Disclosure: Some links on this site are affiliate links. If you purchase through these links, we may earn a commission at no extra cost to you. Thank you for supporting our site.·For informational purposes only—not medical advice.
Fact-checked against primary sources: ASA 2023 Consensus Guidance, 2024 Multi-Society Clinical Practice Guidance (ASA/AGA/ASMBS/SAGES/ISPCOP), AAOS 2025 Meeting Abstract, FDA prescribing information (revised late 2024), and peer-reviewed meta-analysis in American Journal of Gastroenterology (2024).

When to Stop GLP-1 Before Surgery: Current Guidelines for Every Medication (2026)
By the WPG Research Team | Medical information last verified: February 2026 | Sources: ASA, AGA, ASMBS, SAGES, AAOS, FDA prescribing information — see full source list below
If you're wondering when to stop GLP-1 before surgery, here's the bottom line: most patients can actually continue their GLP-1 medication before elective surgery, according to 2024 multi-society guidance from the American Society of Anesthesiologists (ASA), the American Gastroenterological Association (AGA), and three other major medical societies. But — and this is important — some patients need modifications, some need to hold their dose, and a few may need their surgery rescheduled. It depends on your specific risk factors, which medication you're on, and what kind of procedure you're having.
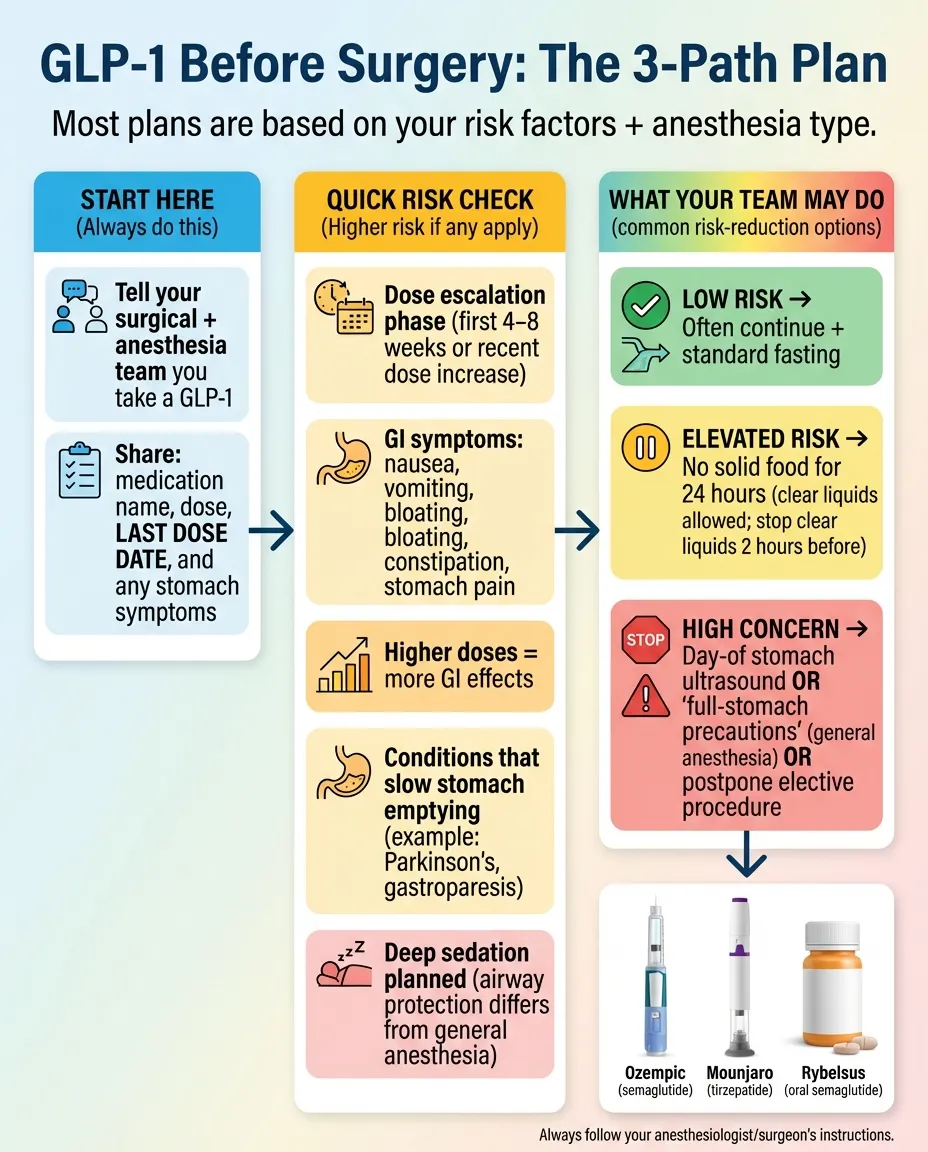
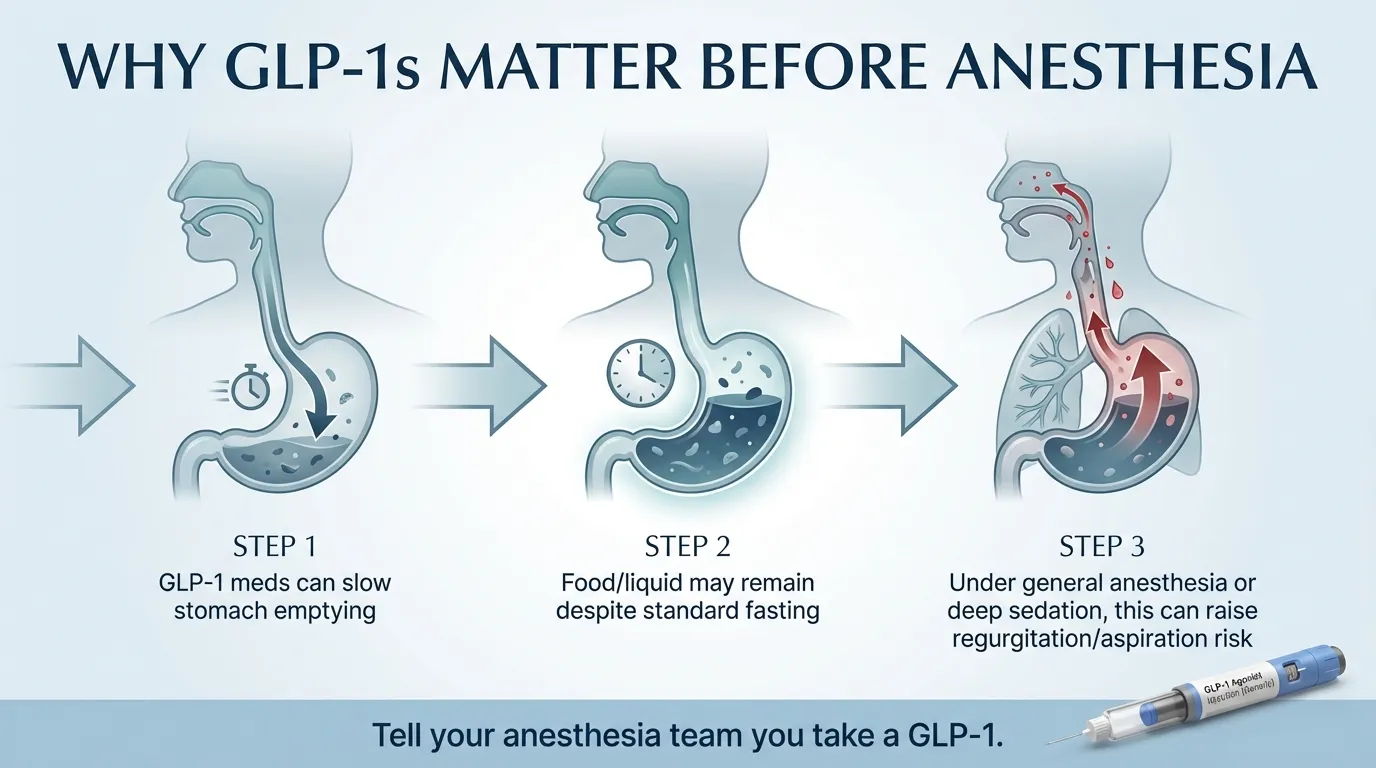
*Illustration for educational purposes only. Always follow your surgical team's specific instructions.*
We spent weeks pulling together every current guideline, FDA label update, and recent study on this topic because the information online is a mess. Some pages still say “stop 7 days before” as a blanket rule. Others say “no need to stop at all.” Neither is fully accurate anymore. The real answer is risk-based and individualized — and that's exactly what we break down below, drug by drug, surgery by surgery, with every major source cited.
