Prior Authorization GLP-1: Requirements, Forms & Approval Checklist
Disclosure: Some links on this site are affiliate links. If you purchase through these links, we may earn a commission at no extra cost to you. Thank you for supporting our site. For informational purposes only—not medical advice.
On this page
On this page: Everything you need to get your GLP-1 medication approved—requirements, forms, checklists, denial fixes, and appeal templates. Use the checklists and templates below to build a complete PA packet and find your plan's specific criteria.
The Short Answer (Read This First)
If you're stuck waiting on prior authorization for a GLP-1 medication like Ozempic, Wegovy, Mounjaro, or Zepbound, here's what you need to know right now:
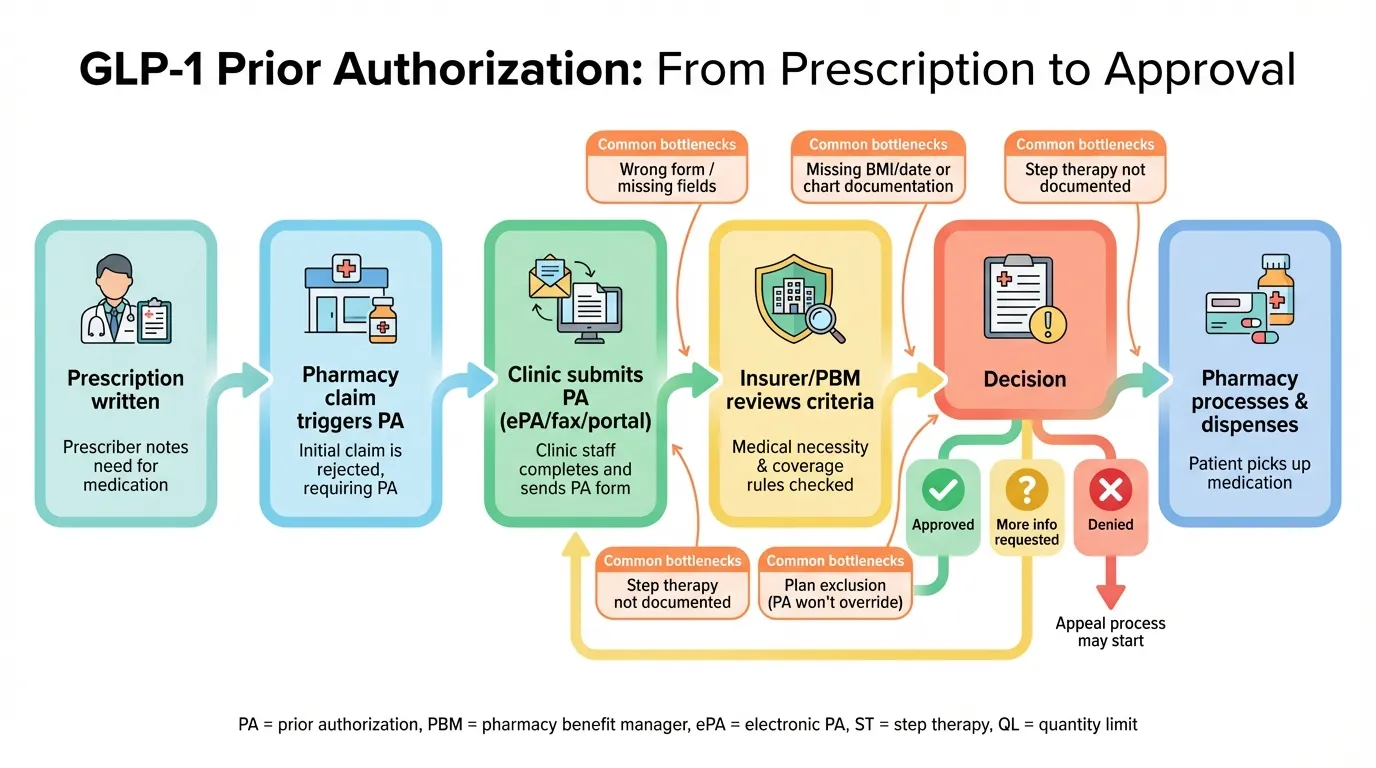
Answer: GLP-1 prior authorization is an insurer review that checks your diagnosis/indication (diabetes, obesity, CV risk reduction, OSA, MASH, etc.), BMI/comorbidities, step therapy history, and whether the request is fully documented. Most delays happen because the PA packet is missing BMI with a date, diagnosis documentation, or prior-treatment history—so the fastest path to approval is submitting those items together with correct diagnosis codes.
| What Insurers Check | Typical Requirement | Common Reason for Denial |
|---|---|---|
| BMI | ≥30, or ≥27 with a health condition | BMI not documented with date |
| Qualifying Health Conditions | Type 2 diabetes, high blood pressure, sleep apnea, heart disease | Comorbidity not in chart notes |
| Prior Treatment | 3–6 months of diet/exercise documentation | No proof of lifestyle attempt |
| Correct Diagnosis Code | ICD-10 matching the drug's approved use | Wrong code or missing code |
| Step Therapy | Trial of other medications first (varies by plan) | Prior meds not documented |
Most insurance plans will approve your GLP-1 prior authorization if you can document three things: (1) a qualifying diagnosis with the right BMI or health conditions, (2) evidence that you've tried lifestyle changes or other treatments first, and (3) complete paperwork with correct diagnosis codes. The process typically takes 5–10 business days when everything is submitted correctly.
The problem? Most requests get delayed or denied because of missing documentation—not because you don't qualify.
This guide exists to fix that. We'll show you exactly what your insurance company needs, help you gather the right paperwork before your appointment, and give you the tools to fight back if you're denied.
GLP-1 (also written GLP1 or GLP 1) medications include Ozempic, Wegovy, Mounjaro, Zepbound, Rybelsus, and Saxenda—all of which typically require prior authorization from insurers.
Do You Actually Need Prior Authorization?
Before we dive in, let's make sure prior authorization is actually what's blocking you.
Prior authorization (PA) is when your insurance company reviews your prescription before agreeing to cover it. For GLP-1 medications, this almost always happens because these drugs are expensive (often four-figure monthly retail prices) and insurers want documentation that you meet their criteria.
Here's the reality check:
You probably need PA if:
- Your pharmacy said "prior authorization required" when trying to fill your prescription
- Your insurance portal shows "PA" or "Prior Auth" next to GLP-1 medications on the formulary
- Your doctor's office said they need to submit paperwork to insurance
You might NOT need PA if:
- You're paying cash (no insurance involvement)
- You have a confirmed Type 2 diabetes diagnosis already on file with your insurer (some plans auto-approve for diabetes)
- Your employer plan has already pre-approved GLP-1 coverage
Important distinction: Prior authorization is different from a plan exclusion. If your plan specifically excludes weight-loss medications, a PA request won't override that—you'd need to request a formulary exception or explore other options (we cover those later in this guide).
Pick Your Situation: The 3 Paths to GLP-1 Approval
GLP-1 medications are FDA-approved for different uses, and your path to approval depends heavily on why you're taking the medication. Insurance companies care about this a lot.
Path A: GLP-1 for Type 2 Diabetes
Medications typically used: Ozempic, Mounjaro, Trulicity, Victoza, Rybelsus, Byetta
If you have Type 2 diabetes, you're on the most straightforward path. Most insurance plans cover GLP-1s for diabetes management, and many will auto-approve if your diabetes diagnosis is already in their system.
What insurers typically require:
- Confirmed Type 2 diabetes diagnosis (ICD-10 code E11.x)
- Plans often require recent diagnostic labs (e.g., A1C or fasting glucose) and documentation of the diabetes diagnosis; the exact thresholds are plan-specific and appear on the PA form
- Trial of metformin first (unless contraindicated)
- Sometimes: trial of a second oral diabetes medication
Pro tip: If you have Type 2 diabetes AND want weight loss benefits, getting approved through the diabetes pathway is usually easier. Ozempic and Mounjaro are approved for diabetes, and weight loss is a documented benefit—your doctor doesn't need to prescribe Wegovy or Zepbound specifically.
