How to Transfer Your GLP-1 Prescription (2026)
By the WPG Research Team — an independent comparison resource for GLP-1 telehealth providers · · Next scheduled review: monthly · Reading time: ~22 minutes
The bottom line
Most "how to transfer GLP-1 prescription to a new provider" guides bury the answer under 1,500 words of preamble. Here it is up front: you usually can't transfer a GLP-1 prescription the way you transfer a refill from CVS to Walgreens. A new provider almost always has to evaluate you and write a fresh prescription. What actually transfers is your documentation — your current medication, dose, prescription label, last fill date, side effects, labs, and insurance status.
That sounds like bad news. It isn't. The good news is that some GLP-1 telehealth providers have a smooth process for reviewing your current-dose proof so you don't have to start over. The key is showing recent documentation — your name, prescriber's name, medication name and strength, and prescription date — so the new clinician can continue your dose if it's medically appropriate. Final approval is always at the licensed clinician's discretion, but with the right paperwork the friction is low.
If you're keeping the same prescriber and just want a different pharmacy (cheaper, closer, faster delivery), that's a different question with a much simpler answer — we cover both paths below. And if you're moving because your compounded provider just got an FDA warning letter or hiked prices, that's a third situation with its own playbook.
Find your situation in the table below, then we'll walk through the rest in the order your brain actually needs it.
Find your situation first
| Your situation | What you actually need | Where to start |
|---|---|---|
| I want a cheaper or better GLP-1 telehealth provider | Provider switch + proof of current treatment | The records checklist below |
| I like my current prescriber but want a new pharmacy | Pharmacy-to-pharmacy transfer | Pharmacy-only transfers section |
| I want FDA-approved Wegovy, Zepbound, or Foundayo (or Ozempic for diabetes) | Brand-name route + insurance or cash-pay check | Insurance and prior authorization section |
| My compounded provider got a warning letter or shut down | Disruption playbook + path decision | FDA warning section |
| I'm not sure which one applies to me | Personalized 60-second match | Take the free GLP-1 matching quiz → |
Looking for a low-cost option to switch to?
Embody is a cash-pay telehealth GLP-1 program — weekly semaglutide or tirzepatide injections, or a needle-free GLP-1 gum — from $99 for your first month of semaglutide injection, then $299/mo ongoing. Fast online intake with 24/7 support, and medication ships to your door if a provider approves treatment. Compounded GLP-1 medications are not FDA-approved finished drugs.
Check Embody Eligibility →Can you transfer a GLP-1 prescription to a new provider?
Quick answer
Not literally, in most cases. A new clinician needs to evaluate your history and write a new prescription. The thing you actually move is your treatment documentation — and reputable providers will use that documentation to continue your current dose if it's medically appropriate.
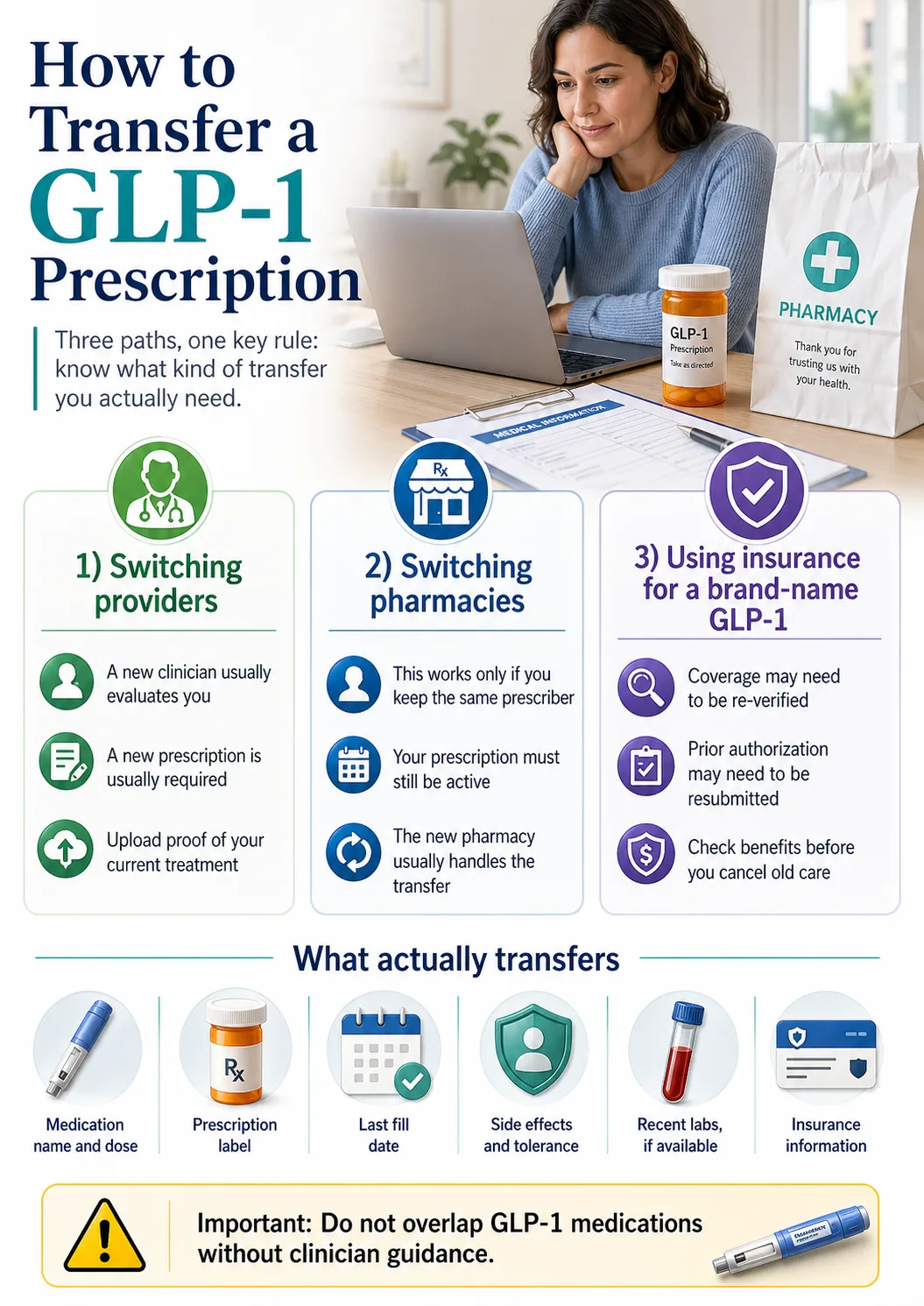
There are three completely different things people mean when they say "transfer my GLP-1 prescription." Mixing them up costs people doses, money, and momentum. So the first job of this guide is to separate them.
