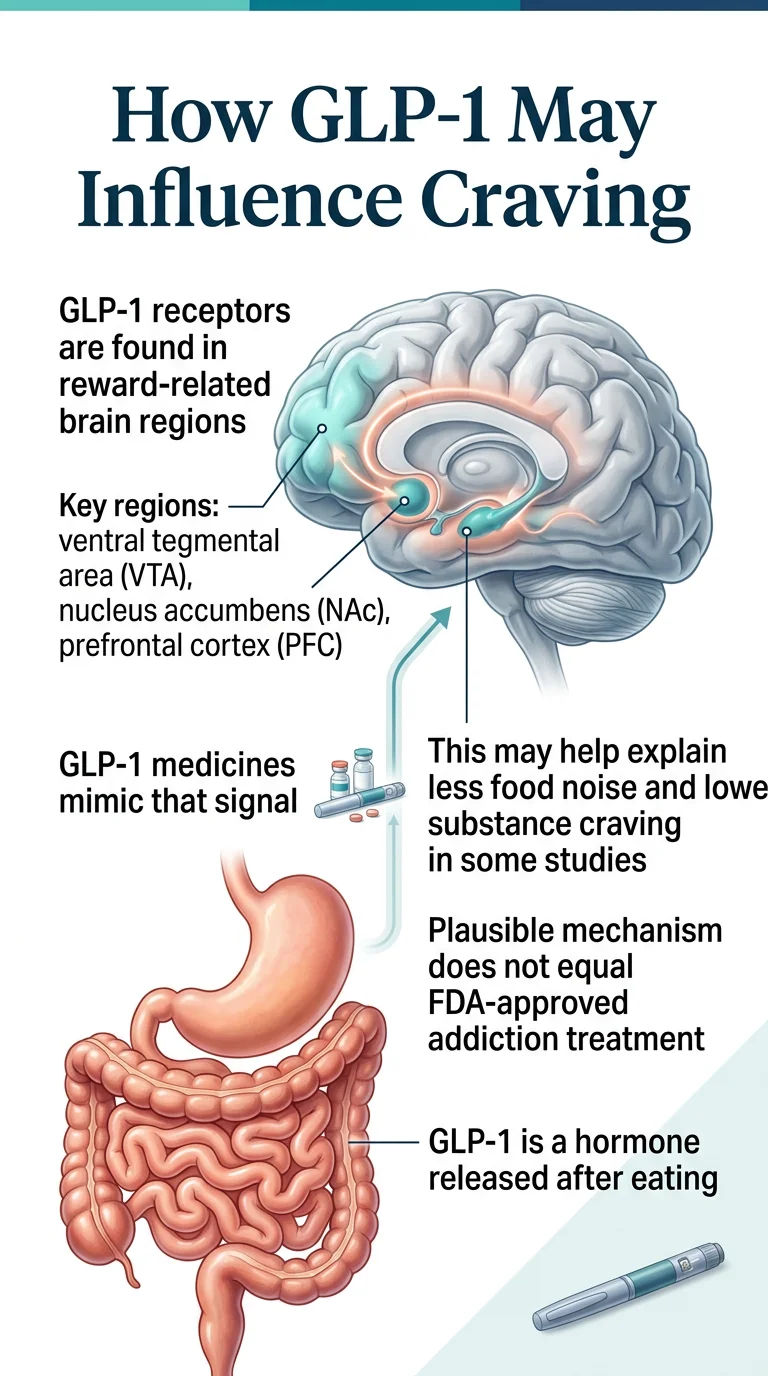
GLP-1 (glucagon-like peptide-1) is a hormone your small intestine naturally releases after you eat. It signals your pancreas to produce insulin, slows the emptying of your stomach, and tells your brain you're full. GLP-1 medications mimic this hormone, but at much higher and longer-lasting levels than your body produces on its own.
That's why they work so well for weight loss and blood sugar control. But here's the part most people miss: GLP-1 receptors aren't just in your gut and pancreas. They're also densely concentrated in specific regions of your brain — including the parts that control reward, motivation, and craving.
The Reward Pathway: Where Food Meets Drugs Meets Gambling
Your brain has a system called the mesolimbic reward pathway. It runs from the ventral tegmental area (VTA) to the nucleus accumbens — and it's powered primarily by dopamine, the neurotransmitter most people associate with pleasure.
Here's the key: this is the same circuit that drives craving for food, alcohol, nicotine, opioids, cocaine, gambling, and compulsive shopping. Addictive substances and behaviors hijack this system, flooding it with dopamine and creating the cycle of craving, use, temporary relief, and more craving.
GLP-1 receptors sit right in these brain regions. When GLP-1 medications activate these receptors, they appear to dampen dopamine signaling in the reward center. The substance or behavior becomes less rewarding — not aversive, just... less interesting.
This is a critical distinction. The drug doesn't make alcohol taste bad or cause nausea when you smoke (the way disulfiram makes you sick if you drink). It appears to reduce the disproportionate pull — the “wanting” that addiction researchers have identified as distinct from “liking.”
