Mounjaro Prior Authorization: How to Get Approved (Checklist, Criteria & Denial Fixes)
Disclosure: Some links on this site are affiliate links. If you purchase through these links, we may earn a commission at no extra cost to you. Thank you for supporting our site.·For informational purposes only—not medical advice.
If your pharmacy just told you “prior authorization required” for Mounjaro — here's the short version. Prior authorization (PA) is your insurance company's approval process before they'll cover Mounjaro (tirzepatide). Nearly every plan requires it. Most plans need four things: a confirmed Type 2 diabetes diagnosis, proof you've tried metformin or another first-line medication, recent A1C lab results, and documentation that you're following a diet and exercise plan.
The process takes anywhere from a few minutes (automated systems) to 30 days. If you're denied, don't panic — a GAO review of state insurance data found that 39–59% of coverage denials were reversed when patients appealed. And in Medicare Advantage prior authorization specifically, KFF's 2024 analysis found that only 11.5% of denied requests were appealed — but 80.7% of those appeals were partially or fully overturned. The takeaway: people who appeal with proper documentation often win. The problem? Most people never appeal at all.
Below, we break down the exact requirements by insurer, give you a printable PA readiness checklist, walk through every common denial reason with specific fixes, and cover what to do if your insurance simply won't budge. We've pulled criteria directly from published policy documents from UnitedHealthcare, Aetna, Cigna, Blue Cross Blue Shield, and Medicare — so you're not guessing.
Do I Actually Need Prior Authorization for Mounjaro?
Almost certainly, yes. The vast majority of commercial insurance plans, Medicare Part D plans, and Medicaid programs require prior authorization before they'll cover Mounjaro. When you or your doctor sends a prescription to the pharmacy, the pharmacy runs it through your insurance. If PA is required, the claim gets flagged and you'll hear one of these:
- “Your insurance requires prior authorization.”
- “We need to contact your doctor.”
- “This medication isn't covered without approval.”
That doesn't mean you can't get Mounjaro. It means your insurance wants proof that it's medically necessary before they pay for a medication that lists at about $1,100+ per month.
How to confirm in 60 seconds:
- Log into your insurance company's member portal or app
- Look up “Mounjaro” or “tirzepatide” in the formulary/drug list
- Check for notes like “PA required,” “step therapy,” or “quantity limits”
- If you can't find it online, call the member services number on the back of your insurance card and ask: “Is Mounjaro on my plan's formulary, and does it require prior authorization?”
One important distinction: prior authorization is different from step therapy, though they often show up together. Prior authorization is the approval process itself. Step therapy is a specific requirement within that process — your insurer wants you to try a cheaper medication first (usually metformin) before they'll approve the more expensive one. Quantity limits cap how many pens you can get per fill. You might face one, two, or all three of these hurdles.
What Is Prior Authorization, Exactly?
Prior authorization is essentially a permission slip from your insurance company. Before they agree to pay for certain medications — especially expensive ones like Mounjaro — they want your doctor to prove it's medically necessary and that the prescription aligns with their coverage rules.
Harvard Health describes it as a requirement where your health plan must approve a service or medication before you receive it, in order for your plan to cover the cost. The National Association of Insurance Commissioners (NAIC) frames it similarly as an insurer's tool to determine whether a treatment meets their criteria for medical necessity.
What prior authorization is NOT:
- Not a guarantee your insurance will pay. Even after PA approval, you're still responsible for your copay or coinsurance.
- Not a medical decision. It's an administrative and financial decision made by your insurer, not your doctor.
- Not permanent. Approvals expire (typically every 6–12 months), and you'll need to go through the process again at renewal.
Why do insurers bother with this? Two reasons. First, cost control — Mounjaro's list price is over $1,000 per month, and insurers want to make sure patients have genuinely tried cheaper alternatives. Second, clinical appropriateness — they want to verify the medication is being prescribed for an FDA-approved use and that it's the right fit for the patient's situation.
You might hear prior authorization called different things depending on your insurer: “precertification,” “pre-approval,” “prior approval,” or simply “PA.” They all mean the same thing.
What Is Mounjaro Approved For (and Why It Matters for PA)?
This is where a lot of prior authorization headaches begin, so let's be crystal clear.
Mounjaro (tirzepatide) is FDA-approved as an adjunct to diet and exercise to improve blood sugar control in adults and pediatric patients aged 10 and older with Type 2 diabetes mellitus. That's it. That's the approved indication per the prescribing information from Eli Lilly.
Mounjaro is not FDA-approved for weight loss or obesity.
This matters enormously for prior authorization because most insurance plans will only cover a medication for its FDA-approved use. If your doctor prescribes Mounjaro and the PA submission lists obesity or weight management as the primary reason — the PA will very likely be denied.
Here's the part that confuses a lot of people: Zepbound is the same active ingredient (tirzepatide), made by the same company (Eli Lilly), but it IS FDA-approved for chronic weight management in adults with obesity (BMI ≥30) or overweight (BMI ≥27) with at least one weight-related condition. Same drug, different brand name, different FDA indication, completely different prior authorization pathway. Learn more in our Zepbound prior authorization guide.
The takeaway: the FDA indication on the prescription drives the PA criteria your insurance applies. Get this wrong and the rest doesn't matter.
What Does Your Insurance Actually Require?
Requirements vary by insurer, but the pattern is remarkably consistent. We pulled criteria from published policy documents for the major carriers and organized them into one table so you can see where your plan likely falls.
Your specific plan may differ from the general policy. Plans within the same insurer (say, a large employer plan vs. a marketplace plan) can have different formularies and rules. The criteria below are drawn from published policy documents but are subject to change — always verify by calling the number on your card.
