GLP-1 After Bariatric Surgery: What Post-Bariatric Patients Should Know Before Starting
By the WPG Editorial Team — an independent comparison resource for GLP-1 telehealth providers · · Next scheduled re-verification: July 27, 2026 · Reading time: ~22 minutes
Yes, you can take a GLP-1 after bariatric surgery — and for many post-bariatric patients dealing with weight regain, plateau, or returning hunger, it's a clinically supported option. GLP-1 receptor agonists (medications like Wegovy, Zepbound, Ozempic, Mounjaro, and Foundayo that mimic the body's glucagon-like peptide-1 hormone to reduce appetite) have produced an additional 8–15% total body weight loss at six months in published post-bariatric studies. But here's the part most pages skip: this is not always a "click and order online" decision. The right path depends on your surgery type, how long it's been, your nutrition labs, your symptoms, and whether you want FDA-approved medication or a cash-pay route.
We're going to walk you through every fork in that decision — and at the end you'll have a clear next step, not a sales pitch.
| Your situation | Bottom line | First step |
|---|---|---|
| 9–18+ months post-sleeve or post-bypass, stable intake, regain or plateau | A GLP-1 is reasonable to discuss | Take the readiness check below |
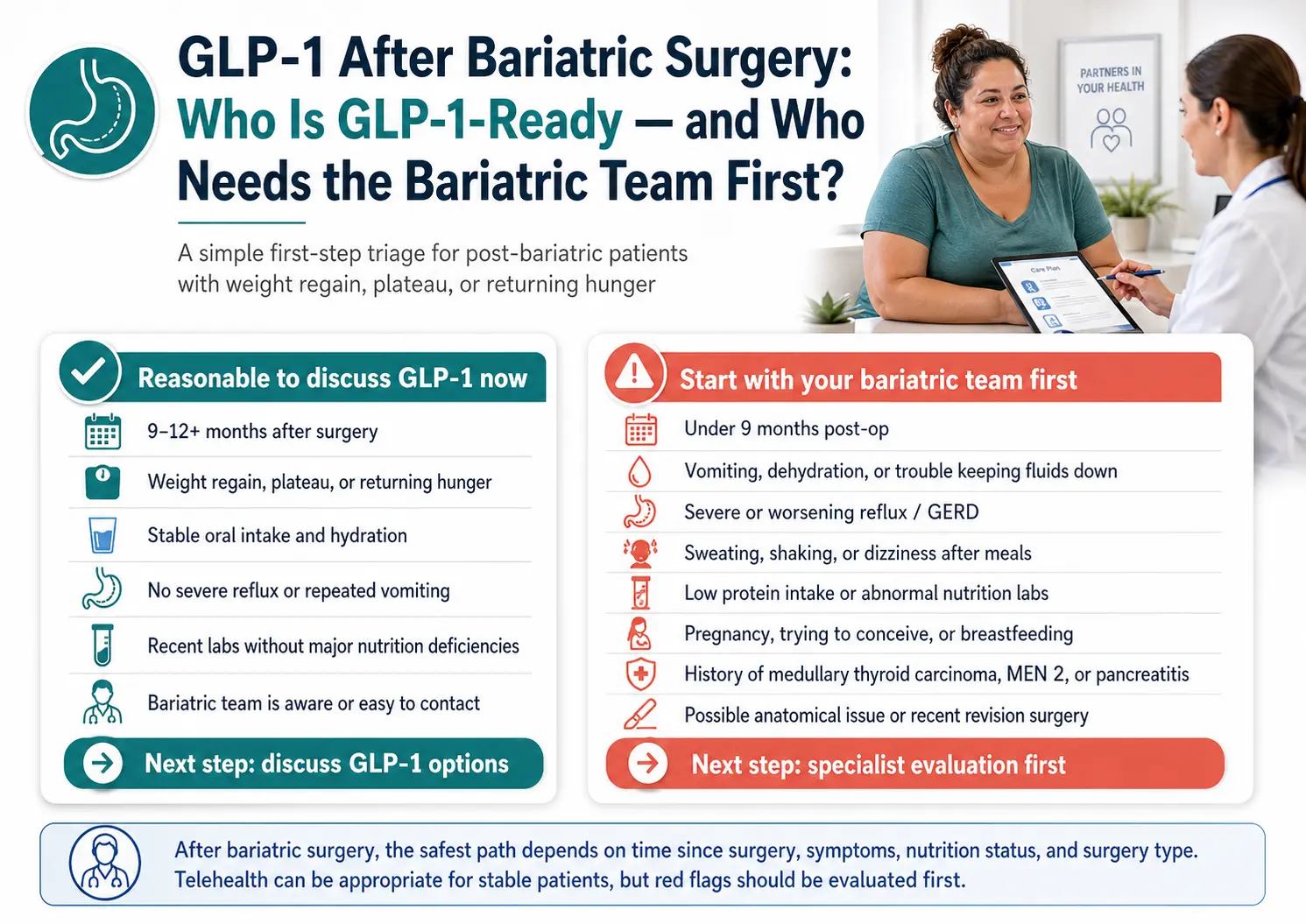
| Severe reflux, vomiting, dehydration, low protein, abnormal labs, or under 9 months post-op | Telehealth is not your starting point | Bariatric team first |
| Want FDA-approved medication and possibly insurance help | Brand-name path is cleanest | Use the readiness check, then see your options |
| Cash-pay, no insurance, no safety red flags | Multiple routes — cost varies widely | Use the readiness check, then compare |
Don't know which row you're in?
→ Build my post-bariatric GLP-1 action plan60 seconds. We'll route you to the right next step — not a checkout.
Why we built this guide differently
Search "GLP-1 after bariatric surgery" and you'll find two kinds of pages: medical articles written for clinicians, and affiliate pages written for people who never had surgery. Neither one talks to you.
You had the surgery. It worked, mostly. Now something's shifted — the scale's creeping up, food noise is back, your A1C ticked up, or that last 30 pounds won't budge. You've heard about Ozempic and Wegovy. You want to know if it's safe with your altered anatomy, whether it means your surgery "failed," and whether you can just go online and order it.
