GLP-1 Fatigue: Why You’re Tired + What Actually Helps (2026)
By Weight Loss Provider Guide Editorial Team · · Editorial standards · Affiliate disclosure
Weight Loss Provider Guide is an independent comparison resource for GLP-1 telehealth providers. We may earn a commission if you sign up through links on this page at no extra cost to you. Our recommendations are based on verified pricing, policies, and reader fit — not on payouts.
Medical note: GLP-1 medications require a prescription and clinician evaluation. This page is informational and is not medical advice.
The bottom line
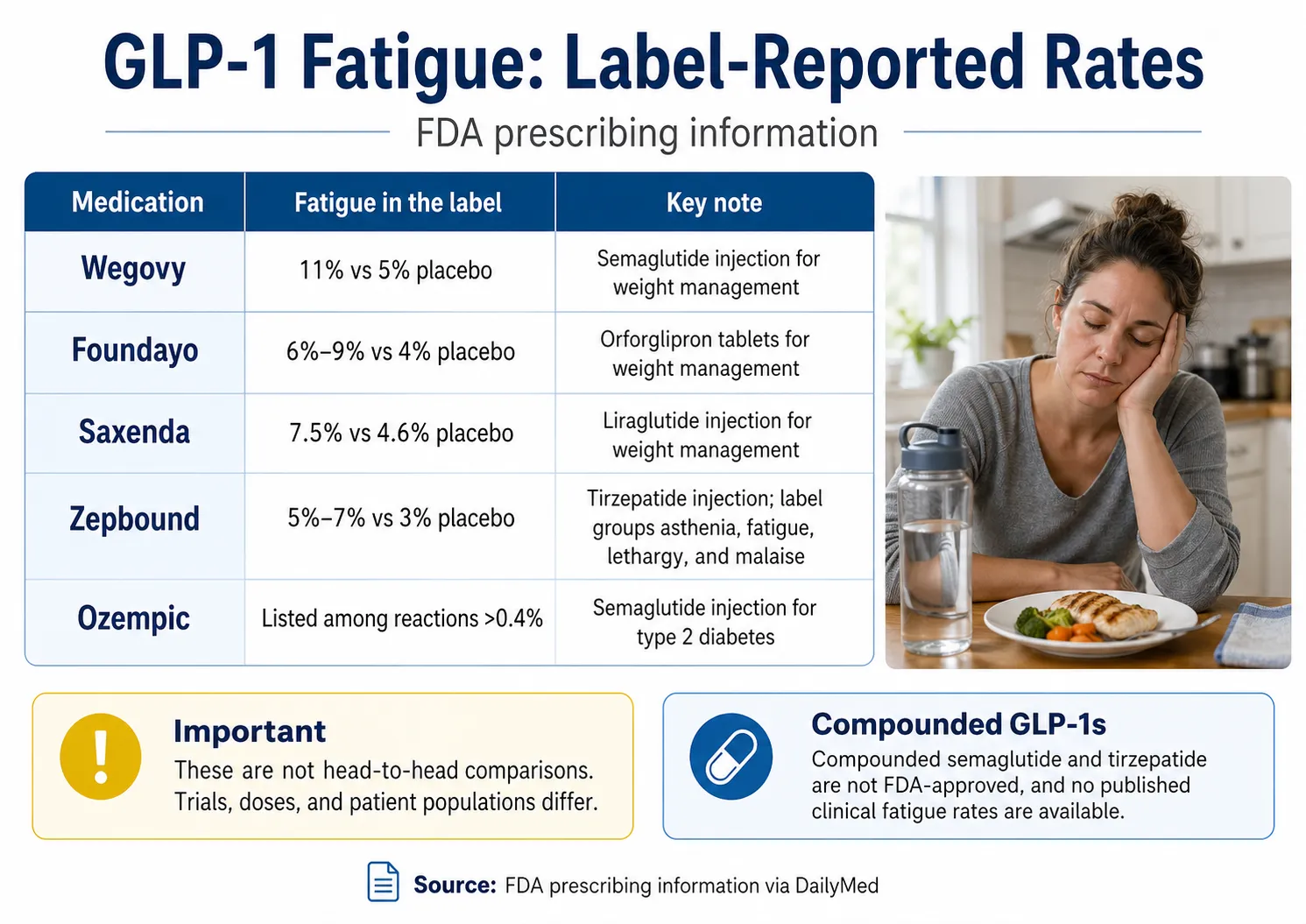
GLP-1 fatigue is real, and it’s listed in the FDA prescribing information for several major GLP-1s. Wegovy reports fatigue in 11% of adults at the 2.4 mg dose vs. 5% on placebo. Foundayo (oral orforglipron) reports fatigue at 6% to 9% depending on dose, vs. 4% on placebo. Zepbound groups asthenia, fatigue, lethargy, and malaise together at 5–7% vs. 3% on placebo. Saxenda reports fatigue in 7.5% of adults vs. 4.6% on placebo. Ozempic, Mounjaro, and Rybelsus don’t list fatigue in their ≥5% common adverse reaction tables.
