Best GLP-1 Provider for People With GERD: 2026 Reflux-Aware Guide
By WPG Research Team · Last verified: April 30, 2026 · Weight Loss Provider Guide is an independent comparison resource for GLP-1 telehealth providers
We may earn a commission through provider links — this does not affect our rankings · Informational only, not medical advice. This page helps you choose a provider path; it does not diagnose GERD, gastroparesis, Barrett's esophagus, or medication eligibility.
The bottom line
The best GLP-1 provider for people with GERD is Ro for most readers — reflux-sensitive patients need three things cheap providers can't deliver: a clear FDA-approved medication path, real insurance and prior-authorization help, and ongoing care from people who'll actually message you back when reflux flares. Ro carries Zepbound (tirzepatide) — the FDA-approved GLP-1 with the lowest reported GERD rate on its label that we extracted: 4–5% across the 5, 10, and 15 mg doses.
If you want a low-cost cash-pay path, Embody is the strong runner-up — from $99 for the first month of semaglutide injection (then $299/month ongoing), no insurance required, with a needle-free GLP-1 gum option for readers who want to avoid injections. If you want cash-pay branded medication, Sesame Care is the alternative — and Costco members can access discounted Wegovy/Ozempic through Sesame.
Use Ro if you want the FDA-approved path with insurance and prior-auth help. Free coverage check before you commit.
Quick-pick: which provider matches your situation?
| If this sounds like you… | Best first path | Why |
|---|---|---|
| GERD + I want FDA-approved medication and insurance help | Ro | Zepbound access (lowest reported label GERD rate among the GLP-1s we extracted), insurance concierge, ongoing care |
| GERD + cash-pay + I want a low first-month price | Embody | Low first-month pricing, HSA/FSA eligible, needle-free GLP-1 gum option, 24/7 care-team messaging |
| GERD + I want branded medication, especially if I'm a Costco member | Sesame Care | Branded GLP-1 access; Costco-member pricing on Wegovy/Ozempic |
| GERD + I want compounded with a clinical-feel program | Enhance.MD | Lab work, ongoing provider care, same monthly cost across doses |
| Stable GERD + needle-averse | SHED | Compounded oral and sublingual semaglutide formats |
| Stable GERD + lowest cost + async is fine | Yucca Health | 24-hour provider review, no live visit, BNPL, all 50 states |
| Severe GERD, Barrett's, suspected gastroparesis, or red-flag symptoms | Talk to a gastroenterologist first | Online intake is not the right starting point |
GERD-Aware GLP-1 Path Match (60-second quiz)
Five questions. Personalized recommendation. Built specifically for reflux-sensitive readers. The quiz asks about your reflux frequency, endoscopy history, gastroparesis status, prior GLP-1 experience, and insurance coverage — then routes you to the right path or flags when you should see a specialist first.
Can you take a GLP-1 if you have GERD?
In July 2025, Annals of Internal Medicine published a population cohort study (Azoulay et al.) comparing GLP-1 receptor agonists to SGLT-2 inhibitors in adults with type 2 diabetes. People on GLP-1s had a 27% higher relative risk of new-onset GERD and a 55% higher relative risk of GERD complications. In absolute terms, roughly 0.7 extra GERD cases per 100 patients over three years. Complications included Barrett's esophagus, esophageal strictures, and esophageal cancer.
The part nobody talks about
In October 2024, researchers from Emory and West Virginia University presented a retrospective cohort abstract at the American College of Gastroenterology annual meeting. They looked at people who already had GERD before starting a GLP-1 and found that group had lower all-cause mortality and lower rates of starting a new PPI versus matched controls who didn't start a GLP-1. The authors said prospective studies are needed to confirm. So the picture is more nuanced than the headlines suggest. GLP-1s do appear to raise GERD risk in people without prior reflux. In people with established GERD, the early evidence is more reassuring — though not yet definitive.
The mechanism. GLP-1s don't increase how much acid your stomach makes. They slow gastric emptying — food and acid sit in your stomach longer. That extra dwell time creates more opportunities for reflux. This means the things that fight reflux — eating smaller meals, not lying down for three hours after eating, raising the head of your bed — work just as well or better on a GLP-1 as they do without one.
