GLP-1 and Hypoglycemia: 2026 Insulin & Sulfonylurea Risk Guide
Call 911 immediately if someone is unconscious, seizing, or unable to swallow safely.
Use a glucagon rescue kit (Baqsimi, Gvoke) if available. Do not attempt to give food or liquid to someone who cannot swallow.
The bottom line on GLP-1 and hypoglycemia
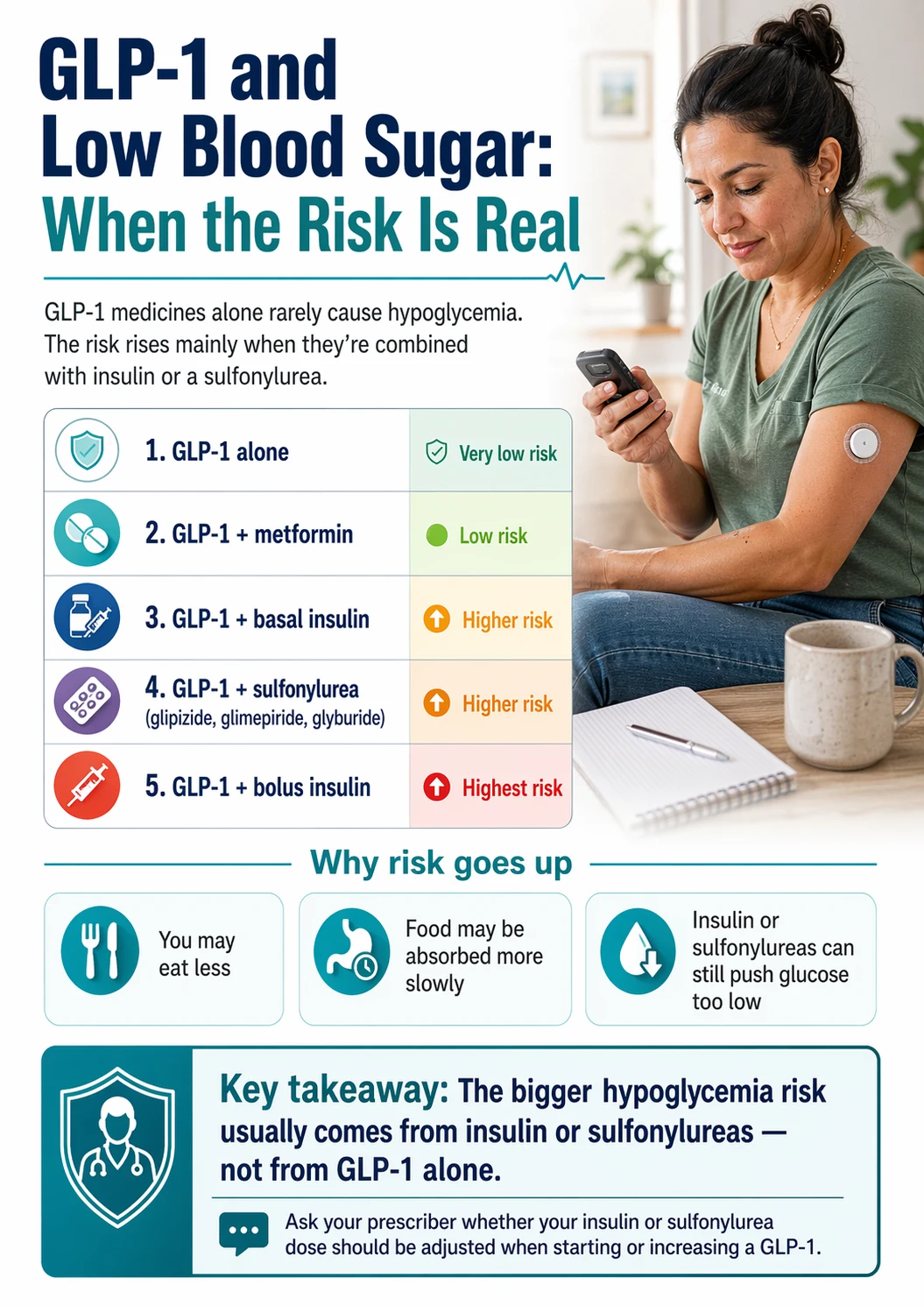
A GLP-1 medication by itself rarely causes low blood sugar. The risk becomes meaningful when a GLP-1 is combined with insulin or a sulfonylurea — glipizide, glimepiride, glyburide. FDA labels for Ozempic, Wegovy, Mounjaro, Zepbound, Rybelsus, and Foundayo all warn about this. In Ozempic's monotherapy trials, documented symptomatic hypoglycemia (≤70 mg/dL) occurred in 1.6–3.8% of patients. In combination settings, rates climb to 17–30%. Prescriber-supervised dose reduction of the insulin or sulfonylurea is the standard response.