Your Most Important Next Step
Tell your surgical team and anesthesiologist that you're on a GLP-1. Do it now — not the day of surgery. That single action prevents most problems.
Quick-Reference: GLP-1 Medications and Surgery Hold Times
If your surgeon or anesthesiologist tells you to hold your medication, here are the timelines based on the 2023 ASA consensus guidance (still the most commonly referenced framework for hold timing):
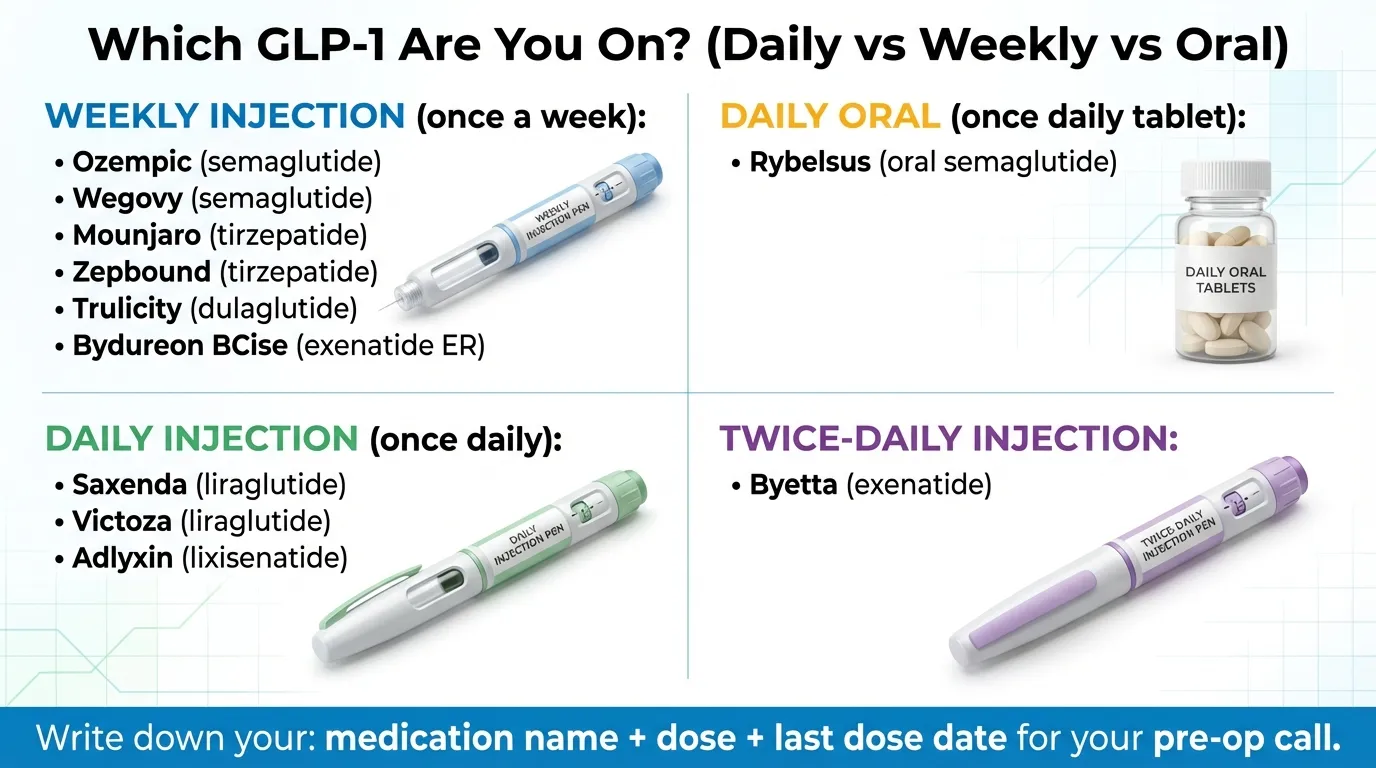
| Medication (Brand) | Generic Name | Daily or Weekly? | If Told to Hold: Timing | Source |
|---|---|---|---|---|
| Ozempic | Semaglutide | Weekly injection | 7 days before (AAOS 2025: 14 days optimal for joint replacement) | ASA 2023; AAOS 2025 |
| Wegovy | Semaglutide | Weekly injection | 7 days before (AAOS 2025: 14 days optimal for joint replacement) | ASA 2023; AAOS 2025 |
| Mounjaro | Tirzepatide | Weekly injection | 7 days before | ASA 2023 |
| Zepbound | Tirzepatide | Weekly injection | 7 days before | ASA 2023 |
| Trulicity | Dulaglutide | Weekly injection | 7 days before | ASA 2023 |
| Bydureon BCise | Exenatide ER | Weekly injection | 7 days before | ASA 2023 |
| Rybelsus | Semaglutide | Daily oral tablet | Day of procedure | ASA 2023 |
| Saxenda | Liraglutide | Daily injection | Day of procedure | ASA 2023 |
| Victoza | Liraglutide | Daily injection | Day of procedure | ASA 2023 |
| Byetta | Exenatide | Twice-daily injection | Day of procedure | ASA 2023 |
| Adlyxin | Lixisenatide | Daily injection | Day of procedure | ASA 2023 |
Critical context: This table shows what to do if your team tells you to hold. The 2024 multi-society guidance says many patients — especially those on a stable dose with no GI symptoms — may not need to hold at all. We explain exactly how to figure out which category you're in below.
Hold times based on 2023 ASA Consensus-Based Guidance on Preoperative Management of Patients on GLP-1 Receptor Agonists. The 2024 Multi-Society Clinical Practice Guidance introduced a risk-based approach where most patients may continue. Always follow your specific surgical team's instructions.
A Closer Look at Each Medication
Not all GLP-1s are identical. Here's what matters for surgical timing with each one.
Semaglutide (Ozempic, Wegovy, Rybelsus) — The most widely prescribed GLP-1 and the one with the most surgical data. Weekly injectable semaglutide has a half-life of approximately one week, meaning it takes roughly 5 weeks to be fully eliminated from your body. But full elimination isn't the goal — the concern is specifically about gastric-emptying effects, which resolve faster than total drug clearance. The 2025 AAOS joint replacement study was conducted specifically with semaglutide. Rybelsus (the daily oral tablet) absorbs differently and has a shorter effective window, which is why the hold time is shorter (day-of rather than 7 days).
Tirzepatide (Mounjaro, Zepbound) — A dual GLP-1/GIP receptor agonist. It works on two hormones instead of one, but the gastric-emptying concern is similar. Tirzepatide has a half-life of approximately 5 days. There is less surgery-specific research on tirzepatide compared to semaglutide, but the ASA guidance treats all GLP-1 class medications the same way for preoperative management.
Liraglutide (Saxenda, Victoza) — A daily injection with a much shorter half-life of approximately 13 hours. Because it's dosed daily and clears faster, the hold time is just the day of the procedure. The gastric-emptying effect is present but wears off more quickly.
Dulaglutide (Trulicity) — A weekly injection with a half-life of about 5 days. Follows the standard 7-day hold if instructed. Less commonly discussed in the surgery context because it's less widely used than semaglutide, but the same class-wide concerns apply.
Exenatide (Byetta, Bydureon BCise) — Byetta is a twice-daily injection; Bydureon BCise is a once-weekly formulation. The twice-daily version has the shortest duration of action in the GLP-1 class. Hold Byetta on the day of the procedure; hold Bydureon BCise for 7 days.
Lixisenatide (Adlyxin) — A daily injection used for type 2 diabetes, often in combination with basal insulin. It's a short-acting GLP-1 RA, so if told to hold, skip it on the day of the procedure. Less commonly prescribed than semaglutide or tirzepatide, but the same class-wide surgical concerns apply.