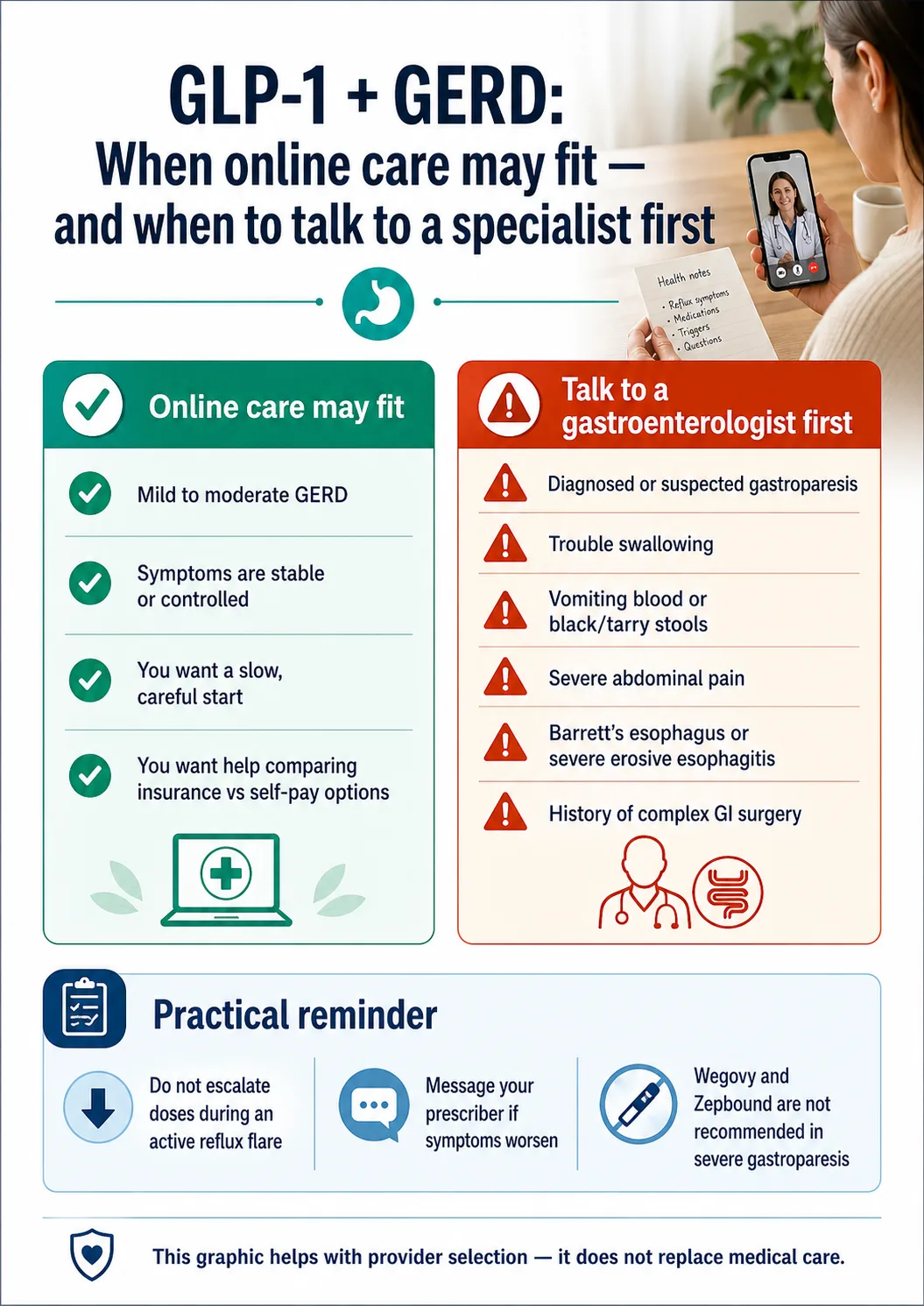
When online-only care isn't enough
Talk to your PCP or gastroenterologist before any online GLP-1 program if you have:
- Trouble swallowing (food sticking, painful swallows)
- Vomiting blood, or stools that look black or tarry
- Severe abdominal pain
- Persistent vomiting that doesn't pass
- Unexplained weight loss before starting any treatment
- Diagnosed or suspected gastroparesis
- Reflux symptoms that started suddenly and are severe
- Recent endoscopy showing severe erosive esophagitis or Barrett's
- A history of complex GI surgery (sleeve, bypass, fundoplication)
- Personal or family history of medullary thyroid carcinoma or MEN 2
These are signs that something more than dietary reflux may be going on.
Which GLP-1 has the lowest GERD risk on its label?