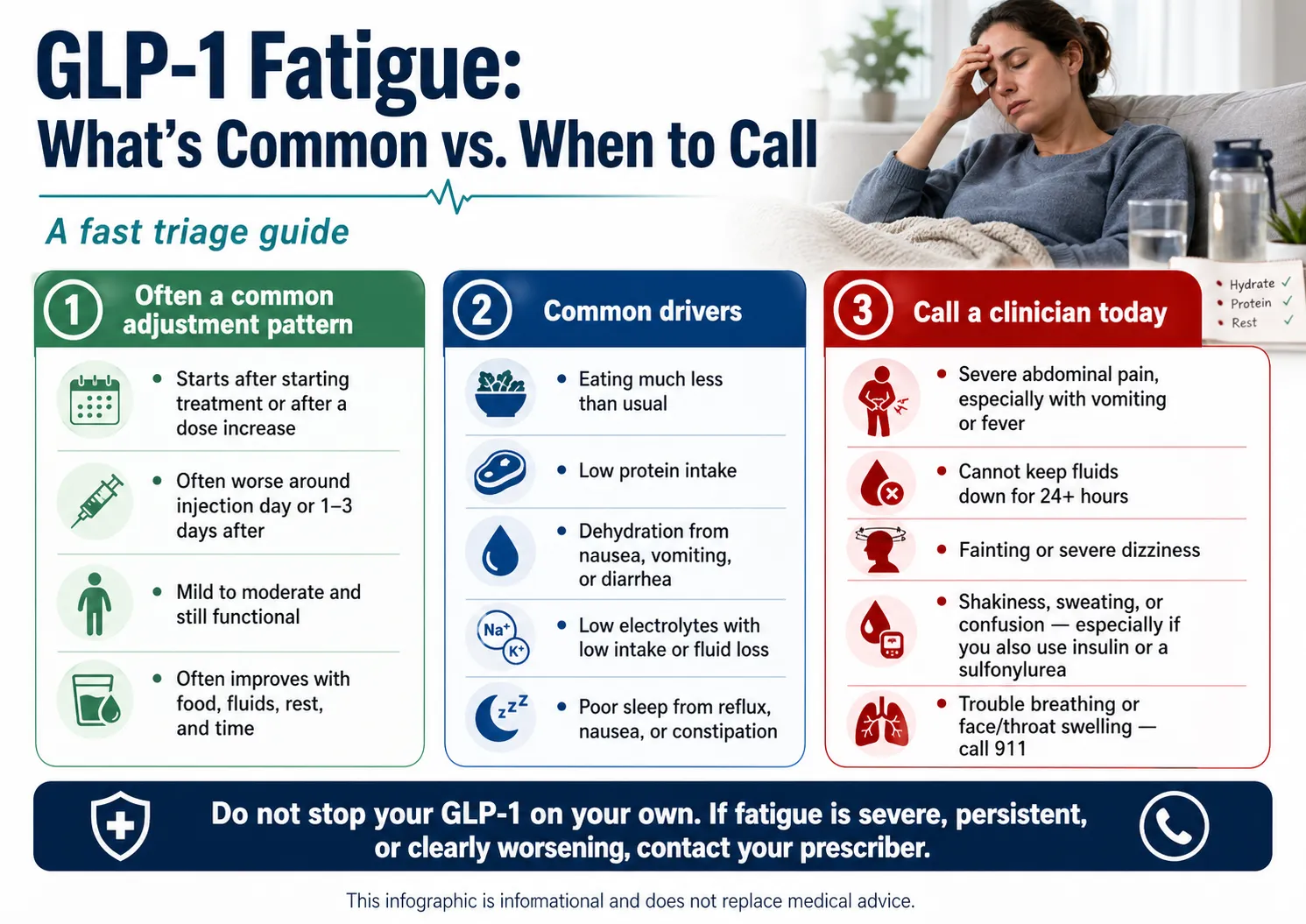
For most people, GLP-1 fatigue clusters around the start of treatment, dose increases, and the day or two after a shot. It’s often indirect — a sudden drop in calories, protein, fluids, and sleep — but it’s also a label-listed adverse reaction, so it’s not “in your head.”