Why Do GLP-1 Medications Matter Before Surgery?
GLP-1 medications — Ozempic, Wegovy, Mounjaro, Zepbound, and others — work partly by slowing down how fast your stomach empties food. That's actually a feature, not a bug. It's one of the reasons you feel full longer and eat less. For diabetes management, it helps smooth out blood sugar spikes after meals.
But here's where it gets tricky with surgery.
Before any procedure that uses general anesthesia or deep sedation, your stomach needs to be as empty as possible. That's why every patient is told to fast — usually no solid food for 6 to 8 hours and no clear liquids for 2 hours before the procedure. When you're under anesthesia, your normal gag and cough reflexes are turned off. If there's food or liquid sitting in your stomach, it can flow backward into your esophagus and get inhaled into your lungs. This is called aspiration, and it can cause aspiration pneumonia — a serious, sometimes life-threatening complication.
GLP-1 medications can make the standard fasting period insufficient for some patients. Even after following the usual “nothing to eat after midnight” instructions, food may still be sitting in your stomach because of delayed gastric emptying.
What Aspiration Actually Looks Like (And Why It's Taken Seriously)
When we say “aspiration,” here's what that means in practice. During anesthesia, if food or stomach acid flows backward from your stomach into your throat and gets inhaled into your lungs, it causes a chemical burn to the lung tissue. This can lead to:
- Aspiration pneumonia — a lung infection caused by bacteria from the stomach contents. This can require ICU admission, IV antibiotics, and mechanical ventilation.
- Acute respiratory distress syndrome (ARDS) — in severe cases, the lung damage triggers widespread inflammation that makes breathing extremely difficult.
- Airway obstruction — solid food particles can physically block airways.
The severity ranges from mild (a small amount of clear fluid that the lungs can clear) to life-threatening (a large volume of particulate matter that causes bilateral pneumonia). The reason every surgical team takes this seriously is that even though it's rare, the consequences when it DOES happen can be devastating.
Perspective on actual risk:
The absolute risk is low. A 2024 peer-reviewed meta-analysis found GLP-1s delay gastric emptying by about 36 minutes on average in scintigraphy studies. The FDA describes aspiration events as “rare postmarketing reports.” Aspiration during anesthesia is uncommon for any patient, but it can be life-threatening — which is why fasting rules exist and why anesthesiologists take GLP-1 disclosure seriously.
The FDA updated the labels on all GLP-1 receptor agonists in late 2024 to reflect this (most labels revised November 2024; Zepbound revised December 2024). The new warning section reads: “There have been rare postmarketing reports of pulmonary aspiration in patients receiving GLP-1 receptor agonists undergoing elective surgeries or procedures requiring general anesthesia or deep sedation who had residual gastric contents despite reported adherence to preoperative fasting recommendations.” (FDA prescribing information for Ozempic, Wegovy, Mounjaro, Zepbound, Saxenda, Victoza, Trulicity — revised late 2024.)
Here's the nuance most pages don't tell you: This effect on gastric emptying is usually strongest during the first weeks of treatment — the dose-escalation phase — when side effects like nausea and bloating are most common. Over time, most patients develop what doctors call tachyphylaxis: the gastric-slowing effect diminishes as your body adjusts to the medication. The ASA's own consensus document acknowledges that the effects on gastric emptying “are reported to be reduced with long-term use.” So someone who has been on a stable dose for six months with no GI symptoms is in a very different position from someone who just started their first dose three weeks ago.
What Are the Current Guidelines? (And Why They Keep Changing)
This is the part that confuses everyone — and honestly, it's confusing for good reason. The guidelines have changed significantly over the past three years, and not every hospital or surgeon has caught up. If you feel like you're getting conflicting advice, you probably are. Here's why.
*Visual summary of guideline evolution. See detailed breakdown below.*
The 2023 ASA Consensus Guidance: “Hold It”
In June 2023, the American Society of Anesthesiologists released the first formal guidance on GLP-1s and surgery. Their recommendation was straightforward:
- Daily GLP-1s (Rybelsus, Saxenda, Victoza, Byetta): Hold on the day of the procedure.
- Weekly GLP-1s (Ozempic, Wegovy, Mounjaro, Zepbound, Trulicity): Hold for 7 days before the procedure.
These applied regardless of whether you take the medication for diabetes or weight loss, regardless of dose, and regardless of surgery type. If the medication wasn't held and the patient had no GI symptoms, they recommended “full stomach precautions” or using a gastric ultrasound to check stomach contents.
The catch: The ASA was transparent that this guidance was based on “sparse” evidence — “limited only to several case reports.” They were being cautious, which made sense. But it meant every surgeon's office started telling patients to hold their GLP-1 for a week, no questions asked.
This guidance is still the most commonly cited framework. Many hospitals haven't updated their pre-op protocols yet, which is why you'll still see “stop 7 days before” on a lot of paperwork and websites.
(Source: American Society of Anesthesiologists, “Consensus-Based Guidance on Preoperative Management of Patients on Glucagon-Like Peptide-1 Receptor Agonists,” published June 29, 2023.)
The 2024 Multi-Society Update: “Most Can Continue”
In October 2024, five major medical societies — the ASA, AGA, ASMBS, ISPCOP, and SAGES — jointly published updated guidance that represented a significant shift. Their headline recommendation:
Most patients should continue taking their GLP-1 medication before elective surgery.
Instead of a blanket “hold for everyone,” they introduced a risk-based approach:
- Low risk (stable dose, no GI symptoms, no other gastric emptying conditions): Continue your GLP-1 as prescribed. Proceed with standard fasting.
- Elevated risk (dose escalation phase, higher doses, mild GI symptoms): A 24-hour liquid-only diet before surgery, along with potential adjustments to the anesthesia plan (like rapid sequence induction) and possible day-of gastric ultrasound.
- High risk (active severe GI symptoms like vomiting, bloating, abdominal pain): Consider delaying elective surgery until symptoms resolve.
If a hold IS needed, they deferred to the original ASA timing: day-of for daily, 7 days for weekly.
The guidance also raised an important point that gets overlooked: withholding GLP-1 medications carries its own risks. For diabetic patients, stopping can cause dangerous blood sugar spikes. Withholding only from obese or overweight patients “could constitute bias or discrimination,” the guidance noted. And for many patients, insurance and cost logistics make stopping and restarting complicated.
(Source: “Multisociety Clinical Practice Guidance for the Safe Use of Glucagon-like Peptide-1 Receptor Agonists in the Perioperative Period,” published in Clinical Gastroenterology and Hepatology, Surgical Endoscopy, and Anesthesiology, October 29, 2024.)
The 2025 AAOS Meeting Abstract: “14 Days for Joint Replacement”
In March 2025, a study presented at the American Academy of Orthopaedic Surgeons (AAOS) Annual Meeting added another data point. Researchers used the TriNetX database to study patients who took Ozempic (semaglutide) before total hip or knee replacement surgery and found that shorter cessation intervals were linked to higher anesthesia complications:
- Delayed emergence from anesthesia: Elevated risk when last Ozempic dose was 5, 3, or 1 day(s) before surgery.
- Aspiration: Elevated risk at 7, 5, 3, and 1 day(s) before surgery.
- Aspiration pneumonitis: Elevated risk at 7, 5, and 1 day(s) before surgery.
- Conversion to intubation: Elevated risk at 7, 5, 3, and 1 day(s) before surgery.
- Patients who continued Ozempic through surgery had the highest risk for all complications studied.
The researchers' conclusion: for total joint arthroplasty, ceasing GLP-1A 14 days before surgery was optimal for minimizing these complications in this cohort.
Important context: This was a retrospective database study (not a randomized trial) focused specifically on semaglutide and joint replacement surgery. It's an important data point but shouldn't be generalized to all drugs and all surgery types. Also note: the AAOS conclusion doesn't say “zero risk at 14 days” — it says 14 days was the optimal timing for risk reduction in this dataset.
(Source: “Optimal Timing for Cessation of GLP-1 Agonist Before Elective Total Hip and Knee Arthroplasty,” presented at AAOS 2025 Annual Meeting, published via TriNetX Research Network data.)