Comparison Table 1: GLP-1 GERD rates from FDA labels and supporting data
| Medication | Brand names | GERD/heartburn signal we extracted | Notes |
|---|---|---|---|
| Tirzepatide | Zepbound, Mounjaro | 4–5% GERD in Zepbound prescribing information across 5/10/15 mg, vs ~1% placebo | Dual-receptor (GLP-1 + GIP) medication — lowest GERD rate extracted from labels |
| Semaglutide injectable | Wegovy, Ozempic | 5% GERD in Wegovy adult label vs 3% placebo | Some head-to-head analyses outside the label have reported higher rates against tirzepatide |
| Semaglutide oral | Rybelsus | Daily oral with a 30-minute fasting window after dosing | Same active ingredient class effect on gastric emptying — oral route is not a reflux workaround |
| Liraglutide | Saxenda, Victoza | ~6–7% GERD/dyspepsia in label data | Daily injection, shorter half-life |
| Orforglipron | Foundayo | FDA approved April 2026 — full GERD label-rate verification still emerging | Oral once-daily, non-peptide GLP-1 |
Sources: Zepbound and Wegovy FDA Prescribing Information; Annals of Internal Medicine July 2025 (Azoulay et al.); Gut 2024 study on shorter-acting vs longer-acting GLP-1 RAs; ACG 2024 abstract. All percentages are reported adverse-event rates from labels — not direct head-to-head trial comparisons unless noted.
Why tirzepatide tends to be a sensible first option for reflux-prone patients
Tirzepatide acts on two receptors — GLP-1 and GIP. Zepbound's label still describes delayed gastric emptying as part of how the medication works. But when you compare GERD adverse-event rates side by side, Zepbound's label numbers are lower than Wegovy's. That's not a guarantee tirzepatide will be easier on your reflux — individual response varies — but it's the strongest signal we can give you from public sources. If your prescriber gives you a choice and your insurance allows it, the label evidence supports tirzepatide as the reflux-conservative default.
Quick note on oral semaglutide (Rybelsus): Some readers think going oral instead of injectable is a reflux workaround. It isn't. The medication still works through the same gastric-emptying-slowing pathway. Rybelsus also requires a 30-minute fasting window after dosing, which can interact with morning reflux routines. If you're choosing oral specifically for reflux reasons, that's a conversation to have with your prescriber — not the obvious answer.
A 2024 study in Gut found that shorter-acting GLP-1 RAs (like exenatide twice daily) were associated with more GERD than longer-acting ones (semaglutide and tirzepatide weekly), in a large population analysis. That supports discussing a longer-acting option with your prescriber if you have GERD.
Best GLP-1 provider for people with GERD: full comparison
For most people with GERD, the right provider gives you a clear FDA-approved or transparently-disclosed compounded option, lets you start at the lowest dose, won't penalize you for staying on a low maintenance dose, and answers symptom messages without trying to rush you up the dose ladder.
We scored the major providers on six things that matter when GERD is part of the picture — not on sticker price, marketing polish, or affiliate payout.
Comparison Table 2: GERD Compatibility Provider Scorecard
Each provider is editorially scored 0–3 on each criterion based on publicly available pricing pages, intake flow language, and support documentation. Higher is better. Composite score out of 18. This is editorial scoring, not a medical claim that any provider's program is "safe for GERD." Verified April 30, 2026.
| Provider | FDA-approved tirzepatide | Low starting dose | Same cost across doses | Multiple med options | Provider messaging | Cancellation clarity | Score (/18) |
|---|---|---|---|---|---|---|---|
| Ro | 3 | 3 | 2 | 3 | 2 | 2 | 15 |
| Embody | 0 | 3 | 0 | 3 | 3 | 2 | 11 |
| Sesame Care | 3 | 3 | 2 | 3 | 2 | 2 | 15 |
| Enhance.MD | 3 | 3 | 3 | 2 | 2 | 2 | 15 |
| SHED | 2 | 3 | 2 | 3 | 2 | 2 | 14 |
| Yucca Health | 2 | 3 | 2 | 2 | 2 | 3 | 14 |
Ro — best for FDA-approved Zepbound with insurance support
Why Ro for GERD: Ro pairs FDA-approved tirzepatide (Zepbound and Zepbound KwikPen) with an insurance concierge that submits prior-authorization paperwork on your behalf. Ro runs a free GLP-1 Insurance Coverage Checker so you find out where you stand before you commit. Ro's care team includes provider-ordered labs when needed and secure messaging.
Best for
GERD readers with commercial insurance. Anyone who specifically wants brand-name Zepbound. Anyone whose reflux is real enough that the insurance concierge is worth it.
Skip if
You're hard self-pay, your insurance excludes weight-loss medication, and brand-name pricing is unworkable. Go to Embody or Yucca instead.