From “Food Noise” to “Drug Noise”
People on GLP-1s for weight loss commonly describe the disappearance of “food noise” — that constant mental chatter about what to eat next, when to eat, whether there's food nearby. It's not that food becomes unpleasant. It's that the obsessive preoccupation fades.
Dr. Al-Aly's hypothesis, based on his team's research, is that the same mechanism quiets what he calls “drug noise” — the relentless craving that drives addiction across substances. As he wrote in STAT News: “A drug designed for diabetes appears to quiet craving for substances with different mechanisms of action. That pattern suggests these addictions share a common biological driver.”
Animal research supports this. When researchers gave semaglutide to vervet monkeys — primates that voluntarily drink alcohol much like humans do — the monkeys drank significantly less. But they didn't show signs of nausea, and their water intake stayed normal. The drug didn't make alcohol aversive. It made alcohol uninteresting.
Why a Mechanism Isn't the Same as Proof
A plausible biological mechanism is necessary but not sufficient. We can explain why GLP-1s might reduce addiction, and that explanation makes sense. But plenty of mechanisms that “make sense” in theory don't hold up in large human trials. That's why the evidence section below matters more than the mechanism. Biology tells us this could work. The studies tell us whether it does.
What Does the Research Actually Show? A Substance-by-Substance Breakdown
This is the heart of this guide. We've graded the evidence for each substance based on four levels: Animal / Preclinical (laboratory studies), Observational (Human) (medical records analysis), Randomized Clinical Trial (Human) (gold standard), and FDA Approval (formally reviewed and approved).
GLP-1 and Alcohol Addiction
Verdict: The strongest human evidence of any substance. Promising, but not yet definitive.
Alcohol use disorder (AUD) is where the GLP-1/addiction conversation has the most data and the most momentum.
The Landmark 600,000-Patient Study (BMJ, March 2026)
Dr. Al-Aly and his team at Washington University analyzed health records from more than 600,000 U.S. veterans with type 2 diabetes over three years. They compared people who started GLP-1 medications to those who started SGLT2 inhibitors. Among people without a prior substance use disorder, GLP-1 users had an 18% lower risk of developing alcohol use disorder. Among those already struggling with AUD, GLP-1 users had significantly fewer hospitalizations, emergency visits, and deaths. [1]
Swedish Nationwide Study (227,000 People)
A Swedish analysis found that people with AUD who took GLP-1 medications had 36% fewer alcohol-related hospitalizations — more than double the 14% reduction seen with naltrexone, the best-performing medication that's actually approved for AUD in that same analysis.
Nature Communications Cohort Study (2024)
Semaglutide was associated with a 50–56% lower risk of both new and recurring alcohol use disorder diagnosis across 12 months, consistent across gender, age, race, and diabetes status. [3]
JAMA Psychiatry Randomized Trial (2025)
This Phase 2 trial — the first randomized controlled trial of semaglutide for AUD — randomized 48 adults with alcohol use disorder to receive low-dose semaglutide or placebo for 9 weeks. Semaglutide reduced the amount of alcohol consumed during a laboratory session and significantly reduced weekly craving compared to placebo. It also reduced cigarettes per day in a subgroup of participants who smoked. [2] This trial was small (48 participants) and short (9 weeks), so it's not definitive. But it's the first controlled human evidence that semaglutide directly reduces drinking behavior.
Reddit Self-Reports (Published Peer-Reviewed Analysis)
An analysis of 68,250 Reddit posts found that among 1,580 alcohol-related posts by GLP-1 users, 71% reported reduced cravings and decreased desire to drink. Self-reported, yes — but consistent with the clinical data.
What We Still Don't Know
- Whether the effects hold long-term (most studies are under 3 years)
- Whether cravings return when the medication stops
- Which patients respond best (and which don't respond at all)
- How GLP-1s interact with existing AUD medications like naltrexone
- Whether the effects are independent of weight loss
What this means today: If you have both alcohol use concerns and a qualifying condition for GLP-1 therapy (obesity, type 2 diabetes), this is a conversation worth having with your doctor. But GLP-1s should not replace established AUD treatments — at least not yet.
GLP-1 and Opioid Addiction
Verdict: Strong observational signal. Clinical trials underway. Do not replace current OUD medications.
Drug overdoses caused more than 79,000 deaths in the U.S. in 2024 alone, according to the CDC. [18] Effective medications exist — buprenorphine (Suboxone) and methadone — but they're massively underutilized, require frequent dosing, and carry their own challenges.
- BMJ 2026 study: GLP-1 users had a 25% lower risk of developing opioid use disorder, and those with existing OUD saw 39% fewer overdoses and 50% fewer substance-related deaths [1]
- Earlier cohort studies suggested up to a 78% reduced opioid overdose risk in patients with comorbid obesity and type 2 diabetes
- One small study found a GLP-1 medication reduced opioid cravings by 40% over 3 weeks
- Animal models: GLP-1 agonists consistently reduce self-administration of heroin, fentanyl, and oxycodone in rodents
What's happening now: Multiple NIH-funded randomized trials are underway, including at Brigham and Women's Hospital/Harvard (Dr. Joji Suzuki) and Penn State.