Path B: GLP-1 for Weight Management (No Diabetes)
Medications FDA-approved for weight loss: Wegovy, Zepbound, Saxenda
This path has more hoops to jump through. Insurers are stricter about weight-loss medications because (1) they're expensive, (2) many plans historically excluded weight-loss drugs, and (3) demand has exploded.
What insurers typically require:
- BMI ≥30, OR BMI ≥27 with at least one weight-related health condition
- Documentation of a supervised weight-loss attempt (usually 3–6 months)
- Proof of comorbidities if your BMI is between 27–30
- Often: trial of lifestyle modification program or another weight-loss approach first
The comorbidities that count:
- Hypertension (high blood pressure)
- Type 2 diabetes or pre-diabetes
- Dyslipidemia (high cholesterol/triglycerides)
- Obstructive sleep apnea
- Cardiovascular disease
- Osteoarthritis
- Fatty liver disease (NAFLD/NASH/MASH)
Reality check: If your employer plan or insurance specifically excludes "weight-loss drugs" or "anti-obesity medications," you may need to pursue a formulary exception—or explore alternatives. Check your Summary of Benefits and Coverage document, or call the number on your insurance card to confirm.
Path C: GLP-1 for Other FDA-Approved Uses
The FDA has approved some GLP-1 medications for uses beyond diabetes and weight loss. If one of these applies to you, your approval path may differ:
Cardiovascular Risk Reduction
- Wegovy is approved to reduce the risk of major cardiovascular events (heart attack, stroke) in adults with established cardiovascular disease who are overweight or obese (FDA label)
- This indication can sometimes provide an alternative coverage pathway
Obstructive Sleep Apnea (OSA)
- Zepbound is approved to treat moderate-to-severe obstructive sleep apnea in adults with obesity (FDA label)
- Requires documented OSA diagnosis (typically via sleep study)
MASH (Metabolic Dysfunction-Associated Steatohepatitis)
- Wegovy is FDA-approved (as of August 2025) to treat noncirrhotic MASH with moderate-to-advanced liver fibrosis (F2–F3) in adults with overweight or obesity (FDA label)
- This is a newer indication and coverage policies are still evolving
Why your indication matters: Insurance criteria often mirror the exact FDA indication language—so the documentation required for CV risk reduction, OSA, or MASH can look very different than obesity-only requests. If you request Wegovy but don't have documentation supporting one of its approved indications, you'll likely be denied—even if you'd clearly benefit from the medication.
What Is Prior Authorization—And Why Do GLP-1s Trigger It?
Let's make sure we're speaking the same language.
The Plain-English Definition
Prior authorization is your insurance company's way of saying: "Before we pay for this expensive medication, prove to us that you actually need it and meet our rules."
It's not a denial. It's a checkpoint. The insurance company reviews your medical records and decides whether to cover the drug based on their criteria.
For GLP-1 medications specifically, prior authorization exists because:
- These drugs are expensive. Many brand-name GLP-1s have four-figure monthly retail prices, which vary by dose, pharmacy, and discount programs. Insurers want to make sure they're not paying for medications that aren't medically necessary or won't be used correctly.
- Demand has exploded. GLP-1 prescriptions have increased dramatically since 2020, and insurers have tightened their approval processes in response.
- FDA-approved uses matter for coverage. A drug approved for diabetes may not be covered when prescribed "off-label" for weight loss, and vice versa.
- There are safety considerations. GLP-1s have contraindications and require appropriate patient selection.
Prior Auth vs. Step Therapy vs. Quantity Limits
These terms often get confused. Here's the difference:
| Term | What It Means | How It Blocks You | How to Resolve |
|---|---|---|---|
| Prior Authorization | Insurance reviews your case before approving | Prescription won't fill until approved | Submit required documentation |
| Step Therapy | Must try cheaper drugs first | Denied until you've tried (and failed) required drugs | Document prior med trials or get exception |
| Quantity Limit | Caps on how much you can fill | Pharmacy won't dispense more than allowed | May need PA for higher quantities |
| Formulary Exclusion | Drug isn't covered at all | Plan won't pay regardless of PA | Request formulary exception or pay cash |
Many GLP-1 prior authorizations involve multiple requirements—you might need to satisfy PA criteria AND complete step therapy AND stay within quantity limits. Understanding which barriers you're facing helps you address the right one.
GLP-1 Medications: Which Drug Is Which?
Before requesting prior authorization, make sure you're requesting the right medication for your situation. The most common PA denial that's entirely avoidable? Requesting a drug that doesn't match your insurance's coverage category.
The GLP-1 Medication Reference Table
| Brand Name | Active Ingredient | FDA-Approved For | Insurance Coverage Category | Typical PA Required? |
|---|---|---|---|---|
| Ozempic | Semaglutide (injection) | Type 2 Diabetes | Diabetes drugs | Yes, usually |
| Wegovy | Semaglutide (injection) | Chronic Weight Management, CV Risk Reduction, MASH (F2-F3) | Weight-loss drugs (if covered) | Yes, strict criteria |
| Rybelsus | Semaglutide (oral tablet) | Type 2 Diabetes | Diabetes drugs | Yes, usually |
| Mounjaro | Tirzepatide (injection) | Type 2 Diabetes | Diabetes drugs | Yes, usually |
| Zepbound | Tirzepatide (injection) | Chronic Weight Management, OSA | Weight-loss drugs (if covered) | Yes, strict criteria |
| Trulicity | Dulaglutide (injection) | Type 2 Diabetes | Diabetes drugs | Often, varies |
| Victoza | Liraglutide (injection) | Type 2 Diabetes | Diabetes drugs | Often, varies |
| Saxenda | Liraglutide (injection) | Chronic Weight Management | Weight-loss drugs (if covered) | Yes, strict criteria |
Note: A generic version of Saxenda (liraglutide injection for weight loss) received FDA approval in August 2025 (Source: Teva); availability and pricing vary by pharmacy and supply.
Key Things to Understand
Same ingredient, different drugs: Ozempic and Wegovy both contain semaglutide, but they're considered different products with different FDA approvals and different insurance coverage pathways. The same applies to Mounjaro and Zepbound (both tirzepatide).
"Off-label" prescribing is harder to get approved: If your doctor prescribes Ozempic for weight loss (not its FDA-approved use), your insurance may deny coverage because it's technically off-label. You'd need stronger clinical justification.
Check your plan's formulary first: Your insurance might cover Trulicity but not Ozempic, or Saxenda but not Wegovy. Knowing what's on your plan's preferred drug list can save you time.
The 6 Criteria Buckets: What Insurers Actually Check
This is where we get specific. Insurance companies evaluate GLP-1 prior authorization requests based on roughly six categories. Understanding these is how you make sure your request gets approved the first time.
Bucket 1: Correct Indication + Diagnosis Proof
What it means: Your documented diagnosis must match the drug's FDA-approved use.
What insurers look for:
- ICD-10 diagnosis code in your medical records
- Clinical notes supporting the diagnosis
- Match between the diagnosis and the requested medication
Diagnosis & Coding: What Insurers Usually Need Documented
| What to Document | What It Looks Like in Chart Notes (Example) | Why It Matters |
|---|---|---|
| Indication diagnosis | Type 2 diabetes (E11.x) | Matches diabetes-only GLP-1 coverage pathways |
| Obesity severity | Obesity diagnosis (code varies by class/plan) + BMI value | Many obesity criteria are BMI-threshold based |
| BMI (value + date) | "BMI 33.4 on 01/28/2026" | Denials often happen when BMI or date is missing |
| Comorbidities | Hypertension, dyslipidemia, OSA, etc. | Needed when BMI is 27–29.9 and plan requires comorbidity |
| "Current use" add-on codes (provider-only) | e.g., Z79.85 can be used for injectable non-insulin antidiabetic drugs | Sometimes helps claims logic / continuity of care |
Important note: Coding is done by clinicians and coders, and requirements vary by payer. New obesity class codes (E66.811, E66.812, E66.813 for Class 1, 2, and 3 obesity) became effective October 2024 (Source: CDC ICD-10-CM update). Don't attempt to self-code—use this information only to understand what documentation your plan may be looking for.