Who needs to pay attention — quick scan
| Your situation | Realistic hypoglycemia risk |
|---|---|
| GLP-1 alone, no diabetes | Very low |
| GLP-1 + metformin only | Low |
| GLP-1 + basal insulin | Meaningful Label examples: Ozempic 16.7–29.8% (documented symptomatic ≤70 mg/dL), Mounjaro 14–19% (<54 mg/dL) |
| GLP-1 + sulfonylurea (glipizide, glimepiride, glyburide) | Meaningful Label examples: Ozempic 17.3–24.4% (≤70 mg/dL), Mounjaro 9.9–13.8%, Zepbound 10.3%, Foundayo 7% (<54 mg/dL among SU users) |
| GLP-1 + rapid-acting / bolus insulin | High complexity — dose adjustments and CGM strongly recommended |
| GLP-1 + no diabetes meds, but eating very little due to nausea | Variable Usually symptoms, not true lows |
| Rates above come from different trials with different definitions and populations. Use them to see the combination pattern, not to rank drugs. Sources: FDA prescribing information via DailyMed. | |
If you're in the top two rows, this page is context. If you're in the bottom four, it's a pre-appointment briefing — read it before your next prescriber conversation.
Can GLP-1 medications cause low blood sugar by themselves?
Not usually. GLP-1 drugs work in a glucose-dependent way. The medication only nudges your pancreas to release insulin when your blood sugar is high enough to need it. As blood sugar approaches normal, the effect tapers off. That built-in off-switch is why GLP-1s have a reputation for being "safe" on blood sugar.
In Ozempic's FDA trials of patients with type 2 diabetes using the drug alone or with metformin, documented symptomatic hypoglycemia (blood glucose ≤70 mg/dL with symptoms) occurred in 1.6–3.8% of patients depending on dose. Severe hypoglycemia — the kind requiring someone else's help — was essentially 0%. Mounjaro, Wegovy, Zepbound, Rybelsus, and Foundayo labels show the same low-monotherapy pattern.
So where does the fear come from? Two places. First: people combine GLP-1s with insulin or sulfonylureas, and those drugs don't have a glucose-dependent off-switch. Second: GLP-1 side effects — nausea, dizziness, fatigue, sometimes a fast heartbeat — overlap with hypoglycemia symptoms. A lot of "I had a low on Ozempic" stories are really "I felt weird and assumed it was a low" without a confirmed fingerstick or CGM reading.
Why GLP-1 + insulin or sulfonylureas raises the risk
GLP-1 medications reduce the amount of glucose your body needs to handle — they slow stomach emptying, shrink appetite, dial down glucagon, and over time improve insulin sensitivity. If your insulin or sulfonylurea dose was calibrated for your pre-GLP-1 body, it can now be too strong. Sulfonylureas specifically stimulate insulin release independently of blood sugar, which is why GLP-1 labels repeatedly warn that combining them raises hypoglycemia risk.
Slower gastric emptying
GLP-1s hold food in your stomach longer. Glucose trickles in instead of arriving in a wave. But your mealtime insulin doesn't know that — it was timed for the old arrival curve. Insulin peaks before glucose does, and you crash.
Smaller meals
You're eating less. But if your insulin or sulfonylurea dose still assumes the meal you used to eat, you've got excess glucose-lowering for the glucose that actually shows up.
Suppressed glucagon
Glucagon is your body's "raise blood sugar" hormone — the one that pulls glucose out of the liver when you're running low. GLP-1s suppress it. When something else (insulin, a sulfonylurea) is also driving glucose down, the normal recovery brake is weaker.
Sulfonylureas force insulin release regardless of blood sugar
This is the one specific to sulfonylureas. Sulfonylureas stimulate insulin secretion whether your glucose is high, normal, or low. The GLP-1's glucose-dependent "off-switch at normal blood sugar" can't save you from a drug that doesn't have one. This is why metformin + GLP-1 is low-risk, but glipizide + GLP-1 is meaningfully higher risk even though both are "diabetes pills."
This is the reason every FDA label for the class doesn't just say "monitor" — it says consider reducing the insulin or sulfonylurea dose before you start. The risk is predictable enough that the fix is prospective, not reactive.