| Requirement | UHC / OptumRx | Aetna / CVS Caremark | Blue Cross Blue Shield | Cigna / Evernorth | Medicare Part D |
|---|---|---|---|---|---|
| T2D Diagnosis Required? | Yes | Yes | Yes | Yes | Yes |
| A1C / Lab Threshold | Lab evidence of T2D (A1C, FPG per payer criteria) | A1C ≥ 6.5% documented | Varies by regional plan | Lab evidence of T2D (A1C, FPG per payer criteria) | Lab evidence of T2D documented |
| Step Therapy (Must Try First) | Metformin or 1 oral diabetes agent | Metformin (or documented intolerance / contraindication) | Typically 2 Step-1 meds (e.g., Ozempic, Trulicity) before Step-2 — varies by plan | 1 oral diabetes medication in lookback period | Metformin or documented failure |
| Diet & Exercise Documentation | Yes | Yes | Yes | Yes | Yes |
| Weight Loss / Obesity Covered? | No — not FDA-approved for this use | No — use Zepbound instead | No | No — explicitly excluded | No |
| Age Requirement | Varies (some ≥ 10) | Varies by plan | Varies by plan | Varies (some ≥ 10) | N/A |
| Approval Duration | Typically 12 months | Typically 12 months | Varies | Typically 12 months | Varies by plan |
| Renewal PA Required? | Yes | Yes | Yes | Yes | Yes |
| Electronic PA (CoverMyMeds)? | Yes | Yes | Yes | Yes | Yes |
Table citation notes: UnitedHealthcare: Based on UHC's published “Prior Authorization/Notification: Diabetes Medications — GLP-1 & Dual GIP/GLP-1 Receptor Agonists” policy document. Aetna: Based on Aetna's published “GIP-GLP-1 Agonist Mounjaro PA with Limit Policy” and Aetna Better Health Mounjaro coverage policy. BCBS: Criteria vary significantly by state and plan. Example based on Johns Hopkins Priority Partners MCO PA form and published BCBS regional policies. Cigna: Based on Cigna's published “Diabetes – Mounjaro Prior Authorization Policy” and “GLP-1 Agonists Prior Authorization Policy” (National Formulary). Medicare Part D: Based on CMS coverage determination guidelines and published Medicare PA requirements. Last verified: February 2026.
The Details That Matter by Insurer
UnitedHealthcare / OptumRx
UHC's published commercial policy requires lab evidence of Type 2 diabetes (A1C ≥ 6.5% or fasting plasma glucose ≥ 126 mg/dL), prior use of at least one oral diabetes medication, and documentation that the prescription is not for weight loss. Authorization is typically granted for 12 months. UHC explicitly states these medications are not FDA-approved for weight management.
Aetna / CVS Caremark
Aetna's published policy requires a T2D diagnosis, an A1C history of ≥ 6.5%, and either an inadequate response to metformin, intolerance, or a contraindication. For patients needing combination therapy, an A1C of 7.5% or greater may be required. Continuation of therapy requires documentation that the patient has been on a stable dose for at least 3 months with clinical improvement.
Blue Cross Blue Shield
BCBS is the trickiest because it varies significantly by state and plan. Some BCBS plans (like Massachusetts) categorize Mounjaro as a “Step 2” medication, meaning you must try and fail two Step 1 medications (commonly Ozempic or Trulicity) before Mounjaro is approved. Other BCBS plans are more straightforward. Your best move: call BCBS directly and ask for your specific plan's Mounjaro PA criteria.
Cigna / Evernorth
Cigna's national formulary policy approves Mounjaro for T2D in patients aged 10 and older. The policy has an auto-adjudication feature — if the system detects a recent lookback of an oral diabetes medication claim and the patient meets age criteria, approval may be nearly instant. Weight loss and metabolic syndrome without T2D are explicitly listed as not covered.
Medicare Part D
Medicare requires PA for Mounjaro with specific quantity limits — typically a maximum of 12 pens over an 84-day period. A confirmed T2D diagnosis is required. Medicare does not cover Mounjaro for weight loss under any circumstances. Manufacturer savings cards (like the Lilly Mounjaro Savings Card) cannot be used with Medicare. However, the Medicare Prescription Payment Plan (M3P), which went into effect in 2025, allows you to spread your prescription costs into fixed monthly payments.