Why requests get denied here:
- Wrong diagnosis code (e.g., requesting weight-loss drug with only diabetes code)
- No diagnosis code included at all
- Diagnosis not documented in recent chart notes
How to avoid this: Make sure your doctor's chart notes from your most recent visit include your diagnosis AND the corresponding ICD-10 code. If you're requesting a weight-loss medication, your BMI and any comorbidities need to be explicitly documented.
Bucket 2: BMI and Weight-Related Comorbidities
What it means: For weight-management medications, insurers require proof that your BMI meets their threshold, and documentation of any qualifying health conditions.
Standard BMI requirements (these vary by plan):
- BMI ≥30 (obesity) — usually qualifies on its own
- BMI ≥27 (overweight) + at least one weight-related comorbidity
- Some stricter plans require BMI ≥35 or even ≥40
What needs to be documented:
- Your weight (in pounds or kg)
- Your height
- The date the measurement was taken
- Calculated BMI
- Any qualifying comorbidities with their own diagnosis codes
Qualifying comorbidities typically include:
- Type 2 diabetes or pre-diabetes
- High blood pressure (hypertension)
- High cholesterol/triglycerides (dyslipidemia)
- Obstructive sleep apnea (requires sleep study)
- Cardiovascular disease
- Joint problems related to weight (osteoarthritis)
- Fatty liver disease (NAFLD/NASH/MASH)
- Polycystic ovary syndrome (PCOS)
Why requests get denied here:
- BMI documented but without a date
- Weight from a year ago (insurers want recent measurements)
- Comorbidities mentioned but not coded in chart notes
- BMI just under the threshold (e.g., 29.8 when plan requires 30)
How to avoid this: At your appointment, ask your doctor to document your current weight, height, BMI, and the date measured. If you have any of the comorbidities listed above, make sure they're noted with their ICD-10 codes.
Bucket 3: Step Therapy / Prior Medications Tried
What it means: Many insurance plans require you to try (and fail) other treatments before approving a GLP-1.
For Type 2 Diabetes path:
- Almost always: metformin trial first
- Often: second oral diabetes medication (sulfonylurea, SGLT2 inhibitor, etc.)
- Exception: documented intolerance or contraindication to metformin
For Weight Management path:
- Usually: documented lifestyle modification attempt (diet + exercise)
- Sometimes: trial of other weight-loss medications (Contrave, Qsymia, phentermine)
- Exception: documented contraindication or prior failure
What counts as "tried and failed"?
- Inadequate response (didn't achieve target A1C or weight loss goal)
- Intolerable side effects (documented in chart notes)
- Contraindication (e.g., metformin + kidney disease)
Why requests get denied here:
- No documentation of prior treatments
- Patient says they tried medications, but no records
- Lifestyle modification not documented by a healthcare provider
How to avoid this: Bring records of any medications you've tried for diabetes or weight loss, including why they didn't work. If you've worked with a dietitian, weight-loss program, or exercise program, bring documentation.
Bucket 4: Lifestyle Program / Weight History Evidence
What it means: For weight-loss indications, insurers want proof that you've attempted non-medication approaches to weight management.
What typically counts as documentation:
- Records from a physician-supervised weight loss program
- Visits with a registered dietitian
- Enrollment in a structured weight-loss program (with dates)
- Weight history showing attempts at weight management
- Exercise program documentation
- Food logs or diet records (sometimes)
Time requirements vary:
- Some plans require 3 months of documented lifestyle modification
- Others require 6 months
- Some accept any evidence of prior attempt
- A few plans waive this if BMI is extremely high (≥40)
Why requests get denied here:
- "I tried dieting" without any documentation
- Weight-loss program enrollment but no visit records
- Lifestyle attempts not documented by a healthcare provider
How to avoid this: If you've participated in any structured weight-loss program, get documentation. Even visits with your primary care doctor where you discussed diet and exercise can count—ask for those chart notes. Some patients work with a dietitian for 2–3 visits specifically to create this documentation.
Bucket 5: Safety Screening / Contraindications
What it means: GLP-1 medications have specific contraindications, and insurers may check that appropriate safety screening was done.
Key safety considerations:
FDA labels list specific contraindications, including:
- Personal or family history of medullary thyroid carcinoma (MTC)
- Multiple Endocrine Neoplasia syndrome type 2 (MEN 2)
- Serious hypersensitivity to the drug or its components
FDA labels also include warnings and precautions that may require clinician screening, such as:
- History of pancreatitis
- Gallbladder disease
- Severe gastrointestinal issues
- Pregnancy or planned pregnancy considerations (handled clinically)
What insurers may check:
- Thyroid history documented
- No contraindications noted in chart
- Appropriate patient selection documented
This bucket rarely causes denials unless there's a clear contraindication in your records. It's more of a safety checkbox on the PA form.
Bucket 6: Dose, Quantity, and Refill Rules
What it means: Even with PA approval, insurers may limit how much medication you can get and how often.
Common restrictions:
- Quantity limits per 30-day fill
- Dose escalation schedules (can't jump straight to highest dose)
- Refill timing restrictions (no early refills)
- Step-up requirements (start at low dose, increase gradually)
Why requests get denied here:
- Requested dose is higher than what plan allows initially
- Quantity requested exceeds plan's limit
- Refill attempted too early
How to avoid this: Make sure your prescribed dose matches your plan's allowed starting dose. If your doctor wants to start you at a higher dose, they may need additional justification.
What to Gather Before Your Appointment: Patient Checklist
The most important thing you can do to get your GLP-1 approved? Show up prepared. Your doctor can only document what they have access to, and you have more control over this than you think.
The 15-Minute Document Checklist
Gather these before your appointment:
Insurance Information
- Insurance card (front and back)
- RxBIN and RxPCN numbers (usually on the card)
- Member ID number
- Phone number for pharmacy benefits (for your doctor's office to call)
Weight History
- Weight measurements from the past 6–12 months (dates + weights)
- If you've tracked your weight at home, bring the records
- Any records from previous doctor visits showing weight over time
Medical Records
- List of your current health conditions (with diagnosis dates if you know them)
- List of all current medications (names + doses)
- Any recent lab results (A1C, cholesterol, blood pressure readings)
- Records of past weight-loss attempts or programs
Medication History
- List of medications you've tried for weight loss or diabetes
- Why they didn't work (side effects, didn't help, etc.)
- Photos of medication bottles if you don't remember exact names
Lifestyle Documentation
- Receipts/records from weight-loss programs, gym memberships, dietitian visits
- Food or exercise logs if you've kept them
- Documentation from any structured program (Weight Watchers, Noom, etc.)
Why this matters: Your doctor's prior authorization submission is only as strong as the documentation they have. If you walk in with your weight history, medication list, and proof of lifestyle attempts, you make it easy for them to check all the boxes insurers want.
What Your Doctor's Office Needs: Provider Checklist
If you're a provider (or a patient who wants to help their doctor's office), here's what needs to be in the prior authorization submission.