Critical context:
Buprenorphine and methadone save lives every day. They are the standard of care for OUD. GLP-1s may eventually become a complementary tool, but they are not a substitute today. If you or someone you love is dealing with opioid addiction, please seek established treatment first.
GLP-1 and Nicotine / Smoking
Verdict: Promising animal data and some human signal. Not ready to replace standard cessation tools.
- BMJ 2026 study: 20% reduced risk of nicotine use disorder among GLP-1 users
- Animal studies: GLP-1 agonists reduce nicotine self-administration and reinstatement of nicotine-seeking behavior in rodents
- The JAMA Psychiatry semaglutide trial for AUD also found reduced cigarettes per day in participants who smoked
- One earlier trial showed increased smoking abstinence with exenatide, but larger studies haven't consistently replicated this
- A potentially unique advantage: GLP-1s may prevent the weight gain that commonly follows smoking cessation
What this means today: If you're already taking a GLP-1 and you notice your smoking urges fading, that's consistent with what the science is suggesting. But don't rely on a GLP-1 as your primary quit strategy. Nicotine replacement therapy, varenicline (Chantix), and behavioral support have far more evidence. For more on GLP-1 medications, see our semaglutide vs tirzepatide comparison.
GLP-1 and Cocaine / Stimulant Addiction
Verdict: Early. Intriguing because no FDA-approved treatment exists for cocaine addiction.
- BMJ 2026 study: 20% reduced risk of cocaine-related substance use disorder [1]
- Animal studies: GLP-1 receptor activation reduces cocaine-seeking behavior in rodent models
- Human data are sparse and mixed. A small acute exenatide study in people with cocaine use disorder did not show reduced cocaine self-administration or subjective cocaine effects [17], and longer-term studies are still needed
Why researchers care: There is currently no FDA-approved medication for cocaine or stimulant addiction. None. If GLP-1s could fill even part of that gap, it would be significant. But we're a long way from knowing.
GLP-1 and Cannabis
Verdict: Some observational signal, but the thinnest evidence among the major substances.
- BMJ 2026 study: 14% reduced risk of cannabis use disorder — the smallest reduction of any substance studied
- One earlier study suggested a 44% reduced risk of cannabis use disorder in patients with type 2 diabetes taking semaglutide
- No clinical trials specifically testing GLP-1s for cannabis use disorder
Context: Like cocaine, there's no FDA-approved medication for cannabis use disorder. That's part of the interest. But “some signal in observational data” is a long way from “works for this.”
GLP-1 and Gambling, Shopping, and Other Behavioral Addictions
Verdict: Biologically plausible. Reports are accumulating. But the evidence is mostly anecdotal.
The logic: gambling, compulsive shopping, and other behavioral addictions involve the same dopamine reward circuitry as substance addiction. If GLP-1s dampen that circuitry broadly, they might reduce behavioral addictions too.
- A peer-reviewed analysis of Reddit data found that 21% of comments reported GLP-1-related interruption of compulsive shopping behaviors
- Clinicians at Brown University, Stanford, and elsewhere have reported patients whose gambling urges decreased on GLP-1s
- Dr. Lembke at Stanford has said researchers are actively examining whether GLP-1s can help with gambling, sex addiction, and shopping
- Boston University researchers have noted that GLP-1 medications may reduce the pleasure derived from compulsive behaviors broadly
What we don't have: Any formal clinical study. No randomized trial. No observational cohort analysis specifically for behavioral addictions. If you're on a GLP-1 and you notice compulsive behaviors decreasing, you're not imagining it. But don't start a GLP-1 specifically to treat a gambling or shopping problem.
What About Food Preoccupation and “Food Noise”?
This one is different because it overlaps directly with GLP-1s' approved uses for weight management. “Food addiction” isn't a formal diagnosis in the DSM-5. But a growing consensus of experts, including Dr. Lembke, agrees that people can become addicted to food — especially ultraprocessed food loaded with sugar, salt, fat, and engineered flavors — leading to compulsive overconsumption. [9]
GLP-1 medications demonstrably reduce food preoccupation. The “food noise” concept is one of the most universally reported experiences among GLP-1 users. This effect is well-documented in obesity trials and is, in a real sense, the foundation of everything we're discussing on this page. However, GLP-1s are FDA-approved for obesity and weight management — not for binge-eating disorder or food addiction as clinical diagnoses.
If GLP-1s can quiet food noise, it's reasonable to ask whether they can quiet other forms of craving noise. That question is exactly what researchers are now trying to answer.
Also exploring GLP-1 care for weight or metabolic health?
If you qualify based on BMI or a metabolic condition, a GLP-1 prescription for an approved indication is the safest path — and the craving-related benefits may follow. Any craving-related effects are not an FDA-approved addiction indication.
Check Your GLP-1 Eligibility →Which GLP-1 Drugs Are Being Discussed in Addiction Research?