This page is built for that conversation. We synthesized the post-bariatric clinical evidence from peer-reviewed sources, reviewed the FDA labels and warnings, and assembled what major telehealth providers publicly state about their formulary, pricing, and intake. Every clinical claim is sourced. Every pricing point has a "last verified" date. We tell you when our affiliate options are wrong for you.
Can you take a GLP-1 after bariatric surgery?
Yes. GLP-1 receptor agonists are increasingly used after bariatric surgery for weight regain, insufficient weight loss, plateau, or returning hunger. In a JAMA Surgery cohort summarized by Johns Hopkins, 15,749 of 112,858 post-bariatric patients — about 14% — initiated a GLP-1 medication after their procedure. The decision is not automatic — it depends on time since surgery, nutrition status, GI symptoms, and existing medications — but the medication class is not blocked by your surgical history.
Bariatric surgery remains the most effective single treatment for severe obesity, but roughly 20–30% of patients experience weight regain or insufficient weight loss after their procedure (Johns Hopkins / JAMA Surgery, 2025). That's not a small slice — that's millions of people across the surgical population. Until recently, the only "next steps" were behavioral or surgical revision, with higher complication risk.
GLP-1s mimic a hormone your gut already releases after meals — one that signals fullness, slows digestion, and tamps down hunger. Bariatric surgery itself raises your body's own postprandial GLP-1 levels (which is part of why surgery works). So when you add a pharmacologic GLP-1, you're not fighting your surgery — you're amplifying a signal it was already using.
Caroline Apovian, MD, co-director of the Center for Weight Management and Wellness at Brigham and Women's Hospital, put it directly in a March 2026 MedCentral interview: "Metabolic surgery alters all gut hormones — not just GLP-1s — so GLP-1 therapy is simply adding to what surgery already does. Many of the bariatric surgery risks are overstated, reflecting long-standing stigma around obesity."
If you're worried that needing a GLP-1 means your surgery failed, you're wrong. Surgery did its job — it gave you a window of dramatic weight loss and metabolic reset. Biology adapts over time. So do treatments. Adding medication doesn't undo what surgery did, any more than adding a second blood-pressure medication means the first one "failed."
Who should NOT start with a telehealth GLP-1 provider after bariatric surgery
If you're less than nine months post-op, currently vomiting or dehydrated, dealing with severe reflux, experiencing hypoglycemia symptoms, eating poorly with low nutrition labs, pregnant, or have a history of medullary thyroid carcinoma or pancreatitis, do not start with a telehealth checkout. Your first appointment should be with your bariatric surgery team, an obesity medicine specialist, or your primary care provider — not an online intake form. Telehealth may still be appropriate for you later, but these issues need bariatric-aware evaluation first.
We're going to do something most affiliate pages won't: tell some of you to leave.
A GLP-1 is not the right first move for every post-bariatric patient. If your regain is driven by an anatomical issue (a dilated pouch, a band complication, a fistula), a medication won't fix it. If you're fighting nausea, vomiting, or dehydration, a GLP-1 will likely make it worse. If your protein intake has slipped and your labs are showing it, adding an appetite suppressant is the wrong order of operations.
Specialist-first red flags
If any of these apply, your starting point is your bariatric team, not a telehealth intake form:
- ✕Less than 6–9 months post-op and still actively losing weight on the surgical curve
- ✕Vomiting, repeated nausea, or trouble keeping fluids down
- ✕Severe reflux or GERD that's worsened since surgery (especially after sleeve gastrectomy)
- ✕Abdominal pain, gallbladder symptoms, or unexplained nausea
- ✕Dizziness, fainting, sweating after meals — possible signs of post-bariatric hypoglycemia or dumping syndrome
- ✕Hair loss, fatigue, low protein intake — possible signs of malnutrition
- ✕Recent labs showing low albumin, B12, iron, zinc, vitamin D, or PTH abnormalities
- ✕Currently on insulin or a sulfonylurea for diabetes (these need supervised dose adjustment)
- ✕Pregnant, trying to conceive, or breastfeeding
- ✕Personal or family history of medullary thyroid carcinoma or MEN-2 — an absolute contraindication per the FDA labels for Wegovy, Zepbound, Foundayo, and other GLP-1 RAs
- ✕History of pancreatitis or active pancreatitis symptoms
- ✕Anatomical concerns — suspected pouch dilation, band slip, fistula, internal hernia
And for everyone else
For most post-bariatric patients more than 9–12 months out, with stable intake, no severe GI symptoms, normal-ish nutrition labs, and no contraindications — you're a reasonable candidate for the conversation. A GLP-1 may genuinely help. Where you go next depends on whether you want FDA-approved medication, whether insurance is in play, and whether your bariatric team can prescribe or refer.
Click to take the free 60-second readiness check
When is it usually reasonable to start a GLP-1 after bariatric surgery?
There is no universal guideline. One expert benchmark cited in a March 2026 MedCentral interview with Caroline Apovian, MD is to wait at least nine months after surgery to confirm a true plateau. In a 112,858-patient post-bariatric cohort published in JAMA Surgery (2025), peak GLP-1 initiation occurred around years 3–4 after surgery, with semaglutide accounting for 57.8% of initiations.
The nine-month benchmark isn't arbitrary. The first year after surgery is when your weight loss curve is steepest, and starting a GLP-1 inside that window confuses the picture: you can't tell if continued loss is the surgery still working or the medication doing something.
| Time since surgery | What it usually means | GLP-1 decision |
|---|---|---|
| 0–3 months | Active rapid surgical weight-loss phase | Bariatric team only — no GLP-1 |
| 3–8 months | Still early; intake, hydration, and nutrition are fragile | Specialist-first; GLP-1 not typical |
| 9–18 months | Surgical curve flattens; plateau or insufficient loss may become visible | GLP-1 worth discussing if a true plateau is confirmed |
| 18 months – 5 years | "The window where regain shows up" — biology adapts, food noise can return | GLP-1 frequently appropriate |
| 5+ years | Regain may involve anatomy, lifestyle, hormones, menopause, diabetes recurrence | Evaluate cause first, then GLP-1 or revision conversation |
| Duodenal switch / SADI / revision history | Higher nutritional vulnerability or unclear anatomy | Always specialist-first regardless of time |
Plateau, regain, and insufficient weight loss — they're not the same thing
Plateau is when your weight loss stalls before you've reached a goal you're satisfied with. The scale isn't going up — it's stuck.