GLP-1 and hypoglycemia risk matrix — by medication combination
Last verified:Your risk depends less on which GLP-1 you're on and more on what else you're taking. Here's how to find your category — and what it changes about your prescriber conversation.
| Your regimen | Risk level | What the label data shows | First question to ask your prescriber |
|---|---|---|---|
| GLP-1 only, no diabetes meds | Very low | Ozempic monotherapy: 1.6–3.8% documented symptomatic ≤70 mg/dL. Severe: ~0%. | "Do I need to monitor glucose at all — and under what circumstances?" |
| GLP-1 + metformin | Low | Metformin doesn't drive insulin release. Combined risk similar to GLP-1 alone. | "Do I need extra monitoring during GLP-1 titration?" |
| GLP-1 + sulfonylurea | Meaningful | Ozempic + SU: 17.3% (0.5 mg) to 24.4% (1 mg) documented symptomatic ≤70 mg/dL. | "Should my sulfonylurea be reduced or stopped before I start the GLP-1?" |
| GLP-1 + basal insulin | Meaningful | Ozempic + basal insulin: 16.7–29.8% documented symptomatic ≤70 mg/dL. | "How much should my basal insulin be reduced at GLP-1 initiation?" |
| GLP-1 + bolus (mealtime) insulin | High complexity | Requires carb-ratio and correction-factor review on top of basal adjustments. | "Can we review my pump or bolus doses before I start?" |
| GLP-1 + insulin + sulfonylurea | Highest | ADA 2026 recommends limiting or discontinuing sulfonylureas when therapy is intensified. | "Can we simplify — drop the sulfonylurea and adjust insulin?" |
| GLP-1 alone, eating little due to nausea | Variable | Mostly symptomatic (feels like a low) rather than true lows. A meter check tells you. | "At what symptom threshold should I call you vs. check a fingerstick?" |
| Notice the pattern: the GLP-1 isn't the danger. The other drug in the combination is. That's why every fix centers on adjusting the other drug, not the GLP-1. | |||
What the FDA labels show — hypoglycemia rates across every major GLP-1
Last verified:Ozempic® (semaglutide) — approved for type 2 diabetes
| Setting | Severe hypoglycemia | Documented symptomatic ≤70 mg/dL |
|---|---|---|
| Monotherapy (placebo / 0.5 mg / 1 mg) | 0% / 0% / 0% | 0% / 1.6% / 3.8% |
| Add-on to basal insulin ± metformin | 0% / 0% / 1.5% | 15.2% / 16.7% / 29.8% |
| Add-on to a sulfonylurea (0.5 mg / 1 mg) | 0.8% / 1.2% | 17.3% / 24.4% |
| Source: Ozempic prescribing information, DailyMed. | ||
Mounjaro® (tirzepatide) — approved for type 2 diabetes
| Setting | Severe hypoglycemia | Blood glucose <54 mg/dL |
|---|---|---|
| Monotherapy (placebo / 5 / 10 / 15 mg) | 0% across all groups | 1% / 0% / 0% / 0% |
| Add-on to basal insulin ± metformin | 0% / 0% / 2% / 1% | 13% / 16% / 19% / 14% |
| Used with sulfonylurea, up to 104 weeks (5 / 10 / 15 mg) | 0.5% / 0% / 0.6% | 13.8% / 9.9% / 12.8% |
| Source: Mounjaro prescribing information, DailyMed. | ||
Wegovy® (semaglutide) — approved for chronic weight management
In adults with type 2 diabetes and BMI ≥27 in the weight-reduction trial: clinically significant hypoglycemia (<54 mg/dL) occurred in 6.2% of patients on Wegovy vs. 2.5% on placebo. One severe episode requiring IV glucose occurred in a Wegovy-treated patient; none on placebo.
Source: Wegovy prescribing information, DailyMed.
Zepbound® (tirzepatide) — approved for chronic weight management
- Plasma glucose <54 mg/dL: 4.2% on Zepbound vs. 1.3% on placebo (type 2 diabetes trial).
- Among patients also using a sulfonylurea: 10.3%.
- Among patients not using a sulfonylurea: 2.1%.
- Adults without type 2 diabetes (Study 1): 0.3% vs. none on placebo.
Source: Zepbound prescribing information, DailyMed.
Rybelsus® (oral semaglutide) — approved for type 2 diabetes
The Rybelsus label warns that using the medication with insulin secretagogues (such as sulfonylureas) or insulin may increase the risk of hypoglycemia, including severe hypoglycemia, and recommends considering a lower dose of the concomitant sulfonylurea or insulin to reduce the risk. Same add-on hypoglycemia warning framework as Ozempic.
Source: Rybelsus prescribing information, DailyMed.
Foundayo® (orforglipron) — approved for chronic weight management, April 2026
NEWFoundayo is the first oral, non-peptide GLP-1 receptor agonist. In the weight-management trial of adults with type 2 diabetes and BMI ≥27:
- Plasma glucose <54 mg/dL: 2% on Foundayo vs. 0.2% on placebo.
- Among patients also using a sulfonylurea: 7%.