This trips people up because there are multiple GLP-1 medications, and the brand name confusion is real. Here's a quick reference:
| Generic Name | Brand Names | How It's Taken | Approved For | Addiction Research Status |
|---|---|---|---|---|
| Semaglutide | Ozempic, Wegovy, Rybelsus | Weekly injection or daily pill | Type 2 diabetes, obesity | Most studied for addiction. Positive Phase 2 RCT for AUD. Largest observational datasets. |
| Tirzepatide | Mounjaro, Zepbound | Weekly injection | Type 2 diabetes, obesity | Included in some observational studies. Less direct addiction data than semaglutide. |
| Liraglutide | Victoza, Saxenda | Daily injection | Type 2 diabetes, obesity | Earlier preclinical work on alcohol. Some tolerance concerns in animal studies. |
| Exenatide | Byetta, Bydureon | Twice-daily or weekly injection | Type 2 diabetes | Used in early addiction trials. Mixed results in human studies. |
| Dulaglutide | Trulicity | Weekly injection | Type 2 diabetes | Some positive animal data for alcohol. No published human addiction trials. |
The short version: Semaglutide is the frontrunner in addiction research by a wide margin. If you see a study about GLP-1s and addiction, it's most likely about semaglutide. Tirzepatide (a dual GIP/GLP-1 agonist) is increasingly included in observational research but has less dedicated addiction data so far.
The addiction effects appear to be a class effect — meaning they seem linked to GLP-1 receptor activation broadly, not to one specific drug. Animal studies have shown craving reduction with exenatide, liraglutide, semaglutide, and dulaglutide. That's consistent with the mechanism being about the GLP-1 receptor pathway itself rather than a unique property of any single molecule.
Real Stories: What People Are Actually Reporting
We want to be careful here. Anecdotes aren't evidence. But they're part of the story — and often the reason you're on this page in the first place. These come from published peer-reviewed analyses, named interviews in major publications, and statements from researchers who treat patients:
The veteran who just stopped smoking.
Dr. Al-Aly described a patient who had tried to quit cigarettes for over a decade. After starting a GLP-1 for diabetes, he lost interest in smoking. No patch. No quit date. No effort. “It happened without effort,” Al-Aly recounted.
The writer who lost her taste for whiskey.
Bridget Pilloud, profiled in Medscape, described how semaglutide eliminated her desire for her favorite Old Fashioned cocktail. She also reported losing interest in compulsive shopping — a pattern that multiple clinicians have observed in their patients.
The 40% opioid craving reduction.
In a small clinical study, patients with opioid use disorder who took a GLP-1 medication saw their cravings drop by 40% over three weeks. That's a measured result, not a social media post — though the study was small.
The Reddit signal.
A peer-reviewed analysis published in Brain Sciences examined nearly 70,000 Reddit posts. Among alcohol-related discussions, 71% of GLP-1 users reported reduced cravings. About 30% described complete cessation of drinking. Among shopping-related posts, 21% reported an end to compulsive buying. [6]
Stanford's clinical experience.
Dr. Anna Lembke, author of Dopamine Nation and professor of psychiatry at Stanford, has said she currently prescribes GLP-1s to treat addiction — primarily for alcohol and food. But she's also clear: not everyone responds, and we still need longer-term data.
The essential caveat:
These stories come from people who noticed a change and spoke up. People who didn't notice anything are far less likely to share their experience. This is called selection bias, and it means the true percentage of people helped is almost certainly lower than what social media suggests. That's exactly why clinical trials — where everyone is tracked regardless of outcome — matter so much.
The 600,000-Patient Study That Changed the Conversation
This study deserves its own section because it's driving so much of the current interest — and because it's important to understand both what it found and what it didn't prove.
Study Details
- Published March 4, 2026 in The BMJ (DOI: 10.1136/bmj-2025-086886) [1]
- Led by Dr. Ziyad Al-Aly, Washington University School of Medicine / VA Saint Louis
- Analyzed electronic health records of 606,434 U.S. veterans with type 2 diabetes
- Followed patients for up to three years
- Compared GLP-1 users to SGLT2 inhibitor users (an important design choice that makes the comparison more rigorous)
- Ran seven parallel analyses covering alcohol, cannabis, cocaine, nicotine, opioids, and other substance use disorders
Key Findings: Patients WITHOUT Prior Substance Use Disorder
| Substance | Reduced Risk Among GLP-1 Users |
|---|---|
| Alcohol | 18% lower risk |
| Cannabis | 14% lower risk |
| Cocaine | 20% lower risk |
| Nicotine | 20% lower risk |
| Opioids | 25% lower risk |
Key Findings: Patients WITH Existing Substance Use Disorders
- 50% fewer substance-related deaths
- 39% fewer overdoses
- 26% fewer drug-related hospitalizations
- 25% fewer instances of suicidal ideation or attempts
Important Limitations
Observational, not randomized.
The study compared groups that already existed. This means we can't rule out that people who chose GLP-1s were different from the comparison group in ways that affected outcomes.
VA population.