What is not normal: severe fatigue paired with abdominal pain, fainting, persistent vomiting, or shakiness with sweating. That’s a clinician call today, not a wait-it-out problem.
Below: a fatigue-rate comparison that doesn’t exist anywhere else on a single page, the four-pattern framework we use to sort normal from concerning, the 7-day reset that targets the under-fueling pattern most people miss, and what to do if your current provider keeps shrugging you off.
Is this urgent? Read this first.
Before anything else, scan this list. If any of these apply right now, stop reading and contact your prescriber — or seek urgent care if it’s severe.
| If this is happening | What to do |
|---|---|
| Severe abdominal pain, especially radiating to the back, with or without vomiting or fever | Contact your prescriber urgently or seek urgent care. GLP-1 labels warn about pancreatitis and acute gallbladder disease. |
| Persistent vomiting or diarrhea, can’t keep fluids down for 24+ hours, very dark urine, dizziness on standing, fainting | Contact a clinician quickly. Semaglutide and tirzepatide labels warn that GI losses can lead to dehydration and acute kidney injury. |
| Shakiness, sweating, confusion, weakness, fast heartbeat — especially if you also take insulin or a sulfonylurea | Check your glucose if you’ve been instructed to, then contact a clinician. Ozempic’s label specifically flags increased hypoglycemia risk with insulin or sulfonylureas. |
| Difficulty breathing, swelling of the face/throat, severe rash, hives | Call 911. This can be a serious allergic reaction. |
| Suicidal thoughts or significant new depression | Contact a clinician or call/text 988. |
| Mild-to-moderate tiredness with no red flags above | You’re probably in adjustment-pattern fatigue. Keep reading. |
That’s the only triage. Everything else on this page assumes you’ve cleared the red-flag list.
What we actually verified for this page
We’re an independent comparison resource for GLP-1 telehealth providers, and we built this page because the existing GLP-1 fatigue articles either dismiss the problem or bury the answer under 1,500 words of preamble. Here’s what we did before writing:
| What we verified | Source | Result |
|---|---|---|
| Wegovy fatigue rate | DailyMed Wegovy label, April 2026 | 11% (2.4 mg) vs. 5% placebo; 11% (7.2 mg) / 9% (2.4 mg) / 5% placebo in higher-dose study |
| Zepbound fatigue rate | DailyMed Zepbound label, April 2026 | 5–7% fatigue-related events vs. 3% placebo |
| Saxenda fatigue rate | DailyMed Saxenda label, April 2026 | 7.5% adults vs. 4.6% placebo; 4.8% pediatric vs. 3.2% placebo |
| Ozempic fatigue listing | DailyMed Ozempic label, April 2026 | Listed at >0.4% frequency; not in ≥5% common adverse reaction table |
| Mounjaro fatigue listing | DailyMed Mounjaro label, April 2026 | Not listed in the ≥5% common adverse reaction table |
| Rybelsus fatigue listing | DailyMed Rybelsus label, April 2026 | Not listed in the ≥5% common adverse reaction table or postmarketing reactions |
| Foundayo fatigue rate | DailyMed Foundayo label, April 2026 | 6% (5.5 mg), 7% (9 mg), 9% (17.2 mg) vs. 4% placebo |
| Ro pricing & formulary | Ro.com pricing and product pages, April 2026 | Membership tiers and that medication is charged separately |
| FDA guidance on compounded GLP-1s | FDA “Concerns with Unapproved GLP-1 Drugs” page | Compounded GLP-1s are not FDA-approved finished products |
| Searcher language | Public Reddit threads (r/Zepbound, r/Mounjaro, r/Ozempic) | Used as voice-of-customer evidence only |
What we didn’t do: we didn’t pay anyone to review this for credentials we don’t have, we didn’t add a fake “medically reviewed by Dr. X” line, and we didn’t apply FDA-approved brand-name trial data to compounded products as if they’re interchangeable. They’re not.