Weight regain is when you've reached a low point (your "nadir") and the scale is now climbing back up. The cutoff for clinically meaningful regain varies, but a 5+ kg increase from nadir is one common threshold.
Insufficient weight loss (IWL) is the formal term — typically defined as less than 50% excess weight loss at 18 months post-surgery.
How much weight loss is realistic with a GLP-1 after bariatric surgery?
Published evidence in post-bariatric patients shows additional total body weight loss of 8–15% at six months on a GLP-1, with tirzepatide trending higher than semaglutide and both exceeding liraglutide. A real-world UT Southwestern cohort of 207 post-bariatric adults found 12.9% body weight loss at 12 months on semaglutide vs. 8.8% on liraglutide. A 2025 systematic review and meta-analysis (Manyari et al., Obesity Surgery) of 964 patients across 8 studies reported −10.97% TBWL with semaglutide and −13.63% with tirzepatide. Roughly 1 in 4 patients are non-responders.
| Study | Medication | Sample | Duration | Result (TBWL) | Limitation |
|---|---|---|---|---|---|
| Mok et al., JAMA Surgery 2023 (BARI-OPTIMISE RCT) | Liraglutide 3.0 mg | 70 (RYGB or sleeve) | 6 months | 8.8% vs. 0.5% placebo | Only RCT to date; not long-term |
| UT Southwestern (Lewis et al., 2023) | Semaglutide vs. liraglutide | 207 adults (~8 yrs post-op) | 12 months | Sema: 12.9% · Lira: 8.8% | Retrospective real-world |
| Jamal et al., Obesity Surgery 2024 | Semaglutide (sleeve) | 70 | 6 months | 10.3% | Single center; sleeve only |
| Jamal et al., Obesity Surgery 2024 | Tirzepatide (sleeve) | 45 | 6 months | 15.5% | Single center; sleeve only |
| Lautenbach et al., Obesity Surgery 2022 | Semaglutide 0.5–1.0 mg/wk | 44 (RYGB or sleeve) | 6 months | 10.3% | Subtherapeutic doses by today's standards |
| Kanai et al., 2024 | Semaglutide (sleeve + T2D) | 29 (Japanese) | 12 months | BMI/HbA1c improved; ↓albumin, B12, zinc | Small; nutrition safety signal flagged |
| Kim et al., JAMA Surgery 2025 | All GLP-1 RAs (57.8% sema) | 112,858 post-bariatric (14% GLP-1 initiators) | Variable | Peak initiation years 3–4 post-op | Pre-dates current tirzepatide adoption |
| Manyari et al., Obesity Surgery 2025 (meta-analysis) | Pooled GLP-1 RAs (964 pts, 8 studies) | 964 | 3–24 months | Tirz: −13.63% · Sema: −10.97% | Heterogeneous; mostly retrospective |
The numbers are real but variable. Across studies, post-bariatric patients on a GLP-1 lost an additional 8–15% of total body weight in six months. For someone weighing 220 pounds, that's 17–33 pounds of additional loss. But "average" hides individual variation, and roughly 1 in 4 patients didn't reach the 5% threshold typically considered a clinical response.
Tirzepatide trends higher than semaglutide. In the Jamal sleeve cohort, tirzepatide produced 15.5% versus semaglutide's 10.3% over six months. The Manyari meta-analysis showed a similar gap (−13.63% vs. −10.97%). If you have access to both, that gap may matter.
Liraglutide has the strongest randomized evidence but the smallest results. BARI-OPTIMISE is the only published RCT in post-bariatric patients. It's a daily injection rather than weekly, and its weight loss numbers are lower than the newer agents.
Long-term data is limited. Most studies run 6 to 12 months. A 2026 Oxford-summarized BMJ analysis found that patients regained an average of 0.8 kg per month for newer agents like semaglutide and tirzepatide after stopping. Plan accordingly.
A reasonable benchmark: 5% additional TBWL by three months is the typical responder threshold. If you haven't hit that on a therapeutic dose, the conversation shifts to switching agents, evaluating anatomy, or escalating care.
Which GLP-1 medication makes the most sense after bariatric surgery?
There's no single best GLP-1 for every post-bariatric patient. Tirzepatide (Zepbound) trends highest in published post-bariatric weight loss data. Semaglutide (Wegovy, Ozempic) has the most cumulative real-world data and broader insurance coverage. Liraglutide (Saxenda) has the only randomized trial in this population. Newer oral options like Foundayo (orforglipron) and the Wegovy pill add convenience but bring absorption considerations — particularly after gastric bypass.
| Medication | Form | Avg. post-bariatric TBWL | Post-bariatric consideration |
|---|---|---|---|
| Tirzepatide (Zepbound) | Weekly subcut. injection | ~13–15% (6 mo) | Highest TBWL in post-bariatric data; dual GLP-1/GIP. Oral contraceptive interaction — use backup for 4 wks after initiation and each dose escalation |
| Tirzepatide (Mounjaro) | Weekly subcut. injection | Same molecule as Zepbound | FDA-approved for T2D only; same drug, different label |
| Semaglutide (Wegovy pen) | Weekly subcut. injection | ~10–13% (6–12 mo) | Most-prescribed agent in post-bariatric cohorts; strongest insurance coverage |
| Semaglutide (Wegovy pill) | Daily oral tablet | Limited post-bariatric data | Must take on empty stomach; 30-min wait before food, drink, or other oral meds. Absorption may be reduced after RYGB |
| Orforglipron (Foundayo) | Daily oral tablet (non-peptide) | Limited post-bariatric data | No empty-stomach restriction. Oral birth-control pill effectiveness reduced — use backup for 30 days after start and each dose increase |
| Liraglutide (Saxenda) | Daily subcut. injection | ~8.8% (BARI-OPTIMISE RCT) | Only randomized post-bariatric evidence; daily injection burden vs. weekly competitors |
| Compounded semaglutide / tirzepatide | Various (subcut, oral, sublingual) | Limited post-bariatric data | Not FDA-approved as finished drug products — not reviewed by FDA for safety, effectiveness, or quality. Quality varies by pharmacy |
Do oral GLP-1 pills work after gastric sleeve or gastric bypass?