Overwhelmingly male and older than the general population. Results may not fully generalize.
Motivation bias.
People starting GLP-1s may be more motivated to improve their health overall, which could independently reduce substance use.
What Dr. Al-Aly has said: “The revelation about GLP-1 medication is that it really works against all major substances, and it works uniformly, not because it acts against alcohol or opioids or nicotine specifically, but because it is likely acting against the craving itself.”
What other researchers have said: Dr. Lorenzo Leggio, clinical director at NIDA: “Even though we don't fully understand the mechanism, somehow the GLP-1 system is tackling addiction biology and the foundational system that underlies all these disorders.”
This study is the strongest signal yet — but signals aren't proof. That's why over 15 randomized clinical trials are now underway globally.
How Do GLP-1s Compare With Treatments That Already Exist for Addiction?
GLP-1s aren't entering a vacuum. FDA-approved treatments exist for some addictions, and the standard of care should not be abandoned based on preliminary evidence.
Alcohol Use Disorder: Current Treatment Landscape
| Treatment | FDA-Approved? | How It Works | Key Limitation |
|---|---|---|---|
| Naltrexone (Vivitrol) | Yes, for AUD | Blocks pleasurable effects of alcohol | Some patients don't respond; requires abstinence for opioid formulation |
| Acamprosate (Campral) | Yes, for AUD | Reduces post-acute withdrawal symptoms | Modest effect size; must be taken 3x daily |
| Disulfiram (Antabuse) | Yes, for AUD | Causes severe nausea if you drink | Aversion-based; poor adherence; can be dangerous |
| GLP-1s (semaglutide, etc.) | No (off-label) | May dampen craving via dopamine/reward pathway | Not approved; limited RCT data; cost/access barriers |
Opioid Use Disorder: Current Treatment Landscape
| Treatment | FDA-Approved? | How It Works | Key Limitation |
|---|---|---|---|
| Buprenorphine (Suboxone) | Yes, for OUD | Reduces cravings and withdrawal | Requires daily dosing; controlled substance |
| Methadone | Yes, for OUD | Stabilizes brain chemistry | Requires daily clinic visits; controlled substance |
| GLP-1s | No (off-label) | May reduce craving broadly | Not approved; no completed RCTs for OUD |
For Cocaine, Cannabis, and Behavioral Addictions
There are no FDA-approved medications for cocaine use disorder, cannabis use disorder, or behavioral addictions like gambling. Behavioral therapy is currently the primary treatment approach. This is partly why GLP-1 interest is so high for these conditions — the bar isn't competing with an established drug. It's competing with nothing pharmacological. Even modest evidence could represent a meaningful advance.
What Are the Risks, Side Effects, and Limitations?
Every medication has trade-offs, and GLP-1s are no exception. For a full guide on GLP-1 side effects, see our GLP-1 side effects guide.
Common Side Effects
- Nausea (especially when starting or increasing dose — the most common complaint, usually improves)
- Vomiting
- Diarrhea or constipation
- Headache
- Dizziness
- Injection site reactions
- Increased heart rate
Serious Warnings
GLP-1 prescribing labels carry a boxed warning about thyroid C-cell tumors based on animal studies. People with a personal or family history of medullary thyroid carcinoma or MEN2 should not take GLP-1 medications.
Other serious but rare risks: pancreatitis, gallbladder problems, kidney injury (usually related to dehydration from GI side effects), severe hypoglycemia (mainly when combined with insulin or sulfonylureas), and potential worsening of diabetic retinopathy (semaglutide).
What We Don't Know About GLP-1s for Addiction Specifically
Do cravings return when you stop?
The biggest unknown. Some people maintain reduced cravings after discontinuing. Others report everything coming back. This mirrors the weight regain pattern.
Is the anti-craving effect independent of weight loss?
If GLP-1s only reduce addiction cravings because people feel better after losing weight, that's a different story than if the drugs directly act on craving circuitry. Animal studies suggest a direct brain effect, but this hasn't been definitively established in humans.
Who responds and who doesn't?
Not everyone on a GLP-1 notices craving changes. We can't yet predict who will benefit.
How do GLP-1s interact with existing addiction medications?
No formal drug interaction studies between GLP-1s and naltrexone, buprenorphine, methadone, or other addiction treatments have been completed. Always tell your prescriber about all medications you're taking.
Could reducing pleasure broadly have downsides?
Some researchers note GLP-1s may cause a general “dulling” of pleasurable experiences. Could this affect motivation, relationships, or quality of life? It's an open question.
Insurance and Cost: The Practical Barrier
Even if a doctor agrees that a GLP-1 could help with addiction, getting it covered is another story. Insurance typically covers GLP-1s for type 2 diabetes and obesity — not for off-label addiction use. If you have a qualifying condition (BMI ≥ 30, or ≥ 27 with a comorbidity), you may be able to get coverage for the approved indication and experience the craving-related benefits as a secondary effect.
