What Is GIP? GIP Hormone Guide (Mounjaro, Zepbound)
Disclosure: Some links on this site are affiliate links. If you purchase through these links, we may earn a commission at no extra cost to you. Thank you for supporting our site. For informational purposes only—not medical advice.

On this page
Key Takeaway
GIP (glucose-dependent insulinotropic polypeptide) is a hormone your gut releases after eating. Its core job is to boost insulin secretion when blood sugar is elevated, helping your body handle the rise in glucose after a meal. GIP is one of two main incretin hormones (the other is GLP-1).
You've likely heard about GIP because tirzepatide—the active ingredient in Zepbound and Mounjaro—is a dual GIP + GLP-1 receptor agonist (it activates both receptors). The FDA labels describe tirzepatide as a "GIP receptor and GLP-1 receptor agonist." This dual-receptor design is one leading hypothesis for why tirzepatide can produce greater weight loss than GLP-1-only medications in head-to-head research. [1][2]
Already know what GIP is? Jump to GIP vs GLP-1 differences or learn how dual agonism works. Want the GLP-1 deep dive? See our complete guide on what GLP-1 is.
GIP at a Glance (Quick Answers Table)
| Question | Short Answer | Why It Matters |
|---|---|---|
| What is GIP? | A gut hormone released after eating that promotes insulin secretion in a glucose-dependent way. | Explains why GIP is called an incretin and why it's central to modern metabolic drugs. [3] |
| What does GIP stand for? | Glucose-dependent insulinotropic polypeptide (also historically called gastric inhibitory polypeptide). | Same hormone, two names—causes confusion online. [3] |
| Where is GIP made? | K cells in the upper small intestine (duodenum/proximal jejunum). | Location explains why it rises quickly after meals. [3][4] |
| How long does natural GIP last? | Only minutes—rapidly degraded (short half-life). | Explains why drugs are engineered to last longer. [3] |
| Is GIP a medication? | No—GIP is a natural hormone. Some medications target the GIP receptor (notably tirzepatide). | Helps you avoid "GIP supplement" scams. [1][2] |
| What is GIP in Zepbound/Mounjaro? | Tirzepatide activates both GIP and GLP-1 receptors (dual agonist). | The dual mechanism is the defining feature of tirzepatide. [1][2] |
| Are "GIP peptides" online legitimate? | Be extremely cautious. FDA and ADA warn about risks with non-FDA-approved products. | Safety, dosing, and sterility concerns are real. [5][6] |
If you only read one section: Read "Why dual GIP + GLP-1 agonists work better" and "Compounded/unapproved products warning."
What Is GIP in Plain English?
GIP is a "message" hormone released by your gut after you eat. When nutrients move from your stomach into your small intestine, gut cells release GIP into the bloodstream. GIP then signals your pancreas to release insulin only when glucose is elevated—helping your body manage post-meal blood sugar.
Because it increases insulin secretion in response to eating, GIP is classified as an incretin hormone. The other major incretin is GLP-1 (if you want the deep dive, see our dedicated What Is GLP-1 page). Together, incretin signaling accounts for a large portion of the insulin response after oral glucose in healthy physiology. [4]
Why the Name Is Confusing: "Gastric Inhibitory" vs "Glucose-Dependent Insulinotropic"
You'll see two names:
- Gastric inhibitory polypeptide (historical name)
- Glucose-dependent insulinotropic polypeptide (modern, function-based name)
They refer to the same hormone. The older name came from early observations of gastric effects; later work emphasized its major physiological role: glucose-dependent insulin release. [3]
Where Is GIP Made and What Triggers It?
Where GIP is produced
GIP is secreted by K cells in the proximal small intestine (duodenum and proximal jejunum). [3][4]
What triggers GIP release
GIP rises after meals. In human physiology, glucose and fat are major stimuli for GIP secretion. [4]
How long GIP lasts (and why that matters)
Natural GIP has a very short half-life (minutes). It's rapidly degraded by enzymes, which is one reason therapeutic molecules are engineered for longer action. [3]
Practical meaning: You can't "take GIP" like a vitamin and expect stable hormone signaling. Legitimate therapies that target incretin pathways are engineered drugs with defined dosing and safety profiles.