If your insurer isn't listed here
Call the member services number on the back of your card. Here's exactly what to say:
“I'd like to know the specific prior authorization criteria for Mounjaro, also known as tirzepatide, under my plan. Is it on my formulary? What tier is it? What step therapy medications are required first? And can you send me a copy of the PA criteria or point me to where I can find it online?”
Write down the representative's name and the reference number for the call. You may need it later.
The PA Readiness Checklist: What to Have Before Your Doctor Submits
Most prior authorization denials aren't because Mounjaro isn't appropriate — they're because the submission was missing something. A missing lab result, a missing medication history, a missing code. Your doctor's office is busy. PA requests stack up. Yours will be stronger if you show up prepared.
Print this. Bring it to your appointment. Go through each item with your doctor's office before they hit “submit.”
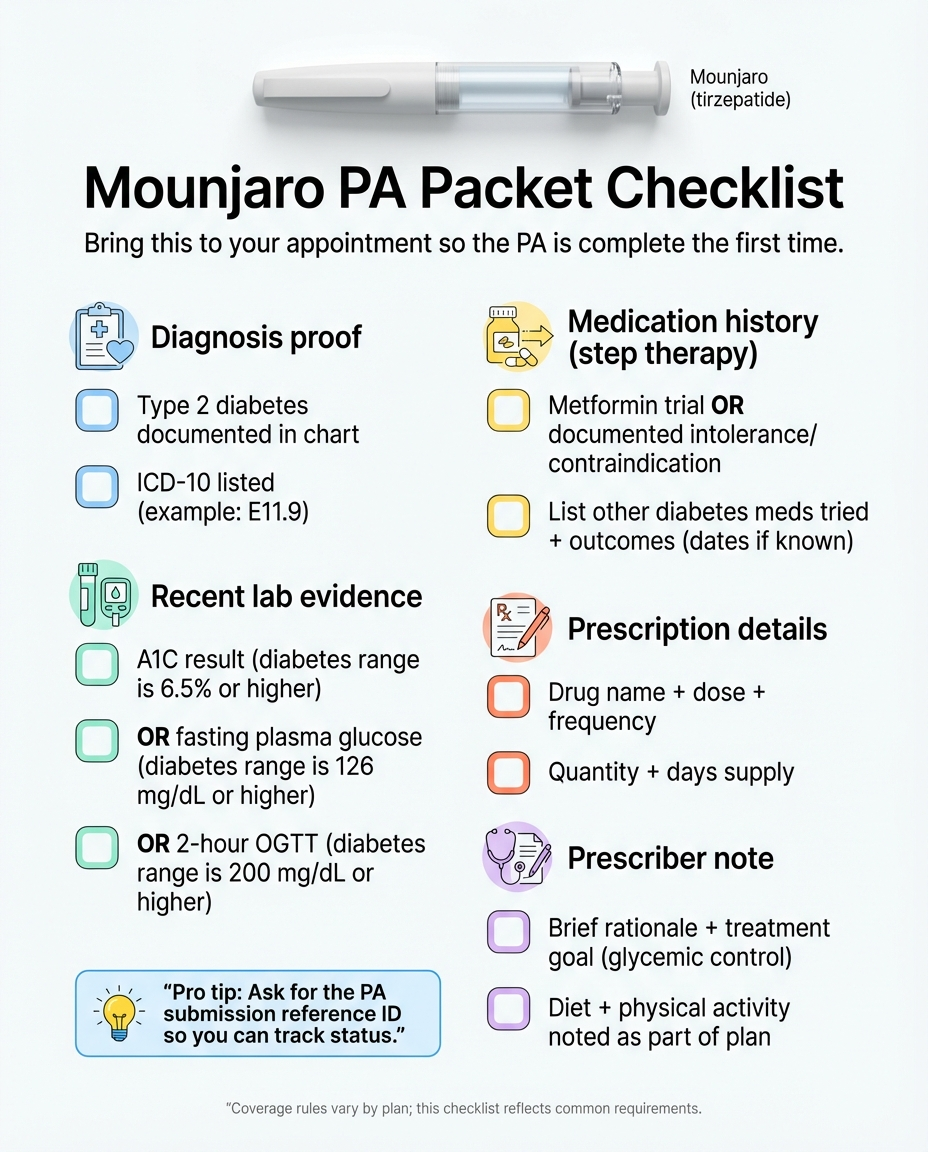
Confirmed Type 2 Diabetes Diagnosis
- • Your chart must have a documented T2D diagnosis, not just “prediabetes” or “metabolic syndrome”
- • ICD-10 code should be documented (most common: E11.9 — Type 2 diabetes without complications)
Recent A1C / HbA1c Lab Results
- • Must show A1C ≥ 6.5% (or fasting plasma glucose ≥ 126 mg/dL, or 2-hour OGTT ≥ 200 mg/dL)
- • Should be from within the last 3–6 months
- • If your A1C is borderline, include trends showing it's rising or not controlled
Complete Medication History (Step Therapy Documentation)
- • List every diabetes medication you've tried, with: drug name and dose, start and end dates (approximate is OK), and reason you stopped
- • Common step therapy drugs insurers look for: metformin, sulfonylureas (like glipizide), DPP-4 inhibitors (like Januvia), SGLT-2 inhibitors (like Jardiance), other GLP-1s (Ozempic, Trulicity, Victoza, Rybelsus)
- • Pro tip: If metformin caused GI side effects you couldn't tolerate, that counts. Document it explicitly.
Diet and Exercise Documentation
- • Mounjaro's FDA indication says “adjunct to diet and exercise” — many PA forms specifically ask about this
- • Your chart should note that you're following a calorie-appropriate diet and engaging in physical activity
- • Even a brief note from your doctor counts: “Patient following reduced-calorie diet and walking program”
Comorbid Conditions (If Applicable)
- • Conditions that strengthen your case: hypertension (I10), hyperlipidemia (E78.5), obstructive sleep apnea (G47.33), non-alcoholic fatty liver disease (K76.0), cardiovascular disease, PCOS (E28.2)
- • These show that diabetes isn't your only concern and that better glycemic control could improve multiple conditions
BMI Documented
Your current BMI should be in your chart, especially if weight-related comorbidities are part of the justification.
Prescribing Details (Correct)
- • Mounjaro (tirzepatide) — spelled correctly
- • Starting dose: typically 2.5 mg subcutaneous injection weekly
- • Quantity: 4 pens per 28 days (or as your insurer's quantity limit dictates — Medicare caps at 12 pens per 84 days)
- • NDC (National Drug Code) matches the correct dose and pen type
Clinical Justification Note from Prescriber
A brief note explaining WHY Mounjaro specifically: “Patient has tried metformin with inadequate response. A1C remains 8.2%. Initiating Mounjaro for improved glycemic control as adjunct to diet and exercise.”
One more thing: Keep a copy of everything. If your doctor's office submits electronically through CoverMyMeds, ask for the submission confirmation number. If they fax, ask for the fax confirmation page. You'll need these if you have to follow up.
How Does the Mounjaro Prior Authorization Process Work? (Step by Step)
Here's the actual sequence. It's more straightforward than most people think — the frustration usually comes from waiting and not knowing what's happening behind the scenes.
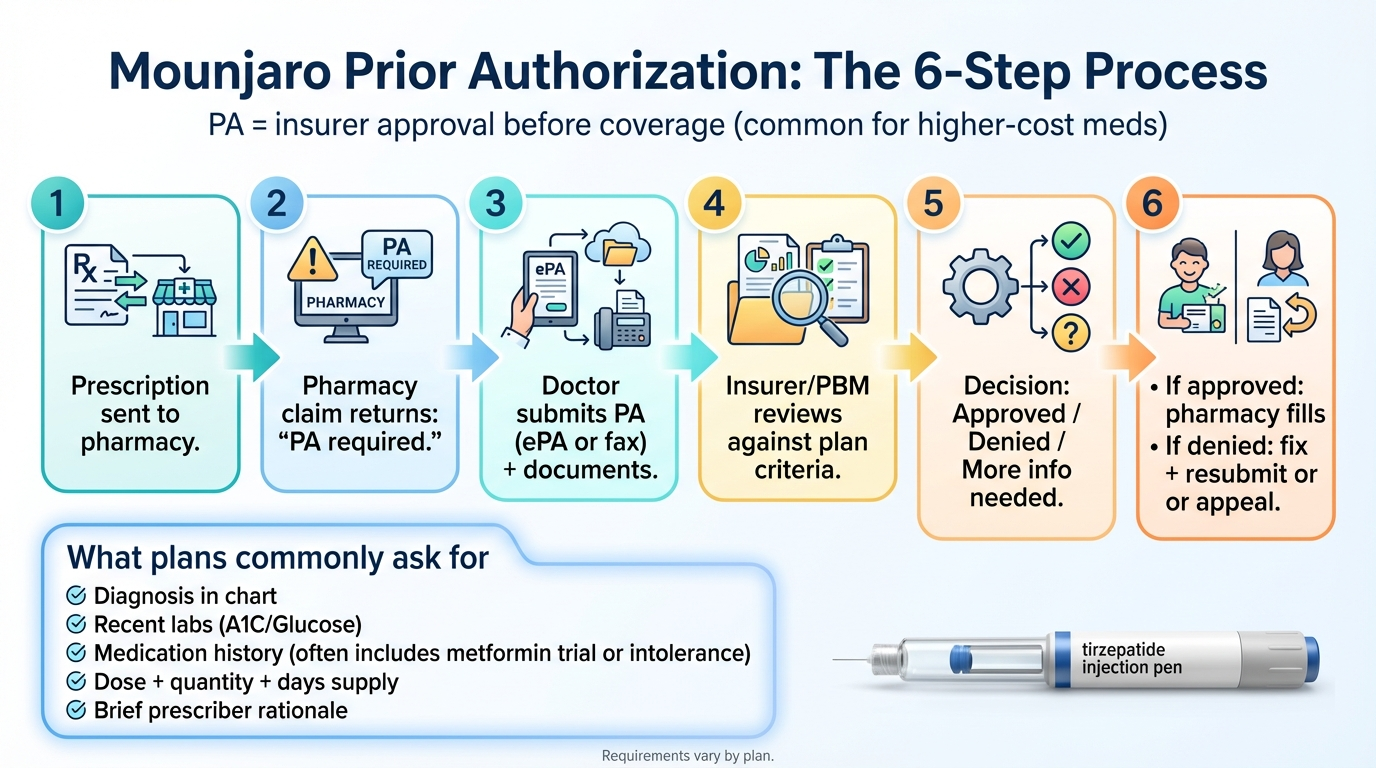
Prescription Is Written
Your doctor writes a prescription for Mounjaro and sends it to your pharmacy (electronically, by fax, or by phone).