Oral peptide GLP-1s like the Wegovy pill have absorption requirements that altered anatomy can complicate — particularly after Roux-en-Y gastric bypass. The Wegovy pill must be taken on an empty stomach with water and requires a 30-minute wait before food, drinks, or other oral medications, per the FDA label. Foundayo (orforglipron) is a non-peptide oral GLP-1 designed without these restrictions, but post-bariatric–specific data is still limited. Subcutaneous injections bypass the absorption question entirely.
If you're a sleeve patient with no anatomical bypass, oral peptide forms generally work, but the 30-minute empty-stomach window is a real adherence challenge. If you're an RYGB patient, talk to your bariatric team specifically about whether oral peptide forms are likely to absorb adequately for you. Foundayo or an injectable is the cleaner choice in most bypass cases.
A note on compounded GLP-1s
You'll see compounded semaglutide and tirzepatide advertised at $179–$299 per month. The FDA has been explicit that compounded GLP-1 drugs are not FDA-approved finished products and are not reviewed for safety, effectiveness, or quality. The FDA's standard for when compounded medication is appropriate is medical-need-not-met-by-an-FDA-approved-drug, or unavailability of the FDA-approved drug — not cost. If a licensed clinician prescribes a compounded preparation for your situation, verify: (1) the state-licensed pharmacy filling it; (2) the exact formulation — the FDA has flagged concerns about salt forms like semaglutide sodium and semaglutide acetate; (3) dose instructions and storage requirements; (4) the clinician's plan for follow-up monitoring.
Can you take GLP-1 after gastric sleeve?
Yes. Sleeve gastrectomy patients are well represented in post-bariatric GLP-1 evidence — including the Jamal et al. 2024 cohort of 115 sleeve patients showing 10.3% weight loss with semaglutide and 15.5% with tirzepatide at six months, and the BARI-OPTIMISE RCT which included sleeve patients. The two key sleeve-specific considerations are reflux risk and slower titration.
Sleeve removes about 80% of your stomach, leaving a tube-shaped remnant. The two GLP-1-relevant issues:
- →Reflux risk. Sleeve patients have higher rates of GERD than bypass patients, and GLP-1-induced delayed gastric emptying can worsen it. If reflux has been creeping up on you, that's a flag to bring up before starting.
- →Nausea amplification. With a smaller stomach plus a medication that slows gastric emptying, you may feel fullness more intensely. Slow titration matters more here — a normal Wegovy ramp may need to go slower.
- →Endogenous GLP-1 is already elevated after sleeve. Adding pharmacologic GLP-1 is additive, not redundant. Most published post-bariatric tirzepatide data is in sleeve cohorts, and the agent works.
Can you take GLP-1 after gastric bypass or RNY?
Yes. Roux-en-Y gastric bypass (RYGB) patients were included in BARI-OPTIMISE and the larger retrospective cohorts. The bypass-specific considerations are oral peptide medication absorption (favor injectables or non-peptide oral options like Foundayo), post-bariatric hypoglycemia, and drug interactions with insulin or sulfonylureas.
→Oral medication absorption is altered. This matters most for oral peptide GLP-1s like the Wegovy pill. Foundayo (orforglipron) is a non-peptide oral GLP-1 designed to be more absorption-stable. Subcutaneous injections bypass the question entirely.
→Post-bariatric hypoglycemia (PBH). A real complication after RYGB. If you experience sweating, shaking, dizziness, or fainting 1–3 hours after meals, this needs evaluation before adding any glucose-lowering medication.
→Drug interactions get serious. Insulin and sulfonylureas combined with a GLP-1 can cause severe hypoglycemia. Doses usually need supervised adjustment.
What about lap band, duodenal switch, or revision history?
Laparoscopic adjustable gastric band: The GLP-1 conversation is more straightforward — unless you have a band complication (slip, erosion, port issue), in which case revision is the discussion, not medication.
Duodenal switch (BPD/DS) and SADI: These are the most aggressive procedures, with substantial malabsorption built in. Oral peptide GLP-1s are the worst fit. Subcutaneous injection works, but specialist supervision is non-negotiable — the combination of malabsorption plus appetite suppression can produce serious deficiencies fast.
Revision history: If you've had a sleeve-to-bypass conversion, band-to-sleeve, or any other revision, coordinate with your team. Don't shop GLP-1 online in this case.
The biggest GLP-1 risks specific to post-bariatric patients
Beyond standard GLP-1 side effects, post-bariatric patients face elevated risk in five areas: nutritional deficiency (especially protein, B12, zinc, and albumin), dehydration from compounded nausea and reduced intake, worsened reflux or severe GI symptoms, hypoglycemia from drug interactions with diabetes medications, and oral medication absorption issues. Kanai et al. 2024 found that albumin, vitamin B12, and zinc levels decreased after starting semaglutide in post-sleeve patients with T2D, even when weight loss and HbA1c improved.
1. Nutritional deficiency — the issue affiliate pages skip
Bariatric surgery already creates lifelong nutritional risk. Add a GLP-1 that drops your appetite, and you can compound the problem fast. Get baseline labs before starting (CBC, CMP, B12, folate, iron studies, ferritin, vitamin D, calcium, PTH, HbA1c). Repeat labs at three months on therapy. Target protein intake at the upper end of your bariatric program's goal or higher. Don't skip your bariatric vitamins.
2. Dehydration and acute kidney injury
GLP-1 nausea plus an already-restricted stomach plus reduced thirst signaling equals a real dehydration risk. The FDA labels for Wegovy and similar agents flag acute kidney injury due to volume depletion. Sip fluids continuously. If you're vomiting more than once or twice in 24 hours, contact your team.
3. Reflux, GERD, and severe GI reactions
Per the Wegovy label, severe gastrointestinal adverse reactions have been reported, and Wegovy is not recommended in patients with severe gastroparesis. Foundayo's labeling includes similar warnings. Sleeve patients are most likely to feel this; titrate slowly and don't push past a dose your stomach hates.