What Does GIP Do in the Body?
Most websites stop at "GIP stimulates insulin." That's true—but incomplete.
GIP receptors (GIPR) are present in multiple tissues, which is why GIP is now discussed as more than "just a pancreas hormone." Here's the clearest, evidence-based way to understand it.
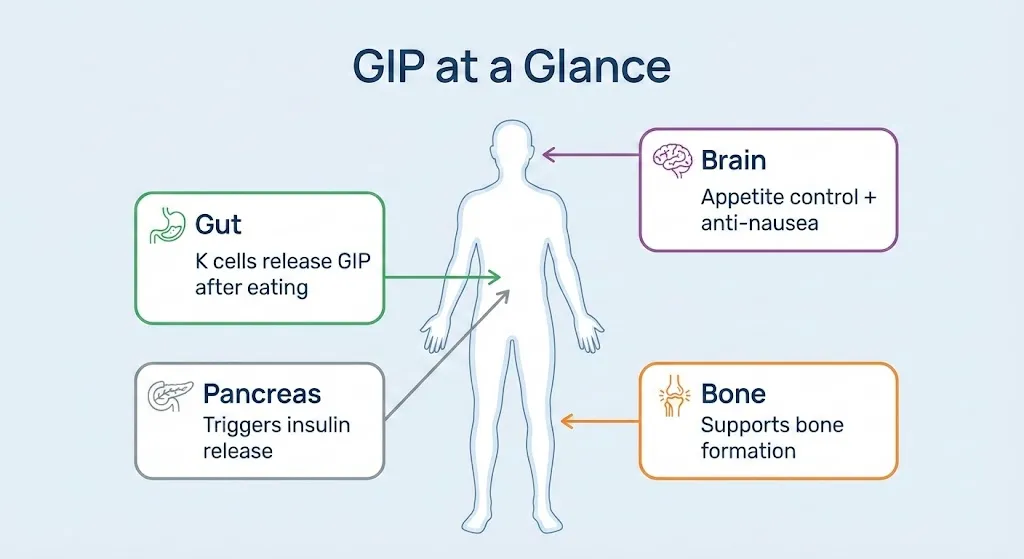
1) Pancreas: glucose-dependent insulin secretion (GIP's core job)
GIP's hallmark effect is to augment insulin secretion in a glucose-dependent manner—meaning GIP's insulin-stimulating effect is strongest when glucose is elevated. [3][4]
This glucose-dependence is important because it helps explain why incretin-based therapies generally have a lower risk of hypoglycemia when used alone (risk can change when combined with insulin or sulfonylureas—see safety section). [1][2]
2) The "GIP resistance" concept in type 2 diabetes
A key clinical observation: in type 2 diabetes, GIP levels can be normal or even increased, but the insulinotropic response to GIP is diminished—sometimes described as "GIP resistance," linked in part to downregulation of GIP receptors on beta cells. [4]
This is one reason GIP was once viewed as a less attractive drug target—until combination approaches demonstrated clinical effectiveness.
3) Adipose tissue: lipid handling, storage signals, and metabolic effects
GIP also acts on adipose tissue. Research supports a role for GIP in adipocyte metabolism and lipid handling. For example:
- In human adipocytes, GIP has been shown to increase lipoprotein lipase (LPL) expression and activity in experimental settings, supporting a plausible mechanism for post-meal lipid storage/processing signals. [8]
- Contemporary reviews describe that GIP biology in adipose tissue is complex, and both GIPR agonism and antagonism have been explored in different models for metabolic benefits. [9]
- A modern rationale paper on GIPR agonism proposes potential benefits of GIPR activation in adipose tissue related to lipid handling and insulin sensitivity pathways (while still acknowledging mechanistic complexity). [10]
The honest takeaway: GIP participates in post-meal nutrient handling (including fat metabolism signals). That does not mean "GIP equals fat gain." In humans, the metabolic story depends on context (energy balance, insulin levels, receptor biology, and drug design).