Pharmacy Runs the Insurance Claim
The pharmacy submits the claim to your insurance (or more precisely, to your Pharmacy Benefit Manager — the company that actually manages drug coverage for your insurer, like OptumRx, CVS Caremark, or Express Scripts). The system flags that PA is required and rejects the claim.
You and Your Doctor Are Notified
You hear "prior authorization required" from the pharmacy. Your doctor's office receives a notification (electronically or by fax) that PA needs to be submitted.
Your Doctor's Office Submits the PA
Your doctor's office gathers the clinical documentation (labs, diagnosis, medication history — everything on the checklist above) and submits the PA request. Most offices now use electronic PA (ePA) platforms like CoverMyMeds, which Eli Lilly specifically supports for Mounjaro.
Insurance Reviews the Request
Your insurer (or PBM) reviews the submitted documentation against their specific criteria for Mounjaro. Three things can happen: Approved, Denied, or More information needed.
Pharmacy Fills the Prescription (If Approved)
Once approved, your pharmacy reruns the claim and fills it. Your PA approval is typically valid for 6–12 months, depending on your plan.
Reauthorization
Before your approval expires, your doctor's office will need to submit a new PA. This one is usually easier — it's focused on showing clinical improvement (better A1C, for example) and continued medical necessity. Set a reminder 30 days before expiration.
Your job at Step 4: Don't assume it's happening. Call your doctor's office 2–3 business days after the pharmacy flags it and ask: “Has the Mounjaro PA been submitted yet? Do you need anything from me?” PA requests can sit in a queue, especially at busy practices.
How Long Does Mounjaro Prior Authorization Take?
The honest answer: anywhere from a few minutes to 30 days. Here's how the range breaks down.
Minutes–24 hrs
Fastest (Auto-Adjudication)
Cigna and some UHC plans with auto-adjudication systems
5–14 days
Typical
Most standard PA reviews with complete documentation
72 hrs / 24 hrs
Medicare Part D (CMS Deadlines)
Standard: 72 hours. Expedited (urgent): 24 hours
What slows things down
- • Missing documentation (most common)
- • Fax-based submissions (slower than electronic)
- • Submitting late on a Friday
- • Insurer sends “more info needed” request → clock resets
What speeds things up
- • Electronic submission through CoverMyMeds
- • Complete documentation on the first submission
- • Proactive follow-up after 5–7 business days
- • Request expedited review if medically urgent
Checking status: Most insurers let you check PA status through their online member portal. You can also call member services with your reference number. If CoverMyMeds was used, patients can receive text or email notifications about their PA outcome (with consent).
Where Do I Find the Mounjaro Prior Authorization Form?
You don't typically need to track down the PA form yourself — your doctor's office handles that. But knowing what it looks like and what it asks for puts you in a better position to make sure nothing's missing.
CoverMyMeds (electronic): Most offices now use CoverMyMeds to submit Mounjaro PAs electronically. The form auto-populates based on your insurer and medication. This is the fastest method and the one Eli Lilly specifically supports.
Insurer/PBM portal: Your insurer or pharmacy benefit manager has PA forms available through their provider portal. Your doctor's office downloads and submits these.
Insurer website (PDF forms): Some plans publish printable PA forms. For example, Johns Hopkins Priority Partners publishes a Mounjaro-specific PA form.
By phone/fax: Some offices still call or fax PA requests. This is slower and harder to track, but still used.
What the form typically asks for:
- • Patient demographics (name, insurance ID, date of birth)
- • Prescriber information (NPI, contact)
- • Diagnosis code (ICD-10 — usually E11.9 for T2D)
- • Medication details (Mounjaro, tirzepatide, dose, quantity, days supply)
- • Clinical history: Has the patient tried metformin? Other diabetes medications? Results?
- • Lab evidence: Recent A1C or fasting glucose
- • Lifestyle: Is the patient following a diet and exercise program?
- • Clinical justification: Why is Mounjaro necessary for this patient?
Your move: You don't fill this form out. But you can bring the checklist from above to your appointment and make sure your doctor has everything the form asks for before they submit.
How Do I Check Mounjaro Prior Authorization Status?
Waiting is the hardest part. Here's how to find out where things stand.
Your insurance member portal or app. Log in and look for “prior authorization,” “pharmacy claims,” or “coverage decisions.”
Call member services. Use the number on the back of your insurance card. Ask for the status with your reference or case number.
Ask your doctor's office. If they submitted through CoverMyMeds, they can check status in the system.
| Status | What It Means | What to Do |
|---|---|---|
| Submitted / Received | The request is in the insurer's system but hasn't been reviewed yet | Wait 3–5 business days, then check again |
| In Review / Pending | An insurer reviewer is evaluating the request | Normal — check again in 5–7 days |
| Additional Info Needed | The insurer came back asking for more documentation | Contact your doctor's office immediately — the clock resets |
| Approved | You're good — go to the pharmacy and fill the prescription | Confirm approval duration and note the expiration date |
| Denied | The request was rejected | Get the denial reason in writing and start the appeal process |
Pro tip: If your PA has been “pending” for more than 10 business days with no update, call both your insurer and your doctor's office on the same day. Sometimes the insurer sent a request for more information to the doctor, and the doctor's office hasn't seen it yet. One phone call can unstick the whole thing.
What If Your Mounjaro Prior Authorization Is Denied?
Getting a denial letter feels like hitting a wall. But here's what most people don't realize: a denial is usually a fixable problem, not a permanent answer.