The honest negative: Ro doesn't carry compounded GLP-1 medication. If you're hard self-pay and your insurance won't cover Zepbound at all, Ro won't be the cheapest path — Embody, Yucca, or SHED will save you money. Ro skips compounded on purpose: every medication is FDA-approved and comes from Lilly or Novo. That's exactly what most GERD readers want when they're already nervous about adding a medication that affects digestion.
Check your Ro coverage and GLP-1 eligibility →If insurance and FDA-approved medication clarity are what's holding you back, this is the lowest-uncertainty place to start.
Embody — best for a low first-month cash-pay price and a needle-free GLP-1 gum option
Why Embody for GERD: Embody is a cash-pay telehealth program built for people without insurance — no insurance is required and HSA/FSA cards are advertised as accepted. For GERD readers, two things stand out: the first month starts low, and Embody offers a needle-free GLP-1 gum alongside weekly injections of compounded semaglutide or tirzepatide. Tirzepatide is the more reflux-friendly default in the label data on this page, and Embody offers it. A 24/7 care team handles messaging if symptoms flare.
Best for
Cash-pay readers who want the lowest first-month price, needle-averse readers who want a GLP-1 gum option, and anyone using HSA/FSA dollars.
Skip if
Your insurance covers Zepbound — Ro will be cheaper — or you specifically want an FDA-approved finished medication.
The honest negative: Embody's shipped medications are compounded semaglutide and tirzepatide — not FDA-approved finished drug products — and ongoing refills cost more than the first month. The FDA has been increasingly active on compounded GLP-1 oversight in 2026. Availability is broad across the U.S. but not every state; confirm your state during intake.
Check Embody eligibility and pricing →Best low-cost cash-pay starting point if a low first-month price or a needle-free option is your priority.
Sesame Care — best for cash-pay branded medication and Costco members
Why Sesame Care for GERD: Sesame's current GLP-1 program lists FDA-approved medications including Wegovy pill, Wegovy pen, Zepbound, Zepbound KwikPen, Foundayo, and Ozempic. The standout for many readers: Costco members can access Ozempic or Wegovy at $349/month, with the first two months at $199/month, through Sesame's Costco partnership. Verify current terms before booking.
Best for
Cash-pay readers who want FDA-approved medication, Costco members, anyone who wants provider-included care without insurance friction.
Skip if
You want concierge-style insurance prior-auth help — Ro is stronger there.
Best cash-pay branded path, especially if you have a Costco membership.
Enhance.MD — best for clinical-feel cash-pay compounded
Why Enhance.MD for GERD: If your reflux is real enough that you want lab work and a more hands-on protocol, but you can't afford the brand-name route, Enhance.MD fits. Programs include metabolic lab testing, ongoing provider care, and same monthly cost across doses — so you're not paying more if you stay on a lower dose because of GERD tolerance. Compounded medications are clearly disclosed as not FDA-approved.
Best for
Self-pay readers who want lab monitoring and tighter clinical oversight specifically because of GERD or other comorbidities.
Skip if
Cost is your top priority — Embody, Yucca, or SHED will be less expensive.
Use this if you want a more clinical-feel program and understand the compounded-medication tradeoff.
SHED — option for the needle-averse
Why SHED for GERD: SHED offers compounded GLP-1s in multiple formats — including injections, oral semaglutide drops, and semaglutide lozenges. For needle-averse readers, the oral formats are a real differentiator.
Best for
Needle-averse readers willing to use a compounded oral or sublingual product, who understand compounded medications are not FDA-approved.
Skip if
You want FDA-approved medication, or your priority is clinical oversight.
Yucca Health — lowest cost async option
Yucca Health offers 24-hour provider review, no live visit required, BNPL payment options, and service in all 50 states. Compounded semaglutide as low as $146/month for new patients on a 6-month plan (provider-stated). Clear plan terms and cancellation language.
Best for
Stable GERD readers who want the lowest published cost and are comfortable with async-only care.
Skip if
You want live provider visits or FDA-approved medication — Ro or Sesame Care is the better fit.
A transparency note on MEDVi
MEDVi is not on our recommendation list for this specific page, and we want to explain why. On February 20, 2026, the FDA issued warning letter #721455 to MEDVi citing false or misleading marketing claims about compounded semaglutide and tirzepatide products. In March 2026, the FDA issued similar warning letters to more than 30 telehealth companies for the same broad category of marketing issues. We feature MEDVi on other pages where the audience and context are different. For a GERD-specific page where readers are already cautious about medication safety, the regulatory context is material — and you deserve to see it before clicking anything. If you're a current MEDVi customer, see their current site for their most recent disclosures and read the FDA letter directly at fda.gov.
FDA-approved vs compounded GLP-1s: which is right if you have GERD?