How common is GLP-1 fatigue on each medication?
Fatigue is most commonly reported on Wegovy (semaglutide 2.4 mg) at 11% of adults in trials, Foundayo (orforglipron) at 6–9% depending on dose, Saxenda (liraglutide) at 7.5%, and Zepbound (tirzepatide) at 5–7%. Ozempic, Mounjaro, and Rybelsus don’t list fatigue in their ≥5% common adverse reaction tables, though Ozempic notes it at >0.4% frequency. Compounded versions don’t have published clinical trial fatigue rates.
Here’s the data side by side, with label citations. This is the comparison that doesn’t exist anywhere else on page one, so we built it.
GLP-1 fatigue rate comparison (FDA prescribing information)
| Medication | Active ingredient | Indication | Reported fatigue rate | Placebo | Source |
|---|---|---|---|---|---|
| Wegovy (2.4 mg injection) | Semaglutide | Weight management | 11% in adults | 5% | DailyMed: Wegovy label |
| Wegovy (7.2 mg study) | Semaglutide | Weight management | 11% at 7.2 mg / 9% at 2.4 mg comparator | 5% | DailyMed: Wegovy label |
| Zepbound | Tirzepatide (injection) | Weight management | 5–7% depending on dose; label groups asthenia, fatigue, lethargy, and malaise together | 3% | DailyMed: Zepbound label |
| Saxenda (adult) | Liraglutide (daily injection) | Weight management | 7.5% | 4.6% | DailyMed: Saxenda label |
| Saxenda (pediatric) | Liraglutide | Weight management (12+) | 4.8% | 3.2% | DailyMed: Saxenda label |
| Foundayo | Orforglipron (oral, daily) | Chronic weight management | 6% (5.5 mg) / 7% (9 mg) / 9% (17.2 mg) | 4% | DailyMed: Foundayo label |
| Ozempic | Semaglutide (injection) | Type 2 diabetes | Listed as >0.4% frequency; not in ≥5% common reactions table | Not separately reported | DailyMed: Ozempic label |
| Mounjaro | Tirzepatide (injection) | Type 2 diabetes | Not listed in the ≥5% common adverse reaction table per current label | — | DailyMed: Mounjaro label |
| Rybelsus | Oral semaglutide | Type 2 diabetes | Not listed in the ≥5% common adverse reaction table or postmarketing reactions per current label | — | DailyMed: Rybelsus label |
| Compounded semaglutide / tirzepatide | Compounded GLP-1s | Off-label | Not FDA-approved. No published clinical trial fatigue rates exist. | — | Not applicable |
A few honest notes on this table
These are not head-to-head comparisons. Each rate comes from a different trial, dose, indication, and patient population. A 5% rate on Zepbound and an 11% rate on Wegovy don’t mean Zepbound is “twice as good” for fatigue — those are different studies with different ground rules.
Compounded products aren’t on this table because they shouldn’t be. Compounded semaglutide and compounded tirzepatide are not FDA-approved finished products. The FDA has not evaluated them for safety, effectiveness, or quality, and there are no published clinical trial fatigue rates to report. If you’re on a compounded GLP-1 and feel exhausted, the practical advice on the rest of this page still applies.
Why GLP-1 medications make you tired
GLP-1 fatigue is often indirect: a sharp drop in calories, missed protein, lower fluid and electrolyte intake, and disrupted sleep from any GI side effects. Fatigue is also label-listed for Wegovy, Foundayo, Saxenda, and Zepbound, so it isn’t only under-fueling — but the indirect causes are the ones you can actually do something about.