Provider switch versus pharmacy transfer versus insurance route
A provider switch is what most people are doing when they search this question. You're leaving Telehealth Company A (Henry Meds, Mochi, Future, your current platform — whoever) and going to Telehealth Company B. This requires a new clinical evaluation and a new prescription. It is not a transfer in the literal sense.
A pharmacy transfer is moving a prescription between fulfillment locations while keeping the same prescriber. If your doctor at Ro writes you a Zepbound prescription and you want to fill it at Amazon Pharmacy instead of CVS, you contact Amazon Pharmacy with the medication name and your current pharmacy and they handle the rest, assuming the prescription has refills available and is transferable. No new doctor visit needed.
An insurance / prior-authorization route is its own beast. Even if your prescription is the same and your medication is the same, switching prescribers can trigger new paperwork from your insurer. Prior authorization (the insurer's coverage decision, separate from the prescription itself) often needs to be re-verified or resubmitted by the new provider.
Before you do anything else, figure out which of these three you actually need. Most of the confusion online happens because writers blur all three together.
What actually transfers (the documentation)
Here's what physically moves with you when you switch GLP-1 providers:
- ✓Your prescription label showing medication, dose, prescriber, and date
- ✓Your last fill date and quantity
- ✓Your dosing schedule (weekly injection day, daily oral, etc.)
- ✓Your side-effect history — what you tolerated, what made you sick
- ✓Your weight history and BMI trend
- ✓Recent labs — comprehensive metabolic panel, HbA1c, anything your last provider ran
- ✓Your insurance card and prior-authorization status if applicable
- ✓Manufacturer savings card or coupon enrollment, if you used one
That's it. That's the package. Build it once, send it to the new provider during intake, and you've done 80% of the work.
Why GLP-1s are easier to "transfer" than people think
Here's a reassuring fact most guides skip: GLP-1 medications are not controlled substances. Semaglutide, tirzepatide, orforglipron, and liraglutide are not scheduled by the DEA. That matters because the strict "one-time-only" prescription transfer rule under 21 CFR 1306.25 that applies to opioids, ADHD stimulants, and other controlled medications doesn't apply to your Wegovy or Zepbound script.
For non-controlled prescriptions, transfer rules are governed by state pharmacy law and are generally permissive. You don't need a court order. You don't need a notary. For a true pharmacy-to-pharmacy transfer, you typically don't need to involve your prescriber at all — though if there are no refills remaining or the prescription has expired, you'll need a new one written. The biggest practical hurdle is just whether your new provider's intake flow makes the documentation handoff easy — which is exactly what the matrix below measures.
The damaging admission (and why it actually protects you)
The frustrating part: a new GLP-1 provider may not just rubber-stamp your old prescription. Their licensed clinician has to look at your dose history, side effects, contraindications, and medication source before writing anything. If you've been on compounded tirzepatide 7.5 mg for nine months, the new provider can't legally call CVS and "transfer" that. They have to evaluate you and prescribe based on their own clinical judgment.
That feels like red tape when you have ten days of medication left.
But it's also the thing that protects you from being prescribed by someone who never reviewed your file. The providers who don't require this — who promise instant approval and ship medication to anyone who pays — are the ones the FDA has been targeting in its enforcement actions. The FDA's March 3, 2026 announcement detailed 30 warning letters to telehealth companies, focused on false or misleading claims about compounded GLP-1 products. The slowness is the safety mechanism. Most reputable providers complete intake review in days, not weeks — Yucca Health says provider review happens within 24 hours, while a compounded provider's full process from approval through compounding and shipping can take several business days.
So the question isn't "how do I avoid the new evaluation?" It's "which provider has the smoothest evaluation process for someone already on a GLP-1 with proof?" That's what the next sections answer.