- Among patients not using a sulfonylurea: 0.5%.
- Adults without type 2 diabetes: 0.6% vs. none on placebo.
Source: Foundayo prescribing information and FDA approval materials, April 2026.
How to treat low blood sugar on a GLP-1 (15-15 rule and when to call 911)
Nobody reads this section because they're curious. They read it because something is happening or just happened. Keeping it practical.

ADA recommendation:
If blood glucose is under 70 mg/dL and you can swallow safely, use the 15-15 rule: 15 grams of fast-acting carbohydrate, wait 15 minutes, recheck. Repeat if still low. CDC describes blood sugar below 55 mg/dL as severely low and notes it may require glucagon or emergency help rather than standard 15-15 alone.
Mild to moderate low (60–70 mg/dL, awake, able to swallow)
- 1
Check if you can.
If you have a meter or CGM, confirm the low. Symptoms without a reading can fool you — especially on a GLP-1.
- 2
Eat 15 grams of fast-acting carbohydrate.
Examples that hit ~15 g: 3–4 glucose tablets, 4 oz of fruit juice (half a typical juice box), 4 oz of regular soda (not diet), 1 tablespoon of honey or sugar, 5 hard candies (Life Savers), 2 tablespoons of raisins.
Chocolate, nuts, and cookies are slow-acting — save them for the stabilization snack after recovery, not first-line treatment.
- 3
Wait 15 minutes.
Don't pile on more carbs in that window. This is the hardest part — you feel awful and want to eat more. Wait.
- 4
Recheck.
If still under 70 mg/dL, repeat steps 2–3. If still under 70 after two cycles, call your prescriber or go to urgent care.
- 5
Once back above 70, eat a stabilization snack.
Protein + carbs: cheese and crackers, half a peanut butter sandwich, a yogurt.
Blood sugar under 55 mg/dL
CDC describes this as severely low. Follow your prescribed low-glucose treatment plan. Very low readings may require glucagon or emergency help rather than oral glucose alone. Confirm the specific threshold and amount with your prescriber before you need it.
Call 911 immediately if someone is unconscious, seizing, or unable to swallow safely.
Use a glucagon rescue kit (Baqsimi, Gvoke) if available. Do not attempt to give food or liquid to someone who cannot swallow.
Glucagon: Baqsimi, Gvoke, or traditional injection kit
Family members and close coworkers should know where it is and how to use it. If you're on insulin or a sulfonylurea and you've ever had a severe low — or you live alone, sleep alone, or have hypoglycemia unawareness — ask your prescriber for a glucagon prescription.
Is this a GLP-1 side effect, or actual low blood sugar?
Many GLP-1 side effects — nausea, dizziness, fatigue, headache, occasional palpitations — overlap with classic hypoglycemia symptoms. The only sure way to tell them apart is a fingerstick or CGM reading. Without one, you're guessing.
| Symptom | Likely GLP-1 side effect | Likely hypoglycemia | Action |
|---|---|---|---|
| Nausea | Very common weeks 1–4 and after dose increases | Occasional | GLP-1 nausea is persistent and dose-dependent; hypoglycemia nausea comes with shakiness or sweating. Check glucose. |
| Dizziness / lightheaded | Possible, often from dehydration | Common | Check glucose. If normal, rehydrate. |
| Fatigue / foggy | Common, especially first month | Possible | Check glucose. Time-of-day matters — fatigue 2–4 hours after a meal is more hypoglycemia-like. |
| Shakiness / trembling hands | Rare | Classic sign | Check glucose promptly. Treat if symptoms persist and you can't check. |
| Sudden intense hunger | Rare on GLP-1 (appetite suppressed!) | Classic sign | Strong indicator on a GLP-1 specifically, because GLP-1s normally kill hunger. Check glucose. |
| Cold sweat, clammy skin | Rare | Classic sign | Check glucose promptly. |
| Fast heartbeat | Possible | Common | Check glucose. |
| Headache | Common (first weeks) | Possible | Time of day matters. Morning headaches with damp sheets can signal overnight lows. |
| Confusion, difficulty concentrating | Rare | Moderate-to-severe low | Check glucose, and treat presumptively if you can't check — better to overtreat than undertreat. |
| Blurred vision | Rare | Possible (esp. ≤54 mg/dL) | Check glucose. |
| Anxiety spike out of nowhere | Possible | Common | Check glucose. On GLP-1 + insulin or SU, treat unexplained anxiety as a possible low until ruled out. |
The tell: sudden hunger is one of the most useful symptoms on a GLP-1.
GLP-1s normally suppress appetite. If you're suddenly ravenous, something's pushing back against that suppression — and low blood sugar is a leading suspect.