Here’s the part that’s easy to miss: the medication is working. Your appetite dropped, you stopped eating constantly, food noise quieted down. That’s the goal. But your daily intake can drop sharply without you noticing, and that gap has to come out of somewhere — usually energy.
| Cause | What it feels like | When it tends to show up | What to track |
|---|---|---|---|
| Under-eating | Brain fog, weakness, irritability, can't power through normal tasks | First 1–4 weeks; after dose increases | Daily calories, meal count |
| Low protein | Muscle weakness, slow recovery from light activity | Anytime appetite is suppressed | Protein grams per meal |
| Dehydration | Lightheaded standing, headache, dark urine, dry mouth | Anytime, worse with GI symptoms | Daily fluid ounces |
| Electrolyte drift | Muscle cramps, weakness, fatigue that water doesn't fix | After GI losses or low intake | Electrolyte intake |
| Sleep disruption from GI symptoms | Wake at 3 a.m., reflux, can't get back to sleep | Anytime; worse after big or late meals | Sleep quality, reflux events |
| Dose escalation | Fatigue spikes after each step up | Days after every titration step | Date of last dose change |
| Direct CNS effect | Less common; baseline tiredness without obvious trigger | Anytime | Pattern over weeks |
JAMA’s patient guidance for adults on GLP-1 therapy points squarely at the indirect causes: protein at every meal, smaller portions more often, slow-digesting carbs, and 2–3 liters of fluids daily for many adults (with individual variation). The Obesity Society’s joint advisory on nutritional priorities during GLP-1 therapy says the same thing in clinical language.
The minor direct mechanism: GLP-1 receptors exist in brain regions that regulate arousal, energy, and sleep-wake signaling. Some researchers believe this contributes to fatigue separately from the eating/hydration cascade above, but a clear direct sedating mechanism hasn’t been established. Address the indirect causes first — those are the ones you can actually move.
Why am I tired the day after my GLP-1 shot?
Many GLP-1 users report a predictable post-injection fatigue window — most often 12 to 48 hours after the shot — that fades later in the week. The mechanism isn’t one thing; it’s usually some combination of peak GI symptoms, lower food and fluid intake, sleep disruption, and the body adapting to the medication’s pharmacokinetics. If your pattern is reliably “wrecked the day after my shot,” your prescriber may be able to discuss shifting injection day so the worst window lands on a day you have more flexibility.
“I get very fatigued for a day or two after my injection. Anyone else?”
“Hit-by-a-truck exhaustion. I genuinely cannot function the day after my injection.”
Semaglutide’s half-life is about a week, so there’s no perfect post-shot recovery window — but the worst day is often 24 to 48 hours in.
What helps:
- Pick a steady injection day and don’t change it without your prescriber’s input
- Keep your worst day as light as possible (don’t pile a heavy work day on top of a hard adjustment day)
- Stack the boring inputs the day before and the day of: protein, fluids, electrolytes, sleep
- Track the pattern for two weeks before deciding it’s the medication and not the rest of life
Could GLP-1 fatigue be low blood sugar?
Fatigue can overlap with low-blood-sugar (hypoglycemia) symptoms, especially if you have diabetes and also use insulin or a sulfonylurea. Ozempic’s label specifically flags increased hypoglycemia risk when used with insulin secretagogues or insulin. If your fatigue comes with shakiness, sweating, confusion, weakness, dizziness, hunger, irritability, or a fast heartbeat, follow your glucose plan and contact your clinician.
You’re at higher hypoglycemia risk if you:
- Use insulin
- Use a sulfonylurea
- Are eating much less than usual
- Recently had a diabetes medication change
- Have type 2 diabetes and started a GLP-1 alongside existing meds
What to do: Check your glucose if you’ve been instructed to do so. Follow your diabetes care plan. Contact a clinician if symptoms are severe, recurring, or confusing. Seek urgent help for severe symptoms — confusion, fainting, inability to treat the low. If you don’t have diabetes and aren’t on insulin or a sulfonylurea, hypoglycemia is much less likely to be the cause of your GLP-1 fatigue.
Could GLP-1 fatigue be dehydration or kidney stress?
Yes, especially if your fatigue comes with vomiting, diarrhea, low intake, dizziness on standing, dark urine, or not urinating much. The Wegovy and Ozempic labels both warn that GI reactions can contribute to dehydration and acute kidney injury, particularly during initiation and dose escalation. This is one of the most important fatigue patterns to catch early — and one of the most overlooked.