The Peer-Reviewed Meta-Analysis: “Maybe We're Overreacting”
On the other end of the spectrum, a 2024 systematic review and meta-analysis published in the American Journal of Gastroenterology (led by researchers at Brigham and Women's Hospital and Houston Methodist) quantified how much GLP-1 medications actually delay gastric emptying. They included 15 studies that met criteria. In the five studies using gastric emptying scintigraphy (the gold-standard test, 247 patients), GLP-1 RA delayed gastric emptying by approximately 36 minutes on average compared to placebo. On liquid-emptying tests, there was no significant delay at all.
The researchers concluded that while the delay is measurable, it's relatively modest compared to the 6- to 8-hour fasting periods required before surgery.
Separately, the Houston Methodist blog summary of related research noted a database analysis estimating aspiration risk at roughly 3 in 100,000 patients on GLP-1s — though this specific figure should be treated as a rough estimate, not a definitive rate, as the underlying study details were not fully published.
(Sources: Hiramoto B, McCarty TR, et al. “Quantified Metrics of Gastric Emptying Delay by Glucagon-Like Peptide-1 Agonists.” American Journal of Gastroenterology, June 2024. PubMed ID: 38634551. Houston Methodist Hospital blog summary, July 2024.)
The Guideline Comparison Matrix
Here's every major guideline in one place so you can see exactly where they agree and where they differ:
| 2023 ASA Consensus | 2024 Multi-Society | AAOS 2025 Abstract | FDA Label (Late 2024) | |
|---|---|---|---|---|
| Default approach | Hold before surgery | Risk-based: most can continue | Ceasing 14 days before was optimal (joint replacement) | “Instruct patients to inform providers” |
| Daily GLP-1s | Hold day of procedure | Continue if low-risk; liquid diet if higher-risk | Not studied separately | No specific hold guidance |
| Weekly GLP-1s | Hold 7 days before | Continue if low-risk; liquid diet if higher-risk | 14 days optimal for semaglutide/joint surgery | No specific hold guidance |
| High-risk patients | Full-stomach precautions or delay | Liquid diet 24h + anesthesia plan changes + ultrasound; rare delay | Cessation <7 days associated with complications | “Available data are insufficient to inform recommendations” |
| If dose wasn't held | Full-stomach precautions or gastric ultrasound | Day-of assessment + shared decision-making | N/A | N/A |
| Evidence basis | Case reports (acknowledged as “sparse”) | Expert consensus + limited clinical data | Retrospective database study (TriNetX) | Postmarketing reports |
This table is why the advice you're getting seems inconsistent. Different providers are following different guidelines — and some hospitals haven't updated their protocols since 2023. None of them are “wrong” per se. They're working with different evidence and different risk tolerance.
What This All Means for You
The guidance has evolved from “always hold” (2023) to “individualized risk assessment” (2024) to “even longer for certain surgeries” (2025), with some researchers questioning whether a blanket hold is needed at all.
Here's our honest take: The truth is somewhere in the middle. The aspiration risk is real but rare. The guidelines are moving toward a more nuanced, risk-based approach. And the most important thing you can do is communicate with your surgical team and let them make the call for YOUR specific situation.
If your surgeon's office tells you to hold for 7 days, that's based on established guidance — follow it. If your anesthesiologist says you can continue with a liquid diet modification, that's based on the newer guidance — follow that. What you should NOT do is make the decision on your own or hide your medication use from your team.
Are You Higher Risk or Lower Risk? A Quick Self-Check
The 2024 multi-society guidance and the ASA's patient-facing information both identify specific factors that increase concern about delayed gastric emptying before surgery. This isn't a formal medical assessment — it's a starting point for the conversation with your team.
*Visual risk assessment guide. Always discuss your individual situation with your surgical team.*
Factors That May Increase Your Risk
- You're in the dose-escalation phase (first 4 to 8 weeks on the medication, or you recently increased your dose). GI side effects — and gastric-slowing effects — are most pronounced during this period.
- You have active GI symptoms right now: nausea, vomiting, bloating, abdominal pain, constipation. Per the ASA: “You shouldn't undergo surgery until the symptoms are gone.”
- You're on a higher dose than typically prescribed. Higher doses mean more GI effects.
- You have other medical conditions that slow gastric emptying, such as gastroparesis, Parkinson's disease, or bowel dysmotility.
- Your procedure uses deep sedation rather than general anesthesia. “Full stomach precautions” (like rapid sequence intubation) are only available with general anesthesia, not sedation.
Factors That Suggest Lower Risk
- You've been on a stable dose for several months with no GI symptoms.
- You're on a daily formulation (shorter-acting).
- You're on a lower dose.
- You have no other conditions that affect gastric emptying.
- You're having a procedure under local or regional anesthesia only (no sedation, no general anesthesia).
If you fall into the lower-risk category, the 2024 multi-society guidance says you may be able to continue your GLP-1 with standard fasting protocols. But — broken record alert — discuss it with your surgical team.
(Sources: ASA patient guidance at madeforthismoment.asahq.org; 2024 Multi-Society Clinical Practice Guidance.)
Does the Type of Surgery Matter?
Yes, significantly. Here's how the guidance breaks down by procedure type.
*Surgery-type-specific guidance overview. Individual instructions from your team take priority.*
Elective Surgery Under General Anesthesia
This is where the bulk of the guidance applies. Follow the risk-based approach above. If you're lower risk, you may continue with standard fasting (or a 24-hour liquid diet if your team prefers extra caution). If you're higher risk, your team may hold the medication, adjust the anesthesia plan, or use a day-of gastric ultrasound.
Endoscopy and Colonoscopy
The American Gastroenterological Association addressed this separately. For endoscopy, GLP-1 medications generally do not need to be stopped, especially for patients taking them for diabetes (where maintaining blood sugar control is important). Standard colonoscopy prep — which already involves a liquid diet and bowel prep — typically takes care of the gastric emptying concern.
If you have severe GI symptoms, your gastroenterologist may recommend additional precautions or consider a transabdominal ultrasound to check stomach contents before the procedure.
(Source: AGA Rapid Clinical Practice Update on Management of Patients Taking GLP-1 Receptor Agonists Prior to Endoscopy.)
Joint Replacement (Hip and Knee)
Based on the 2025 AAOS study, 14 days may be the optimal hold time for semaglutide before total joint arthroplasty. This is more conservative than the standard 7-day recommendation, and it's specific to this surgery type. If you're scheduled for hip or knee replacement and you're on Ozempic or Wegovy, bring this study up with your orthopedic surgeon.
Plastic Surgery (Tummy Tuck, BBL, Breast Augmentation, etc.)
Plastic surgeons tend to be the most conservative. Many require holding GLP-1s for 2 to 4 weeks before surgery. There are actually two reasons for this — not just one.
The aspiration risk is the obvious concern. But the second issue is nutritional status. GLP-1 medications reduce appetite significantly, and some patients — especially those who've lost weight rapidly — develop nutritional deficiencies that impair wound healing. If your body doesn't have adequate protein, vitamins, and minerals, surgical incisions take longer to heal, infection risk goes up, and aesthetic outcomes can suffer.
Some plastic surgeons require:
- Pre-albumin blood tests several months before surgery to check protein status
- A high-protein nutritional shake daily starting one week before surgery and continuing two weeks after
- A complete metabolic panel to check for other deficiencies
- A minimum of 4 weeks off GLP-1 before surgery, with 4 to 6 weeks before restarting after
If you've been eating very little due to your GLP-1's appetite suppression, your surgeon needs to know that. It directly affects your body's ability to recover.
Bariatric Surgery (Gastric Sleeve, Gastric Bypass)
This is a nuanced situation because you're likely on a GLP-1 for weight loss, and the bariatric surgeon may have recommended it as part of your pre-surgical weight loss plan. A liquid diet before bariatric surgery is already standard practice, which partially addresses the gastric emptying concern. The multi-society guidance authors include bariatric surgeons (ASMBS), so the risk-based framework was designed with these patients in mind. Follow your bariatric surgeon's protocol.