Insulin dose adjustment when starting a GLP-1 (prescriber-discussion framework)
Your baseline A1C drives the conversation. Evidence-based guidance and peer-reviewed case series describe basal insulin reductions of roughly 15–25% and bolus insulin reductions of roughly 25–50% in selected patients near glycemic goal at GLP-1 initiation. At higher baseline A1Cs, immediate reductions are often not needed, but closer monitoring is. The final decision belongs to your prescriber — use this as a discussion tool, not a self-adjustment protocol.
| Baseline A1C | Basal insulin (glargine, degludec, detemir, NPH) | Bolus insulin (lispro, aspart, glulisine, regular) | Monitoring to discuss |
|---|---|---|---|
| Above ~9% | Often no initial reduction | Often no initial reduction | Daily fasting check; post-meal check 2–3×/week |
| ~8–9% | Consider ~10% reduction | Consider 15–25% reduction or hold | Daily fasting + at least one post-meal check, first 2 weeks |
| ~7.5–8% | ~15–20% reduction at initiation | ~25% reduction at initiation | Daily fasting + post-meal + bedtime, first 2–4 weeks |
| Below ~7.5% | ~20–25% reduction at initiation | ~25–50% reduction, or hold bolus entirely | Daily fasting, post-meal, bedtime, and overnight where possible |
| Prescriber-discussion framework, not a self-adjustment protocol. Synthesized from Schweitzer et al. (ScienceDirect, 2022), American College of Cardiology guidance, case series in J Case Rep Images Med (2023), and Ozempic/Mounjaro prescribing information. | |||
Why A1C matters: A high baseline A1C means adding a GLP-1 is mostly additive. A low baseline A1C (near 7%) means you're already at goal — any additional glucose-lowering pushes you below normal if the insulin dose doesn't come down.
Why bolus cuts are larger than basal cuts: Bolus insulin was dosed for the meal you used to eat. A GLP-1 shrinks the meal and slows how it arrives. The mismatch hits bolus dosing first.
Why these are starting points: Many patients need further adjustment after 2 weeks, again after each titration step, and again after meaningful weight loss.
Insulin pump users
Pumps are a specialty conversation. Bring a recent download and ask your pump or endocrinology team to review: basal rates, carb ratios, correction factors, CGM alerts, and hybrid closed-loop settings. A CGM is close to essential for pump users starting a GLP-1.
Should your sulfonylurea dose change — or stop?
When adding a GLP-1 to a sulfonylurea (glipizide, glimepiride, glyburide), ADA 2026 Standards of Care support reducing or discontinuing the sulfonylurea when clinically appropriate, because sulfonylureas raise hypoglycemia and weight-gain risk without adding cardiovascular, kidney, weight, or liver benefit. In a 2024 VA retrospective review of patients who started a GLP-1 while on a sulfonylurea, 38.9% discontinued the sulfonylurea and 29.6% had at least one dose reduction within 12 months.
The three common sulfonylureas — know which one you take
Brand: Glucotrol. Short-acting; risk profile generally milder than the other two.
Brand: Amaryl. Once-daily.
Longer-acting. Specifically flagged by the American Geriatrics Society Beers Criteria as higher-risk for older adults because of active metabolites and prolonged action. Worth a separate conversation about switching before adding a GLP-1.
Script to bring up with your prescriber if they don't raise it first:
"I'm starting a GLP-1. The 2026 ADA Standards of Care support reducing or discontinuing sulfonylureas when they're no longer needed, because of hypoglycemia risk. Can we map out what that should look like for me — at initiation and at each GLP-1 titration step?"
You're not being difficult. You're being informed. Most clinicians will appreciate it.
Meglitinides (repaglinide, nateglinide)
Meglitinides are not sulfonylureas, but they're in the same insulin-secretagogue family — they force insulin release independent of glucose. Same hypoglycemia logic applies: ask whether the dose should be reduced or stopped when starting a GLP-1.
When hypoglycemia risk is highest during GLP-1 treatment
Risk isn't constant. It peaks at three specific moments: the first 2 weeks after starting, the first 2 weeks after each titration step up, and during illness, skipped meals, exercise, or alcohol — especially if you're on insulin or a sulfonylurea.
Window 1: the first 2 weeks of any new GLP-1 dose
Every time your GLP-1 dose changes, your body gets a fresh glucose-lowering push. Risk climbs for about 2 weeks, then settles as you adapt.
Practical move: extra fingerstick checks for the first 2 weeks after every titration step — not just the first one.
Window 2: illness and GI symptoms
Nausea, vomiting, or diarrhea cut food intake. Your usual insulin or sulfonylurea dose assumed you'd eat. Ask for sick-day rules at your first GLP-1 appointment. For sulfonylureas, the general principle is to hold the dose if you're not eating — but confirm with your prescriber. For insulin, basal is often continued (possibly reduced) and bolus is skipped for skipped meals.