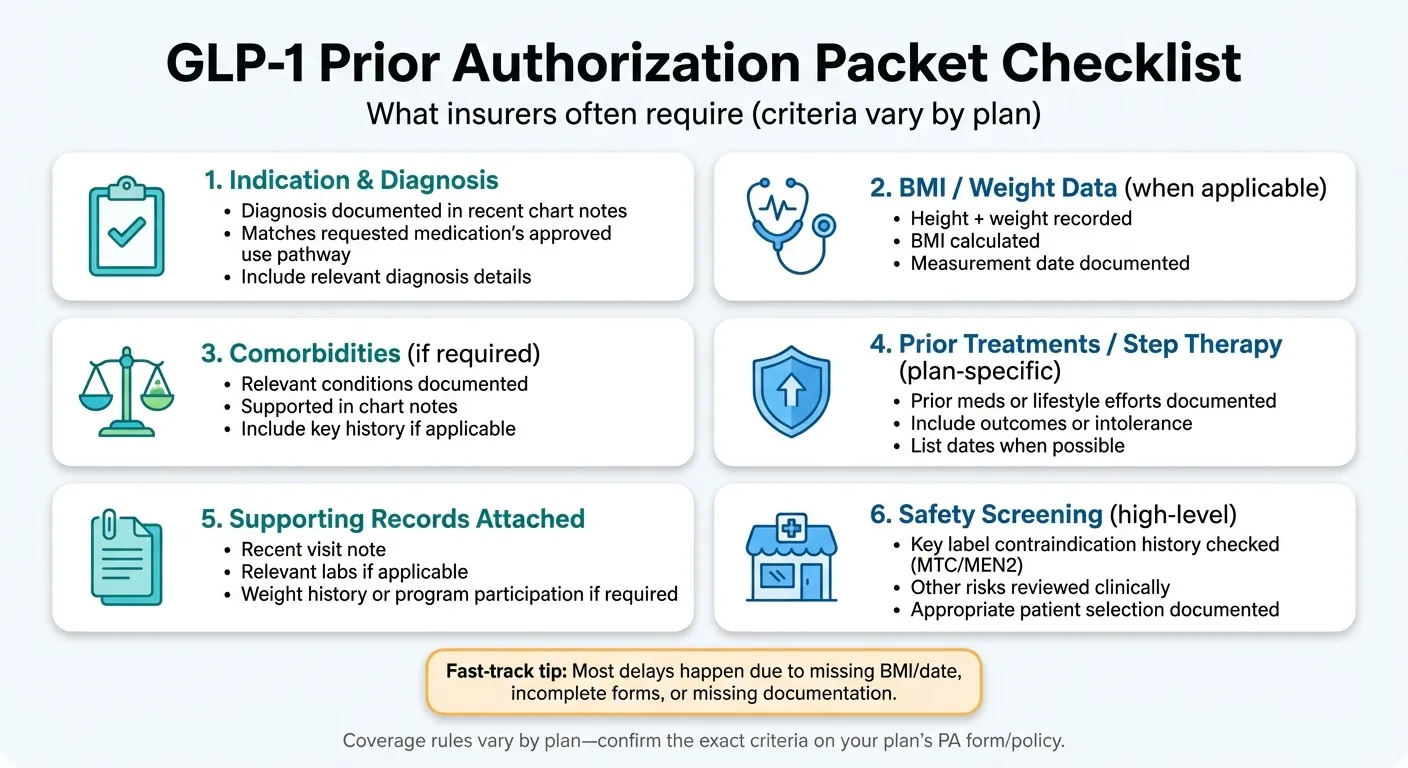
The Complete PA Submission Package
Required Components:
-
Completed Prior Authorization Form
- Use the correct form for the patient's specific insurance/PBM
- Fill out all required fields (incomplete forms = automatic denial)
- Include prescriber NPI and contact information
-
Chart Notes from Recent Visit
- Date of visit
- Current weight, height, calculated BMI (with date)
- Documented diagnosis with ICD-10 codes
- Any relevant comorbidities with their codes
- Statement of medical necessity
-
Letter of Medical Necessity (if required or if criteria are borderline)
- Explain why this specific medication is needed
- Document prior treatments tried and why they failed
- Connect the patient's clinical picture to the drug's indication
-
Supporting Documentation
- Recent lab results (A1C for diabetes, lipid panel, etc.)
- Weight history (multiple data points)
- Records from lifestyle programs or dietitian visits
- Previous medication records
-
Correct Diagnosis Codes
- Primary diagnosis matching the drug's indication
- Secondary diagnoses for comorbidities
- BMI code if applicable
Sample Letter of Medical Necessity Template
Providers can customize this template for their patients:
[Practice Letterhead]
Date: [Insert Date]
Re: Prior Authorization Request for [Drug Name] Patient: [Patient Name] DOB: [Date of Birth] Member ID: [Insurance Member ID]
To Whom It May Concern:
I am writing to request prior authorization for [Drug Name] for my patient [Patient Name], who has been under my care since [Date].
Diagnosis: [ICD-10 Code] - [Diagnosis Description]
Clinical Summary:
- Current BMI: [Value] (measured [Date])
- Current weight: [Value] lbs/kg
- Relevant comorbidities: [List with ICD-10 codes]
- Duration of condition: [Timeframe]
Prior Treatment History: [Patient Name] has previously attempted the following treatments with inadequate response:
- [Medication/Treatment 1]: [Outcome/reason for discontinuation]
- [Medication/Treatment 2]: [Outcome/reason for discontinuation]
- Lifestyle modification: [Details of diet/exercise attempts]
Medical Necessity: [Drug Name] is medically necessary for this patient because [specific clinical rationale]. The patient meets FDA labeling criteria for this indication, and alternative treatments have been insufficient to achieve treatment goals.
Supporting Documentation Enclosed:
- Recent chart notes
- Laboratory results dated [Date]
- Weight history documentation
- [Other relevant records]
Please contact my office at [Phone Number] with any questions regarding this request.
Sincerely,
[Provider Signature] [Provider Name, Credentials] [NPI Number]
Electronic PA (ePA) vs. Traditional Submission
Most insurance plans now accept electronic prior authorization through platforms like CoverMyMeds, SureScripts, or their own portals.
Advantages of ePA:
- Faster processing (sometimes same-day)
- Fewer errors from missing fields
- Real-time status tracking
- Automatic form selection
When traditional fax/portal may be needed:
- Complex cases requiring extensive documentation
- Plans that don't support ePA for certain drugs
- Appeals or resubmissions with additional information
Find Your Plan's GLP-1 Criteria and PA Form
This is where most people get stuck: finding the actual requirements and forms for their specific insurance plan.
Step 1: Identify Your PBM (Pharmacy Benefit Manager)
Your PBM processes your prescription benefits and sets the prior authorization rules. Look at your insurance card for one of these names:
- CVS Caremark (often shows "CVS" or "Caremark")
- Express Scripts (often shows "ESI" or "Express Scripts")
- OptumRx (often shows "Optum" or "UHC")
- Prime Therapeutics (often shows "Prime")
- Cigna (may process their own or use Express Scripts)
- Humana Pharmacy (may process their own)
Can't find it? Call the number on the back of your insurance card and ask: "Who is my pharmacy benefit manager for prescription coverage?"
Step 2: Access Formulary and PA Criteria
Once you know your PBM, you can look up whether GLP-1 medications require prior authorization and what the specific criteria are.
Where to Find PA Criteria by Major PBM:
| PBM/Insurer | Find Criteria | Find PA Forms | Last Verified |
|---|---|---|---|
| CVS Caremark | Caremark.com → Formulary Lookup | Caremark.com → Prior Auth Forms | Jan 2026 |
| Express Scripts | Express-Scripts.com → Drug Lookup | Express-Scripts.com → Forms | Jan 2026 |
| OptumRx | OptumRx.com → Formulary | OptumRx.com → Prior Auth | Jan 2026 |
| Cigna | Cigna.com → Drug Coverage | Cigna.com → Forms Library | Jan 2026 |
| Aetna | Aetna.com → Pharmacy | Aetna.com → Clinical Forms | Jan 2026 |
| UnitedHealthcare | UHC.com → Pharmacy Benefits | Via OptumRx or UHC Portal | Jan 2026 |
| Humana | Humana.com → Pharmacy | Humana.com → Prior Auth | Jan 2026 |
| Blue Cross Blue Shield | Varies by state—check your state's BCBS website | Varies by state | Jan 2026 |
| Medicare Part D | Check your specific Part D plan's formulary | Through plan's website | Jan 2026 |
| Medicaid | Varies by state—search "[State] Medicaid formulary" | State-specific | Jan 2026 |
| TRICARE | Tricare.mil → Pharmacy | Express Scripts (TRICARE) | Jan 2026 |
Note: Always call the number on your insurance card for the most current information. Policies and forms can change.