Without insurance, brand-name semaglutide (Ozempic/Wegovy) costs roughly $800–$1,000+ per month at retail. Telehealth providers offering GLP-1 programs typically charge $149–$399 per month with medication included. For a pricing breakdown, see our GLP-1 cost guide.
“Lost 16 lbs in 10 weeks — no side effects. Down two sizes. I wish I’d started sooner.”
— Verified MEDVi patient on ConsumerAffairs ★★★★★
What About Compounded GLP-1s and Online Clinics?
If you're searching for GLP-1 access — especially without traditional insurance coverage — you'll encounter online telehealth providers and compounded medications.
Compounded GLP-1 medications are custom-prepared by compounding pharmacies. They are not the same as brand-name drugs like Ozempic or Wegovy. The FDA has issued warnings about compounded semaglutide, including concerns about dosing errors and products containing salt forms of semaglutide not demonstrated to be safe and effective.
How to Protect Yourself
- Verify the provider uses a licensed, accredited compounding pharmacy (look for PCAB accreditation or state board licensing)
- Confirm the provider requires a medical evaluation before prescribing
- Be wary of providers that prescribe without a health history review
- Don't assume compounded = identical to brand-name
We maintain a comprehensive comparison of legitimate GLP-1 telehealth providers with verified pricing, pharmacy credentials, and clinical support details. If you're considering this route, start there. For more on compounded medications, see our compounded semaglutide safety guide.
Important:
We never recommend pursuing a GLP-1 prescription solely for addiction treatment. If you also have a qualifying health condition (obesity, metabolic issues, prediabetes, type 2 diabetes), a GLP-1 prescription for that condition is the medically appropriate path — and any craving-related benefits may follow.
What Clinical Trials Are Happening Right Now?
The research is accelerating. Here are the most important trials to watch:
| Condition | Drug | Institution / Lead | Phase | Status |
|---|---|---|---|---|
| Alcohol Use Disorder | Semaglutide (injectable) | USC / Dr. Christian Hendershot | Phase 2 (completed); Phase 3 (planned) | Phase 2 results published |
| Alcohol Use Disorder | Semaglutide | NIDA/NIH / Dr. Lorenzo Leggio | Phase 2 | Recruiting |
| Alcohol Use Disorder | Semaglutide | Oklahoma State / Dr. W. Kyle Simmons | Phase 2 | Recruiting |
| Opioid Use Disorder | GLP-1 agonist | Brigham & Women's / Dr. Joji Suzuki | Phase 2 | Recruiting |
| Opioid Use Disorder | Semaglutide | Penn State / Dr. Patricia Sue Grigson | Phase 2 | Active |
| Alcohol Use Disorder | Semaglutide (oral) | Multiple sites | Phase 3 | Enrolling |
Source: ClinicalTrials.gov and institutional press releases. Verified March 2026.
According to the Harvard Gazette (February 2026), there are more than 15 clinical trials testing GLP-1s for addiction globally. Results from most are expected within the next 2–3 years. We'll update this section as results are published. Bookmark this page.
What Does This Mean for You Today?
This is where we shift from “what the science shows” to “what should I actually do?” The answer depends on where you're coming from.
If You're Already on a GLP-1 and Noticed Your Cravings Changed
You're not imagining it, and you're not alone. The experience of reduced cravings for alcohol, nicotine, or other substances while taking a GLP-1 is consistent with a growing body of research.
- Mention it to your prescriber — they should know
- Don't stop any existing addiction treatment without discussing it with a healthcare provider
- Don't increase or change your GLP-1 dose on your own
- Pay attention to the pattern: which cravings changed, when, and how much?
If You Have Addiction Concerns but Not Obesity or Diabetes
This is the hardest situation right now. Without a qualifying condition, getting a GLP-1 prescribed — and especially getting it covered by insurance — is very difficult.
- Pursue established addiction treatment first. SAMHSA's helpline (1-800-662-4357) is free, confidential, and available 24/7
- Talk to an addiction medicine specialist about your interest in GLP-1s
- Watch the clinical trials — participation gives you access to the medication under medical supervision
If You Have Both Addiction Concerns and Weight or Metabolic Issues
This is where the path is clearest. If you qualify for a GLP-1 based on BMI (≥ 30, or ≥ 27 with a comorbidity like hypertension, sleep apnea, or prediabetes) or type 2 diabetes, you can pursue GLP-1 treatment for the approved indication. The craving-reduction benefits may come as a secondary effect.
This isn't a loophole — it's good medicine. Obesity and addiction frequently co-occur, and treating both simultaneously makes clinical sense.
- Talk to your doctor about GLP-1 treatment for weight management or metabolic health
- If your doctor isn't familiar with the addiction research, bring the BMJ study or this guide
- Consider a telehealth GLP-1 provider if access is a barrier
If You're in Recovery and Don't Want to Destabilize Anything
Recovery is hard-won. We respect that. If your current treatment plan is working — whether that's medication, therapy, support groups, or a combination — adding a new drug should be a careful conversation with your treatment team, not a solo experiment based on internet articles.