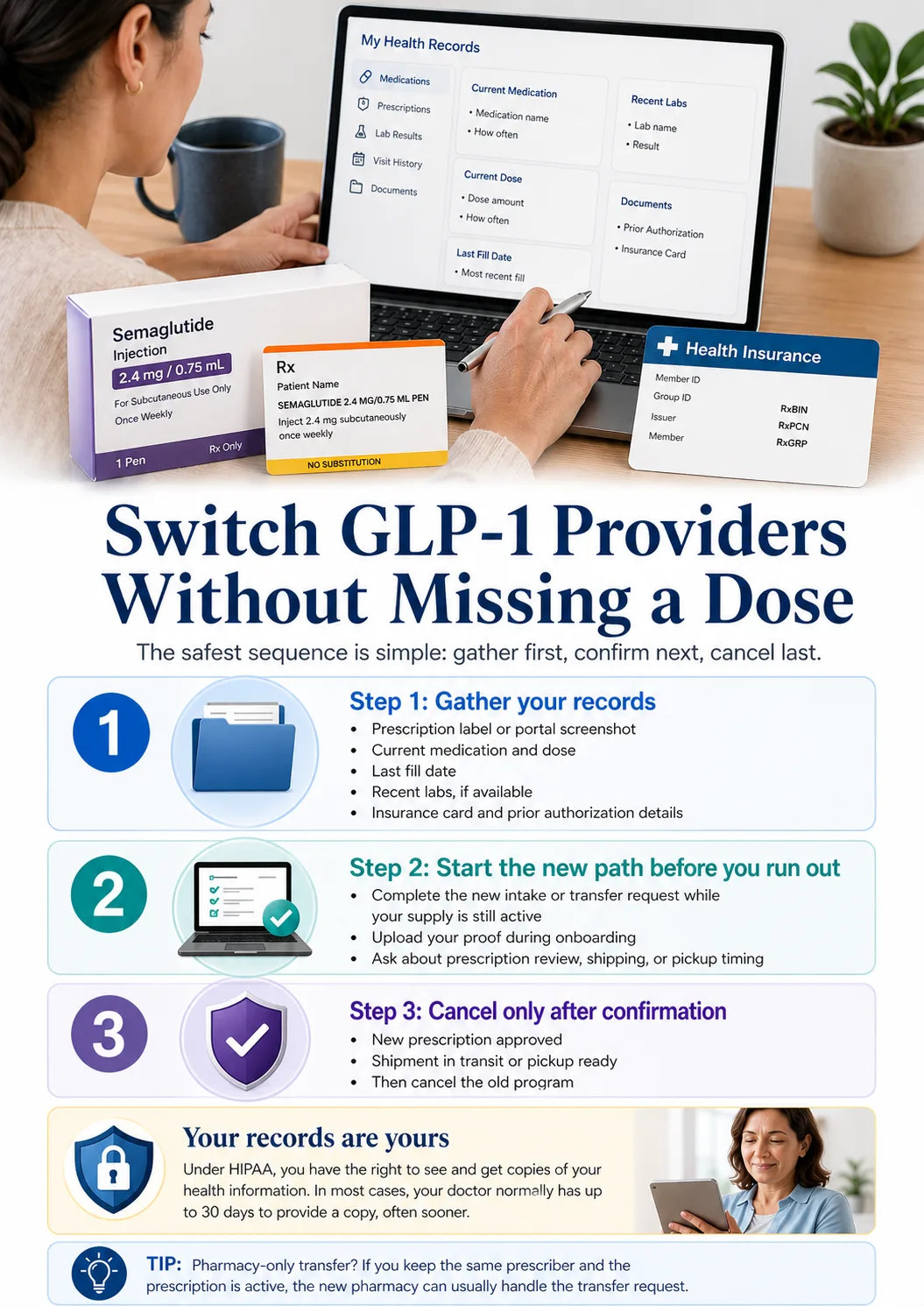
What to gather before you cancel anything
Quick answer
Don't cancel your current provider first. Gather your prescription label, dose history, refill date, labs, side-effect notes, and insurance documents before you start the new intake. You have a federal right under HIPAA to request copies of your treatment records, and most reputable providers send them within days.
This is the single most important paragraph in this whole guide. Read it twice.
Do not cancel your existing GLP-1 program until your new prescription path is confirmed in writing. People do it backwards all the time and end up paying twice or skipping doses while paperwork sorts itself out. The order is: gather → start new intake → confirm new prescription/shipment → then cancel.
The full GLP-1 transfer records checklist
Treatment specifics:
- ✓Current medication name (and whether it's compounded or brand-name)
- ✓Current dose and schedule (e.g., "tirzepatide 7.5 mg weekly, injected Sundays")
- ✓Date of last injection or oral dose
- ✓Date of last fill and quantity received
- ✓Date your next dose is due
- ✓Date you'll run out of medication
Documentation (photograph or screenshot all of these):
- ✓Most recent prescription label
- ✓Medication packaging with the dispensing pharmacy label visible
- ✓Patient portal screenshot showing your active prescription
- ✓Last invoice or receipt from your current provider
- ✓Dosing instructions you were given
Clinical history:
- ✓Side-effect history (nausea, fatigue, GI issues, anything you reported)
- ✓Recent labs if your provider ran them — CMP, HbA1c, lipid panel
- ✓Weight at start of treatment and current weight
- ✓Any other medications you're taking
- ✓Relevant conditions (diabetes, PCOS, obstructive sleep apnea, etc.)
Insurance and billing:
- ✓Insurance card (front and back)
- ✓Prior authorization approval letter, if you have one
- ✓Manufacturer savings card or coupon enrollment, if applicable
- ✓Your current provider's billing date and cancellation deadline
Pro tip the forums get right: screenshot everything before you cancel. Some telehealth providers restrict portal access after cancellation, and pulling records becomes painful. Take five minutes today.
Your right to request your own records
If you can't find something in your portal, you have a federal legal right to request it. Under HIPAA, your provider has up to 30 days to give you copies of your health information, though most respond within days through patient portals. You don't need a reason. You don't need to explain you're switching providers. The records are yours.
Copy-paste template for requesting records
If you need to email your current provider or call their support line:
Hi, I'm transferring my GLP-1 care and need a copy of my current prescription details and treatment records. Please send documentation showing: my medication name, dose and strength, prescribing instructions, prescriber name, the prescription date, the most recent fill date, and any relevant labs or visit notes from the last 12 months. Per my HIPAA rights, I'm requesting these in electronic form within 30 days. Thank you.
Most providers turn this around in a day or two through the portal.
Have your dose proof ready?