FDA-approved brand-name GLP-1s
Zepbound, Wegovy, Mounjaro, Ozempic, Saxenda, Foundayo — from Eli Lilly or Novo Nordisk, made in inspected facilities, full FDA-reviewed labels, published Phase 3 clinical trial data. The exact GERD/heartburn rate, the trial population — all documented.
Compounded GLP-1 products
Prepared by compounding pharmacies under 503A or 503B rules. Typically much cheaper than brand. Not FDA-approved as finished products. Should not be described as generics or the same as FDA-approved products — the FDA has explicitly warned telehealth marketers against that framing.
Why FDA-approved is the more conservative pick for GERD: With brand-name Zepbound, we know from the FDA label what to expect on the GERD dimension. We can quote the label numbers (4–5%). We know how the manufacturer says to titrate. That predictability is the whole reason brand-name medication exists. We don't have the same quality of head-to-head GERD data for every compounded version.
When compounded might still make sense
- You're self-pay and brand-name pricing is genuinely unworkable
- Your insurance excludes weight-loss medication entirely
- You understand and accept the tradeoffs
- You're working with a provider that uses an accredited compounding pharmacy and is transparent about it
- You're starting at a low dose, going slow, and have a clear plan if reflux flares
The 2026 regulatory context
On April 30, 2026, the FDA proposed to formally exclude semaglutide, tirzepatide, and liraglutide from the 503B bulks list. The FDA also issued more than 30 warning letters in March 2026 to telehealth companies for false or misleading compounded GLP-1 marketing. The rules around compounded GLP-1s are tightening. If you go compounded, choose a provider with a clean disclosure and a clear regulatory track record.
How to start a GLP-1 if you have GERD: the practical approach
Step 1: Pick the right medication with your prescriber
The label data leans toward tirzepatide (Zepbound) as the reflux-conservative default. The 4–5% Zepbound label rate vs. Wegovy's 5% adult label rate isn't a dramatic gap, but it's the cleanest signal we have. If cost or insurance forces semaglutide, the rest of this approach still works — just be more deliberate about lifestyle and titration.
Step 2: Start at the absolute lowest dose
- Tirzepatide: 2.5 mg weekly for at least 4 weeks. On-label starting dose for Zepbound and Mounjaro — a non-therapeutic warm-up dose your body adjusts to before you go up.
- Semaglutide: 0.25 mg weekly for at least 4 weeks. Same logic.
- Some compounded providers offer custom or microdose options below 2.5 mg tirzepatide. If you've reacted poorly to standard starting doses before, ask whether your provider offers this.
Step 3: Build the lifestyle scaffold
- Eat 4–5 small meals instead of 2–3 large ones. Smaller meals = less gastric pressure = less reflux.
- Stop eating 3 hours before bed.
- Sleep with the head of your bed elevated 6 inches (a wedge pillow works; just propping pillows under your head doesn't).
- During titration, limit alcohol, caffeine, chocolate, peppermint, citrus, tomato sauce, raw onions, and spicy or very fatty foods.
- Don't lie down or bend over for 60 minutes after eating.
- Drink water between meals, not during them. Big volumes of liquid in a slow-emptying stomach = more pressure = more reflux.
Step 4: Talk to your prescriber about acid-suppression strategy
Some telehealth clinicians discuss starting a short course of a PPI — like omeprazole — when initiating a GLP-1 in patients with reflux history. Published evidence for prophylactic PPI use specifically with GLP-1s is thin, but the strategy is in clinical use. Don't change your PPI or start a new one on your own. The decision of whether to add or continue acid suppression is a clinical conversation — bring it up in your first message.
Step 5: Hold the dose if reflux flares
Standard titration: 2.5 mg → 5 mg → 7.5 mg → 10 mg → 12.5 mg → 15 mg, every 4 weeks. You don't have to follow that schedule. If your reflux flares at the 4-week mark, hold the current dose for another 4–8 weeks. A good provider will support this. A bad one will pressure you to escalate. The provider scorecard above is built around exactly this.
Step 6: Trust that weight loss eventually helps
The ACG 2024 abstract is the long-game silver lining. Among patients with established GERD who started a GLP-1, downstream PPI initiation was lower and mortality was lower than the comparison group. Weight loss is recommended for overweight and obese patients with GERD in major guidelines, and the 10–20% body weight loss most patients hit on these medications reduces intra-abdominal pressure over time. The first three to six months are the toughest. After that, the picture usually changes.