Dehydration warning signs to take seriously:
- Very dark urine, or not urinating for many hours
- Dizziness when standing
- Dry mouth, racing heart at rest
- Persistent vomiting or diarrhea
- Inability to keep fluids down for more than 24 hours
- Confusion or significant weakness
What helps when intake is low or you’re losing fluids:
- Sip steadily through the day instead of trying to “catch up” at night
- Add electrolytes (sodium, potassium, magnesium) if you’ve had any nausea, vomiting, or diarrhea
- Get medical input if you can’t keep fluids down, can’t urinate, or feel dizzy on standing — those aren’t “drink more water” situations
If you have kidney disease, heart failure, hypertension, or any sodium restriction, ask your clinician before adding electrolyte powders or changing your hydration strategy. See also: our guide to GLP-1 pancreatitis warning signs for other urgent symptoms on GLP-1 therapy.
How long does GLP-1 fatigue last?
For many people, GLP-1 fatigue is most noticeable during the first few weeks of treatment, in the day or two after a shot, or after a dose increase. It usually improves as the body adjusts and eating patterns stabilize. Fatigue that’s still severe, worsening, or interfering with daily life past the early adjustment period — especially on a stable dose — is a reason to contact your prescriber, not to push through.
| Phase | What many people experience |
|---|---|
| Weeks 1–2 | First fatigue dip as appetite drops and eating patterns haven’t adjusted. |
| Weeks 2–4 | May intensify around the first dose increase; this is the most common “I almost quit” window. |
| Weeks 4–8 | Gradual improvement as eating, hydration, and sleep stabilize. |
| Weeks 8–12 | Many people are significantly better; some feel more energetic than baseline thanks to weight loss and improved metabolic health. |
| Past 12 weeks on a stable dose | Persistent fatigue at this point isn’t a typical adjustment pattern. Time to investigate something else. |
Each new dose escalation can re-trigger a smaller fatigue dip. That’s normal. Saxenda’s label specifically notes that fatigue, asthenia, malaise, and dizziness were mainly reported in the first 12 weeks and were often co-reported with GI events. Zepbound’s label notes that GI adverse reactions occurred more often during dose escalation and decreased over time.
Normal fatigue vs. red-flag fatigue: how to tell
Normal adjustment fatigue
- ✓Starts after starting treatment or after a dose increase
- ✓Often worse around injection day or 1–3 days after
- ✓Mild to moderate and still functional
- ✓Improves when you eat more, drink more, sleep more
- ✓Tied to obvious under-fueling or low-fluid days
- ✓No abdominal pain, fainting, persistent vomiting, or other red flags
Red-flag — talk to a clinician today
- ⚠Severe persistent abdominal pain (especially radiating to the back) — possible pancreatitis
- ⚠Right upper abdominal pain with fever or yellowing of skin/eyes — possible gallbladder problem
- ⚠Inability to keep fluids down for 24+ hours
- ⚠Fainting, near-fainting, or significant lightheadedness on standing
- ⚠Shakiness, sweating, confusion — especially with insulin or a sulfonylurea
- ⚠Heavy, dark urine + dry mouth + dizziness — severe dehydration
- ⚠Severe, persistent fatigue past 12 weeks on a stable dose
- ⚠Suicidal thoughts or significant new depression
The 7-day GLP-1 Energy Reset
This isn’t a treatment protocol — it’s a structured way to test the four boring variables that drive most adjustment-pattern GLP-1 fatigue: hydration, protein, meal cadence, and sleep. By day 7, you’ll either feel meaningfully better (you were under-fueled) or you won’t (in which case the issue is probably dose-related or something a clinician needs to look at).
We built this as a sequence because that’s how it actually works. Most people read a fatigue article, try to do everything at once on day 1, and burn out by day 3. Stack the levers one at a time.
Hydration baseline
Get to 64 ounces of water minimum. Add electrolytes (sodium, potassium, magnesium) if you've had any nausea, vomiting, diarrhea, or just generally low intake. The goal isn't 128 oz of plain water; it's fluid your body can actually use. If you have kidney disease, heart failure, hypertension, or any sodium restriction, ask your clinician before adding electrolyte powders.