Embody is a cash-pay telehealth GLP-1 option for switchers: weekly semaglutide or tirzepatide injections, or a needle-free GLP-1 gum. Share your current medication and dose at intake, and a licensed provider decides whether to continue your dose. From $99 for your first month of semaglutide injection, then $299/mo ongoing; HSA/FSA accepted, no insurance required. (Compounded GLP-1 medications are not FDA-approved finished drugs. Treatment decisions are at the licensed clinician's discretion.)
Check Embody Eligibility →Will the new provider keep you on your current dose?
Quick answer
Some reputable telehealth GLP-1 providers will continue your current dose if you can show recent proof of treatment, but the explicitness of that commitment varies. Final dose approval at any provider is at the licensed clinician's discretion based on your medical history.
This is the question behind the question. Almost everyone searching "how to transfer my GLP-1 prescription" is really asking: will I have to start over at 0.25 mg semaglutide or 2.5 mg tirzepatide and lose six months of titration progress?
The honest answer is "usually not, if you have documentation." The longer answer is the matrix below.
The Provider Switch-In Policy Matrix
We pulled each provider's published switch-in language from their official help center, FAQ, or onboarding flow. Pricing reflects provider-stated rates as of the verification date and is subject to change — confirm at checkout.
| Provider | Switch-in policy | Required proof | Verified pricing | Best fit |
|---|---|---|---|---|
| Embody | Cash-pay intake — share your current medication and dose with documentation; a licensed provider decides whether to continue your dose | Prescription label or pharmacy records showing name, prescriber, medication name, strength, and prescription date | From $99 first month (semaglutide injection), then $299/mo ongoing; tirzepatide injection $149 first → $399/mo; HSA/FSA accepted; no insurance required; weekly injections or needle-free GLP-1 gum; ships to your door if approved | Cash-pay switchers who want a low first-month price plus injection or needle-free gum options |
| MEDVi | Provider-stated — public support page says: "If you're switching from another company and want to stay on the same dosage, we've got you covered" | Submit proof of most recent prescription via portal or email; final approval is provider discretion | $179 first month for compounded semaglutide injection; $299 ongoing; no contract; certain states only | Broad cash-pay switchers; deeper GLP-1 menu including oral tablets |
| Ro | Standard intake medical review (no specific transfer-continuation guarantee published) | Medical history + current Rx info during intake; insurance concierge handles brand-side paperwork | Get started for $39, then as low as $74/month with annual plan paid upfront; medication billed separately; free GLP-1 Insurance Coverage Checker | FDA-approved brand-name (Wegovy, Zepbound, Foundayo) + insurance support |
| Sesame Care | Provider-choice model — clinician reviews history at booked visit | Prior Rx + medical history at visit | Online weight-loss care from $59/month with annual subscription; cash-pay GLP-1 meds from $149/month; insurance accepted for medications | People who want provider choice, video visits, or pharmacy pickup |
| Hims & Hers | Standard intake medical review post-March 2026 Novo Nordisk partnership | Standard intake medical review | Wegovy pill, Wegovy injection, Ozempic injection at all dosage levels; cash-pay from $149/month; not yet in all 50 states | Familiar consumer telehealth brand with FDA-approved Novo Nordisk medication |
| Yucca Health | Async intake; current dose disclosed at intake | Standard intake disclosures | $0 due today, only charged if approved; provider review within 24 hours; lowest first-month price on 6-month plan in our research | Value-conscious switchers who don't want to pay before approval |
| SHED | Compounded specialist — reviews prior treatment history during intake; transfer-specific policy not directly verified | Intake-disclosed | Portal, app tracking, community, text coaching, unlimited follow-ups | Sublingual / oral compounded; needle-averse switchers |
| Enhance MD | Premium clinical model — supports plateau and dose-up transitions; transfer-specific policy not directly verified | Prior treatment history + lab review | Tirzepatide, combo protocols, repeat lab testing built in | People who plateaued on semaglutide and want a stronger clinical protocol |
We verified Embody's cash-pay pricing and medication options from joinem.co and MEDVi's switch-in language from their public member welcome page. For Ro, Sesame, Hims/Hers, Yucca, SHED, and Enhance MD, the matrix shows their general intake approach — final dose approval is always a clinical decision at every provider in this list.
What counts as proof of your current dose
Reputable providers want documentation that clearly shows your name, the medication, the dose, and the date. Here are the documents that work, ranked from strongest to weakest:
- 1Recent prescription label with your name, the drug name, the strength, the dosing instructions, and the fill date — ideally within the last 12 weeks
- 2Pharmacy invoice or receipt showing the dispensing pharmacy, the medication, the dose, and the fill date
- 3Photo of medication packaging with the dispensing pharmacy's label intact
- 4Patient portal screenshot from your current provider showing your active prescription
- 5Most recent invoice from your telehealth provider listing the medication and dose
When a dose reset can still happen
Even with perfect documentation, the new provider's clinician may decide to step you down. The most common reasons:
- ▸You've been off medication for more than 14 days
- ▸You had significant side effects on your current dose
- ▸You're switching medications, not just providers (e.g., compounded semaglutide → branded Zepbound)
- ▸The new provider's protocol uses a different titration ladder
- ▸Something in your medical history changed
- ▸The provider is moving you from oral to injectable or vice versa
This is a feature, not a bug. A provider who never reconsiders your dose isn't reviewing you — they're rubber-stamping you.
The exact thing to say in the new intake
Use this language during your new intake to maximize your chances of dose continuity:
"I'm currently on [medication name and formulation] at [dose] every [schedule]. My last dose was on [date], and my next dose is due [date]. I have a photo of my prescription label and my last invoice ready to upload. I'm switching providers because [brief reason — cost, service, formulation change, insurance change]. I'd like the clinician to review whether continuing at my current dose is appropriate."
Specific. Concise. Sets up the clinician to make the call, not asks them to skip the call.
Want a low-cost option to switch to?