The data tells the story. A GAO review of state insurance data found that when coverage denials were appealed, 39–59% were reversed. In Medicare Advantage prior authorization specifically, KFF's 2024 analysis found that 80.7% of appealed denials were partially or fully overturned — yet only 11.5% of patients actually appealed. The AMA's 2024 physician survey found that 29% of physicians reported PA-related delays led to serious adverse events for patients.
The catch? Most people never fight back. Don't be one of them.
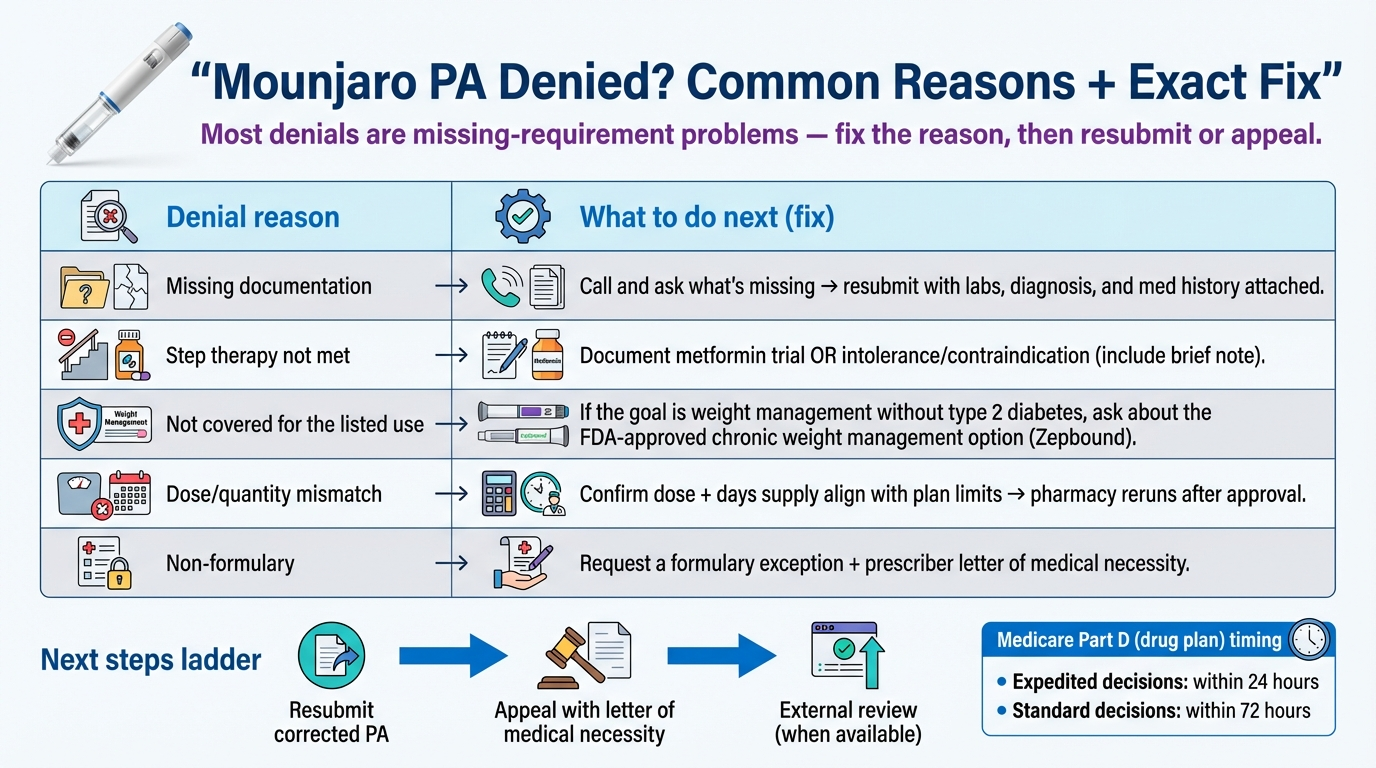
Most Common Denial Reasons (And Exactly How to Fix Each One)
| Denial Reason | What It Actually Means | How to Fix It |
|---|---|---|
| “Not medically necessary” | The insurer says the clinical notes don't justify Mounjaro | Have your doctor submit a Letter of Medical Necessity with detailed A1C history, failed medications, and specific clinical rationale. Eli Lilly provides a template. |
| “Not on formulary” | Mounjaro isn't on your plan's covered drug list | Request a formulary exception through a formal appeal. Cite why alternatives (Ozempic, Trulicity, etc.) are not appropriate for you. |
| “Step therapy not met” | You haven't tried the required cheaper medications first | Document all prior medications with dates, doses, and reasons for discontinuation. Even a brief intolerance to metformin counts if documented. |
| “Off-label use / weight loss” | The primary diagnosis listed was obesity, not Type 2 diabetes | Discuss with your doctor: Is Zepbound (FDA-approved for weight loss) more appropriate? Or does your history support a T2D code? |
| “Incomplete documentation” | The PA form was missing required information | Have your doctor resubmit with ALL required documents. Use the checklist above. Call and ask the insurer exactly what was missing. |
| “Incorrect codes” | Wrong ICD-10 or billing codes were used | Verify codes. For T2D: E11.9, E11.8, or E11.65. Avoid using E66.x (obesity) as the primary code for Mounjaro. |
| “Quantity / dose limits” | Requested amount exceeds plan limits | Verify your insurer's specific quantity limits. Medicare caps at 12 pens per 84 days. Adjust the prescription to match. |
| “Concurrent GLP-1 therapy” | Records show you're on another GLP-1 at the same time | If switching from Ozempic to Mounjaro, the prescriber may need to document discontinuation of the prior GLP-1. |
How to Appeal a Mounjaro PA Denial
Appeals are structured. The winning strategy is matching the insurer's own criteria with documentation and using the correct process for your plan type.
Get the Denial Reason in Writing
Call your insurance company and request the specific, written reason for denial. Then ask two follow-up questions:
- • “What specific clinical criteria were you using to evaluate this PA?”
- • “What exactly was missing or didn't meet the criteria?”
Know Your Deadline
Most commercial plans: 30–180 days from the denial date. Medicare Part D: you generally have 65 days from the date on the denial notice to request the first appeal (redetermination). This was recently extended from 60 days, effective January 1, 2025. Always confirm the exact deadline in your denial letter.
Have Your Doctor Write a Letter of Medical Necessity
This is the most important piece of your appeal. Eli Lilly provides a coverage authorization and appeals guide (available through the Mounjaro Answers Center at 1-800-545-5979). A strong letter includes your specific diagnosis with ICD-10 code, current A1C, every medication tried previously, why Mounjaro is specifically necessary, and any comorbid conditions.