4) Bone: potential effects on bone remodeling
GIP has been investigated for effects on bone remodeling. For instance, research in primary human bone cells has reported that GIP can influence osteoclast and osteoblast biology (e.g., inhibiting bone resorption processes and supporting osteoblast survival in experimental models). [11]
Why you should care: Rapid weight loss can be associated with changes in bone density over time. Understanding whether GIP-targeting therapies have neutral, harmful, or protective bone effects is an active area of research.
5) Brain: appetite signaling and (preclinical) anti-nausea mechanisms
This is the piece that many "what is GIP" pages miss, and it's directly relevant to why dual agonists can feel different than GLP-1-only drugs.
- A preclinical study reported that GIP receptor signaling reduced nausea/vomiting-like responses induced by GLP-1 receptor activation, while preserving effects on food intake and weight in models used for emesis/illness behavior research. [12]
- A contemporary review summarizes proposed mechanisms where CNS GIPR agonism may attenuate nausea and suppress appetite, contributing to negative energy balance in multi-receptor approaches. [10]
Important reality check: The anti-nausea mechanism is supported by preclinical evidence and mechanistic hypotheses, and human experience varies. But it's a credible scientific thread that helps explain why "adding GIP" isn't just marketing—it changes the pharmacology.
The Incretin Effect: Why GIP Matters
If you want the simplest mental model for GIP, it's this:
Your body releases more insulin after you drink glucose than if the same glucose amount is infused into your bloodstream. That difference is the incretin effect.
A pharmacology review describes the incretin effect as accounting for at least ~50% of the insulin secreted after oral glucose in healthy subjects. [4]
Why this matters for "what is GIP?"
Because GIP is not "random." It's one of the main "gut → pancreas" signals that makes the incretin effect possible.
Key points from physiological reviews:
- GIP and GLP-1 are the two principal incretin hormones in humans. [4]
- In healthy individuals, both contribute significantly to the incretin effect after oral glucose (and the balance can vary by experimental conditions and meal composition). [4]
Why the incretin effect is reduced in type 2 diabetes
Reviews describe that in type 2 diabetes, the incretin effect is diminished. GIP secretion may be normal, but the beta-cell response to GIP is reduced (again, the "GIP resistance" concept). [4]
This sets up the modern era: drug designs that amplify incretin signaling—sometimes across multiple receptors—can improve glycemic control and support weight loss through central and peripheral mechanisms.
GIP vs GLP-1: The Key Differences
You already have a full GLP-1 guide, so this section stays focused on what's different about GIP and why the comparison matters.
Comprehensive comparison (includes the "missing" factors users search for)