Embody offers weekly semaglutide or tirzepatide injections — or a needle-free GLP-1 gum — on a cash-pay basis with no insurance required. Bring your current medication and dose to intake; a licensed provider decides whether to continue your dose. From $99 for your first month of semaglutide injection, then $299/mo ongoing. Compounded GLP-1 medications are not FDA-approved finished drugs. Treatment decisions are at the licensed clinician's discretion.
Check Embody Eligibility →What to do if there's a gap between providers
Quick answer
If you've been off your GLP-1 for more than two weeks, contact the prescribing clinician before restarting. Some provider protocols step patients down after gaps, and the new clinician will decide whether to resume at your previous dose, lower it, or restart titration based on your medication, time off, side-effect history, and medical context. The shorter your gap, the higher the likelihood of staying at your current dose.
Common provider practice on dose continuation after a gap
Not an FDA rule. A synthesis of how UCLA Health, Mochi Health, and major telehealth providers describe dose decisions after a treatment gap. Decisions belong to the clinician.
| Time since your last dose | What clinicians often consider |
|---|---|
| Less than 14 days | Resume at previous dose with mild side-effect return possible — usually shorter than initial titration |
| 2 weeks – 3 months | Restart at least one dose level below where you stopped is common practice |
| More than 3 months | Restart at the initial titration dose and re-titrate up |
The biology behind it: semaglutide has a half-life of about one week and takes roughly 5–6 weeks to fully clear your system; tirzepatide has a 5-day half-life and clears in 3–4 weeks. So when you're inside the 14-day window, the medication is often still active in your bloodstream and your tolerance is largely intact. The longer the gap, the more conservative most clinicians get.
How to time your switch to stay inside the 14-day window
Most cash-pay programs ship within 5–10 business days of approval. So if you start your new intake while you still have at least 10 days of medication left, you reduce the risk of a gap. Here's the practical sequence:
- 1Day −10 to −14 (relative to running out):Start your new provider's intake. Upload proof during onboarding.
- 2Day −7 to −10:New clinician reviews. Provider review timing varies — Yucca says 24 hours; other providers take longer.
- 3Day −5 to −7:Pharmacy fills the prescription. Compounded pharmacies typically take several business days; brand-name pharmacies often same-day if covered.
- 4Day −2 to −5:Medication ships overnight or 2-day air with cold packs.
- 5Day −1 to 0:Medication arrives. You inject on your normal day. Zero gap.
Most common mistake: starting the new intake the same week you run out. Almost everyone underestimates how long the pharmacy step takes. Build in a buffer.
What if you're already past 14 days
This is fine. Millions of people pause and restart GLP-1s without permanent setback. Expect:
- ✓A mild return of side effects similar to your initial titration — usually shorter
- ✓Some appetite return as the medication ramps back up
- ✓Possibly 2–4 weeks of adjustment before you're back at your prior effectiveness
Do not overlap or stack medications
Important safety note
Zepbound's prescribing information instructs that Zepbound should not be used with other tirzepatide-containing products or with any other GLP-1 receptor agonist medicines. Wegovy carries similar guidance. If you have leftover doses from your old provider and your new provider just shipped fresh medication, do not double up to "make up" for a gap. Use one supply, finish it, then start the next under clinician guidance.
Step-by-step transfer timeline (the 30-day map)
Quick answer
A clean GLP-1 provider switch typically takes 5–10 business days from new intake to first shipment, but plan for 30 days when insurance, prior authorization, labs, brand-name medication, or pharmacy stock issues are involved. Start the new path while your current supply is still active.
The 30-day GLP-1 switch timeline
| Days before you run out | What to do | Why it matters |
|---|---|---|
| 30 days | Choose your route: provider switch, pharmacy transfer, insurance/brand path, or unsure → take the quiz | Prevents rushed payment decisions when you're stressed about supply |
| 21 days | Gather proof of current treatment, portal screenshots, insurance documents, and recent labs | Avoids review delays and dose-step-downs |
| 14 days | Complete the new intake or pharmacy-transfer request; upload everything during onboarding | Gives the clinician and pharmacy time to process |
| 7 days | Confirm prescription approval, shipment tracking, pickup readiness, and any prior-authorization status | Catches problems while you still have time to fix them |
| After confirmation | Cancel old subscription or billing | Prevents double billing and protects continuity |
What slows the switch down (and how to avoid each)
- ▸Missing or unclear proof of current dose → Solve this on Day 30 by photographing every label and pulling every screenshot now
- ▸Insurance prior authorization → Only relevant for brand-name; cash-pay compounded skips it entirely. If you're going branded, run the Ro coverage checker on Day 30 so you know what you're walking into
- ▸State licensing gaps → Confirm the new provider is licensed in your state before paying. State availability varies by provider and by medication; verify at intake
- ▸New labs required → Some providers require labs only if your last set is over 12 months old; premium clinical providers like Enhance MD include lab review by design. Ask at intake
- ▸Compounding turnaround → Compounded providers' full process from approval through compounding and shipping can take several business days; brand-name retail pharmacies are often same-day if covered. Plan around your specific provider's stated timing
The Switch-Without-Gap Checklist (12 items)
- ☐Counted exactly how many days of medication I have left
- ☐Photographed my most recent prescription label, both sides
- ☐Saved my last pharmacy invoice and provider receipt
- ☐Took a screenshot of my current provider's patient portal showing the active prescription
- ☐Noted my last injection or oral-dose date (for the gap-timing question)
- ☐Confirmed the new provider is licensed in my state
- ☐Started the new intake with at least 10 days of medication remaining
- ☐Disclosed my current dose, medication, and last dose date during intake
- ☐Uploaded all proof during onboarding (didn't wait for them to ask)
- ☐Confirmed the new provider's first shipment is in transit before canceling the old one
- ☐Saved my old provider's records before canceling — I might need them later
- ☐Set a calendar reminder for the new provider's billing renewal date
Need a low-cost program to switch to?