Add the protein anchor
Pick one repeatable protein-forward meal — usually breakfast or lunch — and hit 25–30 grams of protein in that meal. If a full meal feels like too much, split it across two mini-meals. Greek yogurt, eggs, a protein shake, cottage cheese, turkey slices, chicken. Protein is the variable that quietly slips when appetite drops, and it's the single biggest lever for adjustment fatigue. JAMA's GLP-1 patient guidance backs this up: 20–30 grams per meal, working toward roughly 1.0–1.5 g/kg/day.
Meal cadence over meal size
Even when you don't feel hungry, try four to five small touches through the day instead of trying to hit one or two big meals. A Greek yogurt at 10. A protein shake at 2. A few eggs at 6. Steady small inputs beat a heroic dinner you can't actually finish.
Movement minimum
A 15–20 minute walk, ideally outside. Light movement reliably increases energy in adjustment-fatigue patterns; intense workouts during peak adjustment weeks usually make fatigue worse, not better. Save the heavy training for week three or four.
Sleep audit
Note what's actually disrupting your sleep. Reflux from going to bed too full? Late caffeine? Nausea waking you up? Constipation discomfort? Fix the obvious one. If reflux has shown up since starting your GLP-1, don't eat within 2 hours of bedtime, and prop the head of your bed up a few inches. Sleep is where most GLP-1 fatigue actually compounds.
Dose timing review
Look at when you're injecting and whether your worst fatigue days overlap with your hardest life days. If shot day reliably lands on your Monday meeting marathon, consider asking your prescriber about shifting to a Friday injection. This is a clinical conversation, not a unilateral change.
Assess and decide
Compare how you feel today vs. day 1. Meaningfully better? You were under-fueled. Still flat? The issue is probably dose-related or something a clinician needs to look at. Bring your 7-day log to your next provider message or appointment. Specific data gets specific answers.
Should you stop your GLP-1 if you’re exhausted?
Almost never on your own. Most GLP-1 adjustment fatigue resolves with hydration, protein, slower titration, and time. Abrupt discontinuation has consequences — especially if the medication is treating type 2 diabetes — and red-flag symptoms need a clinician’s evaluation, not a unilateral stop.
Here’s what your prescriber may consider:
- Slowing titration — extending each dose level for an extra 2–4 weeks
- Holding the current dose for longer before the next increase
- Reducing the dose to the previous step
- Switching to a different GLP-1 (some patients tolerate tirzepatide better than semaglutide, or vice versa)
- Pausing the medication temporarily with a structured plan to restart
- Running labs to rule out thyroid, iron, B12, electrolyte, or kidney issues
- Addressing the GI side effects directly — anti-nausea medication, stool softeners, dietary changes
- Reviewing your other medications — some combinations make fatigue worse
The one exception: if your fatigue is paired with a red-flag symptom from the triage list at the top of this page — severe abdominal pain, fainting, or persistent vomiting — stop reading articles and call your prescriber or seek urgent care today. There is no “track for 48 hours” answer for those symptoms.
If you’ve worked through the 7-day reset and your fatigue isn’t budging — or your current provider isn’t willing to slow your titration or run labs — that’s not your problem to solve alone.
Take the free 60-second matching quiz →We’ll point you to a GLP-1 program that fits: slower titration, lab-supported care, or FDA-approved options. No email required.
What if your provider isn’t responsive?
A good GLP-1 program shouldn’t treat disabling fatigue as a vague inconvenience. If your provider is slow to respond, dismissive, or unwilling to engage with specifics, document your symptoms, ask specific questions, and start considering whether you need a program with better clinical support.
This is the moment a lot of people search “GLP-1 fatigue” — not because they don’t know what to do, but because their provider has stopped helping them figure it out. Here’s the checklist we use to evaluate whether a GLP-1 program is set up to actually support a patient through side effects:
| Support feature | Why it matters for fatigue |
|---|---|
| Easy provider messaging (in-app or email) | Fatigue can change quickly after dose escalation; you need clinician input within 24–48 hours, not “next available appointment in 3 weeks.” |
| Clear red-flag instructions in writing | The reader needs to know which symptoms are urgent before they hit them. |
| Documented dose-adjustment pathway | Some fatigue patterns require titration changes. The provider should have a process for this. |
| Nutrition guidance available | Under-eating is a common driver. A program that hands you a script and walks away is worse than one with even basic dietitian support. |
| Lab access or referral guidance | Persistent fatigue past 12 weeks may need evaluation. The program should help you get labs, not shrug. |
| Pharmacy transparency (especially for compounded) | If you’re on a compounded product, knowing whether it’s coming from a 503A or 503B facility actually matters. |
| Clear cancellation and refill policies | If you decide the program isn’t a fit, you shouldn’t be locked in. |
If your current program checks two or fewer of these, that’s a signal. A side effect this common shouldn’t put you in a customer-service standoff.