4. Hypoglycemia and diabetes medications
If you're on insulin or a sulfonylurea, a GLP-1 added on top can drop your blood sugar dangerously. RYGB patients with post-bariatric hypoglycemia are particularly vulnerable. This is a "your bariatric and endocrine team coordinate before you start" situation, not an online checkout.
5. Pregnancy and oral contraceptives
Both Wegovy and Zepbound carry pregnancy warnings — discontinue before planned pregnancy. The Zepbound label states oral contraceptives may be less effective due to delayed gastric emptying — barrier or non-oral contraception advised for 4 weeks after starting and after each dose escalation. Foundayo carries a similar 30-day warning. If contraception was a casual checkbox before, revisit it now.
FDA-approved vs. compounded GLP-1 after bariatric surgery — which route?
For most post-bariatric patients, FDA-approved branded medication is the cleaner first route. Compounded GLP-1s are not FDA-approved as finished drug products and are not reviewed by the FDA for safety, effectiveness, or quality. For medically complex post-bariatric patients, that conservative answer matters more than it does for the general population.
When FDA-approved is the right call
- You have commercial insurance that covers GLP-1 medication for chronic weight management
- You have HSA or FSA dollars (FDA-approved branded medication is eligible when prescribed for chronic weight management)
- You have any safety complexity — diabetes meds, prior pancreatitis, complex revision history, current GI issues, pregnancy concerns
For these readers, the cleanest path is Ro — strong insurance support including a free GLP-1 Coverage Checker and insurance concierge. Sesame Care is the strongest cash-pay FDA-approved alternative with the broadest formulary and dose-specific transparent pricing.
When compounded may be appropriate
- A licensed clinician determines that an FDA-approved drug doesn't meet your specific medical needs
- The FDA-approved drug is unavailable
- You've discussed the route with a clinician who's aware of your bariatric history
For this reader, Embody and MEDVi are two cash-pay compounded telehealth options with public pricing.
Want help deciding which route fits your situation?
→ Compare FDA-approved and self-pay GLP-1 pathsWhat's the safest GLP-1 access path for post-bariatric patients?
The safest access path depends on your clinical situation. If you have any specialist-first red flags, your starting point is your bariatric team — not telehealth. If you're stable with no red flags and have insurance, Ro is the strongest FDA-approved path because of its insurance concierge and free coverage checker. If you're stable, cash-pay, and want FDA-approved branded medication, Sesame Care offers the broadest FDA-approved formulary and dose-specific transparent pricing. If a clinician determines compounded medication is appropriate for your specific situation, Embody and MEDVi are two cash-pay telehealth options with public pricing.
| Provider | FDA-approved options | Compounded options | Notable for post-bariatric |
|---|---|---|---|
| Ro | Foundayo, Wegovy pill, Wegovy pen, Zepbound pen, Zepbound KwikPen | No | Insurance concierge + free Coverage Checker; broadest FDA-approved telehealth formulary |
| Sesame Care | Wegovy pill, Wegovy pen, Zepbound KwikPen, Foundayo, Ozempic, Mounjaro, Saxenda | Limited / provider-specific | Provider choice marketplace; dose-specific cash-pay pricing; insurance accepted on some medications |
| Hims / Hers | Wegovy pill, Wegovy pen, Ozempic; LillyDirect routing for Zepbound vials, KwikPen, and Foundayo as of April 23, 2026 | Reduced/deprioritized following Novo Nordisk partnership | Familiar consumer telehealth brands; FDA-approved formulary expanding |
| Embody | None — compounded only, not FDA-approved | Compounded semaglutide and tirzepatide; weekly injection or needle-free GLP-1 gum | Cash-pay from $99 first month (semaglutide injection), then $299/mo; HSA/FSA accepted; 24/7 support |
| MEDVi | Limited — verify | Compounded semaglutide and tirzepatide; broad menu | Cash-pay-friendly; intake form addresses prior bariatric surgery |
Information above is based on public-facing provider pages as of April 27, 2026. Pricing, formulary, and state availability change frequently — confirm current details directly on each provider's site before you pay.
Ro — best for insurance candidates and FDA-approved brand-name preference
Ro is the strongest FDA-approved path when insurance is potentially in play. Their GLP-1 Insurance Coverage Checker is free, takes about 60 seconds, and tells you whether your specific plan covers Wegovy or Zepbound before you spend a dollar. If your plan covers it, their insurance concierge handles the prior authorization paperwork — useful for post-bariatric patients whose surgical history makes documentation longer. Ro Body membership is $39 for the first month, then $149/month — or as low as $74/month with the annual plan. Medication is priced separately. Their formulary covers Foundayo, Wegovy pill, Wegovy pen, Zepbound pen, and Zepbound KwikPen.
Where Ro doesn't win: Ro is a clinical telehealth platform, not a bariatric-specialist clinic. If your case is genuinely complex — recent revision, severe nutritional issues, anatomical concerns — your bariatric team is still the better starting point.
Check your GLP-1 coverage in 60 seconds with Ro's free Coverage Checker →Sesame Care — broadest FDA-approved formulary, provider choice, dose-specific pricing
Sesame is structured as a marketplace: clinicians set their own prices and you pick. Their FDA-approved formulary is the broadest of the major telehealth options (Wegovy pill, Wegovy pen, Zepbound KwikPen, Foundayo, Ozempic, Mounjaro, Saxenda). Cash-pay GLP-1 medications start at $149/month for Wegovy pill and Foundayo, with dose-specific pricing for higher doses. Insurance is accepted on some medications. The Success by Sesame program runs as low as $59/month with annual prepay (medication priced separately).
Where Sesame doesn't win: because each clinician operates independently, the experience varies — there's no single care team coordinating your post-bariatric history across visits. Sesame's strength is choice, formulary breadth, and price transparency.
Compare branded GLP-1 prices on Sesame Care →Hims and Hers — FDA-approved access expanding with LillyDirect partnership
Following the March 2026 Novo Nordisk partnership and an April 23, 2026 announcement, Hims and Hers carry FDA-approved Wegovy pill, Wegovy pen, and Ozempic — and providers on the platform can now send prescriptions for Zepbound vials, Zepbound KwikPen, and Foundayo to LillyDirect for eligible customers. Their intake forms ask about bariatric history. They're a fit if you specifically want a familiar consumer telehealth brand and FDA-approved medication.