Embody is a cash-pay telehealth GLP-1 option — weekly semaglutide or tirzepatide injections, or a needle-free GLP-1 gum — from $99 for your first month of semaglutide injection, then $299/mo ongoing. HSA/FSA accepted, no insurance required, with 24/7 support if a provider approves treatment.
Check Embody Eligibility →If your compounded provider got an FDA warning or shut down
Quick answer
The FDA has been actively enforcing against telehealth companies marketing compounded GLP-1s for false or misleading claims, including 30 warning letters announced on March 3, 2026. If your provider went dark, raised prices sharply, or pivoted to FDA-approved-only options — you have three legitimate paths forward, and the right one depends on whether you want to continue with compounded medication or move to brand-name.
The 2024–2026 enforcement timeline (what actually happened)
- December 19, 2024:FDA declared the tirzepatide shortage resolved
- February 21, 2025:FDA declared the semaglutide shortage resolved
- Early 2025:Enforcement discretion ended for 503A state-licensed pharmacies compounding tirzepatide (March 2025) and semaglutide (April 22, 2025); 503B outsourcing facilities had until May 22, 2025
- Sept 2024 – Mar 2026:FDA issued multiple rounds of warning letters to telehealth companies — including 55+ letters in September 2024 and 30 letters announced March 3, 2026, targeting language like "clinically proven" and claims implying sameness with FDA-approved drugs
- March 2026:Hims & Hers announced direct access to Wegovy pills, Wegovy injections, and Ozempic injections through a Novo Nordisk partnership at cash prices starting at $149/month
- April 2026:FDA clarified that compounded GLP-1 products may qualify under 503A/503B exemptions only when specific conditions are met — including individual patient prescriptions and restrictions on regularly compounding products that are essentially copies of commercially available drugs
Two things are simultaneously true: many compounded providers continue to operate, and the regulatory pressure is real and ongoing. If your provider was sent a warning letter, that is meaningful but not always disqualifying — most warnings target marketing and labeling claims rather than pharmacy manufacturing or medication quality. Read the letter, not the headline.
The three paths forward
Path 1: Stay with compounded medication, but move to a more transparent provider
What "more transparent" looks like in 2026:
- ✓503A pharmacy partner disclosed by name
- ✓No marketing language calling the product "FDA-approved" or "the same as Wegovy/Zepbound"
- ✓Clear visible disclosure that compounded medications are not FDA-approved as finished products
- ✓Real clinician evaluation, not a 30-second checkout flow
For this path, Embody is a strong cash-pay compounded option to check next. Embody offers compounded semaglutide and tirzepatide as weekly injections or a needle-free GLP-1 gum, clearly discloses that its compounded medications are not FDA-approved finished drugs, runs a real clinician intake, and ships to your door if a provider approves treatment — with HSA/FSA accepted and no insurance required. MEDVi remains a strong secondary for people who specifically want oral tablets in addition to injections.
Check Embody Eligibility →Path 2: Move to brand-name, FDA-approved GLP-1 medication
The cash-pay environment got dramatically more favorable in 2025–2026:
- ✓Wegovy injections start at $199/month for first two months at the lowest doses through manufacturer programs (verify current end date at NovoCare)
- ✓Wegovy pills (oral semaglutide) start at $149/month for the lowest doses
- ✓Foundayo (orforglipron, oral) starts at $149/month through Eli Lilly's program (verify current end date)
- ✓Zepbound Self Pay Journey pricing begins around $299/month and rises to $449/month for higher-dose KwikPens, depending on dose and refill timing
- ✓Ozempic 0.25–0.5 mg is available at $199/month for the first two fills through Costco's program through 6/30/26, then $349/month
For this path, Ro is the broadest FDA-approved GLP-1 telehealth provider on the market — they carry Foundayo, Wegovy pill, Wegovy pen, Zepbound pen, and Zepbound KwikPen, match LillyDirect / NovoCare pricing on medication, and include an insurance concierge plus a free GLP-1 Insurance Coverage Checker.
Run the Free Ro Coverage Check →Path 3: Use both — run the free insurance check first, then decide
Most readers in this situation should run a free insurance check before deciding. KFF reported that 19% of firms with 200+ workers covered GLP-1 drugs for weight loss in 2025. If your plan covers Wegovy or Zepbound at a $25 copay, the math beats every cash-pay compounded option. If it doesn't, you keep the compounded path. Either way you've spent five minutes and gained certainty.
Switching from compounded to FDA-approved (and back)
Quick answer
Switching from compounded GLP-1 medication to an FDA-approved brand (or vice versa) is a new clinical and pharmacy path, not a simple transfer. You'll need a new prescription, your treatment documentation, and either insurance approval or a cash-pay brand-name route. A licensed clinician decides the new starting dose after reviewing your prior medication, formulation, dose history, gap timing, and tolerability.
Compounded → brand-name (the more common 2026 direction)
Why people are doing this:
- ✓The regulatory environment around compounded keeps tightening
- ✓Brand-name cash prices dropped meaningfully in 2025–2026 (Wegovy pill at $149/month for lowest doses, Foundayo at $149/month, Zepbound vials/KwikPens from $299 to $449/month depending on dose)
- ✓Insurance coverage is real for some plans; insurance concierge services like Ro's handle the prior-authorization paperwork
- ✓Some people simply want the long-term study data that comes with FDA approval
The right provider for this direction: Ro for the broadest brand formulary plus insurance concierge, Sesame Care for provider-choice and cash-pay pricing, and Hims/Hers for people who want a familiar consumer telehealth brand with FDA-approved Novo Nordisk medication.