Dental Surgery Under IV Sedation or General Anesthesia
Routine dental work with local anesthesia (novocaine, lidocaine) has no relevance to GLP-1 concerns. But dental surgery under IV sedation or general anesthesia — such as wisdom tooth extraction or oral surgery — falls under the same guidelines as any other sedation procedure. Tell your oral surgeon and the anesthesia provider about your GLP-1 use.
Minor Procedures Under Local Anesthesia Only
If your procedure uses only local anesthesia (like a dermatological procedure, dental work with local numbing, or an office-based procedure with no sedation), the aspiration risk doesn't apply. Your protective airway reflexes stay intact. You can generally continue your GLP-1 as usual. Still tell your provider — it's good practice.
Emergency Surgery
There's no time to hold. The surgical team will treat you as a “full stomach” patient and take precautions accordingly — typically rapid sequence induction for intubation. If you're awake and able to communicate, tell the emergency team immediately that you're on a GLP-1. This changes how they manage your airway.
What If You Already Took Your Dose and Surgery Is Soon?
This is one of the most common — and most anxiety-inducing — situations. You took your weekly Ozempic injection three days ago, and your surgery is tomorrow. Or you just realized you were supposed to hold it and didn't.
First: Don't panic. And don't hide it.
Hiding your GLP-1 use from your surgical team is far more dangerous than disclosing it. If they don't know, they can't take precautions. If they do know, they have options.
What Your Anesthesiologist Can Do
If you disclose that you took your GLP-1 recently and it wasn't held as recommended, here's what typically happens:
- They assess your symptoms. No nausea, no bloating, no vomiting? That's a good sign.
- They may use a point-of-care gastric ultrasound to literally look at your stomach and see if there's residual food or liquid. If your stomach is empty, they can proceed normally.
- They may proceed with “full stomach precautions.” For general anesthesia, this means rapid sequence induction — a faster intubation technique designed to protect your airway.
- For sedation cases, they may recommend switching to general anesthesia (which allows for airway protection) or rescheduling.
- In rare cases, they may postpone the surgery — but only if the risk is deemed too high and the procedure isn't urgent.
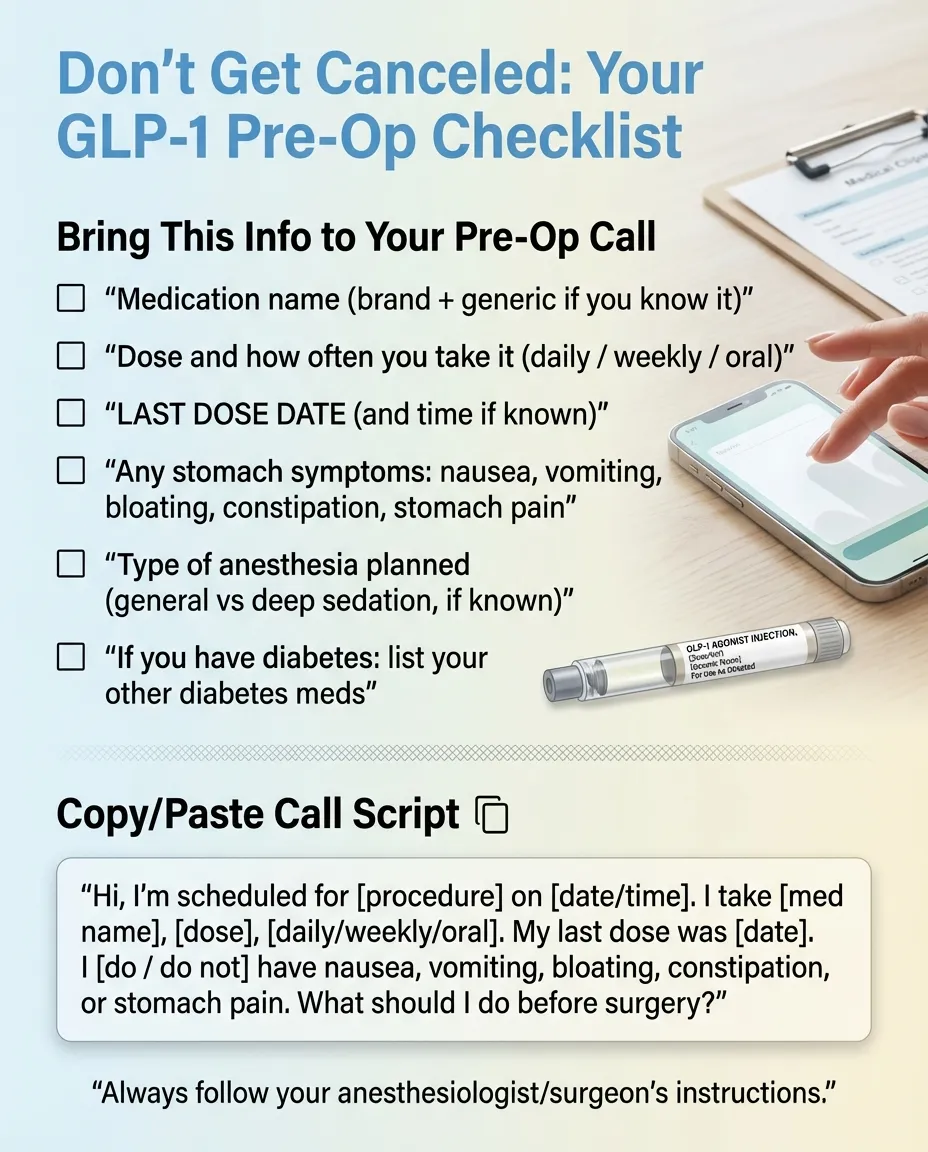
What to Say (A Template You Can Copy)
“Hi, I'm scheduled for [procedure] on [date]. I want to let you know that I take [medication name], [dose], injected/taken [weekly/daily]. My last dose was on [date]. I [do / do not] have any nausea, vomiting, bloating, or abdominal pain right now. What should I do?”
That's it. Give them the information and let them make the call. They deal with this regularly now — a November 2025 KFF poll found about 1 in 8 U.S. adults (12%) are currently taking a GLP-1 drug, with nearly 1 in 5 (18%) having taken one at some point.
Will You Gain Weight If You Stop for Surgery?
We know this is a real concern. It's the question people feel embarrassed to ask, but it matters — because some patients avoid disclosing their GLP-1 use to their surgeon because they're afraid of being told to stop.
For a 1- to 2-week hold: Unlikely to cause meaningful weight regain. The medication's appetite-suppressing effects don't disappear overnight. You may notice slightly increased hunger as the drug wears off, but 7 to 14 days is not enough to undo months of progress.
Obesity specialist Dr. Louis Aronne has noted that after stopping a GLP-1 for weight management, noticeable changes typically take about a month to appear. A short surgical hold is well within that buffer.
For a 3- to 4-week hold (as some plastic surgeons require): You may experience more noticeable hunger and potentially a few pounds of fluctuation. This is temporary and reversible once you restart.
The bottom line: A temporary hold for surgical safety is not going to derail your weight loss journey. But hiding your medication from your surgeon could put your life at risk. Please don't make that trade.
What If You Take GLP-1 for Diabetes?
This is more medically complex. Stopping your GLP-1 will affect blood sugar control. Uncontrolled blood sugar heading into surgery carries its own serious risks, including infection and poor wound healing.
Both the 2023 ASA guidance and the 2024 multi-society update address this directly: If your GLP-1 is held for longer than one dosing cycle, consult your endocrinologist or prescribing doctor about bridging therapy — an alternative diabetes medication to keep blood sugar in range during the hold period.
This is one of the strongest reasons the 2024 guidance shifted toward letting most patients continue: the risks of uncontrolled blood sugar can be just as concerning as the risks of delayed gastric emptying.
Starting, restarting, or switching? See verified pricing.
If Your Team Says Continue: What to Do Before Surgery
Even if you're cleared to keep taking your GLP-1, your team may recommend extra precautions. Here's what that looks like in practice.