| Feature | GIP | GLP-1 |
|---|---|---|
| Full name | Glucose-dependent insulinotropic polypeptide (also "gastric inhibitory polypeptide") [3] | Glucagon-like peptide-1 |
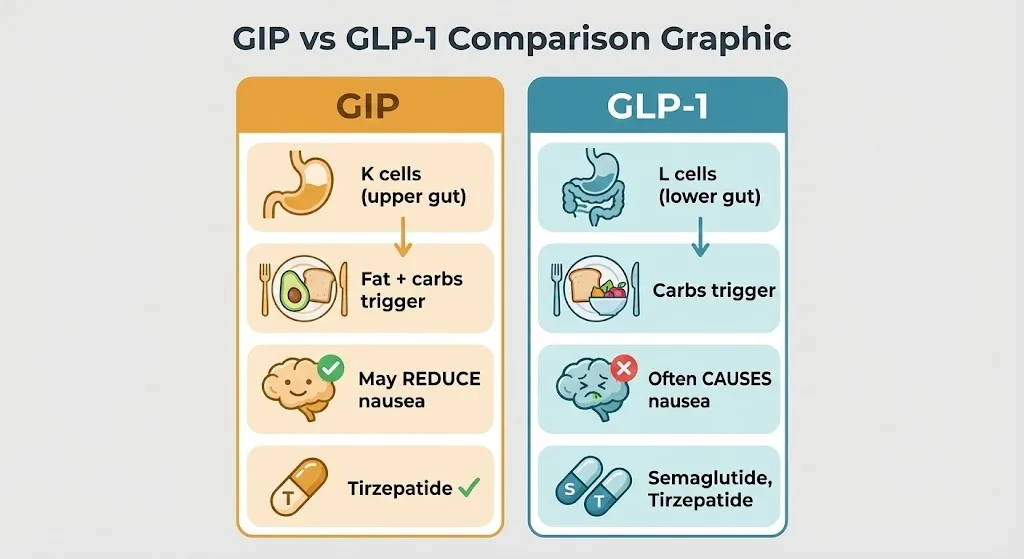
| Main source cells | K cells (upper small intestine) [3][4] | Primarily L cells (distal small intestine/colon) |
| Main meal triggers | Glucose + fat are strong stimuli [4] | Nutrient ingestion stimulates; often discussed in carb-related contexts |
| Primary pancreas effect | Increases insulin secretion (glucose-dependent) [3][4] | Increases insulin secretion (glucose-dependent) |
| Glucagon | Can influence glucagon depending on context; physiology is complex [4] | Typically suppresses glucagon when glucose is high (general physiology) |
| Gastric emptying | Not the primary hallmark | GLP-1 receptor agonism commonly slows gastric emptying (clinically relevant) |
| Appetite | Can participate in CNS regulation (emerging) [10] | Strong appetite suppression is a well-known GLP-1RA effect |
| Nausea profile (mechanistic) | Preclinical evidence suggests GIPR signaling may attenuate GLP-1-induced nausea/emesis [12]; hypothesis summarized in reviews [10] | Nausea is a common class effect for GLP-1 receptor agonists (see prescribing info for each drug) |
| In type 2 diabetes | GIP secretion may be normal but insulinotropic effect is reduced ("GIP resistance" concept) [4] | GLP-1 effect is relatively preserved vs GIP in T2D (physiology reviews) [4] |
| Approved medications that target it | Tirzepatide targets GIPR + GLP-1R [1][2] | Multiple GLP-1 receptor agonists (see our GLP-1 guide) |
The most important takeaway: Asking "GIP vs GLP-1—what's better?" is usually the wrong frame. Modern therapy design often tries to combine mechanisms to improve results and tolerability—especially in obesity and type 2 diabetes.
Why Dual GIP + GLP-1 Agonism Can Outperform GLP-1 Alone
This is the "why" behind the explosion of interest in GIP.
1) The simplest explanation
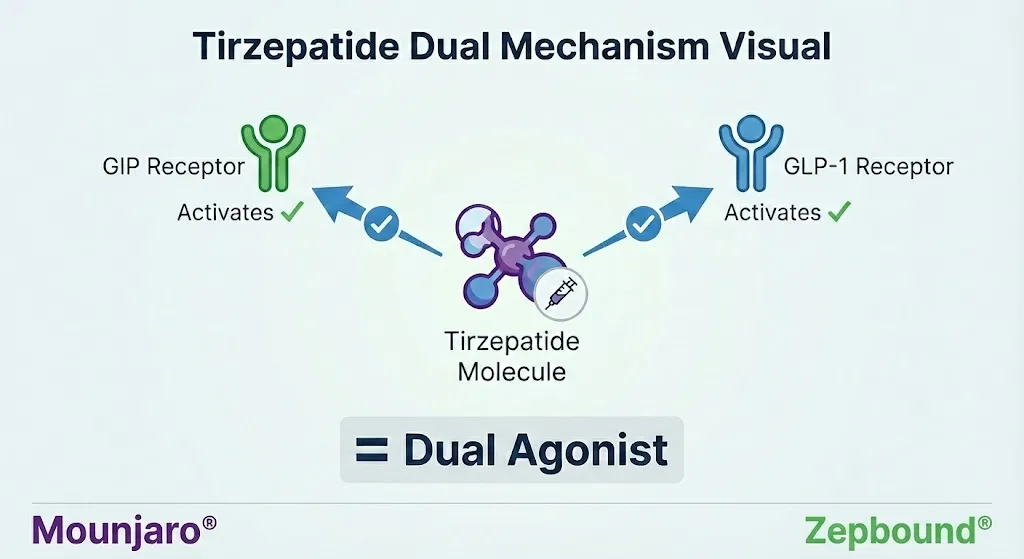
Dual agonists activate two distinct receptor systems that both participate in metabolic regulation. Tirzepatide is designed to activate GIPR and GLP-1R. [1][2]
2) What researchers think might be happening (mechanistic hypotheses)
A contemporary review summarizes several plausible contributions of GIPR agonism in weight management:
- In the CNS, GIPR agonism is implicated in appetite suppression and attenuation of nausea (helping sustain negative energy balance). [10]
- In adipose tissue, GIPR agonism may improve aspects of lipid handling and metabolic pathways related to insulin sensitivity in some models. [10]
Separate experimental work in human adipocytes provides mechanistic plausibility for GIP's adipose effects (e.g., LPL regulation in controlled settings). [8]
3) The evidence users actually want: head-to-head weight loss results
In the SURMOUNT-5 head-to-head trial (72 weeks), the least-squares mean percent change in weight was −20.2% with tirzepatide vs −13.7% with semaglutide. Waist circumference change was −18.4 cm vs −13.0 cm. [13]