Call your prescriber or their after-hours line if you're sick and on insulin or a sulfonylurea. This is not a guess-yourself situation.
Window 3: alcohol, exercise, fasting, and procedures
Alcohol can contribute to delayed lows, including overnight or the next morning. The liver prioritizes metabolizing alcohol over releasing glucose. Drink with food. Avoid drinking on an empty stomach. Lower your overnight CGM alert on nights you drink.
Exercise can lower glucose during and after activity. Ask what pre- and post-exercise glucose checks make sense during GLP-1 titration. Keep fast-acting glucose nearby.
Fasting and procedures — sulfonylureas are commonly held; basal insulin is often reduced; bolus insulin is skipped for skipped meals. Procedure teams may ask you to hold the GLP-1 for a period before surgery (delayed gastric emptying and aspiration risk). Ask, don't guess.
How to monitor your blood sugar on a GLP-1
For the first 2–4 weeks after starting or after each titration step, most prescribers recommend at least once-daily fingerstick checks if you're on insulin or a sulfonylurea. A CGM is the better tool when available, because it catches overnight and asymptomatic lows that fingersticks miss.
If you're on GLP-1 + insulin or a sulfonylurea, minimum monitoring:
- First 2–4 weeks after starting (and after every titration step): fasting + 2 hours after the largest meal, daily. Add a pre-bed check if you took insulin with dinner.
- After stabilizing on a given dose: fasting + one other time, most days.
- Anytime you're sick, changing medications, drinking alcohol, or doing significant new exercise: add checks.
Get a CGM if you qualify
A CGM catches overnight lows you'd sleep through, asymptomatic lows, and trends that let you see a drop coming before it's an emergency.
| Payer | CGM coverage for GLP-1 + insulin/SU users |
|---|---|
| Medicare | Covers therapeutic CGM for people with diabetes who use insulin or have documented problematic hypoglycemia. Sulfonylurea use alone doesn't automatically qualify — but documented hypoglycemia episodes typically do. |
| Commercial insurance | Most cover CGMs for anyone on insulin. Coverage for sulfonylurea-only use varies by plan. |
| OTC CGM (Stelo, Libre Rio) | Labeled for adults NOT using insulin. Not intended for people with problematic hypoglycemia — FDA clearance for Stelo explicitly excludes that group. If problematic hypoglycemia is on your radar, you need a prescribed, alarm-capable CGM. |
If you're on insulin or a sulfonylurea and you don't have a CGM yet, add this to your prescriber list: "Do I qualify for CGM coverage under my plan? If yes, can we start that process today?"
Special situations that raise the risk further
Older adults (65+)
ADA 2026 Section 13: older adults are at greater risk of hypoglycemia, especially with insulin, sulfonylureas, or meglitinides. A severe low at 75 isn't the same as at 35 — consequences include falls, cognitive impact, and slower recovery. Practical adjustments: more conservative dose cuts at GLP-1 initiation, CGM preferred over fingersticks, lower threshold for discontinuing sulfonylurea entirely, and specific attention to glyburide (flagged by Beers Criteria as higher-risk in older adults).
Chronic kidney disease
CKD can increase hypoglycemia risk through impaired insulin clearance and prolonged sulfonylurea effect. Glyburide in particular accumulates and is typically avoided as eGFR declines. If your eGFR has changed since your last medication review, flag it before starting a GLP-1.
Hypoglycemia unawareness
When your body stops giving you warning symptoms (shakiness, sweating, hunger) before a severe low. A CGM isn't optional. Another piece of the management plan is temporarily raising your glycemic target — keeping blood sugars 130+ mg/dL as a floor for a few weeks can partially restore symptom awareness. This is not a DIY adjustment; it's a specific conversation with an endocrinologist.
Alcohol, illness, erratic meals
The combination of a GLP-1, a sulfonylurea, and a pattern of skipped meals is the single highest-risk everyday setup. If any of these are regular parts of your life, you need either tighter monitoring or a smaller initial GLP-1 dose — or both.
Can GLP-1s cause hypoglycemia if you don't have diabetes?
Rarely. GLP-1s are glucose-dependent, so if you're not on insulin or a sulfonylurea and your pancreas is healthy, the drug stops pushing insulin as your blood sugar approaches normal. Most non-diabetic GLP-1 users who feel "low" are actually experiencing GLP-1 side effects, reactive hypoglycemia patterns, or under-eating due to appetite suppression. Lab-proven lows in non-diabetic people on GLP-1 monotherapy are uncommon in the weight-reduction trials for Wegovy, Zepbound, and Foundayo.