If You're Mainly Curious After Seeing Headlines
That's exactly who this page is for. Now you know: the evidence is real and growing, but it's not yet conclusive for most substances. The best thing you can do is stay informed. We'll continue updating this guide as new research publishes.
Ready to check your eligibility for GLP-1 treatment?
Our quick assessment takes 60 seconds and can help you find a GLP-1 program that fits your health profile. Any craving-related effects are not an FDA-approved addiction indication.
Take the Free 60-Second Eligibility Quiz →Questions to Ask Your Doctor About GLP-1 and Addiction
Whether you're bringing this up for the first time or continuing a conversation, these questions can help:
- “I've seen research about GLP-1 medications and addiction. Given my health profile, is this relevant to me?”
- “Do I qualify for a GLP-1 based on weight or metabolic health? Could that also help with my cravings?”
- “Would established addiction treatment be a better first step in my case?”
- “What risks or contraindications should I know about given my medical history?”
- “If I'm already on a GLP-1 and noticing craving changes, how should we interpret that?”
- “Are there clinical trials I might be eligible for?”
You can print this list and bring it to your appointment.
How We Graded the Evidence
Transparency matters, especially on a health topic. Here's how we arrived at the evidence ratings. See our full editorial standards and how we rank providers.
| Evidence Type | Description | Weight |
|---|---|---|
| Randomized Controlled Trial (RCT) | Participants randomly assigned to drug or placebo; gold standard | Highest |
| Large Observational Study | Medical record analysis comparing groups; association but not causation | High |
| Small Study / Case Series | Limited participants, often uncontrolled | Moderate |
| Animal / Preclinical | Laboratory studies in rodents or primates | Lower |
| Anecdotal / Self-Report | Social media, patient stories, case reports | Lowest |
A substance receives a higher evidence rating when multiple study types converge on the same finding, studies are replicated across different institutions and populations, sample sizes are large, and at least one RCT exists with positive results. A substance receives a lower rating when evidence is limited to animal studies or anecdotes, studies are small or unreplicated, or results are mixed.
We do not grade compounded medications separately from their brand-name counterparts. Our assessment covers the active pharmaceutical compounds (semaglutide, tirzepatide, etc.) regardless of formulation.
Sources and References
- Cai M, Choi T, Xie Y, Al-Aly Z. “Glucagon-like peptide-1 receptor agonists and risk of substance use disorders among US veterans with type 2 diabetes: cohort study.” The BMJ. 2026;392:e086886.
- Hendershot CS, et al. “Once-Weekly Semaglutide in Adults With Alcohol Use Disorder: A Randomized Clinical Trial.” JAMA Psychiatry. 2025.
- Wang W, et al. “Associations of semaglutide with incidence and recurrence of alcohol use disorder in real-world population.” Nature Communications. 2024.
- Klausen MK, et al. “The role of glucagon-like peptide 1 (GLP-1) in addictive disorders.” British Journal of Pharmacology. 2022.
- Srinivasan NM, et al. “GLP-1 therapeutics and their emerging role in alcohol and substance use disorders.” Journal of the Endocrine Society. 2025.
- Arillotta D, et al. “Exploring the Potential Impact of GLP-1 Receptor Agonists on Substance Use, Compulsive Behavior, and Libido.” Brain Sciences. 2024;14(6):617.
- Aoun H, et al. “Potential role of GLP-1 receptor agonists in substance use disorder: A systematic review of randomized trials.” Drug and Alcohol Dependence. 2024.
- Sa B, et al. “Psychiatric effects of GLP-1 receptor agonists: A systematic review of emerging evidence.” Diabetes, Obesity and Metabolism. 2026.
- Stanford Medicine / Anna Lembke, MD. “Five things to know about GLP-1s and addiction.” April 2025.
- Brown University / Carolina Haass-Koffler, PhD. “A turning point in addiction psychiatry?” July 2025.
- Harvard Gazette. “What's next for GLP-1s?” February 2026.
- FDA Prescribing Information: Ozempic, Wegovy, Mounjaro.
- SAMHSA National Helpline: 1-800-662-4357. samhsa.gov
- FDA Safety Alert: Dosing errors associated with compounded semaglutide. fda.gov
- ClinicalTrials.gov: NCT05520775, NCT07218354, and related registrations.
- Havens JR, et al. “Effects of exenatide on cocaine self-administration.” Neuropsychopharmacology. 2021.
- CDC: “Understanding the Overdose Epidemic.” cdc.gov/overdose-prevention
Frequently Asked Questions
Can GLP-1 drugs help with addiction?
Growing evidence suggests they can reduce cravings and substance use for multiple types of addiction. The strongest data is for alcohol use disorder. But GLP-1s are not FDA-approved for addiction, and not everyone responds. They should be considered a potential tool, not a cure.
Are GLP-1 medications approved for addiction treatment?
No. As of March 2026, no GLP-1 is FDA-approved for any addiction indication. Use for addiction is off-label. Over 15 clinical trials are underway that could eventually support approval.
Does semaglutide help alcohol cravings?