How to interpret this responsibly:
- These are group averages in a controlled trial setting.
- Real-world outcomes depend on dose tolerance, adherence, access, diet/activity changes, comorbidities, and side effects.
- It does not mean one medication is "best" for every person; it means dual agonism can be clinically meaningful.
4) The "anti-nausea" angle: why this matters to real people
For many patients, nausea is the limiting factor that prevents reaching or staying on higher-dose GLP-1 therapy. Preclinical evidence suggests GIPR agonism can attenuate GLP-1-related nausea/emesis signals in models. [12] Reviews incorporate this as a plausible contributor to improved tolerability and sustained weight loss effects. [10]
Experiencing side effects on your GLP-1 medication? Try our GLP-1 SOS tool for immediate relief strategies, or check our guides for nausea relief and constipation help.
GIP in Tirzepatide: Zepbound, Mounjaro, and What the FDA Says
What is tirzepatide?
Tirzepatide is the active ingredient in:
- Zepbound (FDA-approved for chronic weight management and for moderate-to-severe obstructive sleep apnea in adults with obesity, as an adjunct to lifestyle measures) [1]
- Mounjaro (FDA-approved to improve glycemic control in adults and pediatric patients ≥10 years with type 2 diabetes, as an adjunct to diet and exercise) [2]
How the FDA describes its mechanism
Both FDA labels describe tirzepatide as a "GIP receptor and GLP-1 receptor agonist." [1][2]
That phrase matters because it's the cleanest, most authoritative explanation of "what is GIP in Zepbound/Mounjaro?":
- It means tirzepatide is designed to activate the GIP receptor (GIPR).
- It also activates the GLP-1 receptor (GLP-1R).
- Dual activation is central to its clinical effect profile.
What Zepbound is approved for (high level)
According to the FDA prescribing information, Zepbound is indicated:
- for chronic weight management in adults with obesity or overweight with at least one weight-related comorbid condition, as an adjunct to diet and increased physical activity, and
- to treat moderate to severe obstructive sleep apnea in adults with obesity. [1]
What Mounjaro is approved for (high level)
According to the FDA prescribing information, Mounjaro is indicated:
- to improve glycemic control in adults and pediatric patients 10 years and older with type 2 diabetes, as an adjunct to diet and exercise. [2]
What "dual agonist" does not mean
A common misconception: dual agonist does not mean "double dose GLP-1."
It means the medication activates two different receptors with distinct biology—GIPR and GLP-1R—by design. [1][2]
Want to compare tirzepatide vs semaglutide options? See our semaglutide vs tirzepatide comparison or find the best tirzepatide providers.
Safety, Side Effects, and Who Should Not Use Tirzepatide
For medications, the most authoritative sources are the FDA prescribing information and your clinician/pharmacist. This section summarizes key label information for education.