Acid suppression options and how they compare
Antacids, H2 blockers, and PPIs work differently and fit different reflux severity. The decision of what to use, and for how long, sits with your prescribing provider — not with us, and not with you alone.
| Option | How it works | Typical fit | Watch for |
|---|---|---|---|
| Antacid (e.g., Tums) | Neutralizes acid in the moment | Mild, occasional reflux | Short duration; doesn't treat the underlying issue |
| H2 blocker (e.g., famotidine / Pepcid) | Reduces acid production | Mild–moderate reflux | Tolerance can develop over weeks of daily use |
| PPI (e.g., omeprazole / Prilosec) | Blocks acid production at the source | Moderate–severe reflux | Long-term use should be clinician-guided at lowest effective dose |
Drug-interaction note: GLP-1s slow gastric emptying, which can affect how some oral medications absorb. If you take other prescription medications, ask your prescriber about timing.
GERD severity decision tree: what should you actually do?
Your GERD severity changes which path makes sense. Five tiers below — find yourself.
Mild occasional heartburn (no diagnosis, not on a PPI)
Most providers work. Tirzepatide preferred per label data. Lifestyle scaffold is enough for most.
Recommended path: Embody if you're self-pay; Ro if you have insurance.
Diagnosed GERD, currently controlled on a daily PPI
Tirzepatide preferred. Continue your PPI through titration unless your provider says otherwise. Plan slow titration (8 weeks per dose minimum if symptoms flare).
Recommended path: Ro if insured (the insurance concierge helps document GERD as a comorbidity); Embody if you're self-pay and want a low first-month price to start slow.
Diagnosed GERD with prior endoscopy showing erosive changes
Talk to your gastroenterologist before starting a GLP-1. They may want a repeat endoscopy or a longer trial of acid suppression first. Tirzepatide preferred. Plan extended titration.
Recommended path: Enhance.MD or Ro — both bring more clinical structure. Don't go async-only here.
Barrett's esophagus, severe erosive esophagitis (LA grade C/D), or esophageal stricture
Do not start a GLP-1 without explicit gastroenterologist clearance and a coordinated plan. The cancer-monitoring stakes with Barrett's are real, and you need a specialist managing the timeline.
Recommended path: No provider at this tier without GI input first. Take the matching quiz instead of clicking a provider link.
Diagnosed or suspected gastroparesis (delayed gastric emptying)
GLP-1s are not recommended in severe gastroparesis per the Wegovy and Zepbound labels. GLP-1s further delay gastric emptying. Adding one to gastroparesis can worsen symptoms significantly.
Recommended path: None. Talk to your gastroenterologist about non-GLP-1 weight management options (orlistat, naltrexone-bupropion, or surgical paths).
What to do if reflux gets worse after starting a GLP-1
| Symptom pattern | What to do |
|---|---|
| Occasional mild heartburn after meals | Tighten the lifestyle scaffold (smaller meals, no late dinners); mention at your next check-in |
| Heartburn that started after a dose increase | Message your provider before escalating again. Ask about holding the current dose for another 4–8 weeks |
| Persistent vomiting (more than 24–48 hours) | Contact your provider promptly. Dehydration is the immediate concern |
| Trouble swallowing food, or food sticking | Seek medical care. This is not an online-provider issue |
| Blood in vomit, or black/tarry stools | Go to urgent care or the ER. This is potentially serious GI bleeding |
| Severe abdominal pain, especially upper-right | Contact a clinician urgently. Could be gallbladder-related, a known GLP-1 risk |
| Symptoms that resolved overnight | Don't escalate during an active flare; report at your next check-in and message sooner if symptoms recur |
| Reflux waking you up at night | Add wedge-pillow elevation immediately; message your provider about whether to start or adjust acid suppression |
What this will actually cost
With insurance
- Zepbound through Ro with Lilly Savings Card: as low as $25/fill for eligible commercially insured patients
- Ro insurance concierge handles prior authorization submission
- Wegovy through Ro with Novo Care savings: variable by plan
Without insurance: brand-name
- LillyDirect Self Pay: $299/mo (2.5 mg), $399/mo (5 mg), $449/mo (7.5–15 mg) — verify terms
- Through Ro: $39 to start, then $74–$149/mo membership + medication
- Costco members through Sesame: Ozempic or Wegovy at $349/mo, first 2 months $199/mo
Without insurance: compounded
- Embody compounded sema injection: from $99 first month, then $299/mo
- Embody compounded tirzepatide injection: from $149 first month, then $399/mo
- Yucca Health compounded sema: as low as $146/mo (6-mo plan)
- Enhance.MD: flat across doses; varies by plan length
Hidden costs to verify before you click
- Is medication billed separately from membership?
- Does the intro price jump after month 1?