Copyable provider message — paste this into your patient portal
Generic “I’m tired” messages get generic “drink water” responses. Specific symptom logs get specific clinical answers. Use this template:
That message takes 3 minutes to fill out and gets a 10× better response than “I’m so tired, what should I do.”
You don’t have to stay with a provider who treats this as your problem to solve.
Take the free 60-second matching quiz →We’ll point you to a GLP-1 program built around the support you actually need — slower titration, lab work, microdose flexibility, FDA-approved options, or compounded with clear pharmacy transparency. No email required to see results.
What real users say (voice of customer, not medical evidence)
We pulled these from public Reddit threads in the Zepbound, Mounjaro, and Ozempic communities. They’re searcher language — this is how people describe GLP-1 fatigue when talking to other patients, not to doctors. We’re including them because if you’ve felt any of this, it helps to know you’re not the only one. We are not using these as medical evidence for safety, frequency, or treatment effect.
“I get very fatigued for a day or two after my injection. Anyone else?”
“It takes about 12 hours after my shot before I get tired, and then I’m wiped for the next day.”
“Hit-by-a-truck exhaustion. I genuinely cannot function the day after my injection.”
Source note: These are public forum snippets used to illustrate how patients describe GLP-1 fatigue. They are not clinical evidence. Individual experiences vary, and these quotes do not establish typical results, safety, or efficacy.
Frequently asked questions
Still not sure which GLP-1 program is right for you?
If you’ve worked through the 7-day reset and your fatigue isn’t budging — or your current provider isn’t willing to slow your titration, run lab work, or actually respond when you flag side effects — that’s not your problem to solve alone.
Take the free 60-second matching quiz →We’ll point you to a GLP-1 program that fits your situation: slower titration, microdose flexibility, lab-supported care, FDA-approved medication with insurance support, or compounded options if that’s your preference. No spam. No pressure.
Disclosure: Weight Loss Provider Guide is an independent comparison resource for GLP-1 telehealth providers. We may earn a commission when readers connect with partner providers through our links. We don’t take payment for editorial placement, and we don’t recommend a provider over another to influence clinical decisions about a side effect. Our job is to help you find a program that actually fits — not to push a specific one.
Sources
- Wegovy (semaglutide injection) prescribing information — DailyMed, last verified April 25, 2026
- Zepbound (tirzepatide injection) prescribing information — DailyMed, last verified April 25, 2026
- Saxenda (liraglutide injection) prescribing information — DailyMed, last verified April 25, 2026
- Ozempic (semaglutide injection) prescribing information — DailyMed, last verified April 25, 2026
- Mounjaro (tirzepatide injection) prescribing information — DailyMed, last verified April 25, 2026
- Rybelsus / oral semaglutide prescribing information — DailyMed, last verified April 25, 2026
- Foundayo (orforglipron tablet) prescribing information — DailyMed, last verified April 25, 2026
- FDA: “FDA’s Concerns with Unapproved GLP-1 Drugs Used for Weight Loss”
- FDA: Information for Outsourcing Facilities (503B)
- JAMA Internal Medicine: “I Am Taking a GLP-1 Weight-Loss Medication — What Should I Know?”
- The Obesity Society joint advisory: “Nutritional Priorities to Support GLP-1 Therapy for Obesity”
- Ro pricing and product pages — Ro.com, last verified April 25, 2026
- Public Reddit threads (r/Zepbound, r/Mounjaro, r/Ozempic) — used as voice-of-customer evidence only
This page was researched and written by the Weight Loss Provider Guide editorial team. This is informational content, not medical advice. Talk to your prescriber about your specific situation.