Step 3: Check Coverage Status Before Requesting
Before your doctor submits the PA request, it helps to know:
-
Is the drug on your formulary at all?
- Look up the specific drug (Ozempic, Wegovy, etc.)
- Check what tier it's on (Tier 4+ usually means higher cost)
-
What utilization management applies?
- PA = Prior Authorization required
- ST = Step Therapy required
- QL = Quantity Limits apply
-
Are weight-loss drugs excluded?
- Some plans exclude all anti-obesity medications
- Look for exclusions in your Summary of Benefits
Pro tip: If you call your insurance before the PA is submitted, ask: "What are the specific criteria for prior authorization approval for [Drug Name]?" They're required to tell you.
How Long Does GLP-1 Prior Authorization Take?
The honest answer: it depends on how complete your submission is.
Typical Timelines
| Scenario | Expected Timeline |
|---|---|
| Complete ePA submission, clear approval criteria met | 24–72 hours |
| Complete fax/portal submission, straightforward case | 5–7 business days |
| Standard submission with typical review | 5–10 business days |
| Missing documentation (insurer requests more info) | +7–14 additional days |
| Denial + appeal process | 30–60+ additional days |
What Slows Things Down
- Incomplete forms — Missing fields mean the request sits in a queue for follow-up
- Missing documentation — Insurer sends request back for more info
- Wrong form used — Some plans have drug-specific PA forms
- High volume periods — January (new plan year) is especially busy
- Manual review required — Complex cases take longer than auto-approvals
How to Track Your PA Status
Ask your doctor's office:
- "Has the PA been submitted?"
- "What date was it submitted?"
- "Have you received any response or request for additional info?"
Ask your insurance:
- Call the pharmacy benefits number on your card
- Ask: "What is the status of the prior authorization for [Drug Name] for [Your Name]?"
- Get a reference number for the request
Ask your pharmacy:
- They can often see if a PA is pending or approved
- They may be able to run a test claim to check status
Expedited/Urgent Requests
In some situations, you can request expedited review (24–72 hours instead of 5–10 days):
- Medical urgency (e.g., uncontrolled diabetes with complications)
- Risk of harm if medication is delayed
- Inpatient to outpatient transition
Your doctor needs to specifically request urgent/expedited review and provide justification. Not all cases qualify.
How Long Does GLP-1 Prior Authorization Last (and What You Need to Renew)?
This is one of the most common questions people forget to ask—until their approval suddenly expires.
Typical Approval Durations
Most GLP-1 prior authorizations are approved for a set period, after which you'll need reauthorization:
| Plan Type | Typical Approval Duration |
|---|---|
| Commercial plans | 6–12 months |
| Medicare Part D | Varies by plan (often 12 months) |
| Medicaid | Varies by state (often 6–12 months) |
For example, some UnitedHealthcare commercial policies issue GLP-1 authorizations for up to 12 months before requiring renewal.
What You Need for Reauthorization
When your PA is up for renewal, insurers typically want to see:
For Weight Management GLP-1s:
- Updated weight and BMI (showing treatment response)
- Continued documentation of lifestyle program participation
- Evidence of "positive clinical response" (weight loss maintained)
- Confirmation you're still taking the medication as prescribed
For Diabetes GLP-1s:
- Updated A1C or other diabetes labs
- Continued use documentation
- No contraindications developed
Renewal Checklist
To avoid gaps in coverage when your PA expires:
- Know when your current PA expires (ask your doctor's office or insurance)
- Schedule a follow-up visit 4–6 weeks before expiration
- Have updated weight/BMI documented at that visit
- Bring any lifestyle program documentation from the approval period
- Make sure your doctor's office submits the renewal PA before expiration
Pro tip: Don't wait until you're out of medication. Start the reauthorization process at least 30 days before your current approval expires.
Common Denial Reasons (And the Exact Fix for Each)
If you've been denied, don't panic. Many GLP-1 prior authorization denials are overturned when the right information is provided.
The Denial → Fix Table
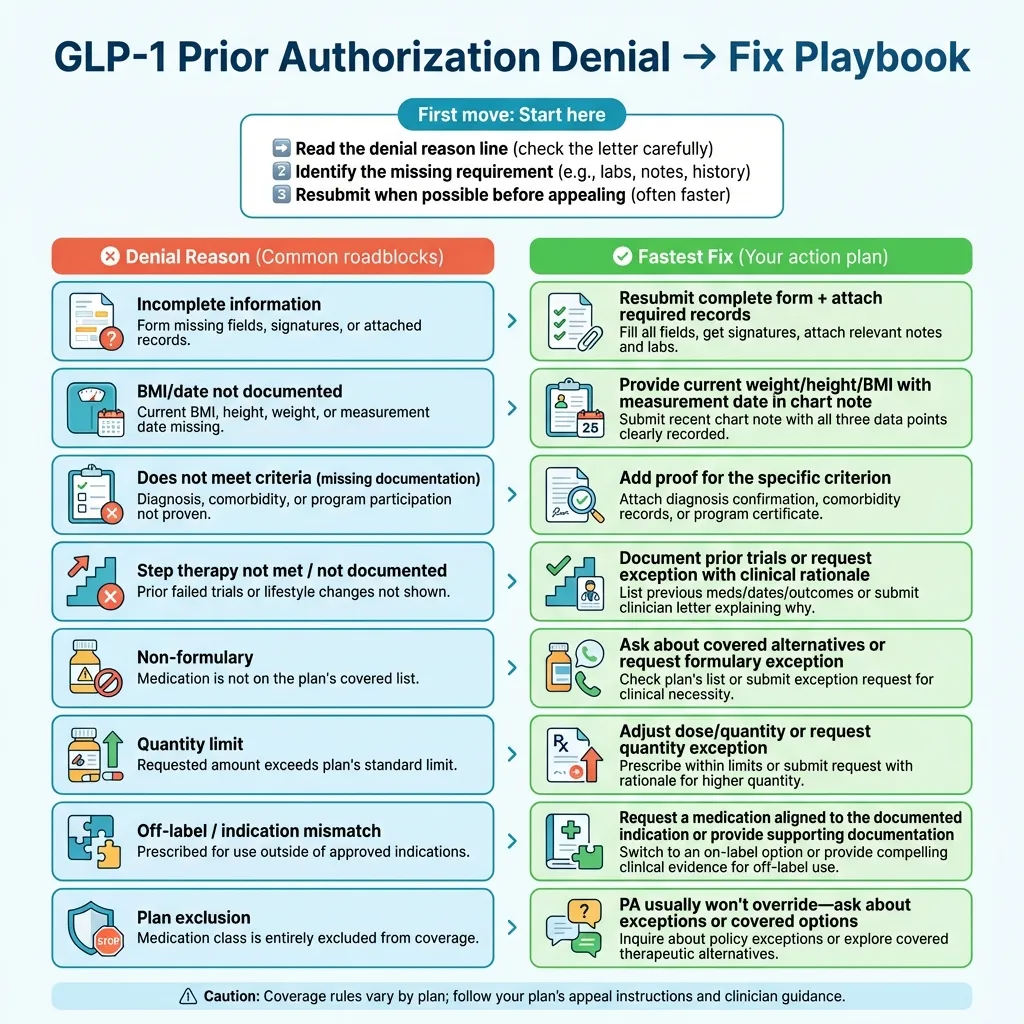
| Denial Reason | What It Really Means | The Fix |
|---|---|---|
| "Does not meet criteria" | Missing BMI documentation, comorbidity proof, or diagnosis code | Resubmit with explicit documentation of BMI + date, qualifying health conditions with ICD-10 codes |
| "Step therapy not met" | Plan requires trial of other medications first | Document prior medication trials (what you tried, why it didn't work) OR get step therapy exception |
| "Prior authorization not obtained" | PA was required but not submitted before filling | Submit PA now; request retroactive review if medication was already dispensed |
| "Non-formulary" | Drug isn't on your plan's covered drug list | Request formulary exception OR switch to covered alternative |
| "Plan exclusion" | Your plan specifically excludes this drug category | Request formulary exception (may be difficult) OR explore alternatives |
| "Incomplete information" | PA form was missing required information | Resubmit complete form with all documentation |
| "Medical necessity not established" | Insurer doesn't see enough clinical justification | Provide detailed letter of medical necessity with supporting records |
| "Quantity limit exceeded" | Requested amount exceeds plan's allowed quantity | Request quantity limit exception OR adjust prescription to match limits |
| "Off-label use" | Drug requested for a use not matching FDA approval | Provide strong clinical rationale OR request drug approved for your indication |
| "Documentation not current" | Records provided are too old | Provide recent documentation (within 3–6 months typically) |
How to Read Your Denial Letter
Your denial letter should include:
- The specific reason for denial — Look for the exact criteria that wasn't met
- What would be needed for approval — Sometimes explicitly stated
- Appeal deadline — Usually 30–60 days from denial date
- Appeal instructions — How to submit an appeal
- External review rights — Your right to an independent review
Save this letter. You'll need it for your appeal.