Where they don't win: less integrated insurance support than Ro for prior authorization. If insurance is in play and you want the broadest FDA-approved options handled in one place, Ro is the stronger pick.
Embody — low first-month price and a needle-free GLP-1 gum option
Embody is cash-pay with a low entry price: semaglutide injection starts at $99 for the first month, then $299/month ongoing, and tirzepatide injection starts at $149 first month, then $399/month. Its standout differentiator is a needle-free GLP-1 gum for readers who want to avoid injections. HSA/FSA is accepted, but Embody does not bill insurance or Medicare. Its shipped medications are compounded — not FDA-approved finished drug products. Availability is broad across the U.S., but confirm your state is supported during intake.
Where Embody doesn't win: if your priority is FDA-approved branded medication or insurance coverage, Sesame, Ro, or manufacturer-direct are the better fit. Embody is a real option for readers whose clinician determines compounded is appropriate and who want the lowest first-month cost or a needle-free route.
Check Embody Eligibility →MEDVi — broad compounded menu and post-bariatric-aware intake
If a licensed clinician determines that compounded medication is appropriate for your specific situation, MEDVi has one of the broader compounded menus — across compounded semaglutide and tirzepatide options. Their intake form addresses prior bariatric surgery. Pricing is transparent ($179 first month, $299 refills for compounded semaglutide). HSA/FSA is accepted at checkout. No membership fees.
Where MEDVi doesn't win: compounded GLP-1s are not FDA-approved as finished drug products. For a post-bariatric patient with medical complexity, FDA-approved is the conservative recommendation when affordable. Choose MEDVi only when a clinician determines compounded is appropriate for your situation — not as a default.
See MEDVi's current options & pricing →Insurance and cost reality for post-bariatric patients
A common assumption: "Insurance won't cover GLP-1 because I already had bariatric surgery." It's frequently wrong. Your post-bariatric records — the documented obesity history, prior treatment, and medical necessity — can support coverage. Wegovy and Zepbound coverage has expanded for many commercial plans through 2025 and 2026. HSA and FSA dollars apply to FDA-approved branded medication when prescribed for chronic weight management.
Insurers want to see: (1) a documented obesity diagnosis; (2) failure of prior less-invasive interventions; (3) current BMI or comorbidities meeting criteria. Your post-bariatric status is generally not a coverage barrier. Where friction usually shows up:
- Prior authorization paperwork — this is where Ro's insurance concierge earns its money.
- Step therapy requirements — some plans require Wegovy before approving Zepbound. Your prescriber can usually appeal.
- Plan-specific exclusions — a small number of plans exclude weight-loss medications entirely. Ro's free Coverage Checker tells you in 60 seconds whether your plan is one of them.
HSA and FSA: When prescribed for chronic weight management, FDA-approved branded Wegovy, Zepbound, Saxenda, and Foundayo are HSA and FSA eligible. Sesame Care, Embody, and others accept HSA/FSA at checkout. Compounded eligibility varies — verify with your benefits administrator.
| Path | Approximate monthly cost |
|---|---|
| Insurance with prior auth | Plan-specific; copay varies. Sesame lists "as low as $25/month" with insurance for some medications |
| Manufacturer direct (LillyDirect, NovoCare) | Varies by medication and dose; typically several hundred dollars per month for branded Wegovy or Zepbound |
| Ro Body cash-pay | $39 first month, then $149/mo (or $74/mo annual) — medication priced separately ($149–$449/mo by medication and dose) |
| Sesame Care (FDA-approved branded, cash) | $149/mo and up dose-specific; Success by Sesame as low as $59/mo annual |
| Embody (compounded, cash-pay) | Semaglutide injection $99 first month, then $299/mo; tirzepatide injection $149 first month, then $399/mo; needle-free GLP-1 gum option |
| MEDVi (compounded) | $179 first month, $299 refills |
Ro
60 seconds · no payment required
Free GLP-1 Coverage Checker · FDA-approved formulary
Find out exactly what your insurance covers — free with Ro's GLP-1 Coverage CheckerShould you use telehealth for GLP-1 after bariatric surgery?
Telehealth can be appropriate for post-bariatric patients who are at least 9–12 months out, have stable oral intake, no severe GI symptoms, recent labs, and no specialist-first red flags. Telehealth is not appropriate as the first step for early post-op patients, complex revision history, malabsorptive procedures with abnormal labs, suspected anatomical issues, post-bariatric hypoglycemia symptoms, or severe reflux.
Telehealth fits if:
- ✓You're 9–12+ months post-op
- ✓Your intake is stable
- ✓You're not vomiting or chronically dehydrated
- ✓Your reflux is manageable
- ✓You don't have unexplained abdominal pain
- ✓Your labs are recent (within 6 months) or the provider orders them
- ✓Your bariatric team is aware (or your records are accessible)
Telehealth doesn't fit if:
- ✕You're early post-op (under 9 months)
- ✕You've had recent revision surgery
- ✕You have complex malabsorption (DS, SADI)
- ✕You have unexplained regain that might be anatomical
- ✕You experience hypoglycemia or dumping syndrome symptoms
- ✕Your reflux has worsened post-op
- ✕Your labs show concerning deficiencies
What a legitimate telehealth provider asks
When you complete a post-bariatric-aware intake, expect questions like: surgery type and date, current weight and post-op nadir, regain amount and timeline, current medications including bariatric supplements, diabetes history and most recent A1C, current GI symptoms, most recent lab values, pregnancy status and contraception, and state of residence. If a provider's intake doesn't ask any of this — particularly the surgery type and date — that's a flag.
What happens if you stop a GLP-1 after bariatric surgery?
Significant weight regain after stopping a GLP-1 is highly likely and well-documented. A 2026 Oxford-summarized BMJ analysis found average regain of 0.8 kg per month for newer agents like semaglutide and tirzepatide. Plan for GLP-1 as long-term therapy from day one — like medication for blood pressure or another chronic condition. Don't start without a maintenance plan you can actually sustain.
The medication works while you're on it. When you stop, biology resumes its previous course. For post-bariatric patients specifically, this matters more than for the general population — you've already done a major intervention and emotionally invested in it being permanent.