Reactive hypoglycemia
Reactive hypoglycemia is a drop in blood sugar 2–4 hours after a meal, especially after meals heavy in refined carbs. If you have a history of it, ask whether short-term glucose monitoring, meal-timing changes, or an endocrinology consultation makes sense before starting a GLP-1.
What tends to help:
- Smaller, more frequent meals with protein at every meal.
- Lower refined-carb, higher-fiber meals.
- Avoiding high-sugar liquids on an empty stomach.
- A short-term CGM to see what's actually happening vs. what you're feeling.
What about compounded GLP-1 medications?
Compounded GLP-1 products are not FDA-approved.
They do not go through the premarket FDA review for safety, effectiveness, and quality that applies to Ozempic, Wegovy, Mounjaro, Zepbound, Rybelsus, and Foundayo. The hypoglycemia warnings and dose-reduction protocols on this page come from FDA-approved labels and should not be assumed to apply the same way to a compounded product.
The interaction concern with insulin or a sulfonylurea still exists for compounded products, but the exact rate data don't apply. If you're using a compounded GLP-1, you need to know exactly what you're receiving — the specific medication name, concentration, dosing units, and the 503A or 503B pharmacy that made it.
If you're on insulin or a sulfonylurea, steer toward FDA-approved options.
A compounded GLP-1 is typically a weight-loss choice for someone who wants a lower price point and doesn't need insurance. It's generally not the right choice for someone managing type 2 diabetes on insulin or a sulfonylurea — because what you actually need is clinical coordination with your existing diabetes care, and that's exactly what a quick-intake compounded telehealth program isn't set up to provide.
Should you start a GLP-1 at all if you're on insulin or a sulfonylurea?
For most people with type 2 diabetes on insulin or a sulfonylurea, the 2026 ADA Standards of Care recommend GLP-1s broadly because of their cardiovascular, kidney, weight, and liver benefits, and because sulfonylureas should generally be phased out. The transition period — the first 2–12 weeks — is the hazard window, and that's where proactive dose reduction, monitoring, and the right kind of prescriber matter.
The honest admission about quick-intake GLP-1 telehealth
If you take insulin or a sulfonylurea, you are not the ideal fit for a 60-second telehealth intake that doesn't ask about your current diabetes meds. Cheap, fast GLP-1 programs are built for weight-loss traffic — mostly non-diabetic patients. If the prescribing clinician isn't asking about insulin, sulfonylureas, hypoglycemia history, and blood sugar readings during the intake, they can't safely dose-adjust you. You want a GLP-1 program with insurance support, prior-authorization handling, and the ability to coordinate with your current diabetes care.
The actual paths for this situation
Path A: Stay with your current prescriber
If you have an endocrinologist or a PCP who manages your diabetes well, this is often the simplest path. Bring the prescriber checklist below to your next appointment. Most prescribers can start a GLP-1 themselves — you don't need a telehealth middleman.
Path B: Ro — FDA-approved GLP-1s with insurance concierge
Ro publicly carries a full FDA-approved GLP-1 formulary — including Ozempic, Wegovy, Mounjaro, Zepbound, and Foundayo — matches LillyDirect / NovoCare pricing on the medication itself, and includes an insurance concierge plus a free GLP-1 Insurance Coverage Checker. For people on insulin or a sulfonylurea who want an FDA-approved brand with insurance support, Ro is the strongest single option.
$39 first month · as low as $74/month with annual plan · medication billed separately
We have not independently verified Ro's internal intake screening, clinician coordination workflow, or prior-authorization performance beyond publicly stated features. Verify their intake process handles your current diabetes regimen before signing up.
Check insurance coverage with Ro's free toolPath C: Use the matching quiz if you're still deciding
If you're earlier in your thinking and unsure what fits your situation, the free 60-second quiz maps your medications, insurance, and current setup to the programs that can actually handle them — including which ones screen for insulin and sulfonylurea use up front vs. which ones don't.
Take the free GLP-1 matching quizWhat to explicitly avoid:
- Quick-intake weight-loss-only programs that don't ask about insulin or sulfonylureas. If the intake form doesn't have a question about current diabetes medications, leave.
- Compounded GLP-1s as a first choice when you're on insulin or a sulfonylurea.
- Changing your insulin or sulfonylurea dose on your own based on an internet article. Including this one. The frameworks here are for your prescriber conversation, not for you to execute at your kitchen table.
What to bring to your prescriber appointment
Print this. Bring it. Check off questions as you go. The appointment goes better when you come in prepared.
Before the appointment — bring these
- Written medication list with current doses and timing (include everything — insulin, oral diabetes meds, blood pressure meds, statins, supplements).