If You Were Denied: The Step-by-Step Appeals Process
Getting denied doesn't mean it's over. In fact, many denials are reversed on appeal when better documentation is provided.
The Appeals Ladder
Level 1: Correct and Resubmit (Fastest)
If the denial was due to missing information or clerical issues:
- Don't appeal—just resubmit with the missing documentation
- This is faster than a formal appeal
Level 2: Internal Appeal / Reconsideration
If you believe you meet criteria but were incorrectly denied:
- Submit a written appeal within the deadline (usually 30–60 days)
- Include new or additional documentation addressing the denial reason
- Reference specific criteria from your plan that you meet
Level 3: Peer-to-Peer Review
Your doctor can request to speak directly with the insurance company's medical director:
- Often available before or during the appeal process
- Allows your doctor to explain the clinical rationale verbally
- Can be very effective for borderline cases
Level 4: External Review
If internal appeals are exhausted:
- You have the right to an independent external review
- An outside organization reviews your case
- Binding on the insurance company in many states
- Usually free to the patient
What to Include in Your Appeal
-
Appeal cover letter stating:
- Patient name, DOB, member ID
- Drug being requested
- Reference to the denial (date, reference number if available)
- Specific reasons why the denial was incorrect
- What documentation is enclosed
-
Point-by-point response to the denial reason:
- If they said "BMI not documented" → include current BMI with date
- If they said "step therapy not met" → document prior medication trials
- If they said "no comorbidity" → provide diagnosis codes and records
-
Updated documentation that addresses the gap:
- Recent chart notes
- Lab results
- Weight history
- Records from lifestyle programs
-
Letter of medical necessity from your doctor (if not previously included)
-
Supporting clinical literature (optional but helpful for complex cases):
- FDA labeling
- Clinical guidelines supporting the treatment
Sample Appeal Letter Template
[Your Name] [Your Address] [Date]
[Insurance Company Name] [Appeals Department Address]
Re: Appeal of Prior Authorization Denial Patient Name: [Your Name] Date of Birth: [Your DOB] Member ID: [Your Member ID] Drug: [Medication Name] Denial Date: [Date of Denial] Denial Reference #: [If available]
Dear Appeals Review Board:
I am writing to appeal the denial of prior authorization for [Drug Name], which was denied on [Date] due to [stated denial reason].
I respectfully disagree with this determination for the following reasons:
[Address each denial reason specifically]
- Regarding [denial reason 1]: [Explain why this is incorrect and what documentation proves it]
- Regarding [denial reason 2]: [Explain why this is incorrect and what documentation proves it]
Enclosed Documentation:
- [List all documents you're including]
- [Recent chart notes dated X]
- [Lab results dated X]
- [Letter of medical necessity from Dr. X]
- [Weight history documentation]
Based on the above, I meet the criteria for coverage of [Drug Name] as specified in your formulary/coverage policy. I request that this denial be reversed.
Please contact me at [phone number] or [email] if additional information is needed.
Sincerely,
[Your Signature] [Your Printed Name]
Timeline for Appeals
| Appeal Type | Typical Timeline |
|---|---|
| Standard internal appeal | 30 days for decision |
| Expedited appeal (urgent cases) | 72 hours for decision |
| External review | Varies by state, typically 45–60 days |
Medicare, Medicaid, and Special Cases
Some insurance situations have unique rules for GLP-1 coverage. Here's what you need to know.
Medicare Part D: The Key Rule Everyone Misunderstands
The important distinction: Medicare Part D CAN cover GLP-1 medications—but with significant restrictions on weight-loss drugs specifically.
What's covered:
- GLP-1s for Type 2 diabetes (Ozempic, Mounjaro, Trulicity, etc.) — generally covered with PA
- GLP-1s for cardiovascular risk reduction in patients with established heart disease (Wegovy) — coverage after CMS guidance opened the door, but varies by plan (Source: KFF)
What's historically NOT covered:
- GLP-1s solely for weight loss/obesity — Medicare is generally prohibited from covering drugs used solely for weight loss by statute (Source: Congressional Budget Office)
What's changing:
- Semaglutide products (Ozempic, Rybelsus, Wegovy) were selected for Medicare drug price negotiation with negotiated prices taking effect in 2027 (Source: CMS)
- CMS has launched the BALANCE model designed to expand access to anti-obesity medications in Medicare Part D for participating plans starting in 2027
- Coverage rules continue to evolve
If you have Medicare:
- Check your specific Part D plan's formulary for the drug you want
- Call your plan to understand what indications are covered
- If you have diabetes AND want weight loss benefits, the diabetes pathway may be easier
- Consider Medicare Advantage plans during open enrollment if weight-loss coverage is important to you
Medicaid: State-by-State Reality
Medicaid coverage for GLP-1s varies dramatically by state.
General patterns:
- Most state Medicaid programs cover GLP-1s for Type 2 diabetes (with PA)
- As of January 2026, KFF reports 13 state Medicaid programs cover GLP-1s for obesity treatment under fee-for-service—managed care coverage may differ (Source: KFF)
- CMS has launched the BALANCE model to expand Medicaid access to anti-obesity medications for participating states beginning in May 2026
- Coverage criteria and PA requirements differ by state
How to find your state's Medicaid coverage:
- Search: "[Your State] Medicaid pharmacy formulary"
- Look up the specific GLP-1 medication
- Check the prior authorization criteria document
- Call your state's Medicaid pharmacy helpline
States with broader coverage tend to have:
- Lower BMI thresholds
- Fewer step therapy requirements
- Coverage for weight-loss indications
TRICARE
TRICARE (military health coverage) uses Express Scripts for pharmacy benefits.
GLP-1 coverage under TRICARE:
- Generally covers GLP-1s for Type 2 diabetes with PA
- Weight-loss GLP-1 coverage is more limited
- Uses Express Scripts' standard PA criteria
Where to find TRICARE PA requirements:
- Tricare.mil → Pharmacy → Drug Search
- Express Scripts TRICARE: 1-877-363-1303
Federal Employee Health Benefits (FEHB)
If you're a federal employee:
- Coverage varies by the specific FEHB plan you've chosen
- Check your plan's formulary and PA requirements
- Contact your plan directly for GLP-1 coverage questions
Employer Plans That Exclude Weight-Loss Drugs
Many employer-sponsored plans specifically exclude "anti-obesity medications" or "drugs used for weight loss."