Gather Supporting Documentation
Attach: Letter of Medical Necessity, recent lab results (A1C, metabolic panel), chart notes from relevant office visits, documentation of prior medication trials and outcomes, and any relevant clinical guidelines (ADA, AACE) that support the treatment choice.
Submit the Appeal
Follow your insurer's specific appeal submission process (it's usually on the denial letter). Submit everything together — the appeal form, the letter, and all supporting docs.
Follow Up
Call after 7–10 business days to confirm receipt and check status. Don't let it sit in a queue unmonitored.
If the Internal Appeal Is Denied — External Review
If your internal appeal fails, you have the right to request an external review. An independent third party reviews the case and makes a binding decision. This process is available through your state insurance department for commercial plans, and through CMS/Medicare for Part D plans.
Medicare patients have a specific appeals ladder: first a redetermination by the plan, then reconsideration by an Independent Review Entity (IRE). CMS publishes specific timelines: 7 days standard / 72 hours expedited for IRE reconsideration.
The bottom line on appeals: The system is designed to discourage you from fighting. Don't let it work. A properly documented appeal has a strong chance of success, and you have the legal right to pursue it through multiple levels.
Mounjaro vs. Zepbound: Which One Should Your Doctor Prescribe?
This is the elephant in the room, and getting it right can make or break your PA.
Mounjaro and Zepbound are the same active ingredient — tirzepatide — made by the same company, Eli Lilly. The difference is the FDA indication:
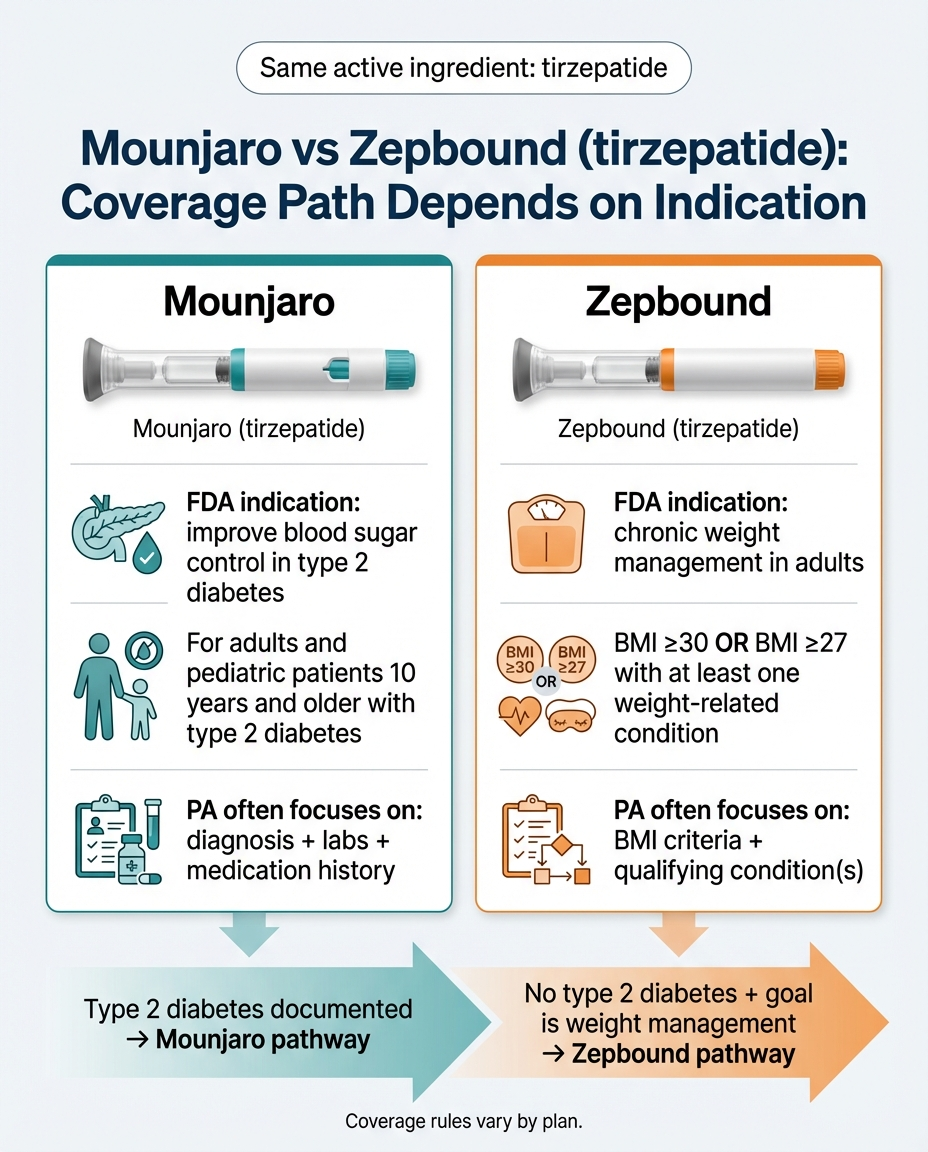
Mounjaro
FDA-approved for Type 2 diabetes (blood sugar control). PA evaluated against T2D criteria: diagnosis, labs, medication history.
Zepbound
FDA-approved for chronic weight management (obesity/overweight with comorbidities). PA evaluated against BMI criteria and qualifying conditions.
If you have Type 2 diabetes (whether or not you also want to lose weight), Mounjaro is the correct prescription. Weight loss is a welcome secondary benefit, but T2D is the documented reason.
If you want weight management and you do NOT have Type 2 diabetes, Zepbound is the correct prescription. Trying to get Mounjaro approved for weight loss without a T2D diagnosis is almost guaranteed to fail.
If you're not sure, talk to your doctor about your full medical picture. Some patients have pre-diabetes, insulin resistance, or early-stage T2D that hasn't been formally documented — which could change the calculus entirely.
The practical impact: One conversation with your doctor about “should we prescribe Mounjaro or Zepbound based on my diagnosis?” can save you weeks of PA delays, denials, and appeals. Read our full semaglutide vs. tirzepatide comparison for more context on how these drugs differ.
What ICD-10 Codes Are Used for Mounjaro Prior Authorization?
Your doctor handles coding, but understanding why it matters can help you advocate for yourself. The ICD-10 code on your PA submission tells the insurer what condition Mounjaro is treating. The wrong code can trigger an automatic denial.