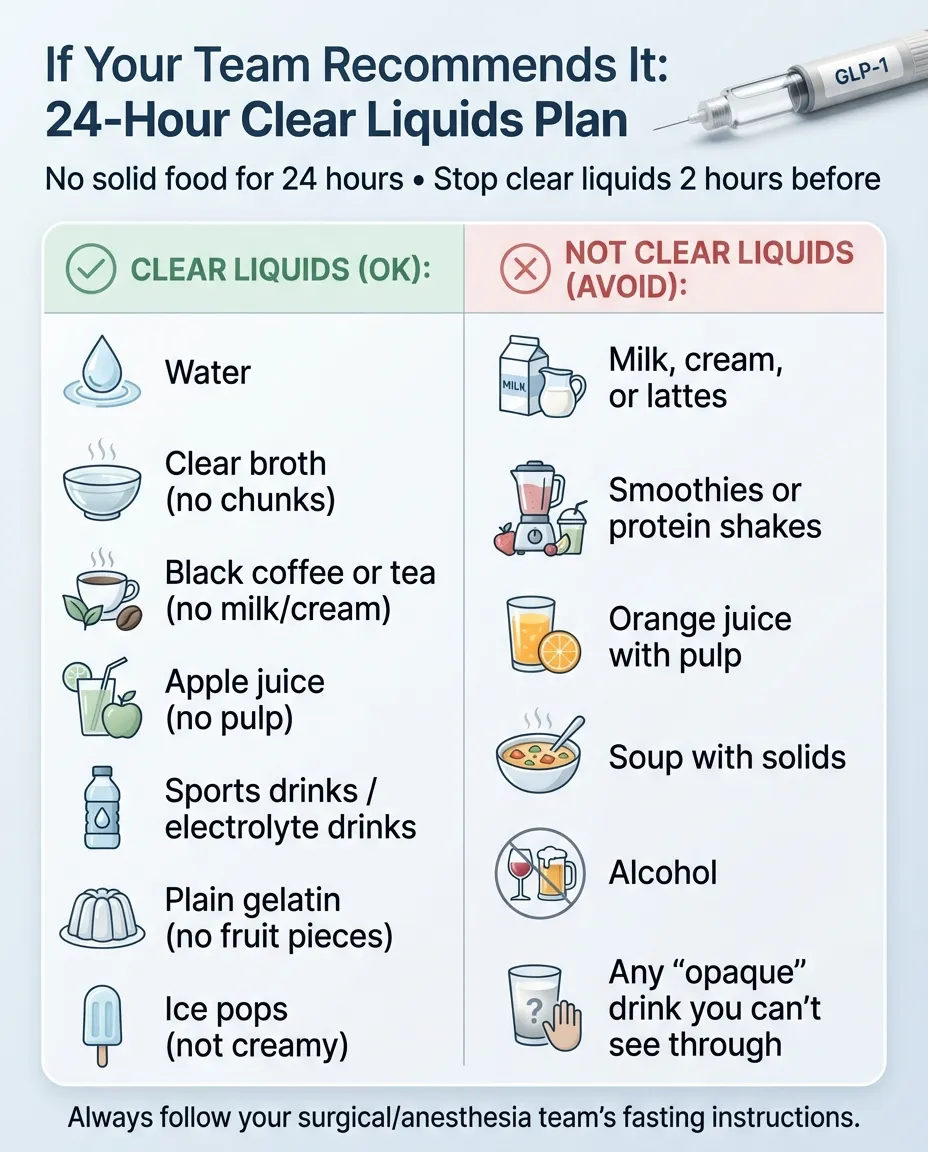
The 24-Hour Liquid Diet (Exactly What It Means)
If you're on a higher dose or your team wants additional risk reduction, you may be asked to follow a 24-hour liquid-only diet before surgery. This is the same concept as colonoscopy prep — give your stomach extra time to empty completely.
Clear Liquids You CAN Have
(Until 2 hours before your procedure)
- Water
- Clear broth (no chunks)
- Black coffee or tea (no cream)
- Apple juice (no pulp)
- Gatorade or Pedialyte
- Plain gelatin (like Jell-O — no fruit pieces)
- Popsicles (not creamy ones)
NOT Clear Liquids (Do NOT Consume)
- Milk
- Smoothies, protein shakes
- Anything creamy or opaque
- Orange juice with pulp
- Soups with solids
- Alcohol
A Simple Schedule
- Morning (day before surgery): Clear liquids only. No solid food starting now.
- Throughout the day: Stay hydrated. Alternate water, broth, and electrolyte drinks.
- Evening: Continue clear liquids.
- [X] hours before surgery: Nothing at all — follow your specific NPO (nothing by mouth) instructions exactly.
Standard Fasting Rules Still Apply
Even if you're continuing your GLP-1, you still follow your team's standard fasting instructions. Typically: no solid food for 6 to 8 hours before surgery, no clear liquids for 2 hours before. These rules exist for ALL patients, not just those on GLP-1s.
Restarting Your GLP-1 After Surgery
This is the question that almost every other page on this topic either skips or answers vaguely. Here's what we know.
When to Restart
There are no formal universal guidelines on exact restart timing. The general principle: restart when you can eat and drink normally without significant nausea or vomiting, and your surgical team gives clearance.
Factors that may delay your restart:
- Surgery involved your GI tract (stomach, intestines) — you may need longer for your gut to recover.
- You're on opioid pain medications post-surgery — opioids also slow gastric emptying. Adding a GLP-1 on top of that can compound the effect.
- You can't tolerate solid food yet — if you're still on IV nutrition or having significant nausea.
- Your surgeon has a specific protocol — especially common after plastic surgery (some require 4 to 6 weeks post-op before resuming).
Do You Need to Re-Titrate?
If you held for less than 2 to 3 weeks, you can usually restart at the same dose you were on. If you held for 4 or more weeks, your prescribing provider may recommend starting at a lower dose and titrating back up to reduce the chance of GI side effects when you restart. Think of it like getting re-acclimated.
Ask your prescribing doctor specifically: “I held my [medication] for [X weeks] for surgery. Should I restart at my previous dose or at a lower dose?”
Your Pre-Surgery GLP-1 Checklist
Print this, screenshot it, or save it to your phone. It covers every step from the moment surgery is scheduled to the day after.
As Soon as Surgery Is Scheduled
- Tell your surgeon's office you are taking a GLP-1 medication. Specify the drug name, dose, and how often you take it.
- Tell your anesthesiologist or anesthesia team (this may be a separate contact).
- Tell the doctor who prescribes your GLP-1 that you have upcoming surgery. If you're diabetic, ask about bridging therapy.
- Ask your surgical team: “Should I hold my GLP-1? If so, when should my last dose be?”
- Ask: “Should I follow a liquid diet the day before surgery?”
- Ask: “When can I restart my GLP-1 after surgery?”
- Get answers in writing if possible (MyChart message, email, or written instructions).
1 to 2 Weeks Before Surgery
- Confirm your last GLP-1 dose date with your care team.
- If holding a weekly injection: Take your last dose at least 7 days before surgery (or 14 days for joint replacement).
- If diabetic and holding: Start bridging therapy as directed by your prescriber.
- Report any new GI symptoms (nausea, vomiting, bloating, constipation) to your surgical team immediately — this may change the plan.
24 Hours Before Surgery
- If directed: Switch to clear liquids only (no solid food).
- If on a daily GLP-1: Skip your dose (or as directed by your team).
- Continue taking all other medications unless specifically told otherwise.
- Stay hydrated with clear fluids.
Day of Surgery
- Follow your NPO (nothing by mouth) cutoff time exactly — no food, no water, no gum, nothing.
- Remind your anesthesiologist or nurse anesthetist about your GLP-1 use and your last dose date.
- If you have ANY GI symptoms (even mild nausea), tell the team immediately. Do not hide them.
- If you forgot to hold and took a dose you shouldn't have — tell them. They have options.
After Surgery
- Resume your GLP-1 only when cleared by your surgical team.
- Make sure you can eat and drink without significant nausea or vomiting first.
- If you held for 4+ weeks: Ask your prescriber about re-titration.
- If diabetic: Discuss the GLP-1 restart timeline explicitly — you may need to continue bridging therapy until you're back on your full dose.
What If You Get Conflicting Instructions?
This happens more often than you'd expect. Your prescribing doctor says continue. Your surgeon says hold for two weeks. Your pre-op packet doesn't mention GLP-1s at all. The nurse on the phone isn't sure. Now you're stuck.