- Are dose increases an upcharge?
- Are labs included or extra?
- Is shipping included?
- What's the cancellation policy if you need to stop because of reflux?
- What happens if insurance denies?
All pricing verified April 30, 2026. Provider pricing changes — always confirm at checkout before enrolling.
What customers are saying
We use customer feedback only as evidence of service experience — not as medical claims about whether GLP-1s are safe for GERD specifically. Individual experiences vary.
"I'm not fighting against my own body anymore."
Frequently asked questions
What is the best GLP-1 provider for acid reflux?
For most people with acid reflux or GERD, the best provider is Ro because it pairs FDA-approved Zepbound (the GLP-1 with the lowest reported GERD rate on its label we extracted, 4–5%) with insurance and prior-authorization support. If you're paying cash, Embody is a low-cost compounded option — from $99 for the first month of semaglutide injection (then $299/month ongoing), with a needle-free GLP-1 gum option and no insurance required. Sesame Care fits cash-pay branded medication, especially for Costco members.
Which GLP-1 is least likely to cause acid reflux?
Of the FDA labels we extracted, Zepbound (tirzepatide) reports the lowest GERD rate — about 4–5% across the 5, 10, and 15 mg doses, vs. ~1% on placebo. Wegovy (semaglutide) injection reports GERD at 5% vs. 3% on placebo in adults. The label evidence supports tirzepatide as the more reflux-friendly default — but the medication choice is a prescriber decision.
Can I take Ozempic if I have GERD?
You can be a candidate, but tirzepatide-based options (Zepbound, Mounjaro) report lower GERD rates than Ozempic in label data. If you have a choice, tirzepatide is the more reflux-friendly default. If you must use Ozempic, start at 0.25 mg, titrate slowly, and discuss acid-suppression strategy with your provider.
Does Wegovy cause acid reflux?
Yes — heartburn, dyspepsia, and GERD are listed on the Wegovy label as possible side effects. The adult Wegovy label reports GERD in about 5% of patients vs. 3% on placebo. Most cases are mild and improve as the body adjusts to a stable dose.
Does Zepbound cause heartburn?
About 4–5% of patients in the SURMOUNT trials reported GERD, compared to roughly 1% on placebo. Wegovy and Zepbound labels also list belching, bloating, nausea, and vomiting as possible side effects.
Should I start a PPI before my GLP-1?
Some telehealth clinicians discuss short-term PPI use when initiating a GLP-1 in patients with reflux history, but the published evidence for prophylactic PPI use specifically with GLP-1s is thin. This is a clinical decision your prescriber should make. Don't change your PPI on your own.
Will a GLP-1 make my GERD worse permanently?
Probably not. Reflux from GLP-1s is reported most often during dose escalation and may decrease at a stable dose. The ACG 2024 abstract suggests that for patients with established GERD, starting a GLP-1 was associated with lower downstream PPI initiation and lower mortality — likely because 10–20% body weight loss reduces reflux pressure over time.
Is tirzepatide safer than semaglutide for someone with GERD?
"Safer" is the wrong word — both are FDA-approved with established safety profiles. But the FDA labels report lower GERD rates for tirzepatide than for semaglutide, so for a reflux-prone patient choosing between them, tirzepatide is the more reflux-friendly default.
Are GLP-1s safe with Barrett's esophagus?
There is no Barrett's-specific contraindication on the Zepbound or Wegovy labels, but the increased GERD complication rate found in the 2025 Annals analysis warrants a gastroenterologist's input before starting if you already have Barrett's. The cancer-monitoring stakes are real.
Can I take a GLP-1 if I have gastroparesis?
GLP-1s are not recommended in severe gastroparesis per the Wegovy and Zepbound prescribing information. They further delay gastric emptying and can worsen symptoms. Talk to your gastroenterologist before considering one.
Are compounded GLP-1s a different reflux risk than brand-name?
There is no published evidence that compounded GLP-1 products have a different GERD profile than the brand-name versions. The pharmacologic class effect — slowed gastric emptying — applies regardless of the product form. Choose between compounded and FDA-approved based on cost, regulatory comfort, and access — not based on reflux risk.
How long until reflux improves after starting a GLP-1?
GI side effects are reported most often during dose escalation and may decrease over time at a stable dose. If your reflux hasn't improved after 8 weeks at a stable dose, talk to your provider about extending the dose or switching medications.
Can I stay on a low GLP-1 dose forever to avoid GERD?
Many patients tolerate 2.5 mg or 5 mg tirzepatide indefinitely and still see meaningful weight loss. If your provider's pricing escalates with dose, this becomes more expensive — which is why the same-cost-across-doses providers are highlighted in the scorecard.