Type 2 Diabetes Codes (Use These for Mounjaro PA)
| E11.9 | Type 2 diabetes mellitus without complications (most commonly used) |
| E11.65 | Type 2 diabetes mellitus with hyperglycemia |
| E11.8 | Type 2 diabetes mellitus with unspecified complications |
| E11.22 | Type 2 diabetes mellitus with diabetic chronic kidney disease |
| E11.40 | Type 2 diabetes mellitus with diabetic neuropathy, unspecified |
Obesity Codes — Proceed With Extreme Caution
E66.01 (Morbid obesity due to excess calories) and E66.09 (Other obesity due to excess calories)
Using an obesity code (E66.x) as the PRIMARY diagnosis for a Mounjaro PA will almost certainly result in denial. Mounjaro is not FDA-approved for obesity. If the primary code is obesity-related, the insurer's system reads it as an off-label use and often auto-denies.
Comorbid Condition Codes (Strengthen Your Case)
Including these as secondary diagnoses can bolster the medical necessity argument:
| I10 | Essential hypertension |
| E78.5 | Hyperlipidemia, unspecified |
| G47.33 | Obstructive sleep apnea |
| K76.0 | Non-alcoholic fatty liver disease |
| E28.2 | Polycystic ovary syndrome |
| I25.10 | Atherosclerotic heart disease |
Can You Get Mounjaro Prior Authorization for Weight Loss?
We're going to be straightforward: it's very unlikely, and here's why.
Mounjaro's FDA indication is for Type 2 diabetes. Period. Most insurance plans restrict coverage to FDA-approved uses. Cigna's published Mounjaro PA policy explicitly states that metabolic syndrome without T2D is not covered. UHC's GLP-1 policy explicitly says these medications are not FDA-approved for weight management. This isn't a loophole problem — it's a structural one.
Your Options If You Want Tirzepatide for Weight Loss
Option 1: Zepbound (the correct path)
If you don't have T2D and your primary goal is weight management, ask your doctor about prescribing Zepbound instead. It's the same active ingredient with a weight-management indication.
Option 2: Document the full picture
If you have T2D and want to lose weight, Mounjaro is appropriate — and the weight loss benefit supports the clinical case. Make sure your T2D diagnosis is primary.
Option 3: Explore telehealth providers
If your insurance won't cover Mounjaro or Zepbound through any pathway, several telehealth platforms prescribe tirzepatide without requiring traditional insurance PA. You pay out of pocket, but there's no PA process.
Option 4: Other FDA-approved weight loss medications
Wegovy (semaglutide) is FDA-approved for weight management and may have different coverage on your plan. Ask your doctor what your plan covers. See our semaglutide vs tirzepatide comparison.
The bottom line: trying to force a Mounjaro PA through with a weight-loss-only justification is almost always a waste of time. Redirect that energy toward the option that actually matches your situation.
Can't Get Insurance Coverage? Explore Telehealth Options
If insurance won't cover Mounjaro or you'd rather skip the PA process entirely, telehealth providers offer tirzepatide (the same active ingredient) without insurance. No prior authorization needed — just a medical consultation and monthly subscription.
Telehealth providers listed include affiliate partners. See our ranking methodology.
How Much Does Mounjaro Cost Without Insurance Approval?
$1,100+
Per month at list price (no insurance)
$25–$500+
Per month with insurance + PA approved
As low as $25
With Lilly Mounjaro Savings Card (commercially insured only)
M3P Available
Medicare patients: fixed monthly payments via M3P program (2025+)
What to Do If Your Insurance Won't Cover Mounjaro
We recommend exhausting the PA and appeal process first — it's almost always the cheapest path long-term. But if you've been denied, appealed, and your insurance still won't budge, you have options.
Manufacturer Assistance Programs: Eli Lilly offers patient assistance programs for eligible uninsured or underinsured patients. Contact the Mounjaro Answers Center at 1-800-545-5979.
Telehealth GLP-1 Providers: Several telehealth platforms prescribe tirzepatide without going through traditional insurance. Costs typically range from $200–$600/month depending on the provider and whether you're getting brand-name or compounded medication. See our best tirzepatide online comparison.
Pharmacy Discount Cards: Services like GoodRx and SingleCare offer discount pricing on Mounjaro at participating pharmacies. These won't bring the price anywhere near insurance-covered levels, but they can help.
Compounded Tirzepatide: Some compounding pharmacies offer tirzepatide at lower prices. The legal landscape around compounded GLP-1s is evolving. Discuss with your doctor whether a compounded version is appropriate. Learn more about compounded GLP-1 safety.
The honest take: Getting brand-name Mounjaro covered through insurance is almost always the most affordable option. The PA process is frustrating, but the potential savings of $800+ per month make it worth the effort. Fight for coverage first. Explore alternatives if that path genuinely closes.
How to Talk to Your Doctor and Insurance About Mounjaro PA
Most patients feel powerless in this process. You're not. You just need to know what to say.
Come prepared with your medication history written down (dates, doses, why you stopped each one). Then:
- • “I want to make sure the PA submission is as strong as possible. Can we go through what you'll be including?”
- • “I brought my medication history with dates — everything I've tried for diabetes/blood sugar management.”
- • “If we get denied, would you be willing to write a Letter of Medical Necessity for the appeal?”
- • “Should we consider Mounjaro or Zepbound based on my specific diagnosis?”
Have your member ID, the denial letter (if applicable), and a pen ready.
- • “What are the specific prior authorization criteria for Mounjaro tirzepatide on my plan?”
- • “Is Mounjaro on my plan's formulary, and what tier?”
- • “What step therapy medications does my plan require before Mounjaro?”
- • After denial: “Can you tell me the exact reason for the denial, and what specific documentation was missing or insufficient?”
Don't assume it's handled. Call 3–5 business days after the PA should have been submitted:
- • “I'm checking on the status of my Mounjaro PA. Has it been submitted?”
- • “Did insurance come back requesting any additional information?”
- • “Can I get the submission confirmation number or reference ID?”
The simple act of following up can shave days off the process.
Does Prior Authorization Expire? (Renewals & Dose Changes)
Yes. PA approvals have expiration dates, and this catches a lot of people off guard.
Typical approval duration: 6–12 months, depending on your insurer. After that, your doctor's office needs to submit a renewal PA — essentially proving that Mounjaro is still medically necessary and that you're showing clinical improvement.