- 2-week blood-sugar log. CGM report if you have one. (Many CGMs have a "share with provider" function — use it.)
- Your most recent A1C and date.
- Your current weight and any recent changes.
- A list of any lows you've had, when, and how you treated them.
The questions to ask
- Based on my baseline A1C and current regimen, how should my basal insulin be adjusted at GLP-1 initiation?
- Should my bolus insulin be reduced or held?
- Should my sulfonylurea be reduced or stopped? At what point?
- How often should I check my blood sugar during the first month?
- Do I qualify for CGM coverage under my plan? If yes, can we start that today?
- Should I have a glucagon rescue kit at home? Which one?
- What symptoms should prompt a same-day call to your office?
- What symptoms should prompt a 911 call instead?
- What should I do if I'm sick and can't eat normally?
- When should we follow up to reassess?
- What happens at each GLP-1 dose increase — do we revisit these adjustments?
If your prescriber doesn't engage with these questions, that's useful information. Consider whether you need a different prescriber or a consultation with an endocrinologist.
Still not sure which GLP-1 program fits your situation?
The free 60-second quiz maps your medications, insurance, and situation to the programs that can actually handle them — including which ones screen for insulin and sulfonylurea use up front.
What we actually verified for this guide
Medical facts verified from primary sources
- FDA prescribing information via DailyMed for Ozempic, Wegovy, Mounjaro, Zepbound, Rybelsus, and Foundayo — rates quoted are pulled directly from current labels.
- ADA Standards of Care in Diabetes — 2026, Sections 6, 9, and 13.
- American College of Cardiology guidance on insulin dose reduction when initiating GLP-1 therapy.
- Schweitzer et al. 2022 (ScienceDirect); VA retrospective analysis 2024 (PMC); case series JCRIM 2023.
- FDA, Medicare, and ADA publications on CGM coverage and indications.
Commercial facts verified separately
- Ro pricing and publicly stated formulary as of April 24, 2026.
- We did not verify Ro's internal intake screening, clinician coordination workflow, or prior-authorization process performance. Where we mention what a program "does," we stick to publicly stated features.
Frequently asked questions
Sources
- Ozempic® Prescribing Information (FDA). DailyMed.
- Wegovy® Prescribing Information (FDA). DailyMed.
- Mounjaro® Prescribing Information (FDA). DailyMed.
- Zepbound® Prescribing Information (FDA). DailyMed.
- Rybelsus® Prescribing Information (FDA). DailyMed.
- Foundayo® Prescribing Information (FDA) and FDA approval materials (April 2026).
- American Diabetes Association. Standards of Care in Diabetes — 2026. Section 6: Glycemic Goals, Hypoglycemia, and Hyperglycemic Crises. Diabetes Care 2026;49(Supp 1).
- American Diabetes Association. Standards of Care in Diabetes — 2026. Section 9: Pharmacologic Approaches to Glycemic Treatment. Diabetes Care 2026;49(Supp 1).
- American Diabetes Association. Standards of Care in Diabetes — 2026. Section 13: Older Adults. Diabetes Care 2026;49(Supp 1).
- American College of Cardiology guidance on insulin dose reduction when initiating GLP-1 therapy.
- Schweitzer M, et al. Deprescribing in type 2 diabetes and cardiovascular disease. ScienceDirect, 2022.
- Reiter M, et al. Adjusting background insulin therapy in type 2 diabetes when initiating a GLP-1. J Case Rep Images Med, 2023.
- Wilkes-Barre VAMC retrospective analysis. Reducing or Discontinuing Insulin or Sulfonylurea When Initiating a GLP-1 Agonist. Federal Practitioner / PMC, 2024.
- CDC. Low Blood Sugar (Hypoglycemia).
- ADA. Low Blood Glucose (Hypoglycemia).
- FDA. FDA's concerns with unapproved GLP-1 drugs used for weight loss.
- FDA. FDA clears first over-the-counter continuous glucose monitor (Stelo).
- Medicare.gov. Continuous glucose monitors.
- American Geriatrics Society Beers Criteria® for Potentially Inappropriate Medication Use in Older Adults.
Still not sure which GLP-1 program fits your situation?
The free 60-second quiz maps your medications, insurance, and current setup to the programs that can actually handle them — including which ones screen for insulin and sulfonylurea use up front vs. which ones don't.
Take the free 60-second quizThis article provides educational information about medication interactions. It is not medical advice and does not replace the judgment of your prescriber. Dose changes must be made under clinical supervision. If you're experiencing severe symptoms of hypoglycemia, call 911. Weight Loss Provider Guide is an independent comparison resource for GLP-1 telehealth providers. We may earn a commission from partner links. Medical content is sourced from FDA prescribing information and the ADA, not affiliate payout. Last verified: .