Brand-name → compounded (less common but legitimate)
Why people do this:
- ▸Insurance dropped coverage at the start of a new plan year
- ▸Prior authorization was denied
- ▸Even with manufacturer programs, brand-name is unaffordable
- ▸They want a different formulation (oral, sublingual)
The right provider depends on what formulation you want: Embody for a low first-month cash-pay price with weekly injections or a needle-free GLP-1 gum, MEDVi for the deepest menu including oral tablets, SHED for compounded sublingual or oral if needles aren't your thing.
The compliance language we use, and the language we don't
We don't say compounded medications have "the same active ingredient as" or are "clinically equivalent to" FDA-approved drugs. That language is exactly what the FDA flagged in its 30 warning letters announced March 3, 2026. We say: compounded GLP-1 medications are not FDA-approved as finished products. Compounding pharmacies are licensed by state pharmacy boards, but the final compounded product hasn't gone through the FDA's safety, effectiveness, and quality review. If a provider tells you their compounded product is "FDA-approved," that's a signal to leave.
Pharmacy-only transfers (when you're keeping the same prescriber)
Quick answer
If you're keeping the same prescriber and only want a different pharmacy, that's a true pharmacy-to-pharmacy transfer — much simpler than switching providers. Contact the new pharmacy with your medication name, dose, and your current pharmacy's name. The transfer typically completes in a few business days, assuming your prescription is active and has refills remaining.
When this path is right for you
Do a pharmacy-only transfer (not a full provider switch) if:
- ✓Your current prescriber is fine, but their preferred pharmacy is expensive or out of stock
- ✓Your insurance changed and your old pharmacy isn't in network
- ✓You moved and need a closer location
- ✓You want home delivery (Amazon Pharmacy, NovoCare, LillyDirect)
- ✓Your current pharmacy is unreliable on cold-chain shipping
The trick: this only works if you have an active prescription with refills remaining. If you're out of refills, you need a new prescription regardless — which usually means a new provider visit.
How a GLP-1 pharmacy transfer actually works
Amazon Pharmacy
Needs the medication name and your current pharmacy's information to transfer an existing prescription. New prescriptions are sent directly by your doctor. Initiate through their app or website.
CVS
Asks for your name, date of birth, current pharmacy information, prescription information, and the CVS location you want to use. Initiate online, on the app, or by calling the new CVS pharmacy.
Most pharmacy transfers complete within a few business days — allow 1–3 days as a baseline, with the process sometimes taking 2–5 days. The receiving pharmacy contacts the sending pharmacy. You typically don't need to call your old pharmacy or your doctor.
When pharmacy transfers fail (and what to do)
- ▸No refills remain → you need a new prescription from your prescriber
- ▸Prescription has expired → most non-controlled prescriptions expire one year from the date written
- ▸Medication is out of stock at the new pharmacy
- ▸Insurance rejects the new pharmacy (in-network vs. out-of-network)
- ▸Prior authorization is tied to the old pharmacy and needs updating
- ▸Telehealth-bound prescriptions — many telehealth providers send prescriptions to specific partner pharmacies and don't allow external transfers
- ▸State legal restrictions — rare for GLP-1s, but possible
Pharmacy-transfer call script
"Hi, I have an active GLP-1 prescription at [current pharmacy name and phone] that I'd like to transfer to your pharmacy. The medication is [name], my prescriber is [name], and I'm currently on [dose]. Can you confirm whether you can transfer it, whether refills remain, whether you have it in stock, and whether my insurance and prior authorization will process at your pharmacy?"
Switching across state lines
Quick answer
State availability is provider-specific and medication-specific, and changes month to month. Embody has broad U.S. availability but not every state — confirm your state during intake. MEDVi is available only in certain states. Hims/Hers states GLP-1 medications are not yet available in all 50 states. Verify state availability during intake before paying any deposit.
Scenario 1: You moved
You need a new provider that holds a license in your new state. State availability by provider:
- Embody:Broad U.S. availability but not every state; confirm your state during intake
- MEDVi:Services available only in certain states; verify at intake
- Hims & Hers:FDA-approved GLP-1 access available, but not yet in all 50 states
- Ro, Sesame, Yucca, others:Verify state coverage on their pricing or onboarding page; some hide it inside the FAQ
Scenario 2: You split time between two states
Telehealth licensing is per-state, and your prescribing clinician must hold a license in the state where you are physically located at the time of the visit. The practical workaround is picking a provider that's licensed in both your states.
Watch for state exclusions on specific compounded formulations. Some providers exclude certain compounded products in specific states; verify at intake or in the provider's official terms before you commit.
Red flags that should stop your transfer
Quick answer
If a provider offers GLP-1 medication without a real prescription review, hides whether the medication is compounded or FDA-approved, uses "research use" labeling, guarantees approval, or charges nonrefundable fees before any clinical review with no refund if denied — stop. The FDA has issued warnings about products falsely labeled "for research purposes" or "not for human consumption" while being sold directly to consumers.
The cheap, fast, no-questions-asked GLP-1 sites that show up in your Instagram ads are exactly what the FDA has been issuing warnings about. Don't chase price into a place that sells you something it shouldn't be selling at all.
The 12 red flags
- 1"No prescription needed" — illegal for prescription medication
- 2"Research use only" or "not for human consumption" labels on products being sold for weight loss
- 3Guaranteed approval before any clinical evaluation
- 4No clinician review at any point in the flow
- 5No disclosure of which pharmacy fills the prescription
- 6Vague "GLP-1 blend" with no medication name
- 7Compounded medication advertised as "FDA-approved" or "the same as" a brand-name drug
- 8No cancellation terms visible before checkout
- 9For refrigerated injectable medications: no temperature-control or shipping details disclosed
- 10Pressure to buy before any medical review
- 11Charging nonrefundable medication or membership fees before clearly disclosing clinician review, medication type, refund policy, and cancellation terms
- 12Reviews that all sound the same and only appear on the provider's own site
The FDA has explicitly warned about unapproved GLP-1 products falsely labeled "for research purposes" or "not for human consumption" while being sold directly to consumers with dosing instructions. If you see any of those phrases on a site offering you a GLP-1 medication, close the tab.