Maintenance questions to answer before you start
- 1.Can I afford this medication for years, not months?
- 2.What happens if my insurance stops covering it?
- 3.What's my nutrition plan during and if I ever discontinue?
- 4.What's my protein target and how will I hit it?
- 5.How will I monitor for muscle loss vs. fat loss?
- 6.What labs will I check, and how often?
- 7.Is there a lower-dose maintenance option once I reach goal?
- 8.What's my plan if side effects force a pause?
- 9.Who's my long-term prescriber — the same one indefinitely, or do I need a backup plan?
When revision surgery, endoscopic revision, or in-person bariatric care beats GLP-1
A GLP-1 can address appetite, weight trajectory, and metabolic markers — but it can't fix anatomy. If your regain is being driven by a dilated pouch or stoma, severe persistent reflux, a band complication, fistula, or another structural issue, revision or endoscopic care is the right conversation, not medication.
Signs the medication conversation is the wrong starting point:
- ✕Severe reflux that's worsened progressively after sleeve, especially with regurgitation, esophagitis, or sleeping symptoms
- ✕Vomiting or inability to keep food down (not just nausea — actual structural intolerance)
- ✕Loss of restriction with rapid regain and noticeably larger meal capacity
- ✕Abdominal pain that's recurring or postprandial
- ✕Dumping or hypoglycemia symptoms that aren't responding to behavioral changes
- ✕Suspected internal hernia, fistula, or band slip
- ✕Significant unexplained malnutrition despite adequate intake
According to a real-world study presented at the ASMBS 2025 Annual Meeting, sleeve gastrectomy and gastric bypass were associated with about five times more weight loss than semaglutide or tirzepatide prescriptions over two years. If a structural issue is driving your regain, that conversation may be worth having again.
Build my specialist-first checklist — get the questions and labs to bring to your bariatric team appointment
→ Build my specialist-first checklistHow to talk to your bariatric team about starting a GLP-1
Re-engage your bariatric surgery or obesity medicine team before starting GLP-1. Bring your surgery type and date, your nadir weight, your current weight, the regain timeline, your current medications, your symptoms, and the specific GLP-1 you're considering. Most teams welcome the conversation.
The appointment goes better when you walk in specific, not defensive.
A 30-second script that works:
"I had [sleeve / RYGB / band / DS] on [date]. My lowest weight was [X] pounds, and I'm now [Y]. Over the past [months/years] I've regained [Z] pounds, and [hunger has returned / I've plateaued / my A1C is up]. I want to discuss whether a GLP-1 medication is appropriate for me, and what labs or anatomy checks you'd want before I start."
Questions worth asking your team
- 1.Is my regain pattern expected or concerning?
- 2.Should we check anatomy (imaging, endoscopy) before I start medication?
- 3.What labs do you want to see before and three months into therapy?
- 4.Are reflux or hypoglycemia concerns specific to my case?
- 5.Would semaglutide, tirzepatide, an oral option, or another agent fit best for me?
- 6.Should I limit myself to FDA-approved, or are there reasons compounded would be appropriate in my case?
- 7.How should we protect my protein intake and muscle mass during weight loss?
- 8.What's the plan if I don't respond — switch agents, escalate care, or revision conversation?
- 9.What's our long-term maintenance plan if I do respond?
Common misconceptions about GLP-1 after bariatric surgery
Five questions we hear repeatedly. Short, direct answers.
"Adding a GLP-1 means my surgery failed."
It doesn't. Surgery did its job — it gave you initial weight loss and metabolic reset most diets can't. Biology adapts over years, and adding medication is treating that adaptation, not undoing the surgery. According to ASMBS 2025 research, bariatric surgery still produces about five times more weight loss than GLP-1 alone over two years, so the surgery's contribution remains the foundation. The GLP-1 is the second tool, not a replacement.
"GLP-1 is unsafe because of my altered anatomy."
Across published post-bariatric studies, side effects have been mostly mild GI symptoms, similar to non-surgical patients, with no severe events specific to post-bariatric anatomy reported in the major retrospective cohorts and the BARI-OPTIMISE RCT. Specific cautions exist (oral peptide absorption after RYGB, reflux risk after sleeve, hypoglycemia with concurrent diabetes meds), but the medication class is well-tolerated when coordinated with your team.
"Insurance won't cover this because I already had surgery."
Frequently the opposite. Your documented bariatric history typically establishes the obesity criteria payers require. Wegovy and Zepbound coverage has expanded for many commercial plans through 2025 and 2026. Use Ro's free GLP-1 Coverage Checker to find out in 60 seconds.
"If I ever stop, I'll regain everything."
You'll likely regain some — published data shows about 0.8 kg per month for newer GLP-1s in the months after stopping (Oxford/BMJ, 2026). But "everything" overstates it. The plan is to treat GLP-1 like any other chronic-disease therapy and not stop without a maintenance strategy in place.
"Compounded is the same as Wegovy or Zepbound, just cheaper."
It isn't. The FDA has issued warning letters to companies that market compounded products as equivalent to FDA-approved drugs. Compounded preparations are made by state-licensed compounding pharmacies under different oversight, and the FDA does not review them for safety, effectiveness, or quality. For medically complex post-bariatric patients, FDA-approved is the more conservative recommendation when an FDA-approved option meets your medical needs.
What we actually verified for this guide
We separated medical claims, regulatory facts, and commercial facts so you can see exactly what was checked.