Boxed warning: thyroid C-cell tumors
Both Zepbound and Mounjaro carry a boxed warning about thyroid C-cell tumors in rodents; it's unknown whether this occurs in humans. The labels list contraindications in people with:
- personal or family history of medullary thyroid carcinoma (MTC), or
- Multiple Endocrine Neoplasia syndrome type 2 (MEN 2). [1][2]
Common side effects (what people actually experience)
Zepbound (weight management trials): The FDA label reports the following adverse reactions (≥2% and greater than placebo) in pooled placebo-controlled weight reduction trials, with dose-related patterns for several GI effects. Examples include nausea, diarrhea, vomiting, constipation, abdominal pain, dyspepsia, injection-site reactions, fatigue, and others. [1]
Example from the Zepbound label's pooled trials (Study 1 and Study 2):
| Side Effect | Placebo | Zepbound |
|---|---|---|
| Nausea | 8% | 25–29% |
| Diarrhea | 8% | 19–23% |
| Vomiting | 2% | 8–13% |
| Constipation | 5% | 11–17% |
(See full label for all listed reactions.) [1]
Mounjaro (type 2 diabetes trials): The label reports common adverse reactions (≥5% in pooled placebo-controlled adult trials) including nausea, diarrhea, decreased appetite, vomiting, constipation, dyspepsia, abdominal pain, with rates that vary by dose. [2]
Serious risks and precautions (high level)
FDA labeling includes warnings/precautions for topics such as:
- pancreatitis
- gallbladder disease
- kidney injury related to dehydration/volume depletion
- hypoglycemia risk when combined with insulin or sulfonylureas
- hypersensitivity reactions
- diabetic retinopathy complications in patients with a history of diabetic retinopathy (diabetes context)
- additional warnings described in labeling (read full prescribing information). [1][2]
Drug interactions: oral medications and oral contraceptives
Because tirzepatide delays gastric emptying, it may affect absorption of some oral medications. The Zepbound label specifically advises patients using oral hormonal contraceptives to switch to a non-oral method or add a barrier method for a period after initiation and after dose increases (see label for exact guidance and timing). [1]
Always confirm your specific situation with a clinician/pharmacist.
Who should not use these medications (contraindications)
Per FDA labels (not exhaustive):
- MTC personal/family history; MEN 2 [1][2]
- known serious hypersensitivity to tirzepatide or excipients [1][2]
Do not self-diagnose contraindications. A prescriber should evaluate risks and benefits for your health profile.
Compounded & Unapproved GIP/GLP-1 Products: FDA + ADA Warnings
This section exists because people searching "what is GIP" are often one click away from unsafe products marketed as "GIP peptide," "research tirzepatide," or "compounded tirzepatide."
FDA: concerns with unapproved GLP-1 drugs used for weight loss
The FDA has published warnings about unapproved GLP-1 drugs marketed for weight loss, including concerns such as:
- dosing errors and adverse events,
- products marketed as "for research use" or otherwise not approved,
- and issues around different forms (e.g., salt forms) and quality concerns in non-approved supply chains. [5]
ADA: recommendation against non-FDA-approved compounded incretin products
The American Diabetes Association states it recommends against using non-FDA-approved compounded GLP-1 receptor agonist products and compounded dual GIP/GLP-1 receptor agonist products, citing concerns about safety, quality, and effectiveness when products are not FDA-approved. [6]
Safety checklist: "legit" vs "high-risk"
High-risk red flags
- "No prescription required"
- Sold as "research peptide" for self-injection
- No licensed pharmacy involvement
- Vague labeling, unclear source, or "too cheap to be real"
- Claims "same as Zepbound/Mounjaro" without FDA approval or verified supply chain
- Pressure tactics (countdowns, "limited supply," "act now")
More legitimate signals (still verify)
- Prescription from a licensed clinician
- Dispensed by a licensed pharmacy
- Clear labeling and documentation
- Ability to answer sourcing and safety questions transparently
Bottom line: The only FDA-approved tirzepatide products are those in FDA labeling (see Zepbound and Mounjaro prescribing info). [1][2]
Decision Framework: Why Are You Searching "What Is GIP"?