What we actually verified for this guide
Verified directly (April 27, 2026):
- ✓Embody's cash-pay pricing — from $99 for the first month of semaglutide injection, then $299/mo ongoing — from joinem.co
- ✓Embody's tirzepatide injection pricing ($149 first month, then $399/mo) and needle-free GLP-1 gum option from joinem.co
- ✓Embody's compounded-medication disclosures (not FDA-approved finished drugs) and clinician intake process from joinem.co
- ✓Embody's HSA/FSA acceptance, no-insurance-required model, and broad (not all-50-state) U.S. availability from joinem.co
- ✓MEDVi's switch-in language from their official member welcome page
- ✓MEDVi's 'available in certain states' terms language from their Terms and Conditions
- ✓Ro's pricing structure ($39 first month, $149 ongoing, $74/month with annual prepay) and FDA-approved formulary from ro.co
- ✓Ro's GLP-1 Insurance Coverage Checker functionality from ro.co
- ✓Hims & Hers' Wegovy / Ozempic access announcement and 'not yet in all 50 states' status from their official newsroom
- ✓Sesame Care's online weight-loss program pricing and structure from sesamecare.com
- ✓Amazon Pharmacy's existing-prescription transfer process from pharmacy.amazon.com
- ✓The two-week clinician-contact guidance from UCLA Health
- ✓The Zepbound non-overlap warning from the official FDA-approved Zepbound prescribing information
- ✓HIPAA records-access rights from HHS.gov
- ✓The FDA compounded GLP-1 enforcement timeline from FDA, NCPA, and AJMC public records
- ✓The 30 warning letters announced by FDA on March 3, 2026
- ✓FDA's April 2026 clarification on 503A/503B compounding limits and 'essentially a copy' rules
- ✓The KFF 2025 employer-coverage figure (19% of firms with 200+ workers covering GLP-1s for weight loss)
- ✓21 CFR 1306 controlled-substance scheduling reference confirming GLP-1s are not scheduled
Provider-stated, not independently verified at policy level:
- ~Switch-in / current-dose continuation policies for Ro, Sesame, Hims/Hers, Yucca, SHED, and Enhance MD — described based on each provider's general intake approach, not a published guarantee
- ~Real-time provider response speed — varies by season and individual case
- ~Insurance plan-specific coverage decisions — run the Ro coverage checker for your specific plan
- ~State pharmacy board interpretations of compounding rules — these vary
- ~Each provider's current state availability for specific compounded formulations — these change monthly
Affiliate disclosure: some providers on this page are affiliate partners. We earn a commission if you sign up via our links — at no extra cost to you. Affiliate relationships did not influence the verification methodology, the matrix data, or the sequence in which we present options.
Next scheduled review: monthly for pricing and policy checks; immediate update on any major FDA enforcement action.
Still not sure which GLP-1 program is right for you?
The right switch depends on six variables — your current medication, your current dose, your insurance status, your state, the trigger that made you start searching, and how much medication you have left. We built a tool that takes all of them and gives you back a personalized 3-step plan with the right provider, the proof to gather, the timeline that fits your situation, and the questions to ask before you pay.
It takes about 60 seconds. No email required to see your match.
Want a low-cost cash-pay option to check next?
Embody offers weekly semaglutide or tirzepatide injections, or a needle-free GLP-1 gum, from $99 for your first month of semaglutide injection, then $299/mo ongoing — HSA/FSA accepted, no insurance required, with 24/7 support if a provider approves treatment.
See If You Qualify for Embody →Cash-pay compounded, low first-month price
From $99 first month (semaglutide injection), then $299/mo ongoing; injections or a needle-free GLP-1 gum; HSA/FSA accepted, no insurance required. Compounded GLP-1 medications are not FDA-approved finished drugs. Treatment decisions are at the licensed clinician's discretion.
Check Embody Eligibility →FDA-approved with insurance handled
Wegovy, Zepbound, Foundayo, or Ozempic. Free coverage check. Get started for $39, then as low as $74/month with annual plan paid upfront. Medication billed separately.
Run the Free Ro Coverage Check →Whatever you choose, gather your records first. Don't cancel before the new path is confirmed. And start the new intake with at least 10 days of medication left so you keep your titration progress and your momentum. You've already done the hard part — deciding to switch. The procedural piece is the easy part. Now you have the map.
Frequently asked questions
Can I transfer my GLP-1 prescription to a new provider?▼
Can I transfer my GLP-1 prescription to another pharmacy?▼
Will I have to restart at the starter dose when switching GLP-1 providers?▼
What proof should I upload when switching GLP-1 providers?▼
Should I cancel my old GLP-1 provider before starting the new one?▼
Does prior authorization transfer to a new GLP-1 provider?▼
Can I switch from compounded semaglutide to Wegovy?▼
Can I switch from Wegovy to Zepbound?▼
Can I have two GLP-1 prescriptions at once during a switch?▼
How long does it take to switch GLP-1 providers?▼
Are GLP-1 medications controlled substances?▼
What is the fastest safe way to switch GLP-1 providers?▼
This guide is for informational purposes only and does not constitute medical advice. Always consult a licensed healthcare provider before starting, stopping, switching, or adjusting any prescription medication. Compounded GLP-1 medications are not FDA-approved as finished products. Pricing and availability change — verify current details directly with the provider before enrolling.