Medical and regulatory claims verified against primary sources:
- FDA prescribing information and Medication Guides for Wegovy, Zepbound, Foundayo, Ozempic, Mounjaro, Saxenda
- FDA published guidance on unapproved GLP-1 drugs and compounding
- Mok et al., JAMA Surgery 2023 (BARI-OPTIMISE randomized trial)
- Kim et al., JAMA Surgery 2025 (112,858-patient post-bariatric cohort)
- Jamal et al., Obesity Surgery 2024 (sleeve cohort, semaglutide vs. tirzepatide)
- Lautenbach et al., Obesity Surgery 2022; Jensen et al., Obesity Surgery 2023; Kanai et al., 2024
- Manyari et al., Obesity Surgery 2025 systematic review and meta-analysis
- Oxford-summarized BMJ 2026 analysis on post-medication regain
- ASMBS 2025 Annual Meeting research and statements
- Apovian, Zandvakili, Buie, and Norris published interviews (MedCentral, UC News, UChicago Medicine, Duke Health, 2025–2026)
Commercial facts based on public-facing provider pages:
- Ro pricing, formulary, and Coverage Checker availability
- Sesame Care pricing, formulary, provider choice flow, and insurance acceptance
- Hims and Hers FDA-approved formulary post-Novo Nordisk partnership and April 23, 2026 LillyDirect announcement
- Embody pricing, formulary, and HSA/FSA acceptance
- MEDVi pricing, intake form structure, and HSA/FSA acceptance
Refresh schedule: This page is reviewed quarterly at minimum. Pricing is re-checked monthly against public provider pages. Material clinical updates trigger immediate re-verification.
Frequently asked questions about GLP-1 after bariatric surgery
17 questions. Short, direct answers sourced to primary evidence.
Can you take Ozempic after bariatric surgery?▼
Can you take Wegovy after gastric sleeve?▼
Can you take Zepbound after gastric bypass?▼
Is semaglutide safe after gastric sleeve or gastric bypass?▼
How long after bariatric surgery can I start a GLP-1?▼
Will my insurance cover Wegovy or Zepbound after bariatric surgery?▼
What weight loss should I expect with a GLP-1 after bariatric surgery?▼
Can I take a compounded GLP-1 after bariatric surgery?▼
Does gastric bypass affect oral GLP-1 pills?▼
Does Foundayo affect birth control pills?▼
Will I regain weight if I stop my GLP-1?▼
Do I need to tell my bariatric surgeon I'm starting a GLP-1?▼
Is GLP-1 better than revision bariatric surgery for weight regain?▼
Should I take semaglutide or tirzepatide after bariatric surgery?▼
Can GLP-1 medications affect vitamin absorption after bariatric surgery?▼
Can GLP-1 help with food noise after gastric sleeve?▼
Should I choose Ro, Sesame, Embody, or MEDVi after bariatric surgery?▼
Still not sure which GLP-1 program is right for you?
You did the hard part already. The surgery, the recovery, the years of work. Adding a GLP-1 isn't undoing any of that — it's continuing what surgery started. The evidence is real. The path is mappable. And you don't have to figure it out alone.
If you're stable, more than 9–12 months out, and have no red flags from the safety triage above, you have legitimate options — and we've laid them out for you above.
→ Take our free 60-second matching quizWe'll ask about your surgery type, time since surgery, symptoms, insurance, and budget — and route you to specialist-first care, FDA-approved access, or a verified provider match. No checkout. Just the next step that fits.
Internal resources you may also want
- →Compounded vs FDA-approved GLP-1 — the full comparison
- →GLP-1 prior authorization guide — how to actually get insurance approval
- →Best GLP-1 providers — our current verified ranking across all use cases
- →HSA/FSA for GLP-1 medication — what's eligible and how to use it
- →Cheapest GLP-1 without insurance — real cash-pay paths compared
- →Ro GLP-1 pricing and review
- →Eden GLP-1 pricing and review
- →MEDVi GLP-1 cost and review
Sources
- Mok J, et al. Safety and Efficacy of Liraglutide, 3.0 mg vs Placebo in Patients With Poor Weight Loss Following Metabolic Surgery: The BARI-OPTIMISE Randomized Clinical Trial. JAMA Surgery. 2023;158(10):1003–1011.
- Kim et al. Use of GLP-1 receptor agonists among individuals undergoing bariatric surgery in the United States. JAMA Surgery. 2025. (Summarized by Johns Hopkins Bloomberg School of Public Health.)
- Çalık Başaran N, Dotan I, Dicker D. Post metabolic bariatric surgery weight regain: the importance of GLP-1 levels. International Journal of Obesity. 2025;49(3):412–417.
- Jamal et al. Semaglutide and Tirzepatide for the Management of Weight Recurrence After Sleeve Gastrectomy: A Retrospective Cohort Study. Obesity Surgery. 2024.
- Lautenbach A, et al. The Potential of Semaglutide Once-Weekly in Patients Without Type 2 Diabetes with Weight Regain or Insufficient Weight Loss After Bariatric Surgery. Obesity Surgery. 2022.
- Jensen et al. Liraglutide and semaglutide for weight regain after bariatric surgery. Obesity Surgery. 2023.
- Kanai R, et al. Effects of once-weekly semaglutide after laparoscopic sleeve gastrectomy in Japanese patients with type 2 diabetes. 2024.
- Manyari et al. Effects of semaglutide and tirzepatide on recurrent weight gain after bariatric surgery: a systematic review and meta-analysis. Obesity Surgery. 2025.
- Johns Hopkins Bloomberg School of Public Health summary of Kim et al. JAMA Surgery 2025 cohort.
- UT Southwestern Medical Center summary of post-bariatric semaglutide vs. liraglutide cohort (2023).
- ASMBS 2025 Annual Meeting research: bariatric surgery vs. GLP-1 medications.
- Oxford / BMJ analysis on weight regain after stopping weight-loss medication (2026).
- MedCentral: GLP-1s for Weight Loss and Maintenance Post-Bariatric Surgery (March 2026), with commentary from Caroline Apovian, MD, Inuk Zandvakili, MD, PhD, and Disha Narang, MD.
- FDA: FDA's Concerns with Unapproved GLP-1 Drugs Used for Weight Loss.
- FDA: Wegovy, Zepbound, Foundayo, Ozempic, Mounjaro, Saxenda prescribing information (FDA AccessData and DailyMed).
- Hims & Hers newsroom announcement, April 23, 2026: LillyDirect prescription routing for Zepbound and Foundayo.
Weight Loss Provider Guide is an independent comparison resource for GLP-1 telehealth providers. We may earn a commission when readers start a program through links on this page. Our recommendations are based on verified provider data and clinical fit, not commission rate. This page is for informational purposes only and is not medical advice. Coordinate care with your bariatric surgery team or a qualified obesity medicine clinician before starting or changing any medication. · Next scheduled review: July 27, 2026