Pick the path that matches your situation.
Path A — "I just want to understand the science"
You now have the correct mental model:
- GIP is a gut hormone released after meals.
- It increases insulin secretion in a glucose-dependent manner.
- It's one of the key incretin hormones that explains why the body responds differently to oral glucose vs IV glucose (incretin effect). [4]
Path B — "I saw GIP mentioned in Zepbound/Mounjaro"
Here's the clean answer:
- Tirzepatide is a dual GIPR + GLP-1R agonist (FDA label language). [1][2]
- Dual agonism is part of why tirzepatide can deliver strong outcomes in clinical trials relative to GLP-1-only approaches in head-to-head reporting. [13]
Path C — "I'm seeing 'GIP peptide' offers online"
Start with:
- FDA warnings about unapproved GLP-1 drugs used for weight loss. [5]
- ADA recommendation against non-FDA-approved compounded incretin products. [6]
Then talk to a licensed clinician/pharmacist before taking any action.
Path D — "I meant hospice GIP"
That's a different meaning (General Inpatient). See CMS hospice resources. [7]
Frequently Asked Questions
What is GIP in medical terms?
In medical terms, GIP refers to glucose-dependent insulinotropic polypeptide, a gut-derived hormone released after meals that augments insulin secretion in a glucose-dependent way. [3][4]
What does GIP stand for?
Glucose-dependent insulinotropic polypeptide. It's also historically called gastric inhibitory polypeptide—same hormone, different name. [3]
Is GIP a hormone?
Yes. GIP is a peptide hormone produced by intestinal K cells. [3][4]
Where is GIP produced?
GIP is produced by K cells in the upper small intestine (proximal small bowel). [3][4]
What triggers GIP release?
Meal nutrients—especially glucose and fat—stimulate GIP secretion from the gut. [4]
What does GIP do?
Its best-known role is to increase insulin secretion in a glucose-dependent manner. It also has roles in tissues like adipose and bone that are actively studied. [3][4][8][11]
What is the GIP receptor?
The GIP receptor (GIPR) is the receptor that binds GIP. Drugs like tirzepatide are designed to activate GIPR (and GLP-1R). [1][2]
Is GIP the same as GLP-1?
No. They're different hormones and bind different receptors. They're both incretins, but they have important differences in physiology and drug effects. [4]
What is the incretin effect?
The incretin effect is the increased insulin response after oral glucose compared with IV glucose, attributable to gut hormones. Reviews describe it as accounting for at least ~50% of insulin secreted after oral glucose in healthy subjects. [4]
What is GIP in Zepbound?
Zepbound contains tirzepatide, which the FDA describes as a "GIP receptor and GLP-1 receptor agonist." [1]
What is GIP in Mounjaro?
Mounjaro contains tirzepatide as well, and the FDA describes it as a "GIP receptor and GLP-1 receptor agonist." [2]
Are Zepbound and Mounjaro the same medication?
They contain the same active ingredient (tirzepatide), but have different FDA-approved indications and are marketed under different brands. [1][2]
Is tirzepatide "better" than semaglutide?
Head-to-head reporting and published records indicate tirzepatide has produced greater average weight loss than semaglutide in a comparative trial context, but "better" depends on individual factors (tolerability, contraindications, cost/coverage, comorbidities). [13]
Does GIP cause weight gain because it affects fat storage?
GIP participates in nutrient handling and adipose signaling; early biology led to concern about fat storage signals. However, modern drug development shows the story is complex: GIPR agonism and antagonism have both been explored, and multi-receptor strategies can drive weight loss. [9][10]
Do "GIP supplements" exist?
As a practical consumer category, "GIP supplements" are not a legitimate, evidence-based way to regulate GIP signaling. Be cautious of marketing that implies you can safely self-inject "GIP peptides" without FDA-approved labeling and clinical oversight. See FDA/ADA warnings for related concerns in the incretin space. [5][6]
What does GIP mean in hospice?