Here's how to handle it:
- Don't try to resolve it yourself. You shouldn't have to be the referee between your medical providers.
- Ask the higher-risk provider to coordinate. Usually, that's the anesthesiologist. Call the surgical team and say: “I'm getting different instructions about my GLP-1 from my prescriber and your office. Can my anesthesiologist and my prescribing doctor coordinate directly?”
- When in doubt, the more conservative approach is usually safer. If one provider says continue and another says hold, holding for the recommended period is unlikely to cause harm (except in diabetic patients where blood sugar management is a concern — and that's precisely why the providers need to talk to each other).
- Get the final answer in writing. A MyChart message, an email, or written instructions. You want clarity, not a game of telephone.
The underlying problem: Many hospitals haven't updated their pre-op protocols since 2023. The nurse reading from a form may be giving you 2023 guidance, while your endocrinologist is aware of the 2024 update. This is a systems problem, not a “someone is wrong” problem. The fix is direct communication between your providers.
Other Medications to Know About Before Surgery
While we're focused on GLP-1s here, you should know that they're not the only medications that get adjusted before surgery. If you're on any of these, mention them to your surgical team as well:
- SGLT2 inhibitors (Jardiance, Invokana, Farxiga): Typically held 3 to 4 days before surgery due to risk of diabetic ketoacidosis.
- Metformin: Often held 1 to 2 days before surgery, especially if you're having a procedure involving contrast dye or if there's risk of kidney stress.
- Blood thinners (Eliquis, Xarelto, Coumadin, aspirin): Hold times vary by medication and procedure — your surgeon will give specific instructions.
- Insulin: Requires a customized plan, usually in coordination with your endocrinologist. Do NOT stop insulin on your own.
If you take multiple medications for diabetes or weight management, make sure your surgical team has the complete list — not just the GLP-1.
What About Compounded Semaglutide or Tirzepatide?
If you're using compounded semaglutide or compounded tirzepatide from a compounding pharmacy (rather than brand-name Ozempic, Wegovy, Mounjaro, or Zepbound), the same pre-surgery guidelines apply. Compounded formulations are not FDA-approved but work through the same mechanism of action. The gastric-emptying effect is the same concern for anesthesia regardless of the product source.
Treat it identically for surgery purposes. And make sure to tell your surgical team the exact dose and how often you're taking it — compounded formulations may have different concentrations than brand-name products.
Looking for a provider? See our verified comparison of telehealth GLP-1 programs.
Frequently Asked Questions: GLP-1 Medications and Surgery
When should I stop Ozempic before surgery?
The most commonly cited guidance is to hold Ozempic for 7 days before surgery (ASA 2023). For hip or knee replacement, emerging evidence suggests 14 days may be better (AAOS 2025). However, the 2024 multi-society guidance says many patients on a stable dose with no GI symptoms may be able to continue. Follow your surgical team's specific instructions.
When should I stop Wegovy before surgery?
Same as Ozempic — both contain semaglutide and are dosed weekly. Hold 7 days if instructed, or discuss continuing with your team if you're low-risk per the 2024 guidance.
When should I stop Mounjaro or Zepbound before surgery?
Both contain tirzepatide and are dosed weekly. The same 7-day hold applies if instructed. The same risk-based approach from the 2024 multi-society guidance applies to all GLP-1 and GLP-1/GIP medications.
When should I stop Rybelsus before surgery?
Rybelsus is oral semaglutide taken daily. If told to hold, skip it on the day of the procedure. Some providers may ask you to skip it the day before as well.
Do I need to stop my GLP-1 for a colonoscopy?
Usually not. The AGA says GLP-1s generally don't need to be stopped for endoscopy. Standard colonoscopy prep (liquid diet + bowel prep) typically handles the gastric emptying concern. Talk to your gastroenterologist if you have GI symptoms.
What if I forgot to stop my GLP-1 before surgery?
Tell your anesthesiologist immediately. They can assess your risk, potentially use gastric ultrasound to check stomach contents, and proceed with full stomach precautions if needed. Do NOT hide it.
Will my surgery be canceled if I didn't stop my GLP-1?
It could be postponed if the anesthesiologist determines the aspiration risk is too high — but that's rare and usually only happens when there are active GI symptoms combined with a recent dose. Communicating early is the best prevention.
Can I just fast longer instead of stopping my GLP-1?
A longer fast alone may not fully address the delayed gastric emptying from GLP-1 medications. However, a 24-hour liquid-only diet before surgery — combined with standard fasting — is one of the risk-mitigation strategies recommended in the 2024 multi-society guidance.
What is gastric ultrasound and will my hospital do it?
A point-of-care gastric ultrasound is a quick, noninvasive scan done on the day of surgery to check whether your stomach still has food or liquid in it. Not every hospital has this capability, but many anesthesia teams can do it. If you're concerned about your GLP-1 and surgery, ask if this option is available.
What if I'm in the dose-escalation phase?
The ASA patient guidance recommends waiting until the escalation phase is over and any GI side effects have resolved before having elective surgery, if possible. If your surgery can't wait, your team will use additional precautions.
My surgeon says hold for 3 weeks, but the ASA says 7 days. Who do I listen to?
Your surgeon. They know your specific procedure and your specific risk factors. The ASA provides general guidance. Your surgeon may have procedure-specific or patient-specific reasons for a longer hold — especially for plastic surgery, bariatric surgery, or joint replacement.
Does this apply to procedures under local anesthesia?
No. Aspiration risk only applies to general anesthesia and deep sedation, where your airway reflexes are suppressed. Procedures under local anesthesia only (like dental work, dermatology, or office procedures) don't carry this risk. Still mention your GLP-1 to the provider for completeness.
Is the aspiration risk actually common?
Rare, but serious when it happens. The FDA describes these as "rare postmarketing reports." A peer-reviewed meta-analysis found GLP-1s delay solid-food gastric emptying by an average of about 36 minutes — relatively modest compared to the 6- to 8-hour pre-surgical fast. The risk is low, but aspiration pneumonia can be severe or fatal, which is why precautions exist.
What if my prescriber and my surgeon give conflicting instructions?
Ask them to communicate directly. If your prescriber says continue and your surgeon says hold, ask one of them: "Can you please coordinate with the other doctor so we're all on the same page?" You should not have to choose between conflicting medical advice on your own.
When can I restart my GLP-1 after surgery?
When you can eat and drink normally without significant nausea, and your surgical team gives clearance. This varies by surgery type and individual recovery. If you held for several weeks, ask about re-titration.
Will I gain weight during the surgical hold?
A 1- to 2-week hold is unlikely to cause meaningful weight regain. Longer holds (3 to 4 weeks) may result in slightly increased hunger, but this reverses once you restart. The surgical safety benefit far outweighs a temporary pause.
Does GLP-1 cause hypoglycemia if I'm fasting for surgery?
GLP-1 medications on their own have a low risk of hypoglycemia because they stimulate insulin release in a glucose-dependent way. However, if you also take insulin or sulfonylureas (like glipizide or glyburide), the combination CAN cause low blood sugar, especially during a prolonged fast. Tell your team about ALL your diabetes medications.
What if I just started my GLP-1 last week — should I postpone surgery?
If your surgery is truly elective and can be rescheduled without medical risk, the ASA patient guidance suggests it may be best to wait until the dose-escalation phase is complete and any GI side effects have subsided. That's typically 4 to 8 weeks. But if the surgery is medically necessary, your team can manage the additional risk with precautions.
Is the risk the same for all GLP-1 medications?
The gastric-emptying effect is a class-wide concern — all GLP-1 receptor agonists share it. However, the degree varies. Short-acting formulations (daily dosing) tend to have less sustained gastric slowing than long-acting ones (weekly dosing). The dose matters too — higher doses produce more pronounced effects. Individual variation is significant.
I had surgery last year while on a GLP-1 and nothing happened. Am I safe to skip the precautions this time?
Past surgical success doesn't guarantee future safety. Your dose may have changed, your health status may be different, and the specific procedure and anesthesia type may differ. Follow the current guidelines and communicate with your team every time, regardless of past experience.