What should I tell my online GLP-1 provider about my GERD?
At intake, share: your current GERD diagnosis (if any), how often you have symptoms, what triggers them, what reflux medications you're on now, any prior endoscopy findings, hiatal hernia history, history of vomiting or nausea, and any prior delayed gastric emptying.
What happens if I need to stop my GLP-1 because of reflux?
Cancellation terms vary by provider — verify on each provider's terms page before enrolling. Generally: month-to-month plans can be canceled before the next billing cycle; multi-month prepay plans may have proration or cancellation rules that limit refunds. This is one of the questions worth asking up front.
Still not sure which path is right for you?
If your situation doesn't fit cleanly into any of the tiers above — or you've already had a bad experience with one GLP-1 — take our matching quiz. It accounts for reflux severity, insurance status, medication preference, budget, and red-flag symptoms, then routes you to the path that fits.
A final note from the team
We built this page because people with GERD deserve a real answer — not a generic "best providers" listicle that ignores their actual situation. The medication choice and the provider choice both matter, and they have to be made together.
If you've recognized yourself in any of the higher-risk tiers, please don't skip the gastroenterologist conversation. The cost of getting this wrong with Barrett's or undiagnosed gastroparesis is real, and we'd rather lose the click than lose your trust.
Methodology: how we made these picks
We ranked providers using a GERD-aware framework, not sticker price or affiliate economics. Medical and regulatory claims were checked against FDA prescribing information, manufacturer safety pages, ACG and AGA guidance, and peer-reviewed sources. Commercial provider claims were checked against official provider pages, intake flows, and support documentation. We weighted clinical support and medication-route clarity more heavily than sticker price because GERD changes the buying decision.
We declined to feature MEDVi as a recommended option on this specific page given the February 2026 FDA warning letter, regardless of its commercial position elsewhere on our site. We may earn a commission if you sign up through provider links. This does not affect our rankings — we have declined affiliate partnerships with providers that didn't meet our standards.
What we actually verified (April 30, 2026)
Zepbound and Wegovy FDA Prescribing Information · Annals of Internal Medicine, July 2025 (Azoulay et al.) — population cohort study on GLP-1s and GERD risk · ACG 2024 abstract (Emory/WVU, TriNetX cohort) — GLP-1 outcomes in patients with established GERD · Gut 2024 — short-acting vs. long-acting GLP-1 RAs and GERD · FDA Warning Letter #721455 to MEDVi (February 20, 2026) · FDA press release on 30+ telehealth warning letters (March 2026) · FDA proposed rule on 503B bulks list (April 30, 2026) · Provider pricing pages: Ro, Embody (joinem.co), Sesame Care, Enhance.MD, SHED, Yucca Health · LillyDirect Self Pay Journey program savings terms · Lilly Zepbound Savings Card terms · ACG patient resource on PPIs · AGA Clinical Practice Guideline on GERD.
Sources
- Azoulay L, et al. "Glucagon-Like Peptide-1 Receptor Agonists and Risk for Gastroesophageal Reflux Disease in Patients With Type 2 Diabetes." Annals of Internal Medicine, July 2025.
- American College of Gastroenterology Annual Scientific Meeting 2024 — abstract on GLP-1 outcomes in patients with established GERD (Emory/WVU, TriNetX cohort).
- Gut 2024 — population-level retrospective cohort study on shorter-acting vs. long-acting GLP-1 RAs and GERD.
- Zepbound (tirzepatide) Prescribing Information, Eli Lilly.
- Wegovy (semaglutide) Prescribing Information, Novo Nordisk.
- Saxenda (liraglutide) Prescribing Information, FDA Access Data.
- FDA Warning Letter #721455 to MEDVi, LLC (February 20, 2026).
- FDA Press Release: FDA Warns 30 Telehealth Companies Against Illegal Marketing of Compounded GLP-1s (March 2026).
- FDA Press Release: FDA Proposes to Exclude Semaglutide, Tirzepatide, and Liraglutide on 503B Bulks List (April 30, 2026).
- ACG patient resource on Acid Reflux/GERD and PPIs · AGA Clinical Practice Guideline: Management of GERD.
Last verified: April 30, 2026. This article is for informational purposes only and is not medical advice. Always consult a licensed healthcare provider before starting any GLP-1 medication. Compounded medications discussed on this page are not FDA-approved as finished drug products. Weight Loss Provider Guide is an independent comparison resource for GLP-1 telehealth providers.
Affiliate disclosure: We may earn a commission if you sign up through links on this page. This does not affect our rankings or analysis.