In hospice context, GIP often means General Inpatient level of hospice care—not the hormone. See CMS resources for hospice levels of care. [7]
What does GIP mean in finance?
In finance, GIP can mean Guaranteed Investment Product (varies by country and institution). That is unrelated to the hormone.
Glossary
- Agonist: A substance that activates a receptor.
- Incretin hormones: Gut hormones that increase insulin secretion in response to eating; the principal incretins are GIP and GLP-1. [4]
- Glucose-dependent: The effect (e.g., insulin secretion) is stronger when glucose is elevated; helps explain lower hypoglycemia risk when not combined with insulin-secretagogues. [4]
- K cells: Intestinal cells that secrete GIP. [3][4]
- GIPR: GIP receptor; drug targets like tirzepatide activate it. [1][2]
- Tirzepatide: Dual GIPR + GLP-1R agonist; active ingredient in Zepbound and Mounjaro. [1][2]
References
FDA / Government / Major Medical Organizations
- FDA Prescribing Information — Zepbound (tirzepatide). FDA AccessData label PDF (217806). FDA.gov
- FDA Prescribing Information — Mounjaro (tirzepatide). FDA AccessData label PDF (215866). FDA.gov
- NCBI Bookshelf / StatPearls — "Physiology, Incretins." National Center for Biotechnology Information. NCBI.gov
- Kim W, Egan JM. "The Role of Incretins in Glucose Homeostasis and Diabetes Treatment." Pharmacol Rev. 2008 (PMC). PMC2696340
- FDA — "Concerns with Unapproved GLP-1 Drugs Used for Weight Loss." FDA postmarket safety information page. FDA.gov
- American Diabetes Association — "Statement on Compounded Incretin Products." ADA press release/statement. Diabetes.org
- Centers for Medicare & Medicaid Services (CMS) — Hospice Benefits / Levels of Care. CMS.gov
Peer-Reviewed / Scientific Literature
- Kim SJ, et al. "GIP increases human adipocyte LPL expression…" J Lipid Res. 2010 (PMC). PMC2952555
- Kagdi S, et al. "The interplay of glucose-dependent insulinotropic polypeptide in adipose tissue." 2024 (PMC). PMC11103678
- Samms RJ, et al. "A Contemporary Rationale for Agonism of the GIP Receptor in the Treatment of Obesity." 2025 (PMC). PMC12278790
- Hansen S, et al. "GIP reduces osteoclast activity and improves osteoblast survival in primary human bone cells." Eur J Endocrinol. 2023. Oxford Academic
- Borner T, et al. "GIP receptor agonism attenuates GLP-1 receptor agonist-induced nausea and emesis in preclinical models." Diabetes. 2021 (PubMed record). PubMed 34326168
- Aronne LJ, et al. "Tirzepatide versus semaglutide for weight loss in adults with overweight or obesity (SURMOUNT-5): a randomised, head-to-head, double-blind, controlled trial." N Engl J Med. 2025. PubMed 40353578 | NEJM DOI
Update Log
January 12, 2026:
- Initial publication with verified FDA prescribing information for Zepbound and Mounjaro. [1][2]
- Verified FDA safety communication page on unapproved GLP-1 drugs. [5]
- Verified ADA statement on compounded incretin products. [6]
- Added adipose, bone, and CNS sections with peer-reviewed sources. [8][9][10][11][12]
- Added head-to-head trial references for tirzepatide vs semaglutide outcomes. [13]
Educational only. Not medical advice. If you think you might be a candidate for an incretin-based medication—or if you're considering any compounded/unapproved product—talk with a licensed clinician and pharmacist first.
How we rank + verify
Last verified: March 3, 2026
What we verified: FDA prescribing information for Zepbound and Mounjaro. Peer-reviewed studies from Pharmacological Reviews, NCBI, and clinical trial data.
Sources: FDA labels [1][2], FDA safety communications [5], ADA statements [6], peer-reviewed studies from NCBI [3][4][8][9][10][11][12], NEJM clinical trial [13]
Related Articles
This content is educational only and does not replace professional medical advice. Always consult a qualified healthcare provider before starting any medication.