What about GLP-1 medications and sedation for procedures like MRI or dental work?
Standard MRI doesn't use sedation for most adults, so no concern. If you need sedation for dental work, minor procedures, or pediatric MRI, the same principles apply as any sedation case: disclose your GLP-1 use, follow fasting instructions, and let the sedation team assess your risk.
The Real-World Timeline: Putting It All Together
To make all of this practical, here's how the timeline actually works for the most common scenarios — someone on a weekly GLP-1 (like Ozempic, Wegovy, Mounjaro, or Zepbound) with elective surgery coming up.
Scenario 1: Low-Risk Patient (Stable Dose, No GI Symptoms)
- 4+ weeks before surgery: Tell your surgical team about your GLP-1 at your pre-op visit. Provide: drug name, dose, injection day, last dose date.
- 1 week before surgery: Your team may say “continue as usual” per 2024 multi-society guidance. Or they may say “hold this week's dose” per 2023 ASA guidance. Follow whatever they say.
- 24 hours before surgery: If directed, switch to clear liquids only. Otherwise, follow standard fasting instructions.
- Day of surgery: Final fasting. Remind the anesthesia team about your GLP-1. If all is clear, surgery proceeds normally.
Scenario 2: Higher-Risk Patient (Dose Escalation, Some GI Symptoms)
- 4+ weeks before surgery: Disclose everything. Mention that you're still in the escalation phase and/or having side effects. Your team may recommend delaying elective surgery until you're stable, or they'll plan additional precautions.
- 1 week before surgery: Hold your weekly dose (7 days before surgery date). If you're diabetic, start bridging therapy as directed.
- 24 hours before surgery: Clear liquids only — nothing solid. Stay hydrated.
- Day of surgery: Full fasting. The anesthesia team may use rapid sequence induction and/or gastric ultrasound. If your stomach is empty and you have no symptoms, surgery proceeds. If there's concern, they'll discuss options with you.
Scenario 3: Joint Replacement Patient
- 3+ weeks before surgery: Based on the AAOS 2025 data, discuss a 14-day hold with your orthopedic surgeon. Take your last dose at least 14 days before your surgery date.
- 2 weeks before surgery: Your last injection should already be behind you.
- 24 hours before surgery: Follow whatever dietary instructions your surgical team gives you.
- Day of surgery: Standard anesthesia approach, with the knowledge that you've had a full 14-day hold.
Scenario 4: Emergency Surgery — No Time to Prepare
Tell the emergency team you're on a GLP-1 as soon as you're able to communicate. They will treat you as a “full stomach” patient: rapid sequence induction, aspiration precautions, close monitoring. This is a well-practiced protocol for any patient with potential gastric contents. The key is that they KNOW about your medication so they can plan accordingly.
What to Do Next
The 5 things that matter most — everything else is detail:
- Tell your surgical team you're on a GLP-1. Name, dose, frequency, last dose date. Do it the moment surgery is scheduled — not the day of.
- Ask specifically whether to hold or continue. Don't assume either way. Get clear instructions.
- If you have GI symptoms, report them immediately. Nausea, vomiting, bloating, or abdominal pain can change the plan.
- If you're diabetic, coordinate bridging therapy. Don't hold your GLP-1 without a backup plan for blood sugar.
- Follow YOUR team's instructions. Not the internet's. Not your friend's. Not ours. Your surgical team knows your case.
You now know more about GLP-1 medications and surgery than 99% of patients walking into a pre-op appointment. Use that knowledge. Call your surgical team. Ask the right questions. Bring the checklist.
And if you're looking for a GLP-1 provider — whether you're starting for the first time, restarting after surgery, or switching from a compounding pharmacy to a telehealth platform — we've compared the top options with verified pricing and honest reviews.
Verified pricing. Honest reviews. No hidden costs.
How We Researched This Guide
We built this guide by synthesizing every current authoritative source on GLP-1 medications and surgery:
- ASA 2023 Consensus-Based Guidance on Preoperative Management of Patients on GLP-1 Receptor Agonists (published June 2023)
- 2024 Multi-Society Clinical Practice Guidance from ASA, AGA, ASMBS, ISPCOP, and SAGES — published in Clinical Gastroenterology and Hepatology, Surgical Endoscopy, and Anesthesiology (October 2024)
- ASA Patient-Facing Guidance at madeforthismoment.asahq.org — “Drugs for Diabetes or Weight Loss: What To Know Before Surgery” (medically reviewed, updated October 2025)
- 2025 AAOS Study — “Optimal Timing for Cessation of GLP-1 Agonist Before Elective Total Hip and Knee Arthroplasty,” presented at AAOS 2025 Annual Meeting (March 2025)
- Houston Methodist Meta-Analysis — published in American Journal of Gastroenterology (June 2024)
- Cleveland Clinic Journal of Medicine — “Should glucagon-like peptide 1 receptor agonists be withheld during the preoperative period?” (April 2025)
- FDA Prescribing Information for Ozempic, Wegovy, Rybelsus, Mounjaro, Zepbound, Saxenda, Victoza, Trulicity — specifically Section 5.9/5.10/5.11 (Pulmonary Aspiration During General Anesthesia or Deep Sedation), updated November 2024
- PMC Review Articles on GLP-1 receptor agonists and perioperative management
We review and update this guide when new guidelines, studies, or FDA label changes are published. All medical information is verified against primary sources. This content is not medical advice — always follow your specific surgical team's instructions.
Sources
- American Society of Anesthesiologists. “Consensus-Based Guidance on Preoperative Management of Patients (Adults and Children) on Glucagon-Like Peptide-1 (GLP-1) Receptor Agonists.” Published June 29, 2023. asahq.org
- Kindel TL, Wang AY, Wadhwa A, et al. “Multisociety Clinical Practice Guidance for the Safe Use of Glucagon-like Peptide-1 Receptor Agonists in the Perioperative Period.” Clinical Gastroenterology and Hepatology; Surgical Endoscopy; Anesthesiology. Published October 29, 2024. PMC (free full text)
- American Society of Anesthesiologists. “Drugs for Diabetes or Weight Loss: What To Know Before Surgery.” Made For This Moment. asahq.org
- Chokshi SN, Hou N, Ford MC, et al. “Optimal Timing for Cessation of GLP-1 Agonist Before Elective Total Hip and Knee Arthroplasty.” Presented at AAOS 2025 Annual Meeting, March 2025. Abstract PDF
- Hiramoto B, McCarty TR, et al. “Quantified Metrics of Gastric Emptying Delay by Glucagon-Like Peptide-1 Agonists: A Systematic Review and Meta-Analysis.” American Journal of Gastroenterology, June 2024;119(6):1126-1140. PubMed
- FDA Prescribing Information for Ozempic (semaglutide injection). Section 5.9/5.10: Pulmonary Aspiration During General Anesthesia or Deep Sedation. Revised November 2024. accessdata.fda.gov
- FDA Prescribing Information for Wegovy (semaglutide injection). Section 5.11. Revised November 2024. accessdata.fda.gov
- FDA Prescribing Information for Zepbound (tirzepatide injection). Revised December 2024. accessdata.fda.gov
- FDA Prescribing Information for Rybelsus (semaglutide tablets). Section 5.9. Revised November 2024. accessdata.fda.gov
- American Gastroenterological Association. “Most patients can continue GLP-1 anti-obesity drugs before surgery.” October 30, 2024. gastro.org
- KFF Health Tracking Poll. “Prescription Drug Costs, Views on Trump Administration Actions, and GLP-1 Use.” November 2025. kff.org
- Cleveland Clinic Journal of Medicine. “Should glucagon-like peptide 1 receptor agonists be withheld during the preoperative period?” April 2025. ccjm.org
- UCLA Health. “Medications to Stop Before Surgery — Endocrine Surgery.” uclahealth.org
Medical Disclaimer: This guide is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always follow the specific instructions of your surgical team, anesthesiologist, and prescribing healthcare provider. Individual medical decisions should be made in consultation with qualified healthcare professionals who know your complete medical history. Guidelines and evidence evolve — we update this page regularly, but we cannot guarantee real-time accuracy.
Last Updated: February 2026 | Next Scheduled Review: March 2026