What the renewal PA typically requires:
- • Updated A1C or lab results showing improvement
- • Confirmation that you're still on Mounjaro (continued therapy)
- • Documentation of clinical response (weight trends, glucose control, side effect profile)
- • Continued medical necessity justification
Dose changes: Some insurers require a new PA if your Mounjaro dose is increased. Others don't. Before your doctor increases your dose, call your insurance to ask: “Does a dose change require a new prior authorization?” This avoids the unpleasant surprise of going to the pharmacy for your new dose and hearing “PA required” again.
Set a reminder. Mark your calendar 30 days before your PA expires. Contact your doctor's office to start the renewal process early. A gap in PA = a gap in medication, and no one wants to go without Mounjaro while paperwork catches up.
For Prescribers and Office Staff: Submit a Clean PA the First Time
We know the PA burden is real. The AMA's 2024 prior authorization physician survey found that physicians and their staff spend an average of 13 hours per week completing prior authorizations, and 29% of physicians reported that prior authorization has led to a serious adverse event for a patient in their care.
What Payers Commonly Ask For
- ICD-10 diagnosis code (E11.9 is most common for T2D)
- Treatment history (prior diabetes medications, dates, and outcomes)
- Lab evidence (A1C, fasting glucose)
- Lifestyle documentation (diet and exercise as adjunct therapy)
- Prescribing details (dose, quantity, days supply)
Common Office Mistakes That Cause Denials
Submitting without recent labs. An A1C from 14 months ago won't cut it. Most plans want results within 3–6 months.
Using the wrong primary diagnosis code. If E66.01 (obesity) is listed as primary instead of E11.9 (T2D), the system may auto-deny.
Not documenting step therapy failures in sufficient detail. “Tried metformin — didn't work” isn't enough. They want dose, dates, and specifically what went wrong.
Submitting via fax when ePA is available. CoverMyMeds is faster, trackable, and less likely to get lost.
Not tracking reauthorization dates. Set up a system to flag patients whose PAs expire in 30 days.
Medicare, Medicaid, and Other Special Cases
Quantity limits are strict. Medicare typically caps Mounjaro at 12 pens per 84-day supply.
CMS sets the timeline. 72 hours for standard requests and 24 hours for expedited (urgent) requests. If the plan fails to issue a decision within the required timeframe, that delay is treated as an adverse decision — meaning the case can be forwarded for independent review by the IRE.
Appeals follow a specific ladder. First a redetermination by the plan, then reconsideration by an IRE (7 calendar days standard / 72 hours expedited), then further levels if needed.
No manufacturer savings cards. Federal law prohibits using manufacturer coupons with Medicare. The Medicare Prescription Payment Plan (M3P) allows fixed monthly payments.
Medicaid coverage for Mounjaro varies significantly by state. According to MACPAC, prior authorization is widely used in Medicaid prescription drug programs, but the specific criteria differ state by state. Call your state's Medicaid pharmacy helpline (listed on your Medicaid card) for your plan's specific PA criteria.
Express Scripts manages TRICARE pharmacy benefits and publishes specific PA request forms. TRICARE beneficiaries or providers can call 1-866-684-4488 or fax the completed PA form to 1-866-684-4477.
Large employers often self-insure and hire a PBM to administer drug benefits. These plans can have completely custom formularies and PA criteria. The plan name on your card might say “Blue Cross” or “Cigna,” but the actual coverage decisions are made by your employer's benefits team. This is why two people with “Cigna” insurance can have entirely different Mounjaro coverage. Always verify with your specific plan.
Explore Tirzepatide Without Insurance PA
If you've exhausted insurance options, telehealth providers prescribe tirzepatide (the same active ingredient in Mounjaro and Zepbound) starting from around $279/month. No PA, no step therapy, no waiting.
Affiliate disclosure: We may earn a commission through partner links. This never affects our recommendations. Full disclosure.
How We Researched This Guide
We built this guide using primary sources, not summaries of summaries. Here's where the information comes from:
- • Insurer criteria: Published PA policy documents from UnitedHealthcare (GLP-1 & dual GIP/GLP-1 agonists policy), Aetna (Mounjaro PA policy), Cigna (National Formulary Mounjaro PA policy), Blue Cross Blue Shield (regional PA forms), and Johns Hopkins Priority Partners (Mounjaro PA form)
- • FDA information: Mounjaro (tirzepatide) and Zepbound (tirzepatide) prescribing information from Eli Lilly
- • Manufacturer resources: Eli Lilly's Prior Authorization Tips Guide and Coverage Authorization Requests and Appeals Guide, including the Letter of Medical Necessity template
- • Government sources: CMS coverage determination and appeals timelines for Medicare Part D, MACPAC prior authorization in Medicaid report, ICD-10 coding reference from CMS
- • Industry data: AMA 2024 Prior Authorization Survey, U.S. Government Accountability Office report on insurance appeals success rates, NAIC prior authorization explainer
- • General PA education: Harvard Health prior authorization guide
What this guide is not: This is not medical advice. We're not doctors, pharmacists, or insurance counselors. Insurance requirements change frequently. Always verify your specific plan's requirements by calling the number on your insurance card.
How we keep this current: We re-check published payer policy documents regularly and update this page when criteria change. The “Last Verified” date on the comparison table reflects when we last confirmed the information against source documents.
What to Do Right Now
You've got the information. Here's your next action based on where you are:
If you haven't started the PA process yet:
Print the readiness checklist, gather your documentation, and bring it to your next doctor's appointment. Be proactive — don't wait for your doctor's office to figure it out.
If your PA is pending:
Call your insurance to check status. If it's been more than 7 business days with no response, call your doctor's office too. Make sure nothing's stuck.
If you've been denied:
Get the denial reason in writing. Talk to your doctor about an appeal. Use the denial-fix table above to identify exactly what needs to change. You have a strong chance of success if you actually appeal.
If insurance won't cover it no matter what:
You still have options. Explore manufacturer assistance programs, telehealth GLP-1 providers that prescribe tirzepatide without insurance, or alternative medications with different coverage on your plan. The list price isn't the only path forward.
Prior authorization is frustrating. It's bureaucratic. It sometimes feels designed to make you give up. But the data says that persistence wins more often than not. Arm yourself with the right information, the right documentation, and the right questions — and you've got a real shot at getting approved.
Frequently Asked Questions
Medical Disclaimer: This guide is for informational purposes only and does not constitute medical, legal, or insurance advice. Insurance coverage requirements change frequently. Always verify your specific plan's criteria by contacting your insurance provider directly. Mounjaro (tirzepatide) is a prescription medication with risks and potential side effects — see full prescribing information from Eli Lilly. This content is not affiliated with or endorsed by Eli Lilly and Company.
• This guide is independently published. We're an affiliate site — not an insurer, not a pharmaceutical company, not a healthcare provider.