How to check for exclusions:
- Review your Summary of Benefits and Coverage (SBC) document
- Look for "Prescription Drug Exclusions" section
- Call your benefits department or the number on your insurance card
If weight-loss drugs are excluded:
- A PA won't override an exclusion
- You can request a "formulary exception" (but approval is difficult for explicit exclusions)
- Consider whether the diabetes pathway might apply to you
- Explore cash-pay alternatives
If Your GLP-1 Isn't Covered: Realistic Alternatives
Sometimes, despite your best efforts, insurance won't cover a GLP-1 for your situation. Here are your options, ranked by safety and practicality.
Option 1: Try a Different Covered GLP-1
If one GLP-1 isn't covered, another might be.
Ask your doctor:
- "Is there a GLP-1 on my formulary that would work for me?"
- "Can we try [covered alternative] instead?"
Common formulary patterns:
- Some plans prefer Trulicity over Ozempic
- Some cover Saxenda but not Wegovy
- Generic liraglutide (the generic version of Saxenda approved in 2025) may be more affordable where available
Option 2: Manufacturer Savings Programs
If you have commercial insurance (not Medicare/Medicaid), you may qualify for manufacturer savings cards that significantly reduce out-of-pocket costs.
Available programs:
- Ozempic/Wegovy/Rybelsus (Novo Nordisk): Check their patient assistance website
- Mounjaro/Zepbound (Eli Lilly): Check their savings program
- Trulicity (Eli Lilly): Check their patient support program
- Saxenda (Novo Nordisk): Check their savings program
Limitations:
- Most savings cards don't work with Medicare or Medicaid
- There may be income requirements for some assistance programs
- Savings amounts and eligibility change—always check current terms
Option 3: Cash-Pay Options
If insurance won't cover your GLP-1 at all, paying out of pocket is an option—though an expensive one.
How to minimize cash-pay costs:
- Check GoodRx, RxSaver, or similar discount sites for cash prices
- Compare prices between pharmacies (they vary widely)
- Consider mail-order pharmacies
- Ask about manufacturer cash-pay programs
Cost reality check:
- Many brand-name GLP-1s have four-figure monthly retail prices, which vary by dose, pharmacy, and discount programs (verify current pricing before deciding)
- Some telehealth programs offer bundled pricing
- Prices change frequently—always verify current costs
Option 4: Telehealth Weight-Loss Programs
Several telehealth companies specialize in GLP-1 prescriptions and may offer alternatives to traditional insurance routes.
How these work:
- Medical evaluation via telehealth
- Direct prescribing of GLP-1s (if appropriate)
- Some include medication cost; others require separate purchase
- Prices vary widely
Telehealth Programs Worth Considering
If you're exploring telehealth options for GLP-1 access, here are some established programs that offer medical evaluations and weight management support:
- Check Out MEDvī — Offers physician-led weight management programs with GLP-1 prescribing
- Check Embody Eligibility — Low first-month price and needle-free GLP-1 gum options
- Visit Yucca Health — Specializes in metabolic health and GLP-1 therapy
These are affiliate partners. We only recommend services we believe provide legitimate medical care. Read our full Yucca Health GLP1 reviews for detailed information.
Important considerations for any telehealth program:
- Make sure the program uses licensed providers in your state
- Verify medications come from licensed U.S. pharmacies
- Be cautious of programs that seem "too easy"—legitimate prescribing requires real medical evaluation
- These programs don't bypass the need for appropriate patient selection
What About Compounded GLP-1s?
Strong caution here. While compounded semaglutide and tirzepatide have become more available, there are significant safety concerns.
FDA warnings about compounded GLP-1s:
- Compounded versions are NOT FDA-approved
- There have been dosing errors with compounded products (different concentrations than brand-name versions)
- The FDA has expressed concerns about quality, safety, and sterility of some compounded products
- Some products labeled as "semaglutide" may contain different ingredients or incorrect doses
If you're considering compounded GLP-1s:
- Only use 503A or 503B compounding pharmacies licensed in your state
- Verify the pharmacy through your state board of pharmacy
- Understand that you're accepting more risk than with FDA-approved products
- Discuss with your doctor who can monitor for safety
We recommend sticking with FDA-approved products from licensed pharmacies when possible. The cost savings of compounded products may not be worth the safety risks.
Safety Section: Avoiding Counterfeit and Unapproved GLP-1s
The demand for GLP-1 medications has unfortunately created a market for fake, counterfeit, and unapproved products. Here's how to protect yourself.
Red Flags to Watch For
Be cautious if:
- A price seems too good to be true
- A website doesn't require a prescription
- The product is shipped from overseas
- The packaging looks different than legitimate products
- You can't verify the pharmacy's license
FDA Warnings You Should Know About
Compounding dosing errors: The FDA has warned that compounded semaglutide products may use different concentrations than brand-name versions, leading to dosing confusion and potential overdose.
Counterfeit products: The FDA has warned consumers about counterfeit Ozempic found in the U.S. drug supply chain, and has identified products falsely labeled as "semaglutide" that contained different or harmful ingredients.
Unapproved GLP-1s: Some products marketed as GLP-1s or "peptides" are not FDA-approved and haven't been evaluated for safety or efficacy.
How to Verify a Pharmacy
Verify online pharmacies using FDA BeSafeRx (fda.gov/besaferx) and NABP Safe.Pharmacy (safe.pharmacy).
The Safe Sourcing Checklist
- Pharmacy is licensed in the United States
- Pharmacy requires a valid prescription
- Pharmacy is verifiable through FDA BeSafeRx or NABP Safe.Pharmacy
- Product is FDA-approved (for brand-name medications)
- Packaging includes NDC number and proper labeling
- Product is not being shipped from overseas
- Price is roughly in line with other legitimate pharmacies
Frequently Asked Questions
General PA Questions
What does "prior authorization" mean for GLP-1 medications? Prior authorization is when your insurance company reviews your prescription before agreeing to cover it. For GLP-1s, this means your doctor submits documentation proving you meet the plan's criteria, and the insurance company either approves or denies coverage based on that review. It's not a denial—it's a checkpoint.
Can I get Ozempic/Wegovy/Mounjaro without prior authorization? Some plans auto-approve for certain diagnoses (like Type 2 diabetes already on file), but most require PA. If you want to avoid the PA process entirely, your options are cash pay, manufacturer savings programs (if eligible), or finding a plan during open enrollment that has fewer restrictions.
How long does GLP-1 prior authorization take? With complete documentation, electronic PA can be approved in 24–72 hours. Traditional submission typically takes 5–10 business days. Missing documentation or appeals can extend this by weeks. The most common cause of delays is incomplete paperwork.
What happens if I start using the medication before PA is approved? If you pay cash to start the medication, your insurance won't reimburse you retroactively (in most cases) if PA is later denied. If PA is approved, some pharmacies may be able to reprocess the claim. It's generally best to wait for approval unless medically urgent.
How long does my PA approval last? Most GLP-1 prior authorizations are approved for 6–12 months. After that, you'll need to submit for reauthorization. Check with your insurance or doctor's office to know your specific expiration date.
Criteria and Requirements
What BMI do I need for GLP-1 coverage for weight loss? Most plans require BMI ≥30, or BMI ≥27 with at least one weight-related health condition (like high blood pressure, diabetes, or sleep apnea). Some strict plans require BMI ≥35 or even ≥40. Check your specific plan's criteria—they vary.
What comorbidities count for GLP-1 coverage? Common qualifying comorbidities include: Type 2 diabetes or pre-diabetes, high blood pressure, high cholesterol, obstructive sleep apnea, cardiovascular disease, fatty liver disease, polycystic ovary syndrome, and obesity-related joint problems. The specific list varies by plan.