The data is encouraging. A randomized trial published in JAMA Psychiatry showed semaglutide reduced alcohol craving and consumption compared to placebo. Large observational studies show significant reductions in AUD risk and alcohol-related hospitalizations.
Can Ozempic help alcohol use disorder?
Ozempic (semaglutide) is the most-studied GLP-1 in the context of alcohol. It has shown craving reduction in both clinical trials and real-world data. However, it is not approved for this use, and established AUD treatments (naltrexone, acamprosate) should be considered first.
Can GLP-1s help opioid addiction?
Large observational studies show reduced overdose risk and fewer substance-related deaths among GLP-1 users. A small study showed a 40% reduction in opioid cravings. Multiple randomized trials are underway. Do not replace buprenorphine or methadone without medical guidance.
Can GLP-1s help people stop smoking?
There is some evidence of reduced cigarettes per day and a potential bonus of preventing post-cessation weight gain. But results from smoking-specific trials are inconsistent, and standard cessation aids (NRT, varenicline) have stronger evidence.
Is there evidence for GLP-1 and marijuana use?
Limited. The BMJ study showed a 14% reduced risk of cannabis use disorder, the smallest effect of any substance studied. No clinical trials exist for this indication.
Can GLP-1s help gambling addiction?
Biologically plausible (same reward circuitry), and anecdotal reports are accumulating. But there are no formal studies. The evidence is too early to act on.
Why do people say GLP-1s reduce food noise?
GLP-1 medications act on dopamine signaling in the brain's reward centers. This dampens the constant mental preoccupation with food that many people with obesity experience. Researchers now believe the same mechanism may quiet substance-related cravings, what some call drug noise.
Are GLP-1s addictive themselves?
No. GLP-1 medications are not addictive, not controlled substances, and do not produce withdrawal symptoms when stopped.
Will insurance cover GLP-1s for addiction?
Almost certainly not for addiction alone. Insurance typically covers GLP-1s for approved indications (type 2 diabetes, obesity). If you qualify for an approved indication, you can get coverage, and the addiction-related benefits may come as a secondary effect.
Are compounded GLP-1s safe?
Compounded medications carry additional risks. The FDA has warned about dosing errors with compounded semaglutide. If you go this route, verify the pharmacy is licensed and accredited, and ensure a medical evaluation is required before prescribing.
What should I do if I need addiction treatment right now?
Call SAMHSA's National Helpline at 1-800-662-4357. It is free, confidential, and available 24/7. Visit FindTreatment.gov to locate treatment near you. For crisis situations, call 988 (Suicide and Crisis Lifeline).
Which GLP-1 has the most addiction research?
Semaglutide (Ozempic/Wegovy) has the most human data, including the largest observational studies and the first positive randomized trial for alcohol use disorder. Exenatide, dulaglutide, and liraglutide also have some clinical data.
Can GLP-1s replace naltrexone, acamprosate, methadone, or buprenorphine?
Not based on current evidence. Established addiction medications have decades of research behind them. GLP-1s may eventually complement these treatments or help patients who don't respond to existing options, but they are not a replacement today.
What happens when you stop taking a GLP-1?
This is one of the biggest unanswered questions. Some people maintain reduced cravings after stopping. Others report cravings returning. Long-term data on craving rebound does not yet exist.
How quickly do GLP-1s reduce cravings?
It varies. Some people notice changes within the first week. Others see effects build over several weeks as the dose increases. Clinical trials have typically measured outcomes over 9-week treatment periods.
Bottom Line
GLP-1 medications are showing real promise for reducing cravings and substance use across alcohol, opioids, nicotine, cocaine, cannabis, and possibly behavioral addictions. The March 2026 BMJ study — 600,000+ patients, consistent benefits across every substance tested — is the strongest signal yet that this is genuine biology, not coincidence.
But promising isn't proven. These drugs are not FDA-approved for addiction. The strongest evidence is for alcohol use disorder. For everything else, we're somewhere between “encouraging” and “too early to say.” Established addiction treatments remain the standard of care, and GLP-1s are not ready to replace them.
What is clear: this is a rapidly evolving field, and the next 2–3 years of clinical trials will be definitive. We will update this guide as the evidence develops.
Need addiction help now?
Call SAMHSA: 1-800-662-4357 (free, confidential, 24/7) | Visit FindTreatment.gov | Crisis: 988
Want a conversation guide for your doctor?
Use the questions checklist above — print it and bring it to your next appointment.
Also exploring GLP-1 care for weight or metabolic health?
If you qualify based on BMI or a metabolic condition, a GLP-1 prescription for an approved indication is the safest path — and the craving-related benefits may follow.
Any craving-related effects are not an FDA-approved addiction indication.
This guide is for educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Always consult a qualified healthcare provider before starting or changing any medication. Weight Loss Provider Guide maintains affiliate relationships with GLP-1 telehealth providers, which are disclosed where relevant. These relationships do not influence our editorial coverage. See our full editorial standards and methodology and affiliate disclosure for details.
Last Updated: March 9, 2026 | Research Verified: March 9, 2026 | By: WPG Research Team