What counts as proof of lifestyle modification? Documentation from a physician-supervised weight-loss program, visits with a registered dietitian, enrollment records from structured programs (like Weight Watchers or Noom), or chart notes showing diet/exercise counseling at medical visits. The key is having provider documentation—not just saying you tried.
What is step therapy and how do I prove I tried prior medications? Step therapy means your plan requires you to try (and fail) other treatments before approving a GLP-1. To prove you've completed step therapy, your medical records need to show what medications you tried, at what doses, for how long, and why they didn't work (inadequate response, side effects, or contraindication).
Denials and Appeals
Why was I denied if I meet the BMI requirement? The most common reasons: BMI wasn't documented with a date, comorbidities weren't coded in your chart notes, step therapy wasn't completed/documented, wrong diagnosis code was used, or documentation was outdated. Check the denial letter for the specific reason.
What is a peer-to-peer review? A peer-to-peer review is when your doctor speaks directly with the insurance company's medical director to discuss your case. It's often available during the PA or appeal process and can be effective for borderline cases where the clinical story isn't fully captured in paperwork.
Can I appeal if my plan excludes weight-loss drugs? You can request a "formulary exception," but success is difficult if the drug category is explicitly excluded. You're essentially asking the plan to make an exception to their policy, which requires strong medical justification and often still results in denial.
Medicare, Medicaid, and Special Plans
Does Medicare cover GLP-1 medications? Medicare Part D covers GLP-1s for Type 2 diabetes (like Ozempic and Mounjaro) with prior authorization. Coverage for weight-loss drugs has historically been excluded by statute, though this is an evolving area. Check your specific Part D plan's formulary.
Does Medicaid cover GLP-1 medications? It varies by state. Most state Medicaid programs cover GLP-1s for Type 2 diabetes. As of January 2026, approximately 13 states cover GLP-1s for weight loss. Check your state's Medicaid formulary for specific coverage and PA requirements.
What's the difference between Wegovy and Ozempic for insurance coverage? They contain the same active ingredient (semaglutide) but have different FDA-approved uses. Ozempic is approved for Type 2 diabetes (and may be covered under diabetes drug benefits). Wegovy is approved for weight management, CV risk reduction, and MASH (and may only be covered if your plan covers weight-loss drugs). The coverage pathway depends on your diagnosis and plan.
Safety and Alternatives
Is compounded semaglutide safe? The FDA has expressed concerns about compounded semaglutide products, including dosing errors and quality issues. Compounded products are NOT FDA-approved. If you choose compounded products, use only licensed compounding pharmacies and understand you're accepting additional risk. We recommend FDA-approved products when possible.
How do I avoid counterfeit GLP-1 medications? Verify online pharmacies using FDA BeSafeRx and NABP Safe.Pharmacy. Require a valid prescription. Be cautious of unusually low prices or overseas shipping. Verify all packaging and labeling. If something seems off, don't use it.
Glossary of Terms
Prior Authorization (PA): Insurance review process that must be completed before a medication is covered.
Preauthorization/Precertification: Same as prior authorization—different plans use different terms.
PBM (Pharmacy Benefit Manager): Company that manages prescription drug benefits for your insurance (examples: CVS Caremark, Express Scripts, OptumRx).
Formulary: Your insurance plan's list of covered medications, usually organized by tier (cost level).
Step Therapy: Requirement to try (and fail) other medications before a more expensive medication is approved.
Quantity Limit (QL): Maximum amount of medication you can fill in a given time period.
ePA (Electronic Prior Authorization): Submitting prior authorization requests electronically rather than by fax or phone.
ICD-10: The coding system used to describe medical diagnoses (e.g., E11.9 for Type 2 diabetes).
NPI: National Provider Identifier—the unique ID number for healthcare providers.
Medical Necessity: The standard insurers use to determine if a treatment is needed for your health condition.
Formulary Exception: Request to cover a drug that's not on your plan's formulary (or that's excluded).
External Review: Independent review of a denied claim by an organization outside your insurance company.
GLP-1 Receptor Agonist: The drug class that includes Ozempic, Wegovy, Mounjaro, Zepbound, and related medications.
Tirzepatide: The active ingredient in Mounjaro and Zepbound (a GLP-1/GIP dual agonist).
Semaglutide: The active ingredient in Ozempic, Wegovy, and Rybelsus.
MASH: Metabolic dysfunction-associated steatohepatitis, a form of fatty liver disease with inflammation and scarring.
Sources and Methodology
How This Guide Is Maintained
This guide is updated regularly as coverage policies, drug approvals, and PA requirements change. Each insurance directory entry is verified against official sources when updated.
Update schedule: Monthly review for policy changes; immediate updates when major coverage changes occur.
Report an error or outdated information: If you notice something incorrect or out of date, please let us know.
Editorial Standards
- All coverage information is sourced from official insurer/PBM publications and verified where possible
- Clinical information references FDA-approved labeling and prescribing information
- We do not provide medical advice—consult your healthcare provider for personal medical decisions
- We may earn affiliate commissions if you use certain partner links; this doesn't affect our recommendations
Key References
FDA Drug Labels:
- Wegovy (semaglutide) prescribing information — accessdata.fda.gov
- Zepbound (tirzepatide) prescribing information — pi.lilly.com
- Ozempic (semaglutide) prescribing information — accessdata.fda.gov
- Mounjaro (tirzepatide) prescribing information — pi.lilly.com
FDA Safety Communications:
- FDA alerts on compounded semaglutide dosing errors — fda.gov
- FDA concerns about unapproved GLP-1 products — fda.gov
- FDA warns consumers about counterfeit Ozempic — fda.gov
Coverage and Policy Sources:
- CMS ICD-10-CM code files — cms.gov
- CDC obesity ICD-10 code update (October 2024) — cdc.gov
- Medicare Part D anti-obesity medication coverage analysis — aspe.hhs.gov
- Congressional Research Service Medicare drug coverage reports — congress.gov
Industry Data:
- AMA prior authorization physician survey — ama-assn.org
- AHA report on commercial health plan coverage challenges — aha.org
- Teva generic Saxenda approval announcement (August 2025) — tevapharm.com
Final Checklist: Your GLP-1 Prior Authorization Action Plan
Before you close this page, here's your game plan:
If you haven't submitted PA yet:
- Identify your PBM and look up your plan's specific criteria
- Gather your documentation before your doctor's appointment
- Make sure your chart notes include BMI + date, diagnosis codes, and comorbidities
- Confirm any step therapy requirements and document prior medication trials
If PA has been submitted:
- Follow up after 5 business days if you haven't heard back
- Keep copies of all documentation submitted
- Know your appeal deadline in case of denial
If you were denied:
- Read the denial letter carefully—identify the specific reason
- Gather additional documentation that addresses the gap
- Submit your appeal before the deadline
- Consider requesting a peer-to-peer review
If insurance won't cover your medication:
- Explore alternative covered GLP-1s
- Check manufacturer savings programs
- Evaluate cash-pay options carefully
- Consider telehealth weight-loss programs (MEDvī, Embody, Yucca Health)
- Avoid unverified or overseas sources
Related Guides:
- Best GLP-1 Online Programs — Compare telehealth providers for GLP-1 prescriptions
- How Much Does GLP-1 Cost Without Insurance — Complete pricing guide
- Semaglutide vs Tirzepatide — Which medication is right for you
- GLP-1 Side Effects Guide — Managing common side effects
This guide is for informational purposes only and does not constitute medical advice. Always consult your healthcare provider for decisions about your health and treatment.
Affiliate Disclosure: Some links on this page are affiliate links. We may earn a commission if you use them to sign up for services, at no additional cost to you. This doesn't affect our editorial recommendations—we only recommend services we believe provide legitimate medical care. See our editorial standards for more information.
This content is educational only and does not replace professional medical advice. Always consult a qualified healthcare